
Abstract
Background
The assistance received by the surgeon from support personnel during operative laparoscopy is extremely important. This includes retraction of instruments and endoscope positioning. However, human assistance is costly and often does not provide satisfaction for the surgeon. The aim of this study was to develop a mechanical arm capable of allowing easy handling and holding of laparoscopic instruments under the surgeon’s control.
Methods
We designed a system, named Endofreeze, based on a particular kinematical construction that maintains an invariant point of constraint motion just above the trocar puncture site through the abdominal wall. The goal was to develop this way a highly intuitive mechanical holding system for laparoscopic instruments, with sufficient precision of action, activated by a single hand movement. We tested a couple of prototypes with different holding arms while performing cholecystectomy in phantom models with swine inserts and compared the results obtained in similar conditions using different holding and positioning systems.
Results
The system allows transparent and intuitive operation, and its setup is easy and quick. It may be adapted either as an instrument retractor or as an optic positioning device. Compared to different systems available or prototypes previously tested, such as AESOP 2000, ENDOASSIST, FIPS Endoarm, TISKA Endoarm, and the Martin Arm, in similar conditions, it was more intuitive, allowing shorter time for completion of surgery.
Conclusion
Endofreeze is a new intuitive mechanical positioning system for endoscopic solo surgery. In phantom models, it demonstrated a shorter time requirement for completion of surgery when compared to other systems available. In our opinion, it represents a valid compromise between human and robotic control for conventional laparoscopic instruments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In recent years, minimally invasive surgical techniques have improved the quality and efficiency of several operative procedures. Nevertheless, surgeons sometimes face difficulties in reaching a stable and optimal position for laparoscopic instruments and endoscope.
Mechanical retractors and then automated surgical robots were developed alleviate the problem of instrument guidance. Currently, different tasks are performed with the help of mechanical or robotic devices not only in general surgery but also in several other surgical disciplines, such as cardiac surgery, orthopedics, neurosurgery, gynecology, and urology [2, 4, 7-9, 13].
A new instrument positioning system developed by Tuebingen Scientific (Tuebingen, Germany) in cooperation with Aesculap AG & CO. KG (Tuttlingen, Germany) is described. It has a characteristic geometry, which should improve the efficiency of laparoscopic surgical maneuvers.
Materials and methods
Technology
The original idea of Gerhard Buess was to develop a mechanical arm capable of allowing manipulation and fixation of a laparoscopic instrument by the operating surgeon. The geometry of an instrument-guiding system for laparoscopic surgery should respect the principle of the invariant point of motion [10] near the point where the trocar enters the abdominal cavity. For this prototype, called the Tuebingen Ball-Trocar (Tuebingen Scientific), a special kinematical principle was chosen. It establishes a remote center of motion, just above the trocar puncture site, ensuring that minimal lateral force is exerted around it. This was obtained by designing a system in which the shaft of a laparoscopic instrument can be moved around the point of trocar insertion as well as rotated and translated along its longitudinal axis. The mechanism consists of a flexible arm with three different flexible segments to allow positioning of the system in spatial coordinates. For this task, two different options are possible: the Leyla arm (Aesculap), a mechanical arm consisting of multiple segments through which a steal wire is passed for blocking the position of the arm (Fig. 1), and the Unitrac arm (Aesculap), which consists of three different segments connected by spherical joints that are pneumatically fixed with the release or activation of a single ergonomical button on the shaft of the arm (Fig. 2). Both arms are therefore easily displaced in spherical coordinates after being connected by a screwing mechanism to the standard rail of the operating table. Both arms are designed with a standard connection to the system. The system is shaped as a ring that encircles a sphere positioned just below the trumpet mechanism of the trocar along the shaft (Fig. 3 and 4). The arm in position holds the trocar. The friction between the sphere over the trocar and the holding ring can be modified by a screwing mechanism (Fig. 5). The system design was modified by Aesculap, which acquired the patent and markets it under the name Endofreeze. The system conforms to the Medical Device Directive 93/42/EEC.

The Leyla arm, a mechanical arm consisting of multiple segments through which a steal wire is passed to block the position of the arm.

The Unitrac arm, consisting of three different segments connected by spherical joints that are pneumatically fixed.

Endofreeze: The arm is connected to the trocar by a ring that encircles the trocar sphere just below the trumpet mechanism.

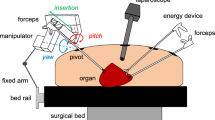
Principle of the Endofreeze system.

