
Abstract
Background
In 1999, the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) introduced the SAGES Outcomes Initiative as a method for its members to use for tracking their own outcomes. This report provides a descriptive analysis of the cholecystectomy database.
Methods
The SAGES Outcome Initiative database was accessed for all gallbladder cases from September 1999 to February 2005. The data from the preoperative, intraoperative, and postoperative entries were summarized. These data are purely descriptive, and no statistical analysis was performed.
Results
The gallbladder registry contained 3,285 cases, with 2,005 follow-up cases. Most patients were employed women with some comorbidities who had elective surgery under general anesthesia. Most of the operating surgeons were attending surgeons and surgical assistants. Most of the patients had biliary colic, and symptoms were improved for more than 95% of the patients. More than 90% of the cases were managed laparoscopically, with a conversion rate of 3%. Biliary imaging was used in the vast majority of cases, with most shown to be normal. Intraoperative gallbladder perforation was common, with bile duct injury occurring in 0.25% of cases. The most frequently cited postoperative event was wound infection, with most complications classified as class 1. More than 95% of the patients were able to return to work.
Conclusions
The SAGES Outcomes Initiative database demonstrates that most participating SAGES members perform laparoscopic cholecystectomies themselves using intraoperative cholangiograms. Adverse outcomes are few, with most patients able to return to normal activity. Importantly, there were relatively few missing data points, implying that when surgeons enter data, the information is relatively complete.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Surgeons, as a group, have been leaders in self-assessment of surgical outcomes, especially complications. This is most evident in the time-honored morbidity and mortality conferences that are a mainstay of surgical practice. It was therefore natural for surgeons to develop more formalized methods for tracking outcomes. Among the first of these was the Society of Thoracic Surgeons’ database, initially for cardiac surgery, but currently including other thoracic procedures as well [12]. This particular database has become so influential that Blue Cross/Blue Shield has tied preferred provider inclusion to participation in this database [12].
In 1999, SAGES launched the Outcomes Initiative to provide its members a vehicle for collecting and tracking their outcomes. Previous publications have introduced the database to the membership [7] and have compared its data for antireflux surgery with the National Inpatient Sample [11]. However, neither of the two cited publications have truly reported the breadth of data that the Initiative records. The purpose of this report is to assess the practice patterns of the SAGES members who input cases into the database for gallbladder surgery. By this assessment we hope to improve the collection of data and to determine whether the results are broadly comparable with other published data.
Materials and Methods
The SAGES Outcomes Initiative was established in May 1999 through the SAGES Outcomes Task Force in an effort to provide an outcomes reporting system for its members. Any SAGES member is eligible to register and input case information. Although participation is voluntary, once a member is enrolled, it is expected that all that member’s cases will be recorded in a consecutive manner, and that they will be potentially subject to a data audit. Case information is entered via the Outcomes link through the SAGES Web site (https://ssl-01-002.ssl-service.com/whispercom/00_default.asp). The Web site is managed by Whisper Communications (Whispercom.com, Kingston, WA, USA). The service is free to any SAGES member.
After obtaining a password and stating adherence to the Health Insurance Portability and Accountability Act (HIPAA) rules, enrollees may access the Web site at any time. Preoperative and operative data common to all operations are entered using the Initial Surgical Log form (Fig. 1), and data specific to cholecystectomies are entered using the Initial Gallbladder Log form (Fig. 2).

The initial surgical input form, surgical log.

The initial gallbladder input form.
At the first postoperative visit, the Surgical Follow-Up form (Fig. 3), and the Gallbladder Follow-Up form (Fig. 4) are completed. Each data form was constructed by a panel of experts, beta tested, and then implemented in the database. Complication severity was fashioned after the classification scheme of Clavien et al. [2].

The surgical follow-up form.

The gallbladder follow-up form.
The SAGES gallbladder registry was accessed for all cholecystectomy cases from September 1999 to February 2005. Descriptive statistics for each data point were calculated, including missing or nonsensical data.
