
Abstract
Background
The therapeutic methods of iatrogenic colon perforation have not been performed despite the increasing rates of successful management by endoscopic clip closure. This study aimed to analyze the efficacy and complications of endoscopic clip closure and to identify the risk factors associated with the need for early surgery to avoid more invasive surgical interventions and adverse complications after endoscopic clip closure for iatrogenic colon perforation.
Methods
A retrospective multicenter review of the clinical course experienced by 32 patients with iatrogenic colon perforation who were treated using immediate endoscopic clip closure between January 2005 and December 2009 was performed.
Results
The technical success rate for endoscopic clip closure was 91% (29/32). After endoscopic clip closure, 22 patients (76%) required medical treatment for colon perforation, and seven patients (24%) had surgical treatment. Of the 22 patients who had only endoscopic clip closure, 17 (59%) had a favorable clinical course. Five patients had a long hospital stay with complication including abscess formation (three cases). Four patients underwent early surgery within 24 h, and laparoscopic simple closure was possible. But for three patients with surgery delayed more than 48 h, open laparotomy with colon resection including diversion were required. The risk factors associated with the need for early surgical treatment within 24 h after endoscopic clip closure were a large perforation [odds ratio (OR), 9.25; 95% confidence interval (CI), 1.85–46.20], leukocytosis (OR 6.58; 95% CI 1.86–23.29), fever (OR 5.05; 95% CI 1.05–24.28), severe abdominal pain (OR 4.30; 95% CI 1.17–15.83), and a large amount of peritoneal free air (OR 4.05; 95% CI 1.40–11.71).
Conclusion
The endoscopic clip closure procedure can significantly reduce the frequency of surgery among patients with iatrogenic colon perforations. However, the decision for surgery must be made early after endoscopic clip closure to prevent adverse complications for patients with higher risk factors.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Colonoscopy is an essential tool for both diagnosis and therapy of colon lesions. Iatrogenic perforation of the colon is a rare but serious feared complication. The frequency of perforation after colonoscopy is estimated to be 0.03–0.9% for diagnostic colonoscopy and 0.15–3% for therapeutic colonoscopy [1–5]. Because the indications for endoscopic resection of precancerous and malignant lesions have been expanded recently with advances in therapeutic colonoscopy such as endoscopic submucosal dissection (ESD), the frequency of colon perforation associated with therapeutic colonoscopy is increasing [5]. Colon perforation can progress rapidly to peritonitis and sepsis, with significant morbidity and mortality. Thus, colon perforations must be treated immediately, and all colonoscopists must be fully aware of treatment methods that prevent colon perforation.
The site of colon perforation must be closed immediately and completely to prevent related complications. Traditionally, surgery has been the standard treatment.
Recently, endoscopic clip closure has become popular as a noninvasive method for closing the site of iatrogenic colon perforation with clean bowel preparation [3, 6]. However, the efficacy and complications of endoscopic clip closure for iatrogenic colon perforation have not been fully elucidated. For some patients with endoscopic clip closure, the development of peritonitis has followed a slow progression with ambiguous symptoms even when the endoscopic clip closure was not complete. In such cases, it is difficult to make a decision about additional surgery, and the inadequate prolonged medical treatment may cause complications such as relapsing peritonitis, abscess, and fistula formation.
For cases with delayed surgical treatment, more invasive surgery including open colon resection with diversion may become inevitable. For cases of iatrogenic colon perforation, medical or surgical treatment should be chosen based on such factors as the patient’s general condition, the leakage of contaminants, the size and location of the perforation, the residual lesions, and the clinical symptoms after the perforation.
The prompt and effective choice of a therapeutic method may prevent both unnecessary and more invasive surgery, including colon resection with diversion due to inadequate prolonged medical treatment after endoscopic clip closure in patients with iatrogenic colon perforation. This study aimed to analyze the efficacy and complications associated with endoscopic clip closure for iatrogenic colon perforation and to identify the predictors indicating the need of early surgery so that invasive surgical treatment and severe complications can be avoided.
