
Abstract
The viscosity of nonsolid foods and the stability of their viscosity over time is critical in managing dysphagia. The time-dependent viscosity of liquids thickened with starch-based thickeners was measured at constant temperature and shear rate. Viscosity was measured between 30-min intervals of rest (zero shear) over a period of 17 h at 20.0°C. Two common types of thickeners were evaluated: maize-based and maltodextrin-based (the latter commonly used in pediatrics). The maize-based thickeners undergo a significant decrease in viscosity over the initial 1–4 h following preparation. The maltodextrin-based thickener’s viscosity increases significantly 30 min following preparation and is then more stable over time than its maize-based equivalent. These findings suggest that the success of current dysphagia therapies that use thickeners could be influenced by the time-dependent nature of thickened fluid viscosity. Acknowledgment and appropriate selection of the thickener type is shown to be of great importance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Dysphagia is a common but relatively short-lived complication of a cerebrovascular accident and can occur on a chronic basis in many neurodegenerative diseases. Dysphagia that is present immediately following a stroke is found to resolve in half of all patients, although a small number of patients in whom dysphagia persists for more than three weeks generally have a less favorable outcome [1]. The condition occurs in as many as 60% of stroke patients [2] and can lead to dehydration, malnutrition, and most notably pulmonary aspiration [3,4]. Aspiration aids the transport of pathogenic bacteria into the lungs and can lead to aspiration pneumonia [5,6]. Numerous respiratory problems have been related to aspiration [7]. Dysphagic patients have difficulty swallowing fluids and often have their fluids thickened with a starch-based thickener as part of prescribed therapy. Exclusive oral consumption, however, can lead to inadequate hydration along with malnutrition when foods are rejected and it is one of the most long-standing and pressing problems in nursing homes. Kayser-Jones et al. [8] found that only one nursing home resident out of 40 consumed an adequate amount of liquids when on an oral diet. Elderly people who do not receive adequate fluids are more susceptible to urinary tract infections, pneumonia, renal failure, decubitus ulcers, and confusion, disorientation, and delirium, which are often misidentified as dementia. In addition, life-threatening electrolyte imbalances (i.e., hypernatremia and hyperkalemia) can occur. Finestone et al. [9] illustrated that dysphagic stroke patients receiving thickened fluid diets failed to meet their fluid requirements compared with patients on enteral feeding and intravenous fluid regimens. These reports highlight the problems with not only the fluid being too thin but also too thick.
It has been reported using electromyography, manometry, and videofluoroscopy techniques [10–13] that prolonged transit times and co-occurring prolongation of floor-of-mouth muscle contraction and pharyngeal manometric events occur with higher viscosity items. Fluids that travel more slowly through the oral cavity, because of their higher viscosities, provide the patient with additional time in which to prepare for pharyngeal swallow onset [14].
This work examines the time dependence of viscosity for two general classes of starch-based thickeners at room temperature (20.0°C). The two classes are pure maize starch and maltodextrin in the presence of a nonionic polysaccharide (carob bean gum/guar gum). Maltodextrins are produced by the enzymatic degradation of starch. It is widely known within the food industry that nonstarch hydrocolloids such as carob bean gum exhibit many functions to control resistance to flow (viscosity) and textural properties of foods and help to maintain overall product quality during storage [15]. This article investigates these two types of thickener by monitoring viscosity over several hours when the fluid is allowed to stand undisturbed.
Background
On a clinical basis the viscosity of thickened fluids is often judged subjectively and described using terms such as syrup or honey. It is vital that drinks of the correct viscosity are prepared consistently, because too low a viscosity may travel faster into the pharynx and may be more likely to enter the airway before protective mechanisms of the swallow can be initiated. Too high a viscosity is generally rejected by patients and can lead to malnutrition and dehydration. It is thought that in some patients a high viscosity and hence increased transit time can increase the likelihood of aspiration. Miller and Watkin [17] and Goulding and Bakheit [18] illustrated that a high-viscosity fluid can also aggravate swallowing, possibly because it increases the force required by the tongue to move the bolus and may worsen dysphagia. Therefore, it is clear that the viscosity must be precise to a certain degree.
