
Abstract
The lymphatic vascular system has an important role in the maintenance of tissue fluid pressure homeostasis, in the mediation of the afferent immune response via recruitment of antigen-presenting cells toward draining lymph nodes, and in the intestinal absorption of dietary lipids. Substantial progress in our understanding of the development and the molecular mechanisms controlling the lymphatic system has been made during the last few years, based on a recent wave of discoveries of lymphatic endothelial cell-specific markers and growth factors. This has also led to new insights into the role of lymphatic endothelium in a number of diseases, including primary and secondary lymphedemas. The emerging role of lymphatic endothelium in the context of inflammation indicates that therapeutics targeting the lymphatic vasculature might represent a new strategy for anti-inflammatory therapies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
To cope with the complex needs of transporting fluids, gases, nutrients, signaling molecules, and cells through tissues, vertebrate organisms have developed two complementary vascular networks, the blood and the lymphatic vasculatures. The physiology of the blood vascular system and the role of angiogenesis (the growth of new blood vessels from pre-existing ones) in disease have been thoroughly studied over the last few decades (Carmeliet 2003). In contrast, substantial progress in our understanding of the development and molecular mechanisms controlling the lymphatic system, first identified almost four centuries ago (Asellius 1627), has only been made during the last few years, based on a recent wave of discoveries of lymphatic endothelial cell (LEC) markers and growth factors. Although the endothelial cells of blood vessels (BECs) and of lymphatic vessels have many features in common, such as their apical-basal polarity and the expression of certain pan-endothelial markers, the unique functional roles of these two vascular networks require extensive specialization.
Physiological functions of the lymphatic vascular system
Tissue fluid homeostasis
The primary role of the lymphatic vascular system is the maintenance of tissue fluid homeostasis by draining excess interstitial fluid (leaking from blood capillaries) and returning it into the blood flow. The lymphatic vascular network is composed of initial lymphatic capillaries and of collecting lymphatic vessels. The initial lymphatic vessels lack a basement membrane and are thin-walled with wide lumina lined by a single layer of overlapping LECs that are anchored to the extracellular matrix by fibrillin-containing anchoring filaments (Gerli et al. 2000). Under conditions of high interstitial pressure, lymphatic capillaries are pulled open by these anchoring filaments, facilitating the uptake of fluid, macromolecules, and cells. The importance of anchoring filaments and the extracellular matrix for lymphatic drainage has recently been demonstrated in extracellular matrix glycoprotein Emilin1-deficient mice (Danussi et al. 2008). These mice display pronounced lymphatic drainage impairment and increased lymphatic leakage.
Lymph flow is unidirectional from the lymphatic capillaries to larger collecting lymphatics and finally into the thoracic duct, which empties into the inferior vena cava (Cueni and Detmar 2006). The forces that move the lymph through the vessels include smooth muscle contraction along the collecting vessels, respiratory movements, and skeletal muscle action (Bridenbaugh et al. 2003). Collecting lymphatic vessels differ from initial lymphatic capillaries in several aspects, in addition to their larger diameter. They are covered by smooth muscle cells and contain intraluminal valves that prevent the backflow of lymph. The exact mechanisms of fluid uptake by initial lymphatic vessels have remained unclear. However, recent studies indicate that overlapping flaps of oak-leaf-shaped LECs of the initial lymphatics lack intercellular junctions at the tip but are anchored on their sides by discontinuous button-like junctions. These differ from the continuous zipper-like junctions seen in the collecting lymphatics (Baluk et al. 2007).
Immune cell trafficking and immune surveillance
The lymphatic system also plays a major role in immune reactions. Immune cells such as antigen-presenting dendritic cells, memory T lymphocytes, and macrophages and soluble antigens use the lymphatic network to drain from peripheral tissues to regional lymph nodes where the immune responses are initiated (Cavanagh and Von Andrian 2002). There is increasing evidence for an active role of lymphatic endothelium in mediating the entry of antigen-presenting cells and lymphocytes into lymphatic vessels (Johnson et al. 2006; Randolph et al. 2005). Indeed, the interaction of immune cells with lymphatics represents an important step in the regulation of the immune response (Ledgerwood et al. 2008). The molecular mechanisms involved will be discussed in more detail below in the context of lymphatic vessel involvement in inflammation.
Dietary fat absorption by intestinal lymphatics
Within the small intestine, specialized lymphatic vessels in the villi, called lacteals, absorb dietary lipids and the fat-soluble vitamins A, D, E, and K. Mucosal enterocytes assemble chylomicrons, viz., lipoprotein complexes of 100–2000 nm in diameter, that are exocytosed into the lamina propria where they come into contact with the lacteals (Blomhoff et al. 1990). Chylomicrons constitute up to 15% of the lymph volume after ingestion of a fat-containing meal. Little is known concerning the modifications of chylomicrons permitting their uptake by lacteal vessels (Van Dyck et al. 2007) or regarding the mechanisms of lipid uptake into lymphatics. However, recent studies have indicated the presence of a link between fat metabolism and lymphatic function in the intestine, based on studies in mice with a deficiency of fasting-induced adipose factor (Fiaf, also known as angiopoietin-like protein-4; Backhed et al. 2007) or of the lymphatic-specific transcription factor Prox1. Prox1 heterozygous mice die within the first 2–3 days after birth on all except one genetic background (Wigle and Oliver 1999). The surviving mice show adult onset obesity with fat deposits in the tissue surrounding the leaky lymphatics (Harvey et al. 2005). Prox1 heterozygous mice also have high levels of circulating insulin and leptin. Additional evidence for a relationship between lymphatic vessels and adipose tissue come from the observation of ectopic adipose tissue growth in edematous regions of individuals with chronic lymphedema (Brorson et al. 2006), and lymph fluid has been reported directly to promote adipocyte differentiation in vitro (Harvey et al. 2005). Studies into the mechanisms of lipid absorption by intestinal lymphatics are needed and might lead to a better understanding of malabsorption syndromes/vitamin deficiencies and of the mechanisms of intestinal lymphatic drug transport (Nordskog et al. 2001).
Development of the lymphatic vasculature
At the beginning of the last century, two opposing models for the embryonic development of the lymphatic system were proposed. Based upon results obtained by ink injection experiments, Florence Sabin proposed that isolated primitive lymph sacs originated from endothelial cells that bud from the cardinal vein during early development (Sabin 1902). The two jugular lymph sacs were thought to develop at the junction of the subclavian and anterior cardinal veins. According to this model, the peripheral lymphatic system originates from the primary lymph sacs and spreads by endothelial sprouting into the surrounding tissues and organs, where local capillaries are formed (Gray 1985; Sabin 1902). An alternative model proposed that lymphatic vessels developed independently from mesenchymal precursor cells (but not from embryonic veins), and that connections with veins were only established later on during development (Huntington and McClure 1910).
At present, most experimental evidence supports Sabin’s model of embryonic lymphatic development. A number of molecular genetics studies have shown that LECs do indeed sprout from the veins in the jugular area, and studies in Prox1 deficient mice have provided insight into the molecular players involved in this process (Wigle et al. 2002; Wigle and Oliver 1999). Recently, a Cre/loxP-based lineage-tracing study of mice expressing Cre recombinase under the control of Tie2, Runx1, or Prox1 promoter elements has provided strong evidence that the mammalian lymphatic system has a venous origin only (Srinivasan et al. 2007). However, circulating bone-marrow-derived cells have been found, at a small percentage of lymphatic vessels affected, to participate in experimental corneal lymphangiogenesis and in chronic renal transplant rejection (Kerjaschki et al. 2006; Religa et al. 2005). The relevance of these observations for normal lymphatic development is unknown.
