
Abstract
Purpose
A surgeon in a sterilized area can perform robotically assisted laparoscopic solo surgery while controlling a laparoscope-holding robot for view stabilization and a forceps robot for pulling organs. At present, no locally operated surgical assistant manipulator with a mechanical remote center of motion (RCM) is available to operate within a small space while providing a wide range of movement. The present study describes a new locally operated detachable end-effector manipulator (LODEM) with diagonal joints and multi-stage telescopic screws.
Methods
A forceps manipulator attached to commercial surgical forceps was developed. This manipulator uses RCM diagonal joints for the yaw and pitch axes, providing an intuitive pivot point and free rotation, and telescopic nested screws with multiple sliders clamp the commercial forceps for the axis of insertion. The manipulator placed above the abdominal wall using a fixed arm connected to a bed rail is motor controlled by a handheld interface with button switches for precise traction and is controlled manually for easy rough positioning.
Results
Positional accuracy at the tip with a load of 5 N was under 0.5 mm. Mechanical deflection was under 2.1 mm. The manually controlled force was under 4.4 N. Successful simulated laparoscopic cholecystectomy using the prototype manipulator to handle the target and maintain stability was performed on a surgically realistic gallbladder model.
Conclusions
A LODEM with diagonal joints and multi-stage telescopic screws was developed to facilitate minimally invasive, robotically assisted laparoscopic solo surgery by a surgeon working near the patient. This electric motor-controlled laparoscopic instrument holder by the surgeon in the surgical field could be used for such applications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Background
Laparoscopic surgery producing only small scars has become widespread as a standard of care in developed countries [1]. Minimally invasive surgery offers substantial benefits to both patients and doctors. Meanwhile, the need for surgery in low- and middle-income countries continues to rise [2]. In order to become a doctor, time and money are needed. In Malawi which is one of the least developed countries, the enrollment rate in higher education is low, and the financial cost of training a medical doctor is over US$ 50,000 [3]. More training time and financial costs for making a surgeon are required after medical school education. The introduction of low-cost surgical assistant robots will give the time to grow up skilled surgeons. Robotically assisted laparoscopic surgery using locally operated assistant manipulators in a sterilized area represents one potential solution. By integrating surgical assistant robots, the surgeon can perform robotically assisted laparoscopic solo surgery while controlling a laparoscope-holding robot for view stabilization and a forceps robot for pulling organs. Solo surgery offers new opportunities for hospitals in reducing the numbers of surgeons present in the operating room (OR).
Collaboration between the surgeon and surgical assistant robots during the surgery is important. The surgeon therefore needs to be provided intuitive pivot manipulation and a wide working area on the abdominal wall. Hence, the robot requires a suitable mechanical remote center of motion (RCM), should occupy a small space, and should be set up with the capacity for a wide range of movement.
State of the art
Tele-operated surgical robots with a camera arm and two or three tool arms [4], such as the da Vinci [5], IBIS [6], Senhance [7] (formerly known as ALF-X [8]), Versius [9], Avatera [10], and Hinotori [11], have been developed for a surgeon as a high-end tool to resolve problems such as limited degrees of freedom (DOFs), minimization of the effects of any hand tremors, and cooperation with assistants. Locally operated surgical assistant robots are intended to assist with the surgical workflow solely in laparoscopy. Laparoscope-holding assistant robots, such as the ViKY [12] (formerly known as LER [13]), FreeHand [14], EMARO [15], and SOLOASSIST II [16], have been developed for view stabilization [17]. Forceps assistant robots, such as the ANSUR [18] and the locally operated detachable end-effector manipulator (LODEM) with a commercial surgical forceps [19,20,21,22,23,24], have been developed for soft tissue retraction. These manipulators are categorized into three types, as follows.
Parallel link manipulators such as da Vinci [5], IBIS [6], and EMARO [15], and slider-crank or gimbal-mount LODEM [20, 24] with a mechanical RCM provide intuitive pivot manipulation, but the mechanisms occupy a large space above the abdominal wall and the range of movement is narrow when close to the horizontal position because of the linkages.