Patients and methods
A retrospective multicenter review of patients with iatrogenic colon perforations was performed at three hospitals in Gwangju province, the Republic of South Korea from January 2005 to December 2009. The patients included in this study had colon perforation confirmed by peritoneal free air detected by plain chest or abdominal X-rays after endoscopic clip closure. The criteria for exclusion from the study specified cases that had suspected perforation with endoscopic clip closure but no peritoneal free air detected by X-ray, colon perforation caused by the underlying disease such as a malignant obstruction or colon diverticulum, and patients with delayed perforation.
A skilled endoscopist performed endoscopic clip closure at the perforation site immediately. If the colonoscope was difficult to handle during closure of the lesion by clipping, a hood or thin upper endoscope was used. The mean number of endoscopic clips used was 7.4 (range, 1–14).
After the endoscopic clip closure for colon perforation, the patient fasted and was treated with antibiotics. The patient also was monitored for the presence of peritonitis in consultation with a colon surgeon.
Decompression of the pneumoperitoneum by percutaneous needle aspiration was attempted for patients who reported severe abdominal distension. The signs and symptoms of peritonitis and sepsis were evaluated through review of symptoms, physical examination, blood testing, and abdominal computed tomography (CT). If clinical aggravation was observed, the patient proceeded to surgery immediately based on the clinician’s judgment. For the surgery, a laparoscopic procedure was used where possible. Simple closure or colon resection with diversion was performed depending on the severity of the peritonitis and the degree of colon inflammation.
A large perforation was defined as 10 mm or larger, and a small perforation was defined as smaller than 10 mm. A favorable prognosis after treatment of the colon perforation was defined as complete resolution of the perforation without complications and a hospital stay shorter than 2 weeks. An unfavorable prognosis was defined as the development of complications and a hospital stay of 2 weeks or longer.
The amount of peritoneal free air was estimated by measuring the distance between the right diaphragm and the upper margin of the liver using plain chest X-ray. If the distance was 3 cm or longer, the amount of free air was considered large.
If abdominal pain could be controlled with antispasmodic or non-narcotic analgesic medications, it was considered mild pain. If it was aggravated or required the use of narcotic analgesic medications on two occasions or more, the pain was considered severe.
The clinical characteristics were analyzed according to the outcome of endoscopic clip closure in terms of perforation size, perforation site, degree of bowel preparation, and clinical data including abdominal pain, abdominal distention, physical examination findings, blood testing over 24 h, and hospital length of stay. For patients who had surgical treatment, the elapsed time from colon perforation to surgery was investigated.
Statistical analysis used SPSS version 15.0 (SPSS Inc., Chicago, IL, USA). Nominal variables were analyzed using chi-square testing, and the Student’s t-test was used to analyze continuous variables. The risk factors for early surgery were analyzed by Cox regression analysis. Statistical significance was accepted as a P value less than 0.05.
Results
Incidence and clinical characteristics
During 4 years at three hospitals, 51,738 patients underwent colonoscopy, with colon perforation occurring in 32 (0.06%) cases. During 43,115 diagnostic colonoscopy procedures, 13 colon perforations (0.03%) occurred. Endoscopic mucosal resection (EMR) was performed in 8,623 cases, 19 (0.2%) of which resulted in colon perforation. A snare was used in 8,275 EMRs, which resulted in eight cases (0.1%) of colon perforation. The endoscopic knife was used in 348 ESDs, with colon perforation occurring in 11 cases (3%). From these patients, 29 who had endoscopic clip closure immediately after the colon perforation were enrolled in this study (Fig. 1). Of these 29 patients, 16 (55%) were men and 13 (45%) were women.

Patient flow chart of initial endoscopic clip closure for iatrogenic colon perforation
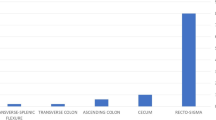
The mean age of the patients was 58.1 ± 9.9 years. The site of perforation was the sigmoid colon in 13 cases (45%), the rectum in six cases (21%), the transverse colon in six cases (21%), the splenic flexure in two cases (7%), the hepatic flexure in one case (3%), and the ascending colon in one case (3%). In all cases, the perforation was large for the diagnostic colonoscopy procedures and small for the therapeutic colonoscopy procedures. The pathology of the polyp was low-grade dysplasia in eight cases, high-grade dysplasia in six cases, and mucosal cancer in five cases. The polyp size was smaller than 10 mm in two cases, 11 to 20 mm in seven cases, 21 to 30 mm in seven cases, and 30 mm or larger in three cases. The shape of the polyp was semipedunculated in six cases, sessile in five cases, and laterally spreading tumor in eight cases.