Molecular control of lymphatic vascular development
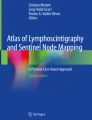
The homeodomain transcription factor Prox1 is the earliest protein known to be expressed in a polarized fashion in the cardinal vein (Wigle and Oliver 1999). A number of studies have revealed that Prox1 is a master gene controlling lymphatic-specific differentiation (Hong et al. 2002; Petrova et al. 2002; Wigle et al. 2002). In mice, Prox1-positive cells appear around embryonic day 9.5 (E9.5) in the cardinal vein and then bud off and migrate to form the first lymph sacs (Fig. 1). Prox1 null embryos die at approximately E14.5 and completely lack a lymphatic vasculature without defects of the blood vasculature (Wigle and Oliver 1999). Prox1 is at present considered to be the most specific lineage marker of the lymphatic endothelium (Wigle et al. 2002). Little is known about the signals upstream of Prox1 that lead to lymphatic commitment of blood vascular endothelium. In contrast, a number of Prox1 target genes have been identified. Overexpression of Prox1 in cultured vascular endothelial cells leads to a lymphatic reprogramming of these cells with upregulation of LEC markers and suppression of certain BEC markers (Hong et al. 2002; Petrova et al. 2002). Prox1 also increases endothelial cell motility and migration (Mishima et al. 2007; Dadras et al. 2008 (in press). LYVE-1, a homolog of the hyaluronan receptor CD44 (Banerji et al. 1999), is the first marker of lymphatic competence and is expressed in the cardinal vein at E8.5 (Oliver 2004). In adults, LYVE-1 is expressed not only by lymphatic endothelium, but also by liver sinusoids, some lung blood vessels, high endothelial venules, and activated tissue macrophages (Jackson 2003). Recently, LYVE-1 has been reported to be downregulated upon incubation of cultured LEC with tumor necrosis factor-alpha and also in an in vivo inflammation model (Johnson et al. 2007). However, the potential function of LYVE-1 function remains unclear since LYVE-1 deficient mice do not exhibit any abnormal phenotype, including lymphatic development and immune cell trafficking (Gale et al. 2007).

Current model of the stepwise embryonic development of the mammalian lymphatic system. During early vascular development, endothelial cells of the embryonic cardinal vein express the two lymphatic markers LYVE1 and vascular endothelial growth factor receptor-3 (LYVE1+ and VEGFR-3+; stage of lymphatic competence). Stimulation by an as yet unidentified mesenchymal signal induces expression of the transcription factor Prox1 in a subset of endothelial cells at the lateral side of the cardinal vein (Prox1+; stage of lymphatic commitment). These cells bud off from the vein and migrate into the surrounding tissue to form primitive lymph sacs. During this process, they adopt the expression of additional lymphatic lineage markers. The formation of a mature lymphatic network involves the function of additional genes, viz., podoplanin, ephrin B2, neuropilin-2, and FoxC2, and continues throughout the first few postnatal days. The mature lymphatic network is composed of initial lymphatic vessels and of collecting vessels covered with smooth muscle cells (SMC)
The vascular endothelial growth factor receptor-3 (VEGFR-3, also known as Flt4) is a specific receptor for the lymphangiogenic factors vascular endothelial growth factor-C (VEGF-C) and VEGF-D (Tammela et al. 2005a). Even before the onset of lymphatic vascular differentiation, VEGFR-3 is highly expressed by blood vascular endothelial cells, but its expression becomes gradually restricted to lymphatic endothelial cells after mid-gestation (Kaipainen et al. 1995). In agreement with its early expression in the blood vasculature, VEGFR-3 deletion in mice causes cardiovascular failure and embryonic death before the emergence of the lymphatic vasculature (Dumont et al. 1998). However, VEGFR-3 mutations have been identified as a cause for the cutaneous lymphedema in Chy mice, demonstrating the essential role of VEGFR-3 in lymphatic development and function (Karkkainen et al. 2001). In the adult, VEGFR-3 expression has also been reported in proliferating blood vessels during tumor angiogenesis (Laakkonen et al. 2007; Paavonen et al. 2000), indicating that VEGFR-3 might also be a mediator of angiogenesis under these conditions. During embryonic development, its ligand VEGF-C is produced by vascular smooth muscle cells and mesenchymal cells in areas adjacent to the sites of initial sprouting of LECs from veins (Kukk et al. 1996). The importance of VEGF-C/VEGFR-3 signaling in lymphatic development has recently been demonstrated in embryos homozygous for the VEGF-C deletion. These mice lack a lymphatic vasculature because of a lack of sprouting of lymphatically differentiated endothelial cells (Karkkainen et al. 2004). Whereas VEGF-C −/− mice die at around E15, VEGF-C +/– mice survive into adulthood but display severe lymphatic hypoplasia (Karkkainen et al. 2004). Although VEGF-D is able to rescue the sprouting in VEGF-C −/− embryos, VEGF-D deficient mice do not exhibit a lymphatic phenotype, indicating that VEGF-D is dispensable for the development of the lymphatic system (Baldwin et al. 2005). In culture, both VEGF-C and VEGF-D promote the proliferation, migration, and survival of lymphatic endothelial cells via signaling through VEGFR-3 (Makinen et al. 2001).
When LECs further migrate to form the first capillary networks, they begin to express the mucin-type transmembrane glycoprotein podoplanin (Schacht et al. 2003). Podoplanin is strongly expressed by lymphatic endothelium but not by blood vascular endothelium in vivo and in vitro (Breiteneder-Geleff et al. 1999; Hirakawa et al. 2003). Podoplanin null mice are characterized by lymphedema, abnormal patterning of the lymphatic vessel network, and impaired lymphatic transport (Schacht et al. 2003), but the detailed molecular functions of podoplanin remain unknown. A number of additional molecules appear to have a role during lymphatic development. Adrenomedullin, known as a potent vasodilator, has been recently found to play a role in lymphatic development based on studies in several knockout mouse models (Fritz-Six et al. 2008). Deficiency of adrenomedullin or of its receptors RAMP2 or calcitonin receptor-like receptor lead to pronounced edema associated with hypoplastic jugular lymph sacs and death at mid-gestation. However, whether impaired adrenomedullin signaling in blood vascular endothelium, associated with enhanced vascular permeability, contributes to the edema phenotype remains unclear (Ichikawa-Shindo et al. 2008).
Molecules involved in the maturation of the lymphatic vascular network
The formation of a mature lymphatic network continues throughout the first few postnatal days, and mechanisms for keeping the blood and lymphatic vascular compartments apart are essential to maintain the proper function of both networks. Circulating endothelial progenitor cells have been found to express the tyrosine kinase SYK and its substrate adaptor molecule SLP-76. Deficiency in SYK or SLP-76 results in arterio-venous shunting and connections between blood vessels and blood-filled lymphatic vessels that show mosaic expression of the lymphatic marker LYVE-1 (Abtahian et al. 2003; Sebzda et al. 2006). These findings have been interpreted to demonstrate a role of circulating progenitor cells for the maintenance of vessel integrity (Abtahian et al. 2003; Sebzda et al. 2006). However, a recent report indicates that the lymphatic-specific glycoprotein podoplanin mediates platelet aggregation via activation of C-type lectin-like receptor 2 (CLEC-2) expressed on platelets, and that this effect involves the activation of SYK and SLP-76 (Christou et al. 2008; Suzuki-Inoue et al. 2007). Thus, interactions between podoplanin and platelet-expressed CLEC-2 might represent a mechanism for preventing leaks between blood and lymphatic vessels.
Fasting-induced adipose factor (Fiaf/Angptl4) also appears to be involved in vascular separation since Fiaf-deficient mice show dilated and blood-filled intestinal lymphatics after birth, associated with reduced expression of the lymphatic marker Prox1 (Backhed et al. 2007). The underlying mechanisms contributing to this phenotype remain to be elucidated. Similarly, blood-filled lymphatic vessels have been found in embryos deficient in adaptor proteins of the Spred/Sprouty family, Spred-1 and Spred-2 (Taniguchi et al. 2007). Spreds are known as negative regulators of growth factor and cytokine-induced ERK activation and might potentially be involved in the negative regulation of VEGFR-3 signaling.
Besides vascular separation, additional molecular and cellular mechanisms are involved in promoting lymphatic vessel maturation. These include the differentiation of lymphatic capillaries and the collecting lymphatic network, the formation of valves, and the coverage of collecting lymphatic vessels and ducts by smooth muscle cells. Maintenance of VEGF-C signaling seems to be important for all of these processes (Karpanen et al. 2006b). An additional molecule that interacts with VEGF-C and VEGF-D, viz., neuropilin-2 (Nrp-2), has been shown to be essential for lymphatic vessel development and maturation, since Nrp-2 knockout mice fail to develop small-diameter lymphatic vessels (Yuan et al. 2002). Nrps are non-kinase type I transmembrane proteins that have an important role in axon guidance within the nervous system. Whereas Nrp-1 is mainly expressed by arterial endothelial cells, Nrp-2 expression is restricted to veins and lymphatics (Hong et al. 2002; Karkkainen et al. 2001; Yuan et al. 2002). Nrp-2 serves as a co-receptor for VEGF-C and may enhance signaling via VEGFR-3 (Karpanen et al. 2006a). Integrins are also involved in postnatal lymphatic maturation, as evidenced by the development of chylothorax resulting from lymphatic fluid accumulation in the pleural cavity in alpha9 integrin-deficient mice (Huang et al. 2000).