Starch is the key ingredient in providing the desirable viscous characteristics of food products [19] and is ideal as a thickening agent. Starch granules are semicrystalline particles composed of a mixture of two polysaccharides, amylose and amylopectin. In solution these two polysaccharides associate via hydrogen bonds either directly or through hydrate bridges, forming semicrystalline molecular aggregates of amylopectin and amorphous areas of amylose [20].
Because starch gels absorb water from the solution into their starch granules (water imbibition) [21] and rely upon the formation of hydrogen bonds for structure, it is understandable that their viscosity is often extremely time dependent. As mentioned, starch pastes and gels are composite materials whose rheologic properties are determined by interactions between the swollen starch granules (dispersed phase) and the continuous viscous matrix [23–25]. The rheologic time-dependent characterization of starch foods establishes relationships between structure and flow and allows correlation with sensory evaluation [26].
Methods
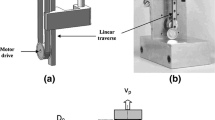
All experiments were performed on a Brookfield concentric cylinder R/S rheometer using a double-gap concentric cylinder attachment (Carl Stuart Ltd., UK). The rheometer was programmed using Brookfield RHEO 2000 software via a networked PC. Temperature was controlled by a Lauda Eco Line RE204 computer-controlled circulator at a constant 20.0°C for all experiments. Four different brands of thickener of varying composition were used. S1 (Hormel Thick and Easy) is 99.2% maize, 0.4% surcrose, 0.3% glucose, and 0.1% maltose. S2 (Nutricia Nutilis) and S3 (Sutherlands Health Ltd Thixo-D) are both 100% maize, yet S3 is a finer powder (granules are of a smaller size). S4 (Cow and Gate Instant Carobel) is 64% maltodextrin, 35% carob bean gum, and 1% calcium lactate.
Sample Preparation
Each solution was made by adding 0.5, 1, 1.5, 2, or 2.5 g (±0.0005 g) of the corresponding commercial starch thickener to 50 ml (±0.08 ml) of ordinary tap water that had been filtered using a commercially available water filter. This produced 1%, 2%, 3%, 4%, and 5% (w/v), respectively. Deionized water was not used because it is not consistent with real-life applications of the thickener. Throughout this article, “concentration” refers to the number of grams in 50 ml of water. All solutions were made by mixing the powdered starch into the water for 30 s at an approximate shear rate of 50 s−1 (analogous to gentle stirring) at room temperature (21–22°C). The solutions were allowed to stand for 5 min before being stirred at a similar shear rate for 30 s. The samples were placed in the rheometer and experiments started once the temperature had equilibrated to 20.0°C.
Experimentation
In dysphagia therapy thickened liquid solutions are often left at the bedside for hours with sporadic consumption. Therefore, it is important to determine how a thickened fluid’s viscosity changes over time with zero shear. The rheometer was programmed to measure the viscosity of the solution every 30 min at a constant shear rate and temperature over several hours. Each sample was subjected to a short period of shear followed by a long rest interval. The shear period was 30 s at a shear rate of 30 s−1 (this is analogous to gentle swirling or pouring [26], which is synonymous with the patient disturbing the fluid while consuming it and, therefore, is pertinent to the level of shear experienced by the fluid at bedside). Viscosity measurements were taken after the sample had been sheared for 10 s to avoid static yield stress or “startup flow.” The static yield stress is the stress needed to overcome the gelled structure to initiate flow. Startup flow is when a shear stress produced by sudden imposition of shear rate on a viscoelastic fluid displays an initial overshoot before reaching a steady state value [27]. Shearing the sample before measurements avoids these complications. A mean average was taken for the remaining 20 s of measurement. A rest period of 30 min was allowed before the next measurement. This experiment was performed for 17 h.
