
Abstract
Atrial fibrillation (AF) affects more than 5 million people worldwide; however, none of the anti-arrhythmic drugs available now are entirely optimal in terms of efficacy and safety. A better understanding of the molecular mechanism of AF will facilitate the process of finding new strategies to prevent AF. As the non-familial AF is the major form of AF, identifying common variants for AF in these populations by genome-wide association studies will definitely accelerate this process. This review summarizes the recently identified common AF variants on 4q25, 16q22, and 1q21 and discusses their implications for the clinic.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Atrial fibrillation (AF), a ubiquitous yet diverse arrhythmia, is characterized by fast and irregular abnormal atrial electrophysiological activities with a prevalence of 1% in the general population (Xiao et al. 2010a, b, 2011a, b). Given AF’s strong association with aging, it affects more than 5% of the population over 65 years of age and increasing with age to 8% in those with age over 80 (Xiao et al. 2010a, b). AF affects over 5 million people worldwide and causes many complications, including heart failure and stroke, which greatly contributes to morbidity and mortality (Qi et al. 2009). Despite extensive research in exploring anti-arrhythmic therapy for AF, nothing that is currently available is optimal in terms of efficacy and safety (Xiao et al. 2010a, b, 2011a, b). Therefore, new strategies to prevent AF are highly desired (Xiao et al. 2010a, b). A better understanding of the molecular mechanism of AF will definitely facilitate this process (Xiao et al. 2011a, b; Cheng et al. 2010).
The first familial AF was reported in 1943 and after the first causal mutation in potassium voltage-gated channel, KQT-like subfamily, member 1 (KCNQ1) for AF was identified in 2003 by Chen et al., at least 17 causal mutations have been identified (Table 1). Although the identified mutations in familial AF have provided great insights into the molecular mechanisms of AF, as the familial AF only accounts for a small fraction of AF patients, they might not be representative of pathogenesis in the more common, non-familial form of AF (Xiao et al. 2011a, b; Gudbjartsson et al. 2007). The common variants recently identified by genome-wide association studies in common AF are relatively of broad interest (Gudbjartsson et al. 2007). Here we have highlighted and discussed recent advances in identifying common variants of AF by genome-wide association studies (Table 2). The locus of these 17 causal mutations and 3 common variants are indicated in Fig. 1.

Locus of variants for atrial fibrillation
Common variants on 4q25
Gudbjartsson et al., for the first time, performed a genome-wide association study by the Illumina Hap300 BeadChip in 550 AF and/or atrial flutter (AFl) patients and 4,476 controls from Iceland. They identified a strong association between two sequence variants (rs2200733 and rs2220464) on chromosome 4q25 and AF and these associations were replicated in an additional Icelandic sample consisting of 2,251 AF/AFl patients and 13,238 healthy controls and two populations of European ancestry, one from Sweden, consisting of 143 AF/AFl cases and 738 controls, and the other from the United States, consisting of 636 AF/AFl cases and 804 controls (Gudbjartsson et al. 2007). Finally, they replicated the association in a Chinese population consisting of 333 AF/AFl cases and 2,836 controls (Gudbjartsson et al. 2007). Later on, Kaab et al. replicated these associations in four independent cohorts from the Framingham Heart Study, the Rotterdam Study, the Vanderbilt AF Registry, and the German AF Network. They found that rs2200733 was associated with AF in all four cohorts, but rs10033464 was only confirmed in the Framingham Heart Study and Vanderbilt AF Registry. Meta-analyses of the relations between AF and rs2200733 or rs10033464 in all available case–control studies provided an odd ratio (OR) of 1.90 for rs2200733 and 1.36 for rs10033464 (Kaab et al. 2009). Anselmi et al. (Anselmi et al. 2008) also validated a positive, significant association between the rs2200733 T allele and patients with AF/AFl in Italian origin. In addition, Lee et al. examined the genotypes of five single-nucleotide polymorphisms (SNPs), rs2634073, rs2200733, rs13143308, rs2220427 and rs10033464 in a Taiwanese population composed of 200 AF patients and 158 healthy controls using multiplex single base extension methods. They confirmed the association between rs2200733 and AF, but failed to confirm the association between rs10033464 and AF (Lee et al. 2010). In sum, these studies consistently showed the association between rs2200733 and AF but not with rs10033464.