R-guided rail manipulators such as Viky [12] and FreeHand [14], and circular telescopic or ring-guided LODEM [21, 23] with a mechanical RCM provide intuitive pivot manipulation and a wide range of movement compared to parallel link manipulators, but the mechanism covers a large, hemispherical space on the abdominal wall.
Serial link manipulators such as Versius [9], Avatera [10], Hinotori [11] and SOLOASSIST II [16] with a motor-controlled RCM provide a wide range of movements, but the pivot manipulation is difficult to understand intuitively and the mechanism occupies a large space above the abdominal wall because of the thick arm. Cylindrical manipulators such as Senhance [7], ANSUR [18], and the SCARA LODEM [19] are also classified as serial link manipulators.
Purpose
At present, no locally operated surgical assistant manipulator offers a mechanical RCM that can operate within a small space while providing a wide range of movement on the abdominal wall. We therefore propose herein a new 3-DOFs forceps manipulator with diagonal joints and multi-stage telescopic screws attached to commercial surgical forceps for robotically assisted laparoscopic surgery performed by a single surgeon.
We have previously reported an overview of the proposed mechanism [25]. The present study describes the newly proposed manipulator with diagonal joints for mechanical RCM and a wide range of potential movements, and multi-stage telescopic screws for the small space. In addition, we report in detail the performance of the proposed manipulator in a simulated laparoscopic solo surgery.
Materials and methods
Concept of robotically assisted laparoscopic surgery with a forceps assistant manipulator
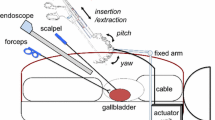
Figure 1 shows a conceptual diagram of robotically assisted laparoscopic surgery performed by a single surgeon. A laparoscope, forceps attached to an assistant manipulator, and two conventional tools operated by the surgeon hands are inserted into the abdomen through ports to remove a target organ, such as a gallbladder. The forceps assistant manipulator connected to a bed rail is placed above the abdominal wall. The manipulator has three DOFs (yaw, pitch, and insertion) and is controlled manually for easy rough positioning and is motor controlled for precise traction. The attached forceps, which have two DOFs (roll and grasp), are controlled manually to grasp the organ. The surgeon can perform robotically assisted laparoscopic surgery while controlling the forceps robot for pulling organs continuously. The manipulator draped with a sterile cover can be removed from the surgical table as required.

Concept of robotically assisted laparoscopic surgery supported by a forceps assistant manipulator
Design and prototype
We propose a new 3-DOFs forceps manipulator with diagonal joints and telescopic multiple screws using multiple sliders attached to commercial surgical forceps. Figure 2a and b shows the mechanical design of the diagonal joints for the yaw and pitch axes, and telescopic multiple screws using multiple sliders for the insertion axis. The gap of 88 mm between the diagonal joints and the pivot is determined from the thickness of a commercial trocar head (50 mm). The yaw axis is set at a diagonal angle of 30° on the horizontal plane and the pitch axis is also set at a diagonal angle of 45°. The motor for the pitch axis is embedded in the diagonal arm using a bevel gear. RCM diagonal joints can produce free rotation to avoid collision with the mechanism for the insertion axis.

Mechanical design of the forceps manipulator with diagonal joints for the yaw and pitch axes, and multi-stage telescopic screws for the insertion axis: a front perspective view; b side perspective view; c telescopic mechanism using three screws and three sliders; and d) nested construction with screws
Figure 2c and d shows the details for the mechanical design of the insertion axis. The telescopic mechanism consists of three screws, three sliders, and a constant force spring. These three screws show a nested construction with screw 3 (length: 130 mm; outer diameter: 16 mm; inner diameter: M12; lead length: 1 mm), screw 2 (length: 130 mm; outer diameter: M12; lead length: 1 mm; inner diameter: M8; lead length: 1 mm), and screw 1 (length: 136 mm; outer diameter: M8; lead length: 1 mm). Three sliders connected to the nested screws are used for linear motion guides. The constant force spring (output force: 5.88 N, CR-5; Accurate, Koshigaya, Japan) is used for precompression in the short direction. The motor of the insertion axis is connected to screw 3 using a spur gear. Commercial surgical forceps (5 mm in diameter, ENDO CLINCH II; Medtronic, Dublin, Ireland) can be clamped using an attachment screw on the outer slider draped with the sterile cover. Manual control of the insertion axis is performed by rolling the motor-coupling part.