Results
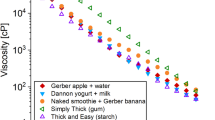
Figure 1a-c is a selection of plots of time versus apparent viscosity (the viscosity of a fluid measured at a given shear rate at a fixed temperature; for a viscosity measurement to be meaningful, the shear rate must be stated or defined) for three thickener brands commonly used in dysphagia therapy. These are maize-based thickeners (S1, S2, and S3) and all behaved in a similar manner to each other. The maize-based thickeners generally exhibit an initial decrease in viscosity followed by a steady increase, which can be approximated to an inverse exponential, the shape of which resembles a smoothed tick. All the graphs are important for dysphagia therapists and patients. Figure 1a shows a viscosity decrease of 33% (16 cP) and 18% (16 cP) for the 1.0- and 1.5-g samples, respectively, over the first 30 min, and a peak decrease of 42% and 50%. Figure 1b shows a viscosity decrease of 18% (2.5 cP) and 20% (10 cP) for 0.5- and 1.0-g samples, respectively, and a peak decrease of 21% and 36%.

Selection of graphs of discrete time versus viscosity for the maize-based thickener (S1, S2, and S3) at 20.0°C. These plots were chosen because they are of the middle-viscosity category, which is a commonly prescribed viscosity.
The maltodextrin-based thickener (S4), commonly used in pediatrics, behaved significantly differently compared with the maize-based thickeners. The viscosity increased dramatically over the first 2 h and in some cases doubled after 30 min. After 4 h the viscosity plateaued and did not change with time.
Figure 2 is a selection of the data for the maltodextrin-based thickener S4, along with a fitted curve based on the model:

Selection of data for viscosity versus time for S4 at 20.0°C.
where t is time in hours, and A, B, and C are parameters. A indicates the plateau viscosity in cP, B is the range of viscosity change (initial to plateau), and C is inversely proportional to the time taken for the plateau to be reached. Table 1 presents the parameter values for the model for five different concentrations.
Discussion
Within dysphagia therapy the required precision for these fluids is ambiguous. Smith et al. [28] attempted to draw boundaries on the perception of viscosity differences. The proposed boundaries of National Dysphagia Diet (NDD) are more widely used and are defined in Table 2. Although Steele and Van Lieshout [29] have shown that for healthy individuals tongue behaviors do not vary significantly in their movement characteristics across swallows of liquids ranging from 5 to 785 cP, the decrease in viscosity over the first 2 h for the maize-based thickeners, shown in Figure 1, is enough to shift the fluid to the lower NDD-defined category. This may have implications for cases where maintaining the upper category is important, especially dysphagic patients for whom viscosity tolerance is highly fragile. There is, however, no empirical evidence regarding swallowing function to support the NDD-defined boundaries.
It is common for tens of minutes up to hours to elapse before fluids are consumed. Therefore, the 30-min period in which the viscosity substantially decreases may leave the patient susceptible to the effects of this lower viscosity, which is conventionally assumed to be pulmonary aspiration. After an initial decrease in viscosity all the samples increased in viscosity. This gradual increase in viscosity is consistent with “syneresis.” Syneresis is the venting of the liquid component of a gel, i.e., in this case water being squeezed out of the matrix due to the formation of more and more hydrogen bonds.
The pure finer maize (S3) shown in Figure 1c was less dynamic and showed no significant decrease in viscosity. The maltodextrin-based thickener (S4) may appear more satisfactory from a therapist’s point of view in that there is no decrease in viscosity, which may indicate why it is used more commonly in pediatrics. However, as we have already mentioned, too thick a fluid can be just as problematic as too thin a fluid. Figure 2, in contrast to the maize data, shows that over the initial 30 min the viscosity increases by more than 100%. For most patients this increase in viscosity will not risk pulmonary aspiration, although it may worsen the condition or exacerbate malnutrition and dehydration as a result of the fluid being rejected [21,22]. Clearly, for fluids at room temperature it is advisable to wait 0.5–1 h if the viscosity is required to stabilize.
