
Abstract
CD33 and MS4A6A genes play potential key roles in the pathogenesis of Alzheimer’s disease (AD). One recent genome-wide association study has revealed that the rs3865444 polymorphism in the CD33 gene and rs610932 polymorphism in the MS4A6A gene are associated with susceptibility to AD in Caucasians. To evaluate the relationship between the polymorphism of the CD33, MS4A6A gene and AD in the ethnic Chinese Han, we conducted a case–control study (n = 383, age > 54) to determine the prevalence of single-nucleotide polymorphism of two genes in patients with AD in Chinese population of Mainland, and clarified whether these polymorphisms are risk factors for AD. The prevalence of the allele (T) in the rs3865444 polymorphism of the CD33 gene and allele (C) in rs610932 polymorphism of the MS4A6A gene was significantly different in AD patients and control subjects (P < 0.001, respectively), and the results were not influenced by age, gender, or APOE status. Our data revealed the allele (T) of the rs3865444 polymorphism of the CD33 gene and the allele (C) of the rs610932 polymorphism of the MS4A6A gene may contribute to AD risk in the Chinese Han population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Alzheimer’s disease (AD) is one of most common progressive neurodegenerative disease and the prevalence has grown rapidly over the past one century (Cornutiu 2011). To date, the pathogenetic mechanisms of AD are undetermined unfortunately, and the classical theory of amyloid hypothesis (Hardy 1997; Hardy and Higgins 1992) could be insufficient to explain the pathogenesis of AD. Recently, increasing studies have focused especially on dysfunction of the immune system in AD, and several key-genes involved the new mechanism are thought to association of the prevalence of AD(Corder et al. 1993; Bertram et al. 2007). Serial recent large genome-wide association studies (GWAS) have resulted in the identification of some novel loci (Naj et al. 2011; Hollingworth et al. 2011). Collectively, these genes now explain around 50% of late-onset Alzheimer's disease (LOAD) genetics and explore three new pathways including immune-system function, cholesterol metabolism, and synaptic cell membrane processes (Morgan 2011). In theory of immune-system dysfunction, the CD33 and MS4A6A gene was significantly associated with LOAD. The CD33 gene is thought to promote cell–cell interactions and regulate functions of cells in the innate and adaptive immune systems. By contrast, researchers found that the MS4A family gene over-expression can increase activation of T cells. However, the genetic analysis in population study was performed only in Caucasian population and has not been confirmed in other independent case–control population yet.
Therefore, we conducted a case–control study (n = 383, age > 54) to determine the prevalence of two single-nucleotide polymorphism (SNP) of CD33(rs3865444) and MS4A6A (rs610932) in patients with AD in Chinese Han population of mainland, and investigated the association between the polymorphism and AD. As APOE is the major susceptible gene for AD, we also analyzed the distribution of ε4 allele in both AD and control cohorts.
Materials and methods
Subjects
A total of 190 AD patients of Chinese Han ethnicity [104 women and 86 men; 73.1 ± 8.7 years old at the recruitment, Mini-Mental State Examination (MMSE) score, 16.7 ± 5.6] were enrolled from the outpatient clinic at the Department of Neurology, Ruijin Hospital affiliated to Shanghai Jiaotong University School of Medicine. All the subjects received a detailed neurological examination and underwent a psychiatric interview. The patients had a clinical diagnosis of probable dementia of Alzheimer type according to National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) (Dubois et al. 2007). One-hundred and ninety-three control subjects (102 women and 91 men; 71.4 ± 9.0 years old at the recruitment; MMSE score 27.8 ± 2.1) were matched for age, gender, and ethnic background. The components of male and female subjects do not vary significantly (P < 0.05) (Table 1). The non-demented elderly control (NEC) subjects were free of neurological or psychiatric disorders by medical history, physical examinations, laboratory examinations, and with MMSE score over 24 (Table 1). All AD-patients and NEC were unrelated Chinese Han. Informed consent for participation in the study was obtained either directly or from his or her guardian. The study was approved by the Research Ethics Committee, Ruijin Hospital affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Methods