Results
A total of 3,285 initial entries with 2,005 follow-up entries were identified in the cholecystectomy database. More than 250 surgeons are registered in the Outcomes Initiative, but approximately 50 surgeons entered the majority of cases in the database. There is no way to determine whether the surgeons were academicians or private practitioners. The mean age ± standard deviation was 49 ± 17 years. There were 2,339 female (72.2%) and 900 male patients. Gender information was missing in 46 cases (1.4%).
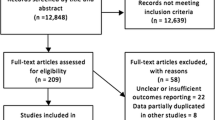
Table 1 presents the data on preoperative work status, American Society of Anesthesiology (ASA) classification, and preoperative comorbidities. Approximately 70% of the patients were employed. More than 80% of the patients were classified as ASA 1 or 2, and more than 70% had at least one comorbidity. Emergency surgery was reported for 465 (14.4%) of 3,240 entries (45 entries were missing, 1.4%). Spinal anesthesia was used for 30 patients, whereas 194 patients had local anesthesia, 3,227 had general anesthesia, and 27 had general with spinal/epidural anesthesia (15 entries were missing). Some patients received more than one type of anesthesia. The average estimated blood loss was 39 ± 91 ml, and the average operating time was 69 ± 40 min. Use of the robot was reported by 194 surgeons (9.2%), whereas 1,906 did not report robot use. Figure 5 presents the distribution of procedure codes reported.

Distribution of primary procedure codes. 47562 = laparoscopic cholecystectomy; 47563 = laparoscopic cholecystectomy with intraoperative cholangiogram; 47564 = laparoscopic cholecystectomy with common bile duct exploration; 47600 = open cholecystectomy; 47605 = open cholecystectomy with intraoperative cholangiogram; 47610 = open cholecystectomy with common bile duct exploration.
Table 2 presents the operating and assistant surgeons. Approximately 70% of the operating surgeons were attending surgeons, whereas more than 50% of the assistants were another attending surgeon. Previous operations were reported for 1,327 patients (42%), whereas 1,848 had no previous surgery (110 entries were missing, 3.3%). Preoperative biliary colic was reported for 2,881 (91.3%) of 3,157 patients, and 2,666 (84.6%) of 3,150 patients had gallstones identified preoperatively.
Table 3 lists the number of disposable instruments used. A mean of two disposable trocars were used per case. The most commonly used were disposable trocars and clip appliers.
Table 4 lists the operations and operative findings. More than 90% of the cases were managed laparoscopically, and the conversion rate was 3.6%. Intraoperative bile duct imaging was performed in 71.1% of the cases.
Table 5 lists the intraoperative events. Spillage of gallstones occurred in more than 25% of the cases, yet the stones were lost in less than 2%. Although bleeding occurred in about 10% of the cases, it resulted in conversion for less than 1%. Pneumoperitoneum was obtained by the open Hasson technique in 1,887 cases, by the Veress needle in 1,104 cases, and by other means in 10 cases (284 entries were missing, 8.6%).
The average follow-up period was 13 ± 9 days. Table 6 lists the postoperative events and complication severity. The most common single postoperative event was the need for postoperative endoscopic retrograde cholangiopancreatography (ERCP). Nearly 90% of the cases did not have a complication, but when complications occurred, they usually were categorized as class 1. Bile duct injury occurred in 8 (0.25%) of 3,182 cases. Readmission was reported in 37 entries (2.1%), but did not occur in 1,724 cases (244 missing, 12,2%). Reoperation was reported in 17 (1%) entries, but did not occur in 1,757 cases (231 missing, 11.5%). Table 7 reports the postoperative symptomatic change and postoperative work status.
Tables 8, 9, and 10 compare the rates for postoperative event occurrence, postoperative symptomatic change, and postoperative work activity by CPT (Current Procedural Terminology) code. These tables show that the laparoscopic approaches generally had fewer complications and faster return to normal activities.
Discussion
Insights from review of these data can be segregated into three categories. First, the quality of the database itself can be assessed. Second, the practice patterns of the SAGES members entering their cases can be elucidated. Third, some broad comparisons can be made, for example, between cases managed laparoscopically and open cases.