Angiopoietin signaling is necessary for normal blood vessel development as has been shown in a number of genetic mouse models (Dumont et al. 1994; Maisonpierre et al. 1997; Suri et al. 1996). Angiopoietin-1 (Ang1) is an activating ligand for the endothelial-specific Tie-2 receptor tyrosine kinase, and paracrine Ang1-mediated activation of Tie-2 acts as a regulator of vessel maturation and vascular quiescence. Ang2 deficient mice are characterized by impaired patterning of the lymphatic vascular network and recruitment of smooth muscle cells during development. Interestingly, these phenotypes (but not the blood vascular abnormalities) can be rescued by Ang1, suggesting that Ang2 might act as context-dependent agonist of Tie-2 during lymphangiogenesis, whereas it plays an antagonist role in angiogenesis (Gale et al. 2002). Recent studies indicate that Ang1 promotes lymphangiogenesis in mice, as demonstrated by the lymphatic hyperplasia observed after the adenoviral or transgenic delivery of Ang1 (Tammela et al. 2005b). The endothelial-restricted expression of Tie-2 has enabled the use of Tie-2 Cre mice for endothelial-specific gene ablation studies (Forde et al. 2002).
Ephrin/Eph signaling systems are involved in both angiogenic and lymphangiogenic processes. EphB2 knockout mice show defects in LEC sprouting, lymphatic patterning, and valve-formation and also have the ectopic coverage of skin lymphatic capillaries by smooth muscle cells (Makinen et al. 2005). The forkhead transcription factor FOXC2 is highly expressed in the developing lymphatic vasculature and in the luminal valves of adult lymphatic vessels. In Foxc2 deficient mice, the lymphatic vessels fail to form valves and lymphatic capillaries acquire ectopic coverage by smooth muscle cells and components of the basal lamina (Petrova et al. 2004). Overall, studies of lymphatic development have led to the identification of a number of novel markers for distinguishing lymphatic and blood vessels in murine and human tissues (Table 1).
Additional lymphatic growth factors
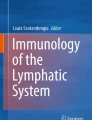
Hepatocyte growth factor (HGF) has recently been identified as a potent lymphangiogenic factor (Kajiya et al. 2005). HGF promotes LEC proliferation, migration, and tube formation via its receptor HGF-R (Fig. 2). The promigratory effects of HGF are partially mediated by the alpha9 integrin that is specifically expressed by LECs (Huang et al. 2000). HGF also promotes lymphangiogenesis in several organs in vivo, as demonstrated in HGF transgenic mice (Kajiya et al. 2005). Fibroblast growth factor-2 (FGF-2) was one of the earliest angiogenic factors identified and its role in angiogenesis has been well documented (Auguste et al. 2003). FGF-2 also promotes lymphangiogenesis by induction of VEGF-C secretion by blood vascular endothelium and perivascular cells in the mouse cornea assay (Kubo et al. 2002). Prox1 has been found to upregulate FGF receptor-3, which binds FGF-2 and mediates lymphangiogenesis independently of VEGFR-3 activation (Shin et al. 2006). Platelet-derived growth factor-BB (Cao et al. 2004) and insulin-like growth factors 1 and 2 (Bjorndahl et al. 2005) have been recently identified as additional factors with lymphangiogenic activity in vitro and in vivo. In consideration of the number of lymphangiogenic factors identified and the substantial cross talk with diverse receptors (Fig. 2), some of these factors may exhibit complex additive or synergistic effects on lymphatic growth and function.

Representation of lymphangiogenic growth factors and their receptors expressed by lymphatic endothelium. Several vascular endothelial growth factors (VEGF-A, VEGF-C, VEGF-D) promote lymphangiogenesis by activation of VEGF receptors-2 and -3 (VEGFR-2, VEGFR-3) and neuropilin-2 (Nrp2). Additional lymphatic growth factors include angiopoietin-1 (ANG-1), hepatocyte growth factor (HGF), fibroblast growth factor-2 (FGF-2), insulin-like growth factors (IGF-1, IGF-2), platelet-derived growth factor-BB (PDGF-BB), and adrenomedullin (AM)
Lymphatic involvement in disease
The distinct role of lymphatic vessels in various diseases has, for a long time, been obscured by the lack of lymphatic-endothelium-specific markers, growth factors, and receptors. The recent discovery of lymphatic markers such as podoplanin, Prox1, and LYVE-1 has made it possible to distinguish lymphatic vessels from blood vessels in situ and to isolate LECs for gene expression and proteomic profiling studies and for functional in vitro tests (Hirakawa et al. 2003; Kriehuber et al. 2001; Roesli et al. 2008). These studies, together with numerous new genetic mouse models, have provided new insights into the contribution of lymphatic endothelium to various diseases. We will focus, in our review, on lymphatic vascular involvement in lymphedema and in inflammatory diseases, since the role of lymphatic vessels in cancer metastasis has been comprehensively covered in recent reviews (Tobler and Detmar 2006; Wissmann and Detmar 2006).
Lymphedema
Impaired formation or function of the lymphatic network results in disfiguring and occasionally life-threatening swelling of the limbs, called lymphedema (Szuba and Rockson 1997). Lymphedema can arise as a hereditary primary disorder or as a secondary disorder. It is accompanied by fibrosis and susceptibility to infections and inflammation (Tabibiazar et al. 2006). Currently, there is no cure for lymphedema, and available treatments consist predominantly of remedial massage and restrictive bandaging.
Mutations that compromise the development or function of lymphatic vessels and that lead to lymphedema have been identified in several human genes. Inactivating mutations in the kinase domain of the VEGFR-3 gene have been found in congenital lymphedema (Milroy’s disease) with autosomal dominant inheritance (Brice et al. 2005; Butler et al. 2007; Karkkainen et al. 2000). These mutations inhibit phosphorylation of the receptor and prevent its downstream signaling. VEGFR-3 mutations have been detected in patients with family history of lymphedema, although de novo mutations have also been reported (Ghalamkarpour et al. 2006). Because of a naturally occurring mutation in VEGFR-3, a similar phenotype is seen in the Chy mouse (Karkkainen et al. 2001). In addition, recent studies have identified mutations in the FOXC2 gene as being responsible for lymphedema-distichiasis syndrome (Fang et al. 2000; Mangion et al. 1999; Sholto-Douglas-Vernon et al. 2005). The underlying mechanisms have been elucidated in FOXC2 deficient mice (Petrova et al. 2004). Mutations of the SOX18 gene, a SRY-related transcription factor, cause autosomal recessive and dominant forms of hypotrichosis lymphedema telangiectasia syndrome (Irrthum et al. 2003). The link to the SOX18 gene has been established by the phenotypic homology to “ragged” mice in which the phenotype is caused by four different premature truncations in SOX18 (Pennisi et al. 2000). In humans, mutations in the DNA-binding domain of SOX18 have been found in the recessive form of the disease, whereas in the dominant form, a heterozygous nonsense mutation has been found in the transactivation domain (Irrthum et al. 2003). The expression of SOX18 is regulated by VEGFR-3 activation and is an early marker of lymphatic differentiation; however, its detailed function remains currently unclear (Cermenati et al. 2008).
A point mutation in the nuclear factor kappa B (NFkB) essential modulator gene NEMO causes a disease with multiple symptoms, referred to as OL-EDA-ID (osteopetrosis, lymphedema, ectodermal dysplasia-anhidrotic, immunodeficiency; Doffinger et al. 2001). This disease indicates the potential importance of the NFkB pathway in lymphatic vascular function. Indeed, NFkB has been found to be constitutively active in lymphatic endothelial cells, although no functional role has as yet been attributed to this activity (Doffinger et al. 2001).