DNA was isolated from peripheral blood through standardized phenol/chlorine extraction method. Genotyping analysis of APOE was performed as previously described (Corder et al. 1993). Primers and restriction enzymes were designed using the Primer software according to the RefSeq gene sequence of CD33 and MS4A6A. The CD33 rs3865444 genotype was determined by DNA amplification of a 421 bp fragment using the forward primer 5′-GCGAACCCCATGTCTAAA-3′ and the reverse primer 5′-CCTACCTCCCTCTGTGCC-3′. Polymerase chain reaction (PCR) was performed on 10 μl of reaction mixture (95°C for 5 min; followed by 35 cycles of 95°C for 30 s, an annealing step 51°C for 30 s, and 72°C for 25 s; with a final extension at 72°C for 10 min). The PCR products were stored at 4°C. After digestion overnight with NcoI (TaKaRa, Japan) at 37°C, the products were separated by 3% agarose electrophoresis. The MS4A6A rs610932 genotype was determined by DNA amplification of a 215 bp fragment using the forward primer 5′-CCCAGAAACATTTCCCAGAA-3′ and the reverse primer 5′-ATATGGGGCTTGCCTTTATG-3′. PCR was performed on 10 μl of reaction mixture (95°C for 5 min; followed by 35 cycles of 95°C for 30 s, an annealing step 61°C for 30 s, and 72°C for 25 s; with a final extension at 72°C for 10 min). The PCR products were stored at 4°C. After digestion overnight with NlaIII (BioLabs, NewEngland) at 37°C, the products were separated by 3% agarose electrophoresis.
Statistical analysis
Statistical analysis was performed with SPSS. Goodness-of-fit to the Hardy–Weinberg equilibrium (HWE) and differences in genotype and allele frequencies between AD and NEC groups were examined by Chi-squared analysis. Exact logistic regression was performed in the multivariate analysis to see whether age, gender and ApoEε4 status would influence the distribution of the CD33 and MS4A6A polymorphisms. The criterion for significance was set at p value <0.01 for all the tests.
Results
We analyzed a total of 190 patients diagnosed with AD and 193 unrelated gender- and age-matched controls in the present study (Table 1). Distributions of the CD33 and MS4A6A polymorphisms in both AD patients (CD33, P = 0.67; MS4A6A, P = 0.05) and controls (CD33, P = 0.11; MS4A6A, P = 0.06) were in HWE. Distributions of the APOE polymorphisms in both AD patients (P = 0.04) and controls (P = 0.64) approached HWE.
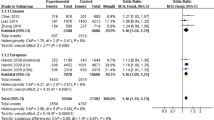
Table 2 showed both genotypic and allelic association for CD33, MS4A6A and APOE in the AD and NEC groups. As expected, the ApoE-4 allele frequencies were more significantly elevated in AD patients than in controls (OR = 0.352, 95% CI: 0.246–0.505, P < 0.001). Importantly, we found the minor alleles frequencies of rs3865444 (G > T) within CD33 were differently distributed in AD patients and NEC (OR = 0.480, 95% CI: 0.351–0.655, P < 0.001), rs610932 (A > C) within MS4A6A were differently distributed in AD patients and NEC (OR = 0.622, 95% CI: 0.467–0.827, P < 0.001), respectively, indicating that the rs3865444 and rs610932 polymorphism may be risk factors for AD. And there was still significant difference between AD patients and NEC in genotype and allele frequencies in rs3865444 and rs610932 polymorphism when these data stratified by the ApoE-4 status (Table 3).
Discussion
The amyloid hypothesis has been a significant theory in AD research since two decades and proposes that Aβ plays a key role in the neurodegenerative process which causes an imbalance between neurotoxic Aβ generation and clearance (Hardy and Higgins 1992). However, the classical theory could be insufficient to explain the pathogenesis of AD. Recently increasing researchers have given notice to alterations in the immune system of AD, such as the presence of circulating autoantibody and the proteins from the complement system in the cerebrum (Boche 2008). A growing number of studies have found the existence of specific anti-Aβ antibodies in the blood and cerebrospinal fluid (CSF) of AD patients (Du et al. 2001; Moir et al. 2005). This implies that, in a sense, the immune system is able of recognizing the proteins that aggregate in the cerebrum in AD as abnormal or “foreign” proteins that should be processed. When dysfunctions of this system, it could be promote the neurodegenerative process. In addition, one recent GWAS study provides a potential new evidence of the genetic pathogenesis (Naj et al. 2011; Hollingworth et al. 2011). It is striking that the two new susceptibility genes CD33 and MS4A6A are all implicated in immune-system function for AD (Morgan 2011).