The manipulator is motor driven after manual positioning in the initial orientation. The operating range is − 90° to 30° for the yaw axis, -60° to 90° for the pitch axis, and 0 to 200 mm for the insertion axis as shown in Fig. 3a–c, decided on the basis of the pulling direction by the assistant’s forceps [26]. The requirements for the tip of the forceps are 5 N of applied force [27], velocity of 100 mm/s [28], and accuracy of 0.5 mm [20].

Operating ranges of the forceps manipulator: a yaw axis; b pitch axis; and c insertion axis
Figure 4a and b shows photographs of a prototype forceps manipulator. Each of the yaw and pitch axes is driven by a direct current (DC) servomotor (maximum continuous torque, 0.0304 Nm; efficiency, 0.88; maximum speed, 9690 rpm; RE25 339,152; Maxon Motor, Sachseln, Switzerland) with a planetary gear head (gear ratio: 139, efficiency: 0.70, GP26A406770; Maxon Motor) and an encoder (resolution: 500 pulse; HEDL5540 110,512; Maxon Motor). The insertion axis is driven by the same DC motor with a planetary gear (gear ratio: 27; GP 26A406764; Maxon Motor) and the same encoder. The main materials are duralumin for the diagonal arm, brass for the telescopic screws, and stainless steel for gears and sliders. The dimensions of the manipulator are 360 mm × 220 mm × 170 mm. The mass is 2.1 kg. The manipulator is motor controlled by a handheld interface (70 mm × 50 mm; 35 g) with button switches as shown in Fig. 4c. Commands to control the individual axes are input by pressing the appropriate buttons, and these commands are processed by a positioning controller (EPOS2 24/2 DCX, 530,239; Maxon Motor), which then outputs the appropriate signals to the manipulator.

Prototype of the forceps manipulator: a front perspective view; b side view; and c handheld interface with button switches
Experimental methods
To evaluate the new manipulator, the prototype was used in the experiments as described below. Experiments 1 and 2 were performed to confirm positional accuracy of the motion trajectory and the manually controlled force. Experiment 3 was designed to confirm the feasibility of using the manipulator as a surgeon’s assistant in simulated laparoscopic surgery.
-
1.
Independent motion trajectories of the prototype with a stainless steel rod (outer diameter: 5 mm; length: 300 mm; weight: 50 g) as the surgical tool for the three axes when loaded by 0 N and 5 N at the tip of the bar were measured using an optical displacement sensor (accuracy: 0.1 mm; OPTOTRAK Certus; NDI, Waterloo, Canada). The length from the pivot to the tip of the bar was 200 mm. The sensor marker measuring the trajectory was attached to the mechanism where the length from the pivot was 218 mm. In these experiments, positional accuracy at the tip of the bar was defined as the maximum difference in hysteresis under a load of 5 N. Mechanical deflection was defined as the maximum difference in motion trajectory between 0 N and under a load of 5 N.
-
2.
The independent, manually controlled force of the unpowered prototype with the stainless steel rod for the three axes was measured using a force gauge (resolution: 0.01 N; ZP-50 N; IMADA, Toyohashi, Japan). Length from the pivot to the tip of the bar was 200 mm. The measuring point was at the tip of the bar in an orthogonal direction for the yaw and pitch axes, and at the motor coupling (outer diameter: 14 mm) in the tangential direction for the insertion axis. Manually controlled force was defined as the averaged static force at the initiation of movement in five trials.