Table 1 shows the parameter values for the exponential model in Eq. (1) when fitted to the S4 data. Parameter A increases consistent with an exponential with increasing concentration, as would be expected since this represents the plateau viscosity (η∞). An empirical relationship linking parameter A and, therefore, η∞ (in cP) to the thickener concentration is shown in Eq. (2).
where g is the concentration of the thickener fluid (grams in 50 ml of water). This can be rewritten in terms of weight by volume (w/v) to give a more generic and practical equation:
where (w/v) is the percentage weight by volume.
The parameter B increases consistent with a linear model and indicates that with increasing concentration the degree of temporal change increases. Relative comparisons indicate that B_ Rel (B/A) remains constant. C increases linearly and indicates that the time taken for the plateau to be reached decreases linearly with increasing concentration. Figure 3 shows the increase in C with increasing concentration.

Graph illustrating increase in the parameter C from the model in Eq. (1) with increasing concentration for S4. Linear model fitted using least-squares fit.
The parameter C is important to therapists. For thicker S4 fluids, waiting a short time (<1 h) would radically improve the viscosity stability of the fluid. For thinner fluids, the viscosity during this time is likely to be highly dynamic.
Table 3 compares the viscosities of the maize and maltodextrin-based thickeners. It is clear that the maltodextrin-based thickener yields a substantially higher viscosity for equal mass than a maize-based thickener, particularly for the more concentrated samples, which are approximately a factor of 10 higher. This is most notably a result of the addition of carob bean gum, which has been shown to dramatically increase the viscosity of a starch system [16].
Conclusion
The starch thickeners used in dysphagia therapy are non-Newtonian (Newtonian describes a fluid where its rate of deformation is directly proportional to the stress applied to the fluid. However, many fluids exhibit a nonlinear response to stress and are called non-Newtonian fluids. Such fluids fall halfway between being a solid and a Newtonian fluid) and exhibit extreme time-dependency. The time-dependent behavior of the maize-based thickeners is of particular interest to therapists and patients because the fluids get thinner over the initial 1–4 h after preparation. This decrease in viscosity may increase the risk of aspiration in some patients even though they are prepared to the correct viscosity initially. In contrast, the maltodextrin-based thickener manifests no decrease in viscosity and the fluid becomes significantly thicker 30 min after preparation. This is also undesirable as there are many patients for whom thicker fluids pose problems. After the initial increase, the maltodextrin-based thickener is more consistent and stable over time than its maize-based equivalent, which is a desirable characteristic.
For S4, waiting for a short period of time dramatically improves the stability of the viscosity over time. Therefore, it may be beneficial for therapists to prepare the fluid to a lower viscosity and allow the fluid to stand to improve stability and avoid excessive thickening. To summarize, improved viscosity stability can be achieved if the fluid is left for a short while, especially for maltodextrin-based thickeners. Maize-based thickened fluids are best consumed immediately following preparation.
References
Barer DH: The natural history and functional consequences of dysphagia after hemispheric stroke. J Neurol, Neurosurg Psychiatry 52:236–241, 1989
Mann G, Hankey GJ, Cameron D: Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke 30:744–748, 1999
Weinberg AD, Minaker KL: Council on Scientific Affairs, American Medical Association: Dehydration: evaluation and management in older adults. JAMA 274:1552–1556, 1995
Axelsson K, Asplund K, Norberg A, Eriksson S: Eating problems and nutritional status during hospital stay of patients with severe stroke. J Am Diet Assoc 89:1092–1096, 1989