The quality of the data appears to be good. All the items chosen for measurement were selected by SAGES surgeons expert in issues involved in gallbladder surgery. Therefore, these items are the patient characteristics, procedure details, and outcomes that matter most to surgeons. Because these are the items that matter most, SAGES members would have an interest in accurately recording these items. In fact, given the number of items that surgeons are asked to record, there are relatively few missing data points. The frequency of missing data points is mostly in the low percentage range, reaching a high of only 12.2%. This low rate of missing data is striking given the richness of the data elements.
In addition, when SAGES members register to input data into the database, they agree to participate in an audit. Nevertheless, to date, audits of individual surgeons have not been conducted. Therefore, we have no independent confirmation of data reliability.
On the other hand, because data are recorded by the surgeon rather than administrative personnel, we can assume that the recorded data actually are the most clinically relevant. The operating surgeon knows exactly the operation performed, the instruments used, the symptomatic outcomes, and the like, which a coder may not believe is important from the standpoint of billing, but which is very important from the standpoint of outcome. For example, when the Outcomes Initiative database was compared with the National Inpatient Sample for antireflux surgery, the complication rates were found to be similar [11].
Another way to assess the “truthfulness” of the data in the registry is to compare it with the data of other population-based studies. For example, Livingston and Rege [9] in reviewing the National Hospital Discharge database found conversion rates of 5% to 10%, whereas the SAGES database reports a conversion rate of 4%. Others have reported bile duct injury rates of 0.25% to 0.5% [5, 10], whereas the SAGES gallbladder registry reports an injury rate of 0.25%. In addition, other findings, such as the rates of acalculus disease and identification of choledocholithiasis, are in keeping with traditionally accepted rates. Therefore, these comparisons are a surrogate for “quality control” of the database.
The practice patterns of the SAGES members contributing to the database were somewhat surprising. First, 94% of the cholecystectomies were completed laparoscopically, with a 4% conversion rate (Table 4). This is despite the fact that surgeons reported difficult dissections in 28% of the cases (Table 5). The attending surgeon was the operating surgeon in nearly 70% of the cases, and interestingly, the assistant surgeon in more than 50% of the cases (Table 2). This implies that most of the entries describe nonteaching cases, although we cannot determine whether these entries were from academic institutions or not. This is somewhat different from the results of a review of the Initiative’s antireflux surgery registry [11]. The patients were what would be considered “typical” gallbladder patients, mostly females in their fifth decade of life, with more than 90% having biliary colic and 85% having gallstones documented preoperatively. This is particularly important because studies using a Medicare administrative database due to the patients recorded in that database have older patients with fewer women [3]. Therefore, the results of those studies may be skewed, because others have shown that cholecystectomy in older patients has more adverse outcomes [1].
Two of the most extensively debated issues in laparoscopic cholecystectomy are bile duct injury and the use of routine intraoperative cholangiograms. It is recognized that laparoscopic cholecystectomy has been associated with higher bile duct injury rates than open cholecystectomy. One of the methods suggested to decrease bile duct injury is the use of the intraoperative cholangiogram [4]. Biliary imaging is reported in the Outcomes Initiative database for 71% of the cases, but was unsuccessful for only 2%. This is a higher rate of intraoperative cholangiography than the 63.7% reported from a population-based study in the state of Washington [5]. The SAGES reported bile duct injury rate is 0.25%. This does show that SAGES members, as a group, more frequently use biliary imaging, and this may be related to the lower bile duct injury rate.
The database can be used to determine the consequences of certain events. For example, whether spillage of gallstones at the time of laparoscopic cholecystectomy causes adverse outcomes or not is still debated [13, 15]. In the gallbladder database, stones reportedly were left in the peritoneal cavity in 1.23% of the cases, yet abscess formation occurred in only 0.15% of the cases. If stone spillage were a more serious issue, we would have expected to see a higher rate of abscess formation. Another example is that 11% of the patients had acalculus gallbladder disease, yet 98% reported marked or somewhat improved symptoms. If acalculus gallbladder disease did not lead to symptoms, then we would expect a lower rate of symptom improvement. This is particularly important in that symptom improvement is the primary motivator of patient satisfaction [6, 8, 14]. However, the problem here may be in the follow-up assessment. With an average follow-up period of about 2 weeks, certainly immediate postoperative complications can be recorded accurately. However, for other outcomes, particularly symptomatic relief, this follow-up period may be too short.