The human CD33 gene is a member of the sialic-acid-binding immunoglobulin-like lectins (Siglec) family located on chromosome 19q13.3 (Crocker et al. 2007). Growing evidence suggests that the primary function of CD33-related Siglecs is to down-regulate host immune responses and set appropriate activation thresholds for regulating cellular-growth, survival and the production of soluble mediators (Cao and Crocker 2011). It is commend this kind of immunological regulation can prevent the microglial cleansing process of aggregating amyloid plaques in AD (Salminen and Kaarniranta 2009). Recent GWAS investigation from United States positioned rs3865444 polymorphism in CD33 as a risk factor for AD (Naj et al. 2011; Hollingworth et al. 2011). In our study, we found that the T allele frequency of rs3865444 in AD subjects was 39.5%. However, the T allele frequency within the control subjects was only 23.8%, which is significantly different from the AD subjects. Thus, we report for the first time, the significant association of the rs3865444 polymorphism in CD33 with an increased risk for AD in the ethnic Chinese Han (OR = 0.480, 95% CI: 0.351–0.655, P < 0.001). Moreover, we find that the significant difference in AD patients and controls was not influenced when these data were stratified by the ApoE-4 status.
MS4A genes including MS4A6A are clustered on chromosome 11q in humans (Liang et al. 2001) in a region with linkage to allergy and atopy (Sandford et al. 1995). The MS4A family includes at least 16 paralogues. Each gene has been probably generated by an ancestral cascade of intrachromosomal duplications during vertebrate evolution (Sandford et al. 1995). Regretfully, this gene family is poorly characterized, although a role in immunity has already been shown for several members of this cluster, including MS4A1 (CD20), MS4A2 and MS4A4B (Zuccolo et al. 2010). Howie D and his co-workers (2009) proposed that T cells preoccupied with immune-defense use the MS4A family to enhance sensitivity to extrinsic Ag stimulation, ensuring its elimination, while Tregs use these adaptors to allow low-level Ag signals to sustain regulatory function. Recent GWAS investigation from United States positioned rs610932 polymorphism in MS4A6A as a risk factor for AD (Naj et al. 2011; Hollingworth et al. 2011). We found that the C allele frequency of rs610932 in AD subjects was 58.7%. Whereas within the control subjects, the C allele frequency was only 46.9%, which is significantly different from the AD subjects. We found the significant association of the rs610932 polymorphism in MS4A6A with an increased risk for AD in the ethnic Chinese Han (OR = 0.622, 95% CI: 0.467–0.827, P = 0.001). Furthermore, we also find a significant difference in AD patients and controls when these data were stratified by the ApoE -4 status.
The polymorphism study of CD33, MS4A6A gene and AD is hypothesized that allele (T) of the rs3865444 polymorphism within CD33 gene and the allele (C) of the rs610932 polymorphism within MS4A6A gene may deteriorate the innate and adaptive immune systems which would increase accumulation of Aβ in the hippocampal and cortical areas of the brain. The hypothetical link between CD33, MS4A6a and AD would add new evidence in favor of the AD immune hypothesis, suggesting a role for the immune system in the pathogenesis of AD. Further research should focus on the detailed function of CD33 and MS4A6A in the pathogenesis of AD.
In summary, our study has identified variants at the CD33 and the MS4A6A gene associated with susceptibility to AD with replication over independent case–control samples. We indicate that the allele (T) of the rs3865444 polymorphism within CD33 gene and the allele (C) of the rs610932 polymorphism within MS4A6A gene may contribute to AD risk in the Chinese Han population. However, it is essential to confirm this finding in a much larger sample of Chinese population in future.