Langmore SE, Skarupski KA, Park PS, Fries BE: Predictors of aspiration pneumonia in nursing home residents. Dysphagia 17(4):298–307, 2002
Langmore SE, Terpenning MS, Schork A, Chen Y, Murray JT, Lopatin D, Loesche WJ: Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia 13(2):69–81, 1998
Marik PE: Aspiration pneumonitis and aspiration pneumonia. N Engl J Med 344(9):665–671, 2001
Kayser-Jones J, Schell ES, Porter C, Barbaccia JC, Shaw H: Factors contributing to dehydration in nursing homes: inadequate staffing and lack of professional supervision. J Am Geriatr Soc 47(10):1187–1194, 1999
Finestone HM, Foley NC, Woodbury MG, Greene-Finestone L: Quantifying fluid intake in dysphagic stroke patients: a preliminary comparison of oral and nonoral strategies. Arch Phys Med Rehabil 82:1744–1746, 2001
Dantas RO, Kern MK, Massey BT, Dodds WJ, Kahrilas PJ, Brasseur JG: Effects of swallowed bolus variables on oral and pharyngeal phases of swallowing. Am J Physiol 258(5):G675–G681, 1990
Reimers-Neils L, Logemann J, Larson C: Viscosity effects on EMG activity in normal swallow. Dysphagia 9(2):101–106, 1994
Ekberg O, Liedberg BO, Owall B: Barium and meat—a comparison between pharyngeal swallow of fluid and solid boluses. Acta Radiol Diagn 27:701–704, 1986
Lazarus CL, Logemann JA, Rademaker AW, Kahrilas PJ, Pajak T, Lazar R, Halper A: Effects of bolus volume, viscosity, and repeated swallows in nonstroke subjects and stroke patients. Arch Phys Med Rehabil 74(10):1066–1070, 1983
Logemann J: Manual for the Videofluoroscopic Study of Swallowing. 2nd ed. Austin, TX: Pro-Ed, 1983
Glicksman M: Function of gums in food products. In: Gum technology in the food industry. New York: Academic Press, 1969, Chap 2, pp 15–55
Funami T, Katoaka Y, Omoto T, Goto Y, Asai I, Nishinari K: Effects of non-ionic polysaccharides on the gelatinization and retrogradation behaviour of wheat starch. Food Hydrocolloids 19:1–13, 2005
Miller JL, Watkin KL: The influence of the bolus volume and viscosity on anterior lingual force during the stage of swallowing. Dysphagia 11:117–124, 1996
Goulding R, Bakheit AMO: Evaluation of benefits of monitoring fluid thickness in the dietary management of dysphagic stroke patients. Clin Rehabil 14:119–124, 2000
Yang H, Irudayaraj J, Otgonchimeg S, Walsh M: Rheological study of starch and dairy ingredient-based food systems. Food Chem 86:571–578, 2004
Christianson DD, Hodge JE, Osborne D, Detroy RW: Gelatinization of wheat starch as modified by xanthan gum, guar gum and cellulose gum. Cereal Chem 58:513–517, 1981
Zobel HF, Stephen AM: Starch: Structure, analysis, and application. In: Food Polysaccharides and their Applications. New York: Marcel Dekker, 1995, Chap 2
Keetels CJAM, van Vliet T, Walstra P: Gelation and retrogradation of concentrated starch systems: Parts 1, 2 and 3. Food Hydrocolloids 10:343–368, 1996
Eliasson AC: Viscoelastic behavior during the gelatinization of starch. J Texture Stud 17:253–265, 1986
Nguyen QD, Jensen CTB, Kristensen PG: Experimental and modelling studies of the flow properties of maize and waxy maize starch pastes. Chem Eng J 70:165–171, 1998
Doublier JL, Llamas G, Paton D: A rheological investigation of oat starch pastes. Cereal Chem 64:21–26, 1987
Sherman P: Food Structure Its Creation and Evaluation: The sensory-rheological interface. Oxford: Butterworths-Heinemann, 1988
Steffe JF: Rheological methods in food process engineering. San Francisco, CA: Freeman Press, 1996
Smith CH, Logemann JA, Burghardt WR, Carrell TD, Zecker SG: Oral sensory discrimination of fluid viscosity. Dysphagia 12:68–73, 1997
Steele CM, Van Lieshout PHHM: Influence of bolus consistency on lingual behaviors in sequential swallowing. Dysphagia 19(3):192–206, 2004
Acknowledgments
The authors gratefully acknowledge the support of the Engineering and Physical Sciences Research Council (EPSRC) and the help of Morecambe Bay NHS PCT.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dewar, R.J., Joyce, M.J. Time-Dependent Rheology of Starch Thickeners and the Clinical Implications for Dysphagia Therapy. Dysphagia 21, 264–269 (2006). https://doi.org/10.1007/s00455-006-9050-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-006-9050-7