Principle of the Endofreeze system and degrees of freedom.
Experimental evaluation
Evaluation of prototypes was performed simultaneously with the technical development of the device. We usually assess new technologies under experimental condition using phantom models with integrated animal organs.
We investigated the feasibility of endoscopic solo surgery by testing different positioning systems. Surgeons skilled in laparoscopic procedures performed five cholecystectomies in combinations of two positioning systems. In a control group, a resident performed the role of the assistant surgeon. As optic positioners, we evaluated the robotic voices-controlled system AESOP 2000 (Computer Motion, Goleta, CA, USA) [11], the robotic helmet-controlled system ENDOASSIST (Armstrong Healthcare, UK) [5], the remoter-controlled system FIPS Endoarm (Nuclear Research Institute, Karlsruhe, Germany) [3], the passive system TISKA Endoarm (Nuclear Research Institute) [12], the Martin Arm (Martin GmbH, Tuttlingen, Germany), and the Endofreeze (Aesculap). In all cases, a TISKA Endoarm was used as an instrument holder, except for the last two groups, in which a second Martin arm and a second Tuebingen Ball-Trocar Arm, respectively, were employed.
All devices were positioned on the right side of the operating table, opposite the surgeon (Fig. 6). Common laparoscopic instruments were used, including a curved grasping forceps designed by Cuschieri, a 30° laparoscope, and the Combination Instrument (Richard Wolf GmbH, Knittlingen, Germany). The experiments took place in the experimental operating theater of the Section for Minimally Invasive Surgery of the University of Tuebingen, Germany. A total of 90 experiments were carried out.

Disposition of instruments and positioning arms around the operating table for lapaoroscopic cholecystectomy.
The procedure time was broken down into segments of time related to different tasks, including setup time for draping the phantom and setting up external devices; positioning time for positioning trocars under vision, connecting devices to their instruments, and positioning the optic; dissection time for performing the complete dissection of the gallbladder; extraction time for extracting the gallbladder; and breakdown time for removing trocars under vision and placing external devices aside.
The statistical analysis was conducted with the Glantz system [6], using analysis of variance (ANOVA), Student’s t test, Kruskal-Wallis test, and Mann-Whitney rank sum tests.
Results
Technological results
Because the Endofreeze system in combination with both arms, Leyla or Unitract, is entirely autoclavable, it can be held directly by the surgeon after preparation of the sterile operating field. The nurse personnel screws the system over the standard rail of the operating table. The surgeon then covers the screwing mechanism with a plastic circle inserted over the shaft of the arm just above the screwing mechanism to ensure sterility of the field. The Endofreeze system is available in 5-10- and 12-mm cannula diameters with 110- or 150-mm lengths. Apart from the additional metal sphere positioned under the valve mechanism, cannulas correspond to conventional products of Aesculap. Therefore, they are used with all different trocars available and require only conventional disinfection and sterilization procedures.
Once inserted, the first trocar of the system is connected to the sphere along the trocar shaft and then rigidified by closing the lever mechanism. The friction of the ring is then fixed by adjustment of its screw.
This geometry allows only movements around the center of the spherical part of the trocar, which lies on the skin surface at the point of incision. Thus, a remote center of motion is established. While the trocar tube and the inserted instrument are moved, they are guided precisely around the invariant point above trocar insertion, with minimal forces exerted to the abdominal wall. Translation and rotation around the longitudinal axis of the instrument are possible and complete the four degrees of freedom necessary to guide the instrument in the abdominal cavity.
Experimental results
The evaluation of the prototype was conducted in phantom models. The overall handling of the system was found to be simple and did not require specific training. The trocar tube can be easily mounted to the instrument-holding device, which is then locked. The friction of the ring around the spherical part of the trocar holds the instrument in place. The friction can be easily adjusted using a screw next to it. A second friction area is obtained by an inner tube at the tip of the trocar. Its adjustment, regulated by a screw, allows the length of insertion of the instrument to be fixed as well as easy handling of the instrument. This was subjectively judged to be very intuitive and easy to perform. It was found to be a particular advantage of the system that repositioning of the instrument can be done with one hand.
During phantom experiments, the principle of the invariant point of constraint motion was confirmed, and the device was found to be atraumatic around the trocar puncture site. Space requirements of the Endofreeze at the operating table are minimal and allow the easy combination of two systems (Fig. 7) for guiding both assisting instrument and laparoscope. For this purpose, both devices should be attached to the operating room table opposite the surgeon to limit conflicts.