References
Bertram L, McQueen MB, Mullin K, Blacker D, Tanzi RE (2007) Systematic meta-analyses of Alzheimer disease genetic association studies: the AlzGene database. Nat Genet 39:17–23
Boche D, Nicoll ARJ (2008) The Role of the immune system in clearance of Ab from the brain. Brain Pathol 18:267–278
Cao H, Crocker PR (2011) Evolution of CD33-related siglecs: regulating host immune functions and escaping pathogen exploitation? Immunology 132(1):18–26. doi:10.1111/j.1365-2567.2010.03368.x (Epub 2010 Nov 11. Review)
Corder EH, Saunders AM, Strittmatter WJ et al (1993) Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 261:921–923
Cornutiu G (2011) The incidence and prevalence of Alzheimer’s disease. Neurodegener Dis 8(1–2):9–14 (Epub 2010 Aug 4)
Crocker PR, Paulson JC, Varki A (2007) Siglecs and their roles in the immune system. Nat Rev Immunol 7:255–266
Du Y, Dodel R, Hampel H, Buerger K, Lin S, Eastwood B et al (2001) Reduced levels of amyloid beta-peptide antibody in Alzheimer disease. Neurology 57:801–805
Dubois B, Feldman HH, Jacova C et al (2007) Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol 6:734–746
Hardy J (1997) Amyloid, the presenilins and Alzheimer’s disease. Trends Neurosci 20:154–159
Hardy JA, Higgins GA (1992) Alzheimer’s disease: the amyloid cascade hypothesis. Science 256(5054):184–185
Hollingworth P, Harold D, Sims R, Gerrish A, Lambert JC, Carrasquillo MM, Abraham R et al (2011) Common variants at ABCA7, MS4A6A/MS4A4E, EPHA1, CD33 and CD2AP are associated with Alzheimer’s disease. Nat Genet 43(5):429–435 (Epub 2011 Apr 3)
Howie D, Nolan KF, Daley S, Butterfield E, Adams E, Garcia-Rueda H, Thompson C, Saunders NJ, Cobbold SP, Tone Y, Tone M, Waldmann H (2009) MS4A4B is a GITR-associated membrane adapter, expressed by regulatory T cells, which modulates T cell activation. J Immunol 183(7):4197–4204 (Epub 2009 Sep 14)
Liang Y, Buckley TR, Tu L, Langdon SD, Tedder TF (2001) Structural organization of the human MS4A gene cluster on Chromosome 11q12. Immunogenetics 53:357–368
Moir RD, Tseitlin KA, Soscia S, Hyman BT, Irizarry MC, Tanzi RE (2005) Autoantibodies to redox-modified oligomeric Abeta are attenuated in the plasma ofAlzheimer’s disease patients. J Biol Chem 280:17458–17463
Morgan K (2011) Commentary: the three new pathways leading to Alzheimer’s disease. Neuropathol Appl Neurobiol. doi:10.1111/j.1365-2990.2011.01181.x (Epub ahead of print)
Naj AC, Jun G, Beecham GW, Wang LS, Vardarajan BN, Buros J, Gallins PJ et al (2011) Common variants at MS4A4/MS4A6E, CD2AP, CD33 and EPHA1 are associated with late-onset Alzheimer’s disease. Nat Genet 43(5):436–441 (Epub 2011 Apr 3)
Salminen A, Kaarniranta K (2009) Siglec receptors and hiding plaques in Alzheimer’s disease. J Mol Med 87(7):697–701 (Epub 2009 Apr 24)
Sandford AJ, Moffatt MF, Daniels SE, Nakamura Y, Lathrop GM et al (1995) A genetic map of chromosome 11q, including the atopy locus. Eur J Hum Genet 3:188–194
Zuccolo J, Bau J, Childs SJ, Goss GG, Sensen CW, Deans JP (2010) Phylogenetic analysis of the MS4A and TMEM176 gene families. PLoS ONE 5:e9369
Acknowledgments
This study was supported by the National Basic Research Development Program of China (No. 2010CB945200, 2011CB504104), National “Twelfth Five-Year” Plan for Science and Technology Support (No.2012BAI10B03), Shanghai Key Discipline Program (No.S30202), Shanghai Key Project of Basic Science Research (No. 09DZ1950400), Shanghai Natural Scientific Fund (No. 09JC1416402, 09ZR1419100), Shanghai Jiao Tong University Medical and engineering Joint Key Project (No.YG2010ZD102) and the Program for Outstanding Medical Academic Leader (No. LJ 06003).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Y.-L. Deng, L.-H. Liu contributed equally to this work.
Rights and permissions
About this article
Cite this article
Deng, YL., Liu, LH., Wang, Y. et al. The prevalence of CD33 and MS4A6A variant in Chinese Han population with Alzheimer’s disease. Hum Genet 131, 1245–1249 (2012). https://doi.org/10.1007/s00439-012-1154-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-012-1154-6