The major cause of secondary lymphedema in developing countries is infection with the mosquito-borne parasites Wuchereria bancrofti and Brugia malayi (Melrose 2002). This disorder, called lymphatic filariasis and more commonly known as elephantiasis, is a painful and profoundly disfiguring disease characterized by massive damage to the lymphatic vessels leading to permanent disability. Despite its major social and economic impact on affected countries, it is categorized as a neglected tropical disease (Beyrer et al. 2007).
In the industrialized countries, secondary lymphedema is mainly caused by surgical removal of lymph nodes or radiation therapy, particularly in patients with breast cancer. Secondary lymphedema remains a significant clinical problem with, according to some studies, one out of five women developing the condition following treatment for breast cancer (Clark et al. 2005).
The recent identification of growth factors capable of directly inducing the growth of lymphatic vessels, such as VEGF-C and VEGF-D, may provide new strategic approaches for the therapy of lymphedema (Rockson 2005). Adeno-associated virus-mediated delivery of VEGF-C to the skin of Chy mice improves the lymphedema phenotype (Karkkainen et al. 2001). Notably, a mutant form of VEGFC, viz., VEGF-C156S, that selectively binds VEGFR-3 but not VEGFR-2 successfully induces the formation of cutaneus lymphatic networks without causing blood vessel leakage, an overt effect observed with wild-type VEGF-C therapy (Saaristo et al. 2002). Therapy with VEGF-C protein has also been successfully applied in a surgical lymphedema model in the rabbit ear (Szuba et al. 2002). Importantly, treatment of lymph node-excised mice with adenovirally delivered human VEGF-C or VEGF-D results in a considerable improvement of the lymphatic draining function, associated with regeneration of mature lymphatic vessels. VEGF-C therapy also greatly improves the outcome of lymph node transplantation, indicating a potential treatment strategy for secondary lymphedema (Tammela et al. 2007).
Inflammation-associated lymphangiogenesis
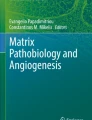
Inflammation is the normal response of the body to injury or infection but may also develop and persist in the context of autoimmune diseases and during tumor growth. Inflammation has also long been known to induce pronounced changes of the blood vasculature thereby significantly contributing to the clinical symptoms of inflammation: redness, warmth, and swelling (Pober and Sessa 2007). In addition to angiogenesis, recent studies have detected pronounced lymphangiogenesis in mouse models of chronic airway inflammation, psoriasis, and rheumatoid arthritis (Baluk et al. 2005; Kunstfeld et al. 2004; Paavonen et al. 2002; Zhang et al. 2007). In particular, pronounced lymphatic hyperplasia occurs in human psoriatic skin lesions and also in a VEGF-A transgenic mouse psoriasis model (Kunstfeld et al. 2004). In inflamed tissues, the lymphangiogenic factors VEGF-C and VEGF-A are secreted by immune cells such as macrophages or by resident tissue cells such as fibroblasts and keratinocytes (Ristimaki et al. 1998). Unpublished observations from our laboratory suggest that lymphangiogenesis is also associated with inflammatory bowel disease in a mouse model of interleukin-10 deficiency (Fig. 3). These findings indicate a potential involvement of the lymphatic vascular system in the pathogenesis of human inflammatory bowel syndromes (ulcerative colitis and Crohn’s disease) in which lymphatic hyperplasia has scarcely been studied (Pedica et al. 2008).

Lymphangiogenesis in colon inflammation. Whereas wild-type mice show normal lymphatic vasculature in the submucosal area of the colon wall (a), C3H/HeJBir.Il10 −/− mice display dramatically enlarged and tortuous lymphatic vessels accompanying the colon inflammation (b). Stained for the lymphatic vessel marker LYVE-1 (red); counter-stained with hematoxylin. Bars 100 μm
Recently, we have found that acute ultraviolet B (UVB) irradiation of murine skin results in leaky, functionally impaired lymphatics, and that blockade of VEGFR-3 prolongs UVB-irradiation-induced inflammation (Kajiya et al. 2007). Importantly, studies in mice indicate that UVB-mediated upregulation of VEGF-A induces lymphatic hyperpermeability that can be blocked by systemic application of an anti-VEGF-A antibody (Kajiya et al. 2006). Furthermore, the nitric oxide/soluble guanylate cyclase alpha1beta1/cGMP pathway has been found to modulate lymphatic vessel function in UVB-irradiation-caused inflammation, indicating that blockade of soluble guanylate cyclase might represent a novel therapeutic strategy for inhibiting lymphangiogenesis and inflammation (Kajiya et al. 2008).
Lymphatic vessels also play a key role in the migration of dendritic cells to draining lymph nodes where they initiate the adaptive immune response (Halin and Detmar 2006). Mature inflammatory-signal-activated dendritic cells upregulate the expression of chemokine receptor CCR7. Lymphatic endothelium actively secretes the respective ligand, CCL21, causing dendritic cell chemotaxis toward lymphatic vessels (Bromley et al. 2005; Debes et al. 2005). CCR7 might also mediate the exit of CD4+ memory T cells from tissues to lymphatic vessels (Yuan et al. 2002). Furthermore, inflammatory stimuli have been reported to increase the lymph flow, which promotes dendritic cell migration to lymph nodes (Gunn et al. 1998). There is increasing evidence that inflammation-induced expression of adhesion molecules on lymphatic endothelium might facilitate the exit of dendritic cells and lymphocytes into lymphatic vessels. Incubation of LECs with tumor necrosis factor-alpha upregulates the expression of intercellular adhesion molecule-1 (ICAM-1), vascular adhesion molecule-1 (VCAM-1), and E-selectin, and systemic blockade of ICAM-1 and VCAM-1 has been reported to inhibit inflammation-induced lymphatic transmigration in vivo (Johnson et al. 2006). Sphingosine-1-phosphate (S1P) and its receptor S1P1/EDG1 have been implicated in the process of lymphocyte egress from the thymus and lymph nodes (Halin et al. 2005; Matloubian et al. 2004). Recent data indicate that stimulation of S1P1 on T lymphocytes by the S1P1 agonist FTY720 inhibits their migration across the endothelium of afferent lymphatic vessels, leading to retention of T lymphocytes in peripheral tissues (Ledgerwood et al. 2008).
Interestingly, lymphangiogenesis is also observed in the lymph nodes draining the inflamed tissue, indicating a remote control by drainage of lymphangiogenic factors from peripheral tissues, although secretion of lymphangiogenic factors by cells residing within lymph nodes might contribute to this effect (Angeli et al. 2006; Halin et al. 2007).
Overall, the biological role of lymphangiogenesis in the pathogenesis of chronic inflammation needs further clarification. On one hand, activation of lymphatic vessels might promote immune cell trafficking to the draining lymph nodes, thereby supporting the establishment of an inflammatory loop. Indeed, lymphangiogenesis has been proposed to contribute to renal transplant rejection by promoting the export of CCR7-positive inflammatory cells guided by LEC-derived CCL21 (Kerjaschki et al. 2004). Moreover, blockade of VEGFR-3 in the initial stage of inflammation in mouse corneas impairs dendritic cell trafficking to draining lymph nodes, the induction of delayed-type hypersensitivity, and the rejection of corneal transplants (Chen et al. 2004). On the other hand, lymphangiogenesis might be beneficial for the resolution of chronic inflammation since lymphatic vessels drain, and thereby remove, accumulated fluid, immune cells, and inflammatory cytokines from the sites of inflammation. Indeed, inhibition of VEGFR-3 signaling has been found to impair the lymphatic vascular network and to promote mucosal edema in a mouse model of chronic airway inflammation (Baluk et al. 2005). Further experimental studies and observations in human inflammatory conditions indicate that impaired lymphatic drainage leads to the exacerbation of disease (Kajiya et al. 2007; Middel et al. 2006; Ryan 1980). VEGF-A and VEGF-C appear to exert opposing effects in chronic inflammation (Halin et al. 2007; Kajiya et al. 2006, 2007). Whereas VEGF-A might promote inflammation by inducing more leaky and non-functional lymphatic vessels, VEGF-C seems to promote lymphatic flow and the resolution of inflammation. However, more experimental evidence is required to support this concept further. Taken together, the emerging role of lymphatic endothelium in the context of inflammation indicates that anti-inflammatory therapeutics targeting the lymphatic vasculature might represent a new strategy to improve the lives of patients with inflammatory conditions.