-
3.
Simulated laparoscopic cholecystectomy was performed on a surgically realistic gallbladder model (50,128; Limbs and Things, Bristol, UK) in a training box (Endowork-pro II; KARL STORZ, Tuttlingen, German) by a specialist. A laparoscope (diameter: 10 mm; Tricam 3D; KARL STORZ) was positioned on the foot side of the surgical table using an autoclavable fixed arm (OCT-03L; Yufu Itonaga, Osaka, Japan) connected to the bed rail. Forceps attached to the manipulator were positioned on the left-hand side of the table using an autoclavable fixed arm (Snowden Pencer Fast Clamp System; CareFusion 2200, San Diego, CA) connected to the bed rail. The operator, a laparoscope specialist, stood at the foot side of the table and used scissors in his right hand and forceps in the left hand. The manipulator was controlled by a handheld interface with button switches. The experimental setup is shown in Fig. 5.

Experimental setup for simulated laparoscopic cholecystectomy using the prototype forceps manipulator
In clinical laparoscopic cholecystectomy, the surgeon dissects the gallbladder using scissors or an electric scalpel under sufficient tension produced by his forceps and the assistant’s forceps. The assistant is needed to keep the lower edge of the liver elevated to allow a perfect view on the gallbladder. The role of the proposed forceps manipulator as the assistant in the simulated surgery was determined to pull up and hold the organ model continuously during dissection. The simulated surgery was started at grasping the organ and ended at completing the dissection. Manual control time, on/off switch control time, and holding the organ time using the prototype forceps manipulator were measured using a video camera filming of a laparoscopic monitor, the experimental setup on the surgical bed, and the laparoscope specialist. This physician had experience using some forceps assistant manipulators with different mechanisms although the controllers of button switches were similar in shape [20, 21, 23, 24]. The specialist had training with the new manipulator before the experiment for a few minutes. The on/off switch controller and the gallbladder model were familiar to the surgeon, however, the manual control and the motor control for the proposed manipulator were the first time in the simulated surgery.
Results
Results of the three experiments were as follows.
-
1.
Figure 6 presents the results of trajectory measurements in the moving direction under loads of 0 N and 5 N. Positional accuracy at the tip of the bar was 0.5 mm for the yaw axis (Fig. 6a), 0.4 mm for the pitch axis (Fig. 6b), and 0.4 mm for the insertion axis (Fig. 6c). Mechanical deflection was 2.1 mm for the yaw axis, 1.1 mm for the pitch axis, and 0.5 mm for the insertion axis.
-
2.
Manually controlled force at the tip of the bar was 4.3 N for the yaw axis, 1.8 N for the pitch axis, and 4.4 N for the insertion axis.
-
3.
Figure 7 shows a photograph of the simulated laparoscopic cholecystectomy. Manipulator angle was changed manually to grasp and pull the gallbladder model so as to perform the simulated laparoscopic cholecystectomy. The forceps manipulator was then driven by the motors under the control of the surgeon and retracted the organ model continuously. The organ model could be pulled in various desired directions using the forceps attached to the manipulator. The forceps held in the left hand could also be used to grasp and pull the model organ in the opposite direction with sufficient tension, while the scissors held in the right hand could be used to dissect the organ model. Smooth dissection of the organ model was performed by the laparoscope specialist at sigh. Successful simulated laparoscopic surgery was performed for 15 min 30 s, as shown in Fig. 8. Detailed durations were 1 min 9 s for manual control, 4 min 4 s for the on/off switch control, 9 min 23 s for holding organs in operations using the surgeon’s hands, and 54 s for forceps replacement. Even though accidental forceps replacement was occurred, a few manual controls to change the operative field, and a dozen of on/off switch controls to maintain the tension for the organ model were performed.