In addition, the Outcomes Initiative database is capable of analyzing “linked” data (e.g., does an association exist between spilled stones and intraabdominal abscesses). However, the database must be interrogated specifically for this purpose.
Although the SAGES and other databases appear useful, databases have general shortcomings. The most significant issue is data accuracy. The SAGES database is recorded by surgeons. Consequently, there may be a bias against the recording of “bad” outcomes. In administrative databases, problems with the data could result from failure to include uninsured persons, turnover of coverage for low income persons, and the recording of only health care that results in a payment claim to the insurer. In addition, because clerical staff records the data, problems in data quality may result from inaccurate coding, incomplete recording of comorbidities, and lacks clinical meaningfulness. Ultimately, the purpose of such databases is not health care or services research, but payment for services rendered. Therefore, databases in general have limitations.
In conclusion, the SAGES Outcomes Initiative database is useful for assessing the practice patterns of SAGES members. Missing data are relatively few, and the data are comparable with other published data on cholecystectomy. Future directions of the Initiative should include increasing participation by SAGES members, confirming the value of the database as a repository SAGES members can use to document their outcomes, and using the database as a benchmarking tool.
References
Brunt LM, Quasebarth MA, Dunnegan DL, Soper NJ (2001) Outcomes analysis of laparoscopic cholecystectomy in the extreme elderly. Surg Endosc 15: 700–705
Clavien PA, Sanabria JR, Strasberg SM (1992) Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 111: 518–526
Flum DR, Cheadle A, Prela C, Dellinger EP, Chan L (2003) Bile duct injury during cholecystectomy and survival in Medicare beneficiaries. JAMA 290: 2168–2173
Flum DR, Flowers C, Veenstra DL (2003) A cost-effectiveness analysis of intraoperative cholangiography in the prevention of bile duct injury during laparoscopic cholecystectomy. J Am Coll Surg 196: 385–393
Flum DR, Koepsell T, Heagerty P, Sinanan M, Dellinger EP (2001) Common bile duct injury during laparoscopic cholecystectomy and the use of intraoperative cholangiography: adverse outcome or preventable error? Arch Surg 136: 1287–1292
Kane RL, Maciejewski M, Finch M (1997) The relationship of patient satisfaction with care and clinical outcomes. Med Care 35: 714–730
Khaitan L, Aprelgren K, Hunter J, Traverso LW (2003) A report on the Society of American Gastrointestinal Endoscopic Surgeons Outcomes Initiative: what have we learned and what is the potential. Surg Endosc 17: 365–370
Lee J, Velanovich V (2003) Factors influencing patients satisfaction after cholecystectomy. Surg Endosc 17: S252
Livingston EH, Rege RV (2004) A nationwide study of conversion from laparoscopic to open cholecystectomy. Am J Surg 188: 205–211
MacFadyen BV Jr, Vecchio R, Ricardo AE, Mathis CR (1998) Bile duct injury after laparoscopic cholecystectomy: the United States experience. Surg Endosc 12: 315–321
Morton JM, Galanko JA, Soper NJ, Hunter J, Traverso LW NIS vs SAGES: a comparison of national and voluntary databases. Surg Endosc, in press
Orringer MB (2001) STS database activities and you: “What’s in it for me?” Ann Thorac Surg 72: 1–2
Sathesh-Kumar T, Saklani AP, Vinayagam R, Blackett RL (2004) Spilled gallstones during laparoscopic cholecystectomy: a review of the literature. Postgrad Med J 80: 77–79
Traverso LW, Lonborg R, Pettingell K, Fenster LF (2000) Utilization of cholecystectomy: a prospective outcome analysis in 1,325 patients. J Gastrointest Surg 4: 1–5
Turner AR, Yuksek YN, Yasti AC, Gozalan U, Kama NA (2005) Dropped gallstones during laparoscopic cholecystectomy: the consequences. World J Surg Mar 22 [Epub ahead of print]
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Velanovich, V., Morton, J.M., McDonald, M. et al. Analysis of the SAGES outcomes initiative cholecystectomy registry. Surg Endosc 20, 43–50 (2006). https://doi.org/10.1007/s00464-005-0378-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0378-0