References
Abtahian F, Guerriero A, Sebzda E, Lu MM, Zhou R, Mocsai A, Myers EE, Huang B, Jackson DG, Ferrari VA, Tybulewicz V, Lowell CA, Lepore JJ, Koretzky GA, Kahn ML (2003) Regulation of blood and lymphatic vascular separation by signaling proteins SLP-76 and Syk. Science 299:247–251
Albelda SM, Muller WA, Buck CA, Newman PJ (1991) Molecular and cellular properties of PECAM-1 (endoCAM/CD31): a novel vascular cell-cell adhesion molecule. J Cell Biol 114:1059–1068
Angeli V, Ginhoux F, Llodra J, Quemeneur L, Frenette PS, Skobe M, Jessberger R, Merad M, Randolph GJ (2006) B cell-driven lymphangiogenesis in inflamed lymph nodes enhances dendritic cell mobilization. Immunity 24:203–215
Asellius G (1627) De lacteibus sive lacteis venis quarto vasorum mesaroicum genere novo invente Gasp. Mediolani, Milan
Auguste P, Javerzat S, Bikfalvi A (2003) Regulation of vascular development by fibroblast growth factors. Cell Tissue Res 314:157–166
Backhed F, Crawford PA, O’Donnell D, Gordon JI (2007) Postnatal lymphatic partitioning from the blood vasculature in the small intestine requires fasting-induced adipose factor. Proc Natl Acad Sci USA 104:606–611
Baldwin ME, Halford MM, Roufail S, Williams RA, Hibbs ML, Grail D, Kubo H, Stacker SA, Achen MG (2005) Vascular endothelial growth factor D is dispensable for development of the lymphatic system. Mol Cell Biol 25:2441–2449
Baluk P, Tammela T, Ator E, Lyubynska N, Achen MG, Hicklin DJ, Jeltsch M, Petrova TV, Pytowski B, Stacker SA, Yla-Herttuala S, Jackson DG, Alitalo K, McDonald DM (2005) Pathogenesis of persistent lymphatic vessel hyperplasia in chronic airway inflammation. J Clin Invest 115:247–257
Baluk P, Fuxe J, Hashizume H, Romano T, Lashnits E, Butz S, Vestweber D, Corada M, Molendini C, Dejana E, McDonald DM (2007) Functionally specialized junctions between endothelial cells of lymphatic vessels. J Exp Med 204:2349–2362
Banerji S, Ni J, Wang SX, Clasper S, Su J, Tammi R, Jones M, Jackson DG (1999) LYVE-1, a new homologue of the CD44 glycoprotein, is a lymph-specific receptor for hyaluronan. J Cell Biol 144:789–801
Beyrer C, Villar JC, Suwanvanichkij V, Singh S, Baral SD, Mills EJ (2007) Neglected diseases, civil conflicts, and the right to health. Lancet 370:619–627
Bjorndahl M, Cao R, Nissen LJ, Clasper S, Johnson LA, Xue Y, Zhou Z, Jackson D, Hansen AJ, Cao Y (2005) Insulin-like growth factors 1 and 2 induce lymphangiogenesis in vivo. Proc Natl Acad Sci USA 102:15593–15598
Blomhoff R, Green MH, Berg T, Norum KR (1990) Transport and storage of vitamin A. Science 250:399–404
Breiteneder-Geleff S, Soleiman A, Kowalski H, Horvat R, Amann G, Kriehuber E, Diem K, Weninger W, Tschachler E, Alitalo K, Kerjaschki D (1999) Angiosarcomas express mixed endothelial phenotypes of blood and lymphatic capillaries: podoplanin as a specific marker for lymphatic endothelium. Am J Pathol 154:385–394
Brice G, Child AH, Evans A, Bell R, Mansour S, Burnand K, Sarfarazi M, Jeffery S, Mortimer P (2005) Milroy disease and the VEGFR-3 mutation phenotype. J Med Genet 42:98–102
Bridenbaugh EA, Gashev AA, Zawieja DC (2003) Lymphatic muscle: a review of contractile function. Lymphat Res Biol 1:147–158
Bromley SK, Thomas SY, Luster AD (2005) Chemokine receptor CCR7 guides T cell exit from peripheral tissues and entry into afferent lymphatics. Nat Immunol 6:895–901
Brorson H, Ohlin K, Olsson G, Langstrom G, Wiklund I, Svensson H (2006) Quality of life following liposuction and conservative treatment of arm lymphedema. Lymphology 39:8–25
Butler MG, Dagenais SL, Rockson SG, Glover TW (2007) A novel VEGFR3 mutation causes Milroy disease. Am J Med Genet [A] 143:1212–1217
Cao R, Bjorndahl MA, Religa P, Clasper S, Garvin S, Galter D, Meister B, Ikomi F, Tritsaris K, Dissing S, Ohhashi T, Jackson DG, Cao Y (2004) PDGF-BB induces intratumoral lymphangiogenesis and promotes lymphatic metastasis. Cancer Cell 6:333–345
Carmeliet P (2003) Angiogenesis in health and disease. Nat Med 9:653–660
Cavanagh LL, Von Andrian UH (2002) Travellers in many guises: the origins and destinations of dendritic cells. Immunol Cell Biol 80:448–462
Cermenati S, Moleri S, Cimbro S, Corti P, Del Giacco L, Amodeo R, Dejana E, Koopman P, Cotelli F, Beltrame M (2008) Sox18 and Sox7 play redundant roles in vascular development. Blood 111:2657–2666
Chen L, Hamrah P, Cursiefen C, Zhang Q, Pytowski B, Streilein JW, Dana MR (2004) Vascular endothelial growth factor receptor-3 mediates induction of corneal alloimmunity. Nat Med 10:813–815
Christou CM, Pearce AC, Watson AA, Mistry AR, Pollitt AY, Fenton-May AE, Johnson LA, Jackson DG, Watson SP, O’Callaghan CA (2008) Renal cells activate the platelet receptor CLEC-2 through podoplanin. Biochem J 411:133–140
Clark B, Sitzia J, Harlow W (2005) Incidence and risk of arm oedema following treatment for breast cancer: a three-year follow-up study. Q J Med 98:343–348
Cueni LN, Detmar M (2006) New insights into the molecular control of the lymphatic vascular system and its role in disease. J Invest Dermatol 126:2167–2177
Dadras SS, Skrzypek A, Nguyen L, Shin J, Schulz MMP, Arbiser J, Mihm MC, Detmar M (2008) Prox-1 promotes invasion of kaposiform hemangioendotheliomas. J Invest Dermatol (in press)
Danussi C, Spessotto P, Petrucco A, Wassermann B, Sabatelli P, Montesi M, Doliana R, Bressan GM, Colombatti A (2008) Emilin1 deficiency causes structural and functional defects of lymphatic vasculature. Mol Cell Biol 28:4026–4039
Debes GF, Arnold CN, Young AJ, Krautwald S, Lipp M, Hay JB, Butcher EC (2005) Chemokine receptor CCR7 required for T lymphocyte exit from peripheral tissues. Nat Immunol 6:889–894
Doffinger R, Smahi A, Bessia C, Geissmann F, Feinberg J, Durandy A, Bodemer C, Kenwrick S, Dupuis-Girod S, Blanche S, Wood P, Rabia SH, Headon DJ, Overbeek PA, Le Deist F, Holland SM, Belani K, Kumararatne DS, Fischer A, Shapiro R, Conley ME, Reimund E, Kalhoff H, Abinun M, Munnich A, Israel A, Courtois G, Casanova JL (2001) X-linked anhidrotic ectodermal dysplasia with immunodeficiency is caused by impaired NF-kappaB signaling. Nat Genet 27:277–285
Dumont DJ, Anderson L, Breitman ML, Duncan AM (1994) Assignment of the endothelial-specific protein receptor tyrosine kinase gene (TEK) to human chromosome 9p21. Genomics 23:512–513
Dumont DJ, Jussila L, Taipale J, Lymboussaki A, Mustonen T, Pajusola K, Breitman M, Alitalo K (1998) Cardiovascular failure in mouse embryos deficient in VEGF receptor-3. Science 282:946–949
Ebata N, Nodasaka Y, Sawa Y, Yamaoka Y, Makino S, Totsuka Y, Yoshida S (2001) Desmoplakin as a specific marker of lymphatic vessels. Microvasc Res 61:40–48