Results of trajectory measurements of the forceps attachment in the direction of movement when loaded by 0 N or 5 N: a yaw axis; b pitch axis; and c insertion axis

Simulated laparoscopic cholecystectomy performed on a surgically realistic gallbladder model in a training box by a laparoscope specialist using the prototype forceps manipulator

Results of time measurements for simulated laparoscopic cholecystectomy by the laparoscope specialist using the forceps manipulator prototype in situations categorized as 1–4: 1 manual control; 2 on/off switch control; 3 holding organ; and 4 forceps attachment
Discussion
The forceps manipulator with diagonal joints and multi-stage telescopic screws was developed to keep the mechanical RCM within a small space while providing a wide range of movement. The diagonal joints in the pitch and yaw axes can produce a mechanical pivot point on the abdominal wall for intuitive manipulation similar to parallel linkage [5, 6, 15] and R-guided rail [12, 14] manipulators and can also produce a wide range of movement comparable to that with serial link manipulators [7, 9, 11, 16, 18] in principle when the arm does not collide with the insertion axis. The multi-stage telescopic screws of the insertion axis occupy a small space when shortened.
The direct rotational pitch axis, the bevel-geared rotational yaw axis, and the screwed linear insertion axis lead to the required positional accuracy because of a few air gaps and backlash. The multiple sliders and constant-force spring of the insertion axis lead to suppression of mechanical deflection because of the closed loop mechanism and precompression. Mechanical deflection for the yaw and pitch axes of the diagonal joints can be reduced once processing and assembly accuracy are improved.
Positional accuracy under 0.5 mm and manually controlled force under 5 N contributed to precise traction and easy rough positioning for target organ as the surgical assistant in the simulated surgery. The new forceps assistant manipulator could be used by the laparoscope specialist to successfully handle the target organ model. The intuitive pivot manipulation, wide working area on the abdominal wall, and quick and accurate provision of the required surgical scenes for the surgeon were confirmed in a dry laboratory environment. Robotically assisted laparoscopic solo surgery produced by a doctor working near the patient while controlling the forceps manipulator was also confirmed. According to comparison of different laparoscope robots in a gallbladder phantom model [29], dissection time using early robots such as AESOP and FIPS was between 13 and 18 min, while a control group involving an assistant surgeon was 16 min. Although a simple comparison is not accurate, the simulated surgery for 15 min in this study equal to the result using the former gimbal-mount LODEM [24] indicates that the proposed forceps manipulator could be pulling and holding the gallbladder continuously as the assistant.
The pitch and yaw axes of the manipulator are not perpendicular. The perpendicular gimbal coordinate is more intuitive in general, but the specialist could smoothly control the manipulator with oblique coordination. The reason for this smooth control is that the surgeon estimates the pulling force and direction from the surface of the organ in the laparoscope monitor. A forceps assistant manipulator is important to facilitate collaboration with the surgeon during robotically assisted surgery.
The interface for controlling the manipulator is important. The proposed manipulator for the present system is controlled by a handheld button switch. Laparoscope assistant manipulators can be controlled by interfaces such as handheld switches [16], head-mounted sensors [14, 15], and vocal commands [12]. In the meantime, tele-operated surgical robots represent a master-follower system. Movement of the master device is similar to that in conventional open or laparoscopic surgery, so the surgeon can operate intuitively. A hybrid controller with easy on/off switching and intuitive master-follower movement appears suitable for the assistant manipulator. A master-follower selectable control system enables control devices to be exchanged easily [30].
Many types of laparoscope or forceps fixed arms, such as mechanical type using experiments in this study, pneumatic type [31], hydraulic type, and spring type [32] have been developed. The passive instrument holder requires handling and fixation repeatedly when the tension of organs come loose, for example elevating the gall bladder. The surgeon is difficult to concentrate the laparoscopic monitor while controlling the passive holder manually on the surgical bed, whereas the surgeon can perform pulling organs with focusing the monitor while controlling the proposed motor driven active holder. However, additional electronic devices in OR lead to more electric wiring and maintenance time for surgical operations.