Clinical symptoms in 24 h
The frequency of severe abdominal pain was significantly greater for the patients who had a diagnostic perforation (70%) than for the patients who had a therapeutic perforation (32%) (P = 0.048). A large amount of peritoneal free air was found in ten cases (100%) among the diagnostic perforation patients and in ten cases (45%) among the patients with therapeutic perforations (P = 0.009). Among the diagnostic perforation patients, one patient had a high fever (≥38°C), and three patients had a mild fever (37–38°C). No patient had a leukocyte count increased to more than 15,000/mm3 within 24 h after perforation. Eight diagnostic perforation patients (80%) and six therapeutic perforation patients (32%) showed a mild increase reaching 10,000–15,000/mm3 (P = 0.013).
Efficacy and complication of endoscopic clip closure
The technical success rate for initial endoscopic clip closure was 91% (29/32). Of the 29 patients, 22 (76%) had continued medical treatment after endoscopic clip closure for colon perforation, and 7 (24%) had surgical treatment. Four diagnostic perforation patients (40%) and three therapeutic perforation patients (16%) received surgical treatment. A favorable course after endoscopic clip closure was experienced by 17 patients (59%). Five patients had a long hospital stay of 2 weeks or longer, including three patients with abscess formation. The mean hospital stay was 7.7 ± 3.0 days for favorable cases and 28.3 ± 14.4 days for cases with complications.
Four of the patients who required surgery had a simple laparoscopic closure, and three patients had an open laparotomy with colon resection and diversion. The elapsed time from colon perforation to surgery was less than 24 h in four cases, 52 h in one case, 76 h in one case, and 120 h in one case. For all the patients who had early surgery within 24 h, laparoscopic simple closure was possible. However, for the patients whose surgery was delayed more than 48 h, open laparotomy with colon resection and diversion was required due to the development of peritonitis and edema of the colon at the site of perforation. The mean hospital stay was 6.8 ± 0.9 days for the patients with laparoscopic simple closure, whereas the stay was 22, 25, and 120 days for the patients who required colon resection and diversion (Table 1).
Risk factors for consideration of early surgical treatment after colon perforation
Of the 29 patients, 12 (41%) had failed or unfavorable clinical outcomes after endoscopic clip closure including the patients who underwent surgery (seven patients) and those who required a long hospital stay (five patients). After endoscopic clip closure for iatrogenic colon perforation, a decision about surgery should be made as soon as possible to avoid colon resection with diversion and to enable the use of less invasive laparoscopic simple closure procedures where possible. The risk factors for considering early surgical treatment within 24 h after colon perforation were large perforation [odds ratio (OR), 9.25; 95% confidence interval (CI), 1.85–46.20], leukocytosis (OR 6.58; 95% CI 1.86–23.29), fever (OR 5.05; 95% CI 1.05–24.28), severe abdominal pain (OR 4.30; 95% CI 1.17–15.83), and a large amount of peritoneal free air (OR 4.05; 95% CI 1.40–11.71) (Table 2; Fig. 2).

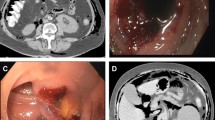
The difference in clinical courses between patients with large and small colon perforations. (A) Endoscopic photograph showing large colon perforation during screen colonoscopy. (B) Initial endoscopic clip repair of perforation site. (C) Chest X-ray showing a large amount of peritoneal free air. The patient experienced complete recovery after early laparoscopic primary repair. (D) Endoscopic photograph showing a small colon perforation during endoscopic submucosal dissection (arrow). (E) Initial endoscopic clip repair for perforation. (F) Chest X-ray showing a small amount of peritoneal free air. The patient experienced complete recovery without surgery
Discussion
Iatrogenic colon perforation is the most feared complication among colonoscopists. Recently, with expansion of the indications for EMR, an endoscopic knife often is used to resect neoplastic lesions of the colon, in addition to the conventional snaring [7, 8]. The frequency of colon perforation has increased with the introduction of ESD for early colon cancer and flat or depressed lesions that cannot be removed properly using conventional snaring [7, 8].