Fang J, Dagenais SL, Erickson RP, Arlt MF, Glynn MW, Gorski JL, Seaver LH, Glover TW (2000) Mutations in FOXC2 (MFH-1), a forkhead family transcription factor, are responsible for the hereditary lymphedema-distichiasis syndrome. Am J Hum Genet 67:1382–1388
Forde A, Constien R, Grone HJ, Hammerling G, Arnold B (2002) Temporal Cre-mediated recombination exclusively in endothelial cells using Tie2 regulatory elements. Genesis 33:191–197
Fritz-Six KL, Dunworth WP, Li M, Caron KM (2008) Adrenomedullin signaling is necessary for murine lymphatic vascular development. J Clin Invest 118:40–50
Gale NW, Thurston G, Hackett SF, Renard R, Wang Q, McClain J, Martin C, Witte C, Witte MH, Jackson D, Suri C, Campochiaro PA, Wiegand SJ, Yancopoulos GD (2002) Angiopoietin-2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by angiopoietin-1. Dev Cell 3:411–423
Gale NW, Prevo R, Espinosa J, Ferguson DJ, Dominguez MG, Yancopoulos GD, Thurston G, Jackson DG (2007) Normal lymphatic development and function in mice deficient for the lymphatic hyaluronan receptor LYVE-1. Mol Cell Biol 27:595–604
Gerli R, Solito R, Weber E, Agliano M (2000) Specific adhesion molecules bind anchoring filaments and endothelial cells in human skin initial lymphatics. Lymphology 33:148–157
Ghalamkarpour A, Morlot S, Raas-Rothschild A, Utkus A, Mulliken JB, Boon LM, Vikkula M (2006) Hereditary lymphedema type I associated with VEGFR3 mutation: the first de novo case and atypical presentations. Clin Genet 70:330–335
Gray H (1985) The lymphatic system. In: Clemente CD (ed) Anatomy of the human body. Lea and Febiger, Philadelphia
Gunn MD, Tangemann K, Tam C, Cyster JG, Rosen SD, Williams LT (1998) A chemokine expressed in lymphoid high endothelial venules promotes the adhesion and chemotaxis of naive T lymphocytes. Proc Natl Acad Sci USA 95:258–263
Halin C, Detmar M (2006) An unexpected connection: lymph node lymphangiogenesis and dendritic cell migration. Immunity 24:129–131
Halin C, Scimone ML, Bonasio R, Gauguet JM, Mempel TR, Quackenbush E, Proia RL, Mandala S, von Andrian UH (2005) The S1P-analog FTY720 differentially modulates T-cell homing via HEV: T-cell-expressed S1P1 amplifies integrin activation in peripheral lymph nodes but not in Peyer patches. Blood 106:1314–1322
Halin C, Tobler NE, Vigl B, Brown LF, Detmar M (2007) VEGF-A produced by chronically inflamed tissue induces lymphangiogenesis in draining lymph nodes. Blood 110:3158–3167
Harvey NL, Srinivasan RS, Dillard ME, Johnson NC, Witte MH, Boyd K, Sleeman MW, Oliver G (2005) Lymphatic vascular defects promoted by Prox1 haploinsufficiency cause adult-onset obesity. Nat Genet 37:1072–1081
Hirakawa S, Hong YK, Harvey N, Schacht V, Matsuda K, Libermann T, Detmar M (2003) Identification of vascular lineage-specific genes by transcriptional profiling of isolated blood vascular and lymphatic endothelial cells. Am J Pathol 162:575–586
Hong YK, Harvey N, Noh YH, Schacht V, Hirakawa S, Detmar M, Oliver G (2002) Prox1 is a master control gene in the program specifying lymphatic endothelial cell fate. Dev Dyn 225:351–357
Huang XZ, Wu JF, Ferrando R, Lee JH, Wang YL, Farese RV Jr, Sheppard D (2000) Fatal bilateral chylothorax in mice lacking the integrin alpha9beta1. Mol Cell Biol 20:5208–5215
Huntington GS, McClure CFW (1910) The anatomy and development of the jugular lymph sac in the domestic cat (Felis domestica). Am J Anat 10:177–311
Ichikawa-Shindo Y, Sakurai T, Kamiyoshi A, Kawate H, Iinuma N, Yoshizawa T, Koyama T, Fukuchi J, Iimuro S, Moriyama N, Kawakami H, Murata T, Kangawa K, Nagai R, Shindo T (2008) The GPCR modulator protein RAMP2 is essential for angiogenesis and vascular integrity. J Clin Invest 118:29–39
Irjala H, Johansson EL, Grenman R, Alanen K, Salmi M, Jalkanen S (2001) Mannose receptor is a novel ligand for L-selectin and mediates lymphocyte binding to lymphatic endothelium. J Exp Med 194:1033–1042
Irrthum A, Devriendt K, Chitayat D, Matthijs G, Glade C, Steijlen PM, Fryns JP, Van Steensel MA, Vikkula M (2003) Mutations in the transcription factor gene SOX18 underlie recessive and dominant forms of hypotrichosis-lymphedema-telangiectasia. Am J Hum Genet 72:1470–1478
Jaalouk DE, Ozawa MG, Sun J, Lahdenranta J, Schlingemann RO, Pasqualini R, Arap W (2007) The original Pathologische Anatomie Leiden-endothelium monoclonal antibody recognizes a vascular endothelial growth factor binding site within neuropilin-1. Cancer Res 67:9623–9629
Jackson DG (2003) The lymphatics revisited: new perspectives from the hyaluronan receptor LYVE-1. Trends Cardiovasc Med 13:1–7
Johnson LA, Clasper S, Holt AP, Lalor PF, Baban D, Jackson DG (2006) An inflammation-induced mechanism for leukocyte transmigration across lymphatic vessel endothelium. J Exp Med 203:2763–2777
Johnson LA, Prevo R, Clasper S, Jackson DG (2007) Inflammation-induced uptake and degradation of the lymphatic endothelial hyaluronan receptor LYVE-1. J Biol Chem 282:33671–33680
Kaipainen A, Korhonen J, Mustonen T, van Hinsbergh VW, Fang GH, Dumont D, Breitman M, Alitalo K (1995) Expression of the fms-like tyrosine kinase 4 gene becomes restricted to lymphatic endothelium during development. Proc Natl Acad Sci USA 92:3566–3570
Kajiya K, Hirakawa S, Ma B, Drinnenberg I, Detmar M (2005) Hepatocyte growth factor promotes lymphatic vessel formation and function. EMBO J 24:2885–2895
Kajiya K, Hirakawa S, Detmar M (2006) Vascular endothelial growth factor-A mediates ultraviolet B-induced impairment of lymphatic vessel function. Am J Pathol 169:1496–1503
Kajiya K, Kunstfeld R, Detmar M, Chung JH (2007) Reduction of lymphatic vessels in photodamaged human skin. J Dermatol Sci 47:241–243
Kajiya K, Huggenberger R, Drinnenberg I, Ma B, Detmar M (2008) Nitric oxide mediates lymphatic vessel activation via soluble guanylate cyclase alpha1beta1-impact on inflammation. FASEB J 22:530–537
Karkkainen MJ, Ferrell RE, Lawrence EC, Kimak MA, Levinson KL, McTigue MA, Alitalo K, Finegold DN (2000) Missense mutations interfere with VEGFR-3 signalling in primary lymphoedema. Nat Genet 25:153–159
Karkkainen MJ, Saaristo A, Jussila L, Karila KA, Lawrence EC, Pajusola K, Bueler H, Eichmann A, Kauppinen R, Kettunen MI, Yla-Herttuala S, Finegold DN, Ferrell RE, Alitalo K (2001) A model for gene therapy of human hereditary lymphedema. Proc Natl Acad Sci USA 98:12677–12682
Karkkainen MJ, Haiko P, Sainio K, Partanen J, Taipale J, Petrova TV, Jeltsch M, Jackson DG, Talikka M, Rauvala H, Betsholtz C, Alitalo K (2004) Vascular endothelial growth factor C is required for sprouting of the first lymphatic vessels from embryonic veins. Nat Immunol 5:74–80