Limited space requirements at the operating table allow the easy combination of two systems for guiding both assisting instrument and laparoscope.
All statistical results from tests for interval variables were confirmed by rank tests.ANOVA and the Kruskal-Wallis test showed a significantly variable distribution for all task except for cholangiography time.
The mean global time (Fig. 8), the setup time (Fig. 9), and the breakdown time (Fig. 10) using the Endofreeze were statistically equivalent to those of the control group as well as those obtained using the TISKA Endoarm and Martin Arm. These combinations all scored a mean global time significantly less than that when AESOP, ENDOASSIST, and FIPS Endoarm were employed as optic positioners (p < 0.01). The positioning time (Fig. 11) showed a significant advantage for the control group in comparison with all other groups (p < 0.001). No significant difference was demonstrated in the analysis of extraction time (Fig. 12).

Mean global time for endoscopic cholecystectomy in the phantom model with different combinations of systems.

Setup time for draping the phantom and setting up external devices.

Breakdown time for removing trocars under vision and placing external devices aside.

Time required for positioning trocars under vision, connecting devices to their instruments, and positioning the optic.

Extraction time for the gallbladder.
Use of the Endofreeze resulted in the shortest time for dissection (Fig. 13), although it was statistically significant only versus AESOP (p < 0.01), FIPS Endoarm (p < 0.05), and ENDOASSIST (p < 0.001).