Solo thee-incision laparoscopic cholecystectomy using the laparoscope holder is performed to overcome an inexperienced scopist or a shortage of skilled manpower [33]. The solo laparoscopic surgery using active holders with the laparoscope and the forceps could be used for other surgical procedures. Expansion into other surgeries using the proposed forceps manipulator is under consideration. The proposed system has a potential to be used for benign diseases, such as appendectomy, inguinal hernia repair, uterine myomectomy, or nephrectomy. For operations in humans, downsize mechanism made of stainless material and attachments applied to commercial forceps are needed. Furthermore, two or more assistant manipulators are used for complex procedures. As to the installation of the robot with light weight separately, connection to the surgical bed rail is suitable [9, 12, 14, 16]. The easy fixed arm for the assistant robot is needed. Future work includes also improvements of simulated surgery. The experimental environment using a surgical gallbladder model in this study is limited. The use of a liver model covering the gallbladder model is one of the improvement simulated surgery to produce holding the liver up to create tension for the dissection from above.
Tele-operated robotic surgical systems have high fixed costs, with prices ranging from US$ 1 million to US$ 2.5 million [34]. Laparoscope-holding assistant robots have relatively low costs, with prices about US$ 100,000 [35]. Further simple structured assistant robot leads to lower cost and the robotic assisted solo surgery using assistant robots would be feasible for low- and middle-income countries.
Conclusions
We developed a 3-DOFs forceps manipulator with diagonal joints and multi-stage telescopic screws attached to commercial surgical forceps for laparoscopic surgery performed by a single surgeon. The mechanism of diagonal joints and multi-stage telescopic screws, providing the mechanical RCM within a small space while offering a wide range of movement, was designed to facilitate minimally invasive, robotically assisted laparoscopic solo surgery by a doctor working near the patient. The present results indicate that the proposed manipulator may be feasible for use in such applications.
References
Jensen KK, Andersen P, Erichsen R, Scheike T, Iversen L, Krarup P (2016) Decreased risk of surgery for small bowel obstruction after laparoscopic colon cancer surgery compared with open surgery: a nationwide cohort study. Surg Endosc 30(12):5572–5582. https://doi.org/10.1007/s00464-016-4930-x
Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA, Bickler SW, Conteh L, Dare AJ, Davies J, Mérisier ED, El-Halabi S, Farmer PE, Gawande A, Gillies R, Greenberg SLM, Grimes CE, Gruen RL, Ismail EA, Kamara TB, Lavy C, Lundeg G, Mkandawire NC, Raykar NP, Riesel JN, Rodas E, Rose J, Roy N, Shrime MG, Sullivan R, Verguet S, Watters D, Weiser TG, Wilson IH, Yamey G, Yip W (2015) Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 386(9993):569–624. https://doi.org/10.1016/S0140-6736(15)60160-X
Muula AS, Panulo B Jr (2007) Lost investment returns from the migration of medical doctors from Malawi. Tanzan Health Res Bull 9(1):61–64. https://doi.org/10.4314/thrb.v9i1.14295
Taylor RH, Menciassi A, Fichtinger G, Fiorini P, Dario P (2016) Medical robotics and computer-integrated Surgery. In: Siciliano B, Khatib O (eds) Springer handbook of robotics. Springer, Cham, pp 1657–1684
Guthart GS, Salisbury JJ (2000) The intuitive telesurgery system: overview and application. In: Proceedings of IEEE ICRA, pp 618–621. https://doi.org/10.1109/ROBOT.2000.844121