Karpanen T, Heckman CA, Keskitalo S, Jeltsch M, Ollila H, Neufeld G, Tamagnone L, Alitalo K (2006a) Functional interaction of VEGF-C and VEGF-D with neuropilin receptors. FASEB J 20:1462–1472
Karpanen T, Wirzenius M, Makinen T, Veikkola T, Haisma HJ, Achen MG, Stacker SA, Pytowski B, Yla-Herttuala S, Alitalo K (2006b) Lymphangiogenic growth factor responsiveness is modulated by postnatal lymphatic vessel maturation. Am J Pathol 169:708–718
Kerjaschki D, Regele HM, Moosberger I, Nagy-Bojarski K, Watschinger B, Soleiman A, Birner P, Krieger S, Hovorka A, Silberhumer G, Laakkonen P, Petrova T, Langer B, Raab I (2004) Lymphatic neoangiogenesis in human kidney transplants is associated with immunologically active lymphocytic infiltrates. J Am Soc Nephrol 15:603–612
Kerjaschki D, Huttary N, Raab I, Regele H, Bojarski-Nagy K, Bartel G, Krober SM, Greinix H, Rosenmaier A, Karlhofer F, Wick N, Mazal PR (2006) Lymphatic endothelial progenitor cells contribute to de novo lymphangiogenesis in human renal transplants. Nat Med 12:230–234
Kriehuber E, Breiteneder-Geleff S, Groeger M, Soleiman A, Schoppmann SF, Stingl G, Kerjaschki D, Maurer D (2001) Isolation and characterization of dermal lymphatic and blood endothelial cells reveal stable and functionally specialized cell lineages. J Exp Med 194:797–808
Kubo H, Cao R, Brakenhielm E, Makinen T, Cao Y, Alitalo K (2002) Blockade of vascular endothelial growth factor receptor-3 signaling inhibits fibroblast growth factor-2-induced lymphangiogenesis in mouse cornea. Proc Natl Acad Sci USA 99:8868–8873
Kukk E, Lymboussaki A, Taira S, Kaipainen A, Jeltsch M, Joukov V, Alitalo K (1996) VEGF-C receptor binding and pattern of expression with VEGFR-3 suggests a role in lymphatic vascular development. Development 122:3829–3837
Kunstfeld R, Hirakawa S, Hong YK, Schacht V, Lange-Asschenfeldt B, Velasco P, Lin C, Fiebiger E, Wei X, Wu Y, Hicklin D, Bohlen P, Detmar M (2004) Induction of cutaneous delayed-type hypersensitivity reactions in VEGF-A transgenic mice results in chronic skin inflammation associated with persistent lymphatic hyperplasia. Blood 104:1048–1057
Laakkonen P, Waltari M, Holopainen T, Takahashi T, Pytowski B, Steiner P, Hicklin D, Persaud K, Tonra JR, Witte L, Alitalo K (2007) Vascular endothelial growth factor receptor 3 is involved in tumor angiogenesis and growth. Cancer Res 67:593–599
Ledgerwood LG, Lal G, Zhang N, Garin A, Esses SJ, Ginhoux F, Merad M, Peche H, Lira SA, Ding Y, Yang Y, He X, Schuchman EH, Allende ML, Ochando JC, Bromberg JS (2008) The sphingosine 1-phosphate receptor 1 causes tissue retention by inhibiting the entry of peripheral tissue T lymphocytes into afferent lymphatics. Nat Immunol 9:42–53
Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, Compton D, McClain J, Aldrich TH, Papadopoulos N, Daly TJ, Davis S, Sato TN, Yancopoulos GD (1997) Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science 277:55–60
Makinen T, Veikkola T, Mustjoki S, Karpanen T, Catimel B, Nice EC, Wise L, Mercer A, Kowalski H, Kerjaschki D, Stacker SA, Achen MG, Alitalo K (2001) Isolated lymphatic endothelial cells transduce growth, survival and migratory signals via the VEGF-C/D receptor VEGFR-3. EMBO J 20:4762–4773
Makinen T, Adams RH, Bailey J, Lu Q, Ziemiecki A, Alitalo K, Klein R, Wilkinson GA (2005) PDZ interaction site in ephrinB2 is required for the remodeling of lymphatic vasculature. Genes Dev 19:397–410
Mangion J, Rahman N, Mansour S, Brice G, Rosbotham J, Child AH, Murday VA, Mortimer PS, Barfoot R, Sigurdsson A, Edkins S, Sarfarazi M, Burnand K, Evans AL, Nunan TO, Stratton MR, Jeffery S (1999) A gene for lymphedema-distichiasis maps to 16q24.3. Am J Hum Genet 65:427–432
Matloubian M, Lo CG, Cinamon G, Lesneski MJ, Xu Y, Brinkmann V, Allende ML, Proia RL, Cyster JG (2004) Lymphocyte egress from thymus and peripheral lymphoid organs is dependent on S1P receptor 1. Nature 427:355–360
Melrose WD (2002) Lymphatic filariasis: new insights into an old disease. Int J Parasitol 32:947–960
Middel P, Raddatz D, Gunawan B, Haller F, Radzun HJ (2006) Increased number of mature dendritic cells in Crohn’s disease: evidence for a chemokine mediated retention mechanism. Gut 55:220–227
Mishima K, Watabe T, Saito A, Yoshimatsu Y, Imaizumi N, Masui S, Hirashima M, Morisada T, Oike Y, Araie M, Niwa H, Kubo H, Suda T, Miyazono K (2007) Prox1 induces lymphatic endothelial differentiation via integrin alpha9 and other signaling cascades. Mol Biol Cell 18:1421–1429
Nordskog BK, Phan CT, Nutting DF, Tso P (2001) An examination of the factors affecting intestinal lymphatic transport of dietary lipids. Adv Drug Deliv Rev 50:21–44
Oliver G (2004) Lymphatic vasculature development. Nat Rev Immunol 4:35–45
Paavonen K, Puolakkainen P, Jussila L, Jahkola T, Alitalo K (2000) Vascular endothelial growth factor receptor-3 in lymphangiogenesis in wound healing. Am J Pathol 156:1499–1504
Paavonen K, Mandelin J, Partanen T, Jussila L, Li TF, Ristimaki A, Alitalo K, Konttinen YT (2002) Vascular endothelial growth factors C and D and their VEGFR-2 and 3 receptors in blood and lymphatic vessels in healthy and arthritic synovium. J Rheumatol 29:39–45
Pedica F, Ligorio C, Tonelli P, Bartolini S, Baccarini P (2008) Lymphangiogenesis in Crohn's disease: an immunohistochemical study using monoclonal antibody D2–40. Virchows Arch 452:57–63
Penn PE, Jiang DZ, Fei RG, Sitnicka E, Wolf NS (1993) Dissecting the hematopoietic microenvironment. IX. Further characterization of murine bone marrow stromal cells. Blood 81:1205–1213
Pennisi D, Gardner J, Chambers D, Hosking B, Peters J, Muscat G, Abbott C, Koopman P (2000) Mutations in Sox18 underlie cardiovascular and hair follicle defects in ragged mice. Nat Genet 24:434–437
Petrova TV, Makinen T, Makela TP, Saarela J, Virtanen I, Ferrell RE, Finegold DN, Kerjaschki D, Yla-Herttuala S, Alitalo K (2002) Lymphatic endothelial reprogramming of vascular endothelial cells by the Prox-1 homeobox transcription factor. EMBO J 21:4593–4599
Petrova TV, Karpanen T, Norrmen C, Mellor R, Tamakoshi T, Finegold D, Ferrell R, Kerjaschki D, Mortimer P, Yla-Herttuala S, Miura N, Alitalo K (2004) Defective valves and abnormal mural cell recruitment underlie lymphatic vascular failure in lymphedema distichiasis. Nat Med 10:974–981
Pober JS, Sessa WC (2007) Evolving functions of endothelial cells in inflammation. Nat Rev Immunol 7:803–815
Quinn TP, Peters KG, De Vries C, Ferrara N, Williams LT (1993) Fetal liver kinase 1 is a receptor for vascular endothelial growth factor and is selectively expressed in vascular endothelium. Proc Natl Acad Sci USA 90:7533–7537