The frequency of colon perforation caused by ESD varies according to the pattern of colonic lesion or the colonoscopist’s skill and is known to be approximately 5% (1.4–10%) [5, 8–11]. In the current study, colon perforation occurred for 8 (0.1%) of 8,275 patients who received EMR using snaring and for 11 (3%) of 348 patients who had lesion removal using endoscopic knives. This shows that the most common cause of colon perforation is the endoscopic knife in advanced therapeutic colonoscopy centers.
The clinical symptoms of iatrogenic colon perforation are variable. Depending on the cause, size, and site of the perforation, the patient may experience no pain, a sudden onset local instantaneous pain only, severe crampy pain, or abdominal distention [12, 13]. If a small perforation occurred by the snaring or the endoscopic knife used in polypectomy, the patient have only local pain or no symptoms. It is important to recognize the presence of perforation during therapeutic colonoscopy [5]. Moreover, a perforation must be distinguished from the so-called “pseudoperforation,” which appears as a localized hole caused by different incision depths within the swollen submucosal layer by use of the endoscopic knife or snaring.
The treatment of a patient with a colon perforation requires rapid assessment of risk and treatment options. Surgical procedures include simple closure, resection with primary anastomosis, and resection with diversion (stoma) based on the presence of colon inflammation, the severity of peritonitis, and the presence of residual lesions. Recently, less invasive laparoscopic surgery is used more frequently than the more traditional open laparotomy approach.
When treatment is delayed after perforation, colon inflammation or peritonitis around the site of perforation may worsen, requiring more invasive surgery and intensive medical management. Thus, a surgical decision should be made as early as possible within 24 h after a colon perforation [14]. For low-risk patients such as those with good colon preparation and a small perforation, medical treatment alone with endoscopic clip closure, fasting, and antibiotics might be adequate [4, 15, 16]. Even if the perforation is larger than 10 mm, it can be sutured using clips from the edge of the perforation. If the endoscopic view or handling of the scope is too difficult for endoscopic clipping of the perforation, a hood or a thin upper endoscope may be preferred.
In this study, the technical success rate for endoscopic clip closure was 91% (29 patients) among the 32 patients with colon perforations. The rates of successful endoscopic clip closure without the need for surgery have increased for patients with iatrogenic colon perforation.
Endoscopic clip closure, however, has its limitations and problems for the treatment of colon perforation. First, complete closure of the perforation site after endoscopic clip closure is difficult to evaluate. If endoscopic clip closure is incomplete or the clips detach early, minor leakage can develop, and this may delay the appearance of the symptoms associated with peritonitis. In such cases, the symptoms may not be clear-cut, and it may be difficult to make a decision about surgery. The surgery may be delayed beyond the optimal period. Three cases in this study had delayed surgery after endoscopic closure, and as a result, aggressive surgical treatment including colon resection with diversion had to be performed.
Second, delayed complications such as peritoneal abscess formation can develop because of extraluminal contaminants or intermittent minor leakage. In this study, peritoneal abscess formation developed in three (50%) of six patients who underwent continuous medical treatment after endoscopic clip closure for a large perforation.
Third, procedure-related adverse events can develop. If the procedure time for endoscopic clip closure is prolonged and the air supply increases, these factors can aggravate abdominal distention and may increase the risk of peritoneal infection.
Fourth, if laparoscopic surgery is performed after endoscopic clipping, laparoscopic closure can interfere with attachment to multiple clips at the perforation site.
Prompt endoscopic clip closure should be considered a noninvasive method that can be used to avoid surgery for patients with iatrogenic colon perforation. In this study, 22 (76%) of the 29 patients were recovered with medical treatment only. However, the five patients who had a long hospital stay of more than 2 weeks included three patients who experienced a peritoneal abscess. For four of the seven patients who underwent surgery after endoscopic clip closure, a simple laparoscopic closure was performed within 24 h after the perforations, and they all were discharged from the hospital within 1 week with no complications. However, the three patients who underwent delayed surgery (after >48 h) had colon resection with diversion. In addition, they had a long hospital stay, and a second reconstruction surgery was required.
The decision to perform surgery should be made promptly within 24 h after colon perforation. The high-risk clinical factors also should be determined within 24 h. The high-risk factors identified in this study included a large perforation (10 mm or larger or perforation by the scope), leukocytosis, fever, severe abdominal pain, and a large volume of peritoneal free gas within 24 h after colon perforation.