Dissection time for performing the complete dissection of the gallbladder.
Discussion
In recent years, laparoscopic surgery has become increasingly widespread, supported by new developments in the instrumentarium available. Less attention has been paid to the comfort of the first surgeon and his or her assistant, who were often forced into tiring standing positions and to perform monotonous tasks. This can result in an unsatisfactory interaction between the two, making it difficult to find an optimal working position. Moreover, the high costs of the operating theater, even for standard laparoscopic procedures, require the involvement of less experienced fellows, such as residents, leading to further increases in operation time [14]. Especially in community hospitals and private institutions, where the role of the surgical assistant is assumed by either assistant physicians or trained nurses, the introduction of positioning systems for laparoscopic procedures may alleviate some of the pressure due to limited resources.
Mechanically assisted systems, such as Iron Intern (Automated Medical Products, New York, NY, USA) and Omnitract (Minnesota Scientific, St. Paul, MN, USA), reduce costs. On the other hand, they are not ergonomic because they do not offer a true instant release capability to the laparoscope surgeon and are therefore scarcely used. This is mainly a consequence of their original design for open surgery. We were able to confirm these impressions from personal experience on phantom models using retractors originally designed for open surgery. Therefore, we decided to develop a passive positioning system designed to meet the requirements of laparoscopy.
The design of the Endofreeze, based on the principle of mechanical maintenance of the invariant point of motion, allows simple, single-hand operation. According to our personal experience, changing the endoscope or instrument position was intuitive when operating with released instruments. Motions of the abdominal wall (i.e., from the patient’s breathing) have practically no influence on the position of the instrument. The position of the trocar sheath is maintained while the instrument is changed.
Studied mainly as a simple instrument retractor, the Endofreeze is easily used as a passive optical positioning device and simpler than advanced remote-controlled guiding systems. The low space requirements of the system allow it to be combined with further do positioning arms, even on the same side of the patient. This is not always easy to do with other systems. A combination of two Endofreeze systems can be used for both optic and instrument positioning, thus avoiding the need for an assistant surgeon in standard laparoscopic procedures. In phantom experiments, this solo surgery solution appeared to be comfortable for the surgeon.
In this study, we have shown that the best results can be achieved with the combination of mechanical positioning systems, which are the only comparable to human assistance, instead of the higher priced automated systems, such as AESOP and Endoassist, or the prototype FIPS Endoarm. This should be confirmed by an ongoing prospective randomized clinical study. Cost issues favor the use of simple mechanical systems, which are capable of demonstrating a user-friendly design and effectiveness comparable to human assistance.
The Endofreeze represents a valid compromise between human and robotic assistance [1] for laparoscopic instruments. Further data on the influence of positioning systems on the course of endoscopic solo surgery will be obtained from routine use in clinical settings.
References
A Arezzo F Ulmer O Weiss MO Schurr M Hamad GF Buess (2000) ArticleTitleExperimental trial on solo surgery for minimally invasive therapy: comparison of different systems in a phantom model Surgl Endosc 14 955–959 Occurrence Handle10.1007/s004640000106 Occurrence Handle1:STN:280:DC%2BD3M7gvFOqtw%3D%3D
AL Benabid S Lavallee D Hoffmann P Cinquin J Demongeot F Danel (1992) ArticleTitlePotential use of robots in endoscopic neurosurgery Acta Neurochir Suppl 54 93–97 Occurrence Handle1:STN:280:By2B1c%2Fks1E%3D
GF Buess A Arezzo MO Schurr F Ulmer H Fischer L Gumb T Testa C Nobman (2000) ArticleTitleA new remote-controlled endoscope positioning system for endoscopic solo surgery Surg Endosc 14 395–399 Occurrence Handle10.1007/s004640020066 Occurrence Handle1:STN:280:DC%2BD3c3ltlymtQ%3D%3D Occurrence Handle10790562
BL Davies RD Hibberd MJ Coptcoat JE Wickham (1989) ArticleTitleA surgeon robot prostatectomy-a laboratory evaluation J Med Eng Technol 13 273–277 Occurrence Handle1:STN:280:By%2BC3szosVU%3D Occurrence Handle2614807
PA Finlay MH Ornstein (1995) ArticleTitleControlling the movement of a surgical laparoscope IEEE Eng Med Biol 14 289–291 Occurrence Handle10.1109/51.391775
SA Glantz (1996) Primer of Biostatistics, Version 4.0 McGraw-Hill New York
PJ Kelly BA Kail S Goerss F Earnest (1986) ArticleTitleComputer assisted stereotactic laser resection of intra-axial brain neoplasm J Neurosurg 64 427–439 Occurrence Handle1:STN:280:BimC2czgtFA%3D Occurrence Handle3005528
H Koyama T Uchida H Funakubo K Takakura H Fankhauser (1990) ArticleTitleDevelopment of a new microsurgical robot for stereotactic neurosurgery Stereotact Funct Neurosurg 54-55 462–467 Occurrence Handle1:STN:280:By6C1c%2Fltlc%3D Occurrence Handle2080368
FA Matsen JL Garbini JA Sidles B Pratt D Baumgarten R Kaiura (1993) ArticleTitleRobotic assistance in orthopaedic surgery. A proof of principle using distal femoral arthroplasty Clin Orthop 296 178–186 Occurrence Handle8222422
J Mueglitz Kunad P Dautzenberg B Neisius R Trapp (1993) ArticleTitleKinematic problems of manipulators in minimally invasive surgery Endosc Surg Allied Technol 1 160–164 Occurrence Handle1:STN:280:ByuA3s3mtlA%3D Occurrence Handle8055317
JM Sackier Y Wang (1994) ArticleTitleRobotically assisted laparoscopic surgery. From concept to development Surg Endosc 8 63–66 Occurrence Handle1:STN:280:ByuB3cvptFA%3D Occurrence Handle8153867
MO Schurr A Arezzo B Neisius HH Rininsland HU Hilzinger J Dorn K Roth GF Buess (1999) ArticleTitleTrocar and instrument positioning system TISKA: an assist device for endoscopic solo-surgery Surg Endosc 13 528–531 Occurrence Handle10.1007/s004649901029 Occurrence Handle1:STN:280:DyaK1M3ksVOltg%3D%3D Occurrence Handle10227959
KS Taylor (1993) ArticleTitleRobodoc: study tests robot’s use in hip surgery Hospitals 67 46 Occurrence Handle1:STN:280:ByyB3sbhsFA%3D
LW Traverse KP Koo K Hargrave et al. (1997) ArticleTitleStandardizing laparoscopic procedure time and determining the effect of patient age/gender or absence of surgical residents during operations Surg Endosc 11 226–229 Occurrence Handle10.1007/s004649900331 Occurrence Handle9079597
Acknowledgments
We thank Dr. Theodor Lutze and Dr. Dieter Weisshaupt of Aesculap AG & CO. KG (Tuttlingen, Germany) for their support in the development of the Endofreeze system.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arezzo, A., Schurr, M.O., Braun, A. et al. Experimental assessment of a new mechanical endoscopic solosurgery system: Endofreeze. Surg Endosc 19, 581–588 (2005). https://doi.org/10.1007/s00464-003-9132-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-003-9132-7