Randolph GJ, Angeli V, Swartz MA (2005) Dendritic-cell trafficking to lymph nodes through lymphatic vessels. Nat Rev Immunol 5:617–628
Religa P, Cao R, Bjorndahl M, Zhou Z, Zhu Z, Cao Y (2005) Presence of bone marrow-derived circulating progenitor endothelial cells in the newly formed lymphatic vessels. Blood 106:4184–4190
Ristimaki A, Narko K, Enholm B, Joukov V, Alitalo K (1998) Proinflammatory cytokines regulate expression of the lymphatic endothelial mitogen vascular endothelial growth factor-C. J Biol Chem 273:8413–8418
Rockson SG (2005) Lymphedema therapy in the vascular anomaly patient: therapeutics for the forgotten circulation. Lymphat Res Biol 3:253–255
Roesli C, Mumprecht V, Neri D, Detmar M (2008) Identification of the surface-accessible, lineage-specific vascular proteome by two-dimensional peptide mapping. FASEB J 22:1933–1944
Ryan TJ (1980) Microcirculation in psoriasis: blood vessels, lymphatics and tissue fluid. Pharmacol Ther 10:27–64
Saaristo A, Veikkola T, Tammela T, Enholm B, Karkkainen MJ, Pajusola K, Bueler H, Yla-Herttuala S, Alitalo K (2002) Lymphangiogenic gene therapy with minimal blood vascular side effects. J Exp Med 196:719–730
Sabin F (1902) On the origin of the lymphatic system from the veins and the development of the lymph hearts and thoracic duct in the pig. Am J Anat 1:367–391
Schacht V, Ramirez MI, Hong YK, Hirakawa S, Feng D, Harvey N, Williams M, Dvorak AM, Dvorak HF, Oliver G, Detmar M (2003) T1alpha/podoplanin deficiency disrupts normal lymphatic vasculature formation and causes lymphedema. EMBO J 22:3546–3556
Sebzda E, Hibbard C, Sweeney S, Abtahian F, Bezman N, Clemens G, Maltzman JS, Cheng L, Liu F, Turner M, Tybulewicz V, Koretzky GA, Kahn ML (2006) Syk and Slp-76 mutant mice reveal a cell-autonomous hematopoietic cell contribution to vascular development. Dev Cell 11:349–361
Shin JW, Min M, Larrieu-Lahargue F, Canron X, Kunstfeld R, Nguyen L, Henderson JE, Bikfalvi A, Detmar M, Hong YK (2006) Prox1 promotes lineage-specific expression of fibroblast growth factor (FGF) receptor-3 in lymphatic endothelium: a role for FGF signaling in lymphangiogenesis. Mol Biol Cell 17:576–584
Sholto-Douglas-Vernon C, Bell R, Brice G, Mansour S, Sarfarazi M, Child AH, Smith A, Mellor R, Burnand K, Mortimer P, Jeffery S (2005) Lymphoedema-distichiasis and FOXC2: unreported mutations, de novo mutation estimate, families without coding mutations. Hum Genet 117:238–242
Srinivasan RS, Dillard ME, Lagutin OV, Lin FJ, Tsai S, Tsai MJ, Samokhvalov IM, Oliver G (2007) Lineage tracing demonstrates the venous origin of the mammalian lymphatic vasculature. Genes Dev 21:2422–2432
Suri C, Jones PF, Patan S, Bartunkova S, Maisonpierre PC, Davis S, Sato TN, Yancopoulos GD (1996) Requisite role of angiopoietin-1, a ligand for the TIE2 receptor, during embryonic angiogenesis. Cell 87:1171–1180
Suzuki-Inoue K, Kato Y, Inoue O, Kaneko MK, Mishima K, Yatomi Y, Yamazaki Y, Narimatsu H, Ozaki Y (2007) Involvement of the snake toxin receptor CLEC-2, in podoplanin-mediated platelet activation, by cancer cells. J Biol Chem 282:25993–26001
Szuba A, Rockson SG (1997) Lymphedema: anatomy, physiology and pathogenesis. Vasc Med 2:321–326
Szuba A, Skobe M, Karkkainen MJ, Shin WS, Beynet DP, Rockson NB, Dakhil N, Spilman S, Goris ML, Strauss HW, Quertermous T, Alitalo K, Rockson SG (2002) Therapeutic lymphangiogenesis with human recombinant VEGF-C. FASEB J 16:1985–1987
Tabibiazar R, Cheung L, Han J, Swanson J, Beilhack A, An A, Dadras SS, Rockson N, Joshi S, Wagner R, Rockson SG (2006) Inflammatory manifestations of experimental lymphatic insufficiency. PLoS Med 3:e254
Tammela T, Enholm B, Alitalo K, Paavonen K (2005a) The biology of vascular endothelial growth factors. Cardiovasc Res 65:550–563
Tammela T, Saaristo A, Lohela M, Morisada T, Tornberg J, Norrmen C, Oike Y, Pajusola K, Thurston G, Suda T, Yla-Herttuala S, Alitalo K (2005b) Angiopoietin-1 promotes lymphatic sprouting and hyperplasia. Blood 105:4642–4648
Tammela T, Saaristo A, Holopainen T, Lyytikka J, Kotronen A, Pitkonen M, Abo-Ramadan U, Yla-Herttuala S, Petrova TV, Alitalo K (2007) Therapeutic differentiation and maturation of lymphatic vessels after lymph node dissection and transplantation. Nat Med 13:1458–1466
Taniguchi K, Kohno R, Ayada T, Kato R, Ichiyama K, Morisada T, Oike Y, Yonemitsu Y, Maehara Y, Yoshimura A (2007) Spreds are essential for embryonic lymphangiogenesis by regulating vascular endothelial growth factor receptor 3 signaling. Mol Cell Biol 27:4541–4550
Tobler NE, Detmar M (2006) Tumor and lymph node lymphangiogenesis–impact on cancer metastasis. J Leukoc Biol 80:691–696
Van Dyck F, Braem CV, Chen Z, Declercq J, Deckers R, Kim BM, Ito S, Wu MK, Cohen DE, Dewerchin M, Derua R, Waelkens E, Fiette L, Roebroek A, Schuit F, Van de Ven WJ, Shivdasani RA (2007) Loss of the PlagL2 transcription factor affects lacteal uptake of chylomicrons. Cell Metab 6:406–413
Wigle JT, Oliver G (1999) Prox1 function is required for the development of the murine lymphatic system. Cell 98:769–778
Wigle JT, Harvey N, Detmar M, Lagutina I, Grosveld G, Gunn MD, Jackson DG, Oliver G (2002) An essential role for Prox1 in the induction of the lymphatic endothelial cell phenotype. EMBO J 21:1505–1513
Wissmann C, Detmar M (2006) Pathways targeting tumor lymphangiogenesis. Clin Cancer Res 12:6865–6868
Young PE, Baumhueter S, Lasky LA (1995) The sialomucin CD34 is expressed on hematopoietic cells and blood vessels during murine development. Blood 85:96–105
Yuan L, Moyon D, Pardanaud L, Breant C, Karkkainen MJ, Alitalo K, Eichmann A (2002) Abnormal lymphatic vessel development in neuropilin 2 mutant mice. Development 129:4797–4806
Zhang Q, Lu Y, Proulx ST, Guo R, Yao Z, Schwarz EM, Boyce BF, Xing L (2007) Increased lymphangiogenesis in joints of mice with inflammatory arthritis. Arthritis Res Ther 9:R118
Author information
Authors and Affiliations
Corresponding author
Additional information
Research from the authors' laboratory is supported by National Institutes of Health grant CA69184, Swiss National Fund grant 3100A0-108207, Austrian Science Foundation grant S9408-B11, Cancer League Zurich, and Commission of the European Communities grant LSHC-CT-2005-518178 (M.D.).
Rights and permissions
About this article
Cite this article
Jurisic, G., Detmar, M. Lymphatic endothelium in health and disease. Cell Tissue Res 335, 97–108 (2009). https://doi.org/10.1007/s00441-008-0644-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00441-008-0644-2