Tadano K, Kawashima K (2010) Development of a master–slave system with force-sensing abilities using pneumatic actuators for laparoscopic surgery. Adv Robot 24(12):1763–1783. https://doi.org/10.1163/016918610X522559
Stephan D, Sälzer H, Willeke F (2018) First experiences with the New Senhance® Telerobotic system in visceral surgery. Visc Med 34(1):31–36. https://doi.org/10.1159/000486111
Gidaro S, Buscarini M, Ruiz E, Stark M, Labruzzo A (2012) Telelap Alf-X: a novel telesurgical system for the 21st century. Surg Technol Int 22:20–25
Atallah S, Parra-Davila E, Melani AGF (2019) Assessment of the Versius surgical robotic system for dual-field synchronous transanal total mesorectal excision (taTME) in a preclinical model: Will tomorrow’s surgical robots promise newfound options? Tech Coloproctol 23:471–477. https://doi.org/10.1007/s10151-019-01992-1
Rassweiler JJ, Autorino R, Klein J, Mottrie A, Goezen AS, Stolzenburg JU, Rha KH, Schurr M, Kaouk J, Patel V, Dasgupta P, Liatsikos E (2017) Future of robotic surgery in urology. BJU Int 120(6):822–841. https://doi.org/10.1111/bju.13851
Kikuchi K, Suda K, Shibasaki S, Tanaka T, Uyama I (2021) Challenges in improving the minimal invasiveness of the surgical treatment for gastric cancer using robotic technology. Ann Gastroenterol Surg 00:1–10. https://doi.org/10.1002/ags3.12463
Gumbs AA, Crovari F, Vidal C, Henri P, Gayet B (2007) Modified robotic lightweight endoscope (ViKY) validation in vivo in a porcine model. Surg Innov 14(4):261–264. https://doi.org/10.1177/1553350607310281
Long JA, Cinquin P, Troccaz J, Voros S, Berkelman P, Descotes JL, Letoublon C, Rambeaud JJ (2007) Development of miniaturized light endoscope-holder robot for laparoscopic surgery. J Endourol 21(8):911–914. https://doi.org/10.1089/end.2006.0328
Stolzenburg JU, Franz T, Kallidonis P, Minh D, Dietel A, Hicks J, Nicolaus M, Al-Aown A, Liatsikos E (2010) Comparison of the FreeHand robotic camera holder with human assistants during endoscopic extraperitoneal radical prostatectomy. BJU Int 107(6):970–974. https://doi.org/10.1111/j.1464-410X.2010.09656.x
Tadano K, Kawashima K (2014) A pneumatic laparoscope holder controlled by head movement. Int J Med Robot 11(3):331–340. https://doi.org/10.1002/rcs.1606
Gillen S, Pletzer B, Heiligensetzer A, Wolf P, Kleeff J, Feussner H, Fürst A (2014) Solo-surgical laparoscopic cholecystectomy with a joystick-guided camera device: a case–control study. Surg Endosc 28(1):164–170. https://doi.org/10.1007/s00464-013-3142-x
Bihlmaier A (2016) Endoscope robots and automated camera guidance. In: Learning dynamic spatial relations. Springer, Wiesbaden, pp 23–71. https://doi.org/10.1007/978-3-658-14914-7
A-traction Inc. https://www.a-traction.co.jp/. Accessed 1 July 2021
Kawai T, Hashida J, Myongsyu S, Nishizawa Y, Nakamura T, Morita N, Murotani T, Mochizuki S (2012) Locally operated detachable end-effector manipulator for endoscopic surgery. JJSCAS 14(1):5–14. https://doi.org/10.5759/jscas.14.5
Kawai T, ShinM NY, Horise Y, Nisihkawa A, Nakamura T (2015) Mobile locally operated detachable end-effector manipulator for endoscopic surgery. Int J CARS 10(2):161–169. https://doi.org/10.1007/s11548-014-1062-4
Kawai T, Hayashi H, Nishizawa Y, Nishikawa A, Nakamura R, Kawahira H, Ito M, Nakamura T (2017) Compact forceps manipulator with a spherical-coordinate linear and circular telescopic rail mechanism for endoscopic surgery. Int J CARS 12(8):1345–1353. https://doi.org/10.1007/s11548-017-1595-4
Kawai T, Matsumoto T, Nishikawa A, Nishizawa Y, Nakamura T (2016) Bending forceps manipulator with offset distance for single-port laparoscopy. ABE 5:56–62