In conclusion, the endoscopic clip closure procedure could significantly reduce the frequency of surgery among patients with iatrogenic perforation of the colon. However, an early decision about further surgery after endoscopic clip closure is needed to prevent adverse outcomes for patients at high risk for complications.
References
Anderson ML, Pasha TM, Leighton JA (2000) Endoscopic perforation of the colon: lessons from a 10-year study. Am J Gastroenterol 95:3418–3422
Mana F, De Vogelaere K, Urban D (2001) Iatrogenic perforation of the colon during diagnostic colonoscopy: endoscopic treatment with clips. Gastrointest Endosc 54:258–259
Celestino C, Harz C, Decaestecker J, Saenz R (2006) Endoscopic treatment of an iatrogenic perforation of the colon by using endoloop. Gastrointest Endosc 64:653–654
Gosen C, Poulose B, Trunzo J, Marks J (2009) Endoscopic management of iatrogenic colon perforation during colonoscopy. Am Surg 75:184–186
Panteris V, Haringsma J, Kuipers EJ (2009) Colonoscopy perforation rate, mechanisms, and outcome: from diagnostic to therapeutic colonoscopy. Endoscopy 41:941–951
Kang HY, Kang HW, Kim SG, Kim JS, Park KJ, Jung HC, Song IS (2008) Incidence and management of colonoscopic perforations in Korea. Digestion 78:218–223
Lohsiriwat V, Sujarittanakarn S, Akaraviputh T, Lertakyamanee N, Lohsiriwat D, Kachinthorn U (2009) What are the risk factors of colonoscopic perforation? BMC Gastroenterol 9:71
Tanaka S, Oka S, Kaneko I, Hirata M, Mouri R, Kanao H, Yoshida S, Chayama K (2007) Endoscopic submucosal dissection for colorectal neoplasia: possibility of standardization. Gastrointest Endosc 66:100–107
Yoshida N, Yagi N, Naito Y, Yoshikawa T (2010) Safe procedure in endoscopic submucosal dissection for colorectal tumors focused on preventing complications. World J Gastroenterol 16:1688–1695
Tamegai Y, Saito Y, Masaki N, Hinohara C, Oshima T, Kogure E, Liu Y, Uemura N, Saito K (2007) Endoscopic submucosal dissection: a safe technique for colorectal tumors. Endoscopy 39:418–422
Saito Y, Uraoka T, Matsuda T, Emura F, Ikehara H, Mashimo Y, Kikuchi T, Fu KI, Sano Y, Saito D (2007) Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video). Gastrointest Endosc 66:966–973
Cobb WS, Heniford BT, Sigmon LB, Hasan R, Simms C, Kercher KW, Matthews BD (2004) Colonoscopic perforations: incidence, management, and outcomes. Am Surg 70:750–757
Iqbal CW, Chun YS, Farley DR (2005) Colonoscopic perforations: a retrospective review. J Gastrointest Surg 9:1229–1235
Hansen AJ, Tessier DJ, Anderson ML, Schlinkert RT (2007) Laparoscopic repair of colonoscopic perforations: indications and guidelines. J Gastrointest Surg 11:655–659
Raju GS, Fritscher-Ravens A, Rothstein RI, Swain P, Gelrud A, Ahmed I, Gomez G, Winny M, Sonnanstine T, Bergstrom M, Park PO (2008) Endoscopic closure of colon perforation compared to surgery in a porcine model: a randomized controlled trial (with videos). Gastrointest Endosc 68:324–332
Magdeburg R, Collet P, Post S, Kaehler G (2008) Endoclipping of iatrogenic colonic perforation to avoid surgery. Surg Endosc 22:1500–1504
Acknowledgment
Sung Bum Cho, Wan Sik Lee, Young Eun Joo, Hyeng Rok Kim, Sang Wook Park, Chang Hwan Park, Hyeun Soo Kim, Sung Kyu Choi, and Jong Sun Rew have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cho, S.B., Lee, W.S., Joo, Y.E. et al. Therapeutic options for iatrogenic colon perforation: feasibility of endoscopic clip closure and predictors of the need for early surgery. Surg Endosc 26, 473–479 (2012). https://doi.org/10.1007/s00464-011-1903-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1903-y