Sasaki A, Amemori H, Kawai T, Nishikawa A, Nishizawa Y, Nakamura T (2019) Forceps manipulator with circular ring guided rail and linear guide roller for laparoscopic surgery. In: Proceedings of EMBC: FrPOS-36.31
Han S, Kawai T, Nishikawa A, Nishizawa Y, Nakamura T (2020) Portable forceps manipulator with closed loop mechanism using gimbal-mounted parallel linkage for endoscopic surgery. JJSCAS 22(1):5–13. https://doi.org/10.5759/jscas.22.5
Sasaki A, Kawai T, Nishikawa A, Nishizawa Y, Nakamura T (2020) Forceps manipulator with diagonal joints and telescopic multi screws for laparoscopic surgery. In Proceedings of ACCAS, pp 94–95
Sasaki A, Kawai T, Nishizawa Y, Ikeda K, Tsukada Y, Sasaki T, Ito M (2020) Measurement of pulling direction and holding time for assistant’s forceps in laparoscopic colorectal surgery. In Proceedings of JSES: OS43–3
Visser H, Hijnsdijk EAM, Herder JL, Pistecky PV (2002) Forces and displacements in colon surgery. Surg Endosc 16(10):1426–1430. https://doi.org/10.1007/s00464-002-9003-7
Mitsuishi M, Sugita N, Yasunaka S, Hashizume M (2008) Design of a surgical robot for use inside the human body. JRSJ 26(3):242–246. https://doi.org/10.7210/jrsj.26.242
Arezzo A, Ulmer F, Weiss O, Schurr MO, Hamad M, Buess GF (2000) Experimental trial on solo surgery for minimally invasive therapy: comparison of different systems in a phantom model. Surg Endosc 14(10):955–959. https://doi.org/10.1007/s004640000106
Fukui S, Kawai T, Nishizawa Y, Nishikawa A, Nakamura T, Iwamoto N, Horise Y, Msamune K (2021) Locally operated assistant manipulators with selectable connection system for robotically assisted laparoscopic solo surgery. Int J CARS 16(4):683–693. https://doi.org/10.1007/s11548-021-02338-9
Mamelak AN, Danielpour M, Black KL, Hagike M, Berci G (2008) A high-definition exoscope system for neurosurgery and other microsurgical disciplines: preliminary report. Surg Innov 15(1):38–46. https://doi.org/10.1177/1553350608315954
Bosma J, Boeken Kruger A, Jaspers J (2015) A novel, intuitive instrument positioner for endoscopy, involving surgeons in design and feasibility. Minim Invasive Ther Allied Technol 24(6):326–333. https://doi.org/10.3109/13645706.2015.1039547
Choi S, Choi Y, Han H, Yoon Y, Cho JY, Kwon S, Jang JS, Choi J, Kim S (2016) Solo three-incision laparoscopic cholecystectomy using a laparoscopic scope holder for acute cholecystitis. J Minim Invasive Surg 19:141–147. https://doi.org/10.7602/jmis.2016.19.4.141
Barbash GI, Glied SA (2010) New technology and health care costs–the case of robot-assisted surgery. N Engl J Med 363(8):701–704. https://doi.org/10.1056/nejmp1006602
Wagner AA, Varkarakis IM, Link RE, Sullivan W, Su LM (2006) Comparison of surgical performance during laparoscopic radical prostatectomy of two robotic camera holders, EndoAssist and AESOP: a pilot study. Urology 68(1):70–74. https://doi.org/10.1016/j.urology.2006.02.003
Funding
The present study was supported in part by Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Numbers 21K03986.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest with regard to this study.
Ethical approval
This article does not describe any studies with human or animal subjects.
Informed consent
This article does not contain patient data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 1139 kb)
Rights and permissions
About this article

Cite this article
Sasaki, A., Kawai, T., Nishizawa, Y. et al. Surgical assistant manipulator with diagonal joints and multi-stage telescopic screws for laparoscopic solo surgery. Int J CARS 17, 487–495 (2022). https://doi.org/10.1007/s11548-021-02553-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11548-021-02553-4