Shi et al. (Shi et al. 2009) also carried out a case–control study with AF patients and non-AF controls to confirm the association of rs2200733 on chromosome 4q25 with AF in a Chinese Han population. They confirmed a significant association with OR = 1.81 between rs2200733 and AF (Shi et al. 2009). Interestingly, when the AF cases in their study were divided into lone AF (32.6%) and other types of AF (67.4%), a significantly stronger association with lone AF compared to other types of AF was observed. This suggests that the influence of genetic factors might be much stronger in lone AF than in other types of AF and that rs2200733 confers a stronger risk in populations with lone AF than in populations with other types of AF (Shi et al. 2009).
Lubitz et al. (Lubitz et al. 2010) genotyped 34 SNPs at chromosome 4q25 in 790 AF patients and 1,177 controls from Massachusetts General Hospital and tested their associations with AF. They identified two novel susceptibility signals marked by rs17570669 and rs3853445 after adjustment for rs2200733, a well-known AF common variant. These associations were also confirmed in 5,066 AF case and 30,661 controls from the German Competence Network for AF, Atherosclerosis Risk in Communities Study, Cleveland Clinic Lone AF Study, Cardiovascular Health Study, and Rotterdam Study (Lubitz et al. 2010). However, as all subjects in their study were of European ancestry, whether these two SNPs could be validated in other ancestries is yet to be confirmed.
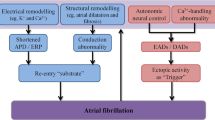
No known gene is present in the linkage disequilibrium (LD) block containing the common variants identified above (Gudbjartsson et al. 2007). The paired-like homeodomain 2 (Pitx2) gene located in the adjacent upstream LD block is the closest gene to these risk variants (Gudbjartsson et al. 2007). Pitx2 has been found to be necessary for the development of the pulmonary myocardium, or the sleeve of cardiomyocytes extending from the left atrium into the initial portion of the pulmonary vein (Gudbjartsson et al. 2007; Sinner et al. 2011). Interestingly, trigger activities from pulmonary veins play a critical role in initiating and maintaining AF, indicating that Pitx2 might play a role in the genesis of AF (Sinner et al. 2011). Recently, Wang et al. found that Pitx2 null ± adult mice had atrial arrhythmias, including AFl and atrial tachycardia, supporting that Pitx2 haploinsufficiency causes a predisposition to atrial arrhythmias (Wang et al. 2010). Using the mRNA microarray, they found that the sinoatrial node (SAN)-genes Shox2 and Tbx3, as well as many other channel genes, were up-regulated in the Pitx2 null-mutant embryos when compared with controls, indicating a Shox2-mediated mechanism (Wang et al. 2010). They also found that KCNQ1, a potassium channel gene that has been implicated in familial AF through a gain-of-function mutation was up-regulated (Wang et al. 2010; Chen et al. 2003). In addition, they found that atrial natriuretic peptide, NPPA, a protein identified within atrial myocardium of AF patients through a gain-of-function mutation was up-regulated (Wang et al. 2010; Hodgson-Zingman et al. 2008). The potential mechanisms are indicated as Fig. 2. These results indicate that Pitx2 likely has multiple targets that are relevant to the predisposition to atrial arrhythmia (Wang et al. 2010). Recently, Pitx2c expression has been reported to be decreased in human patients with sustained AF (Chinchilla et al. 2011); however, there is still no direct evidence that the variants associated with AF lead to a reduction in Pitx2c in the human heart. As Pitx2c is mainly expressed in the adult left atrium (Kirchhof et al. 2011), it would be urgent to collect left atrium samples from AF patients and conduct further studies to solve this issue.

Potential mechanisms for the increased susceptibility to AF in Pitx2null ± adult mice NPPA natriuretic peptide A, KCNQ1 KQT-like subfamily, member 1
Common variants on 16q22
After identifying the common variants in 4q25, Gudbjartsson et al. (Gudbjartsson et al. 2009) expanded their genome-wide association study on AF in Iceland and found a variant (rs7193343) on chromosome 16q22 significantly associated with AF. Later on, Benjamin et al. (Benjamin et al. 2009) found that rs2106261 on chromosome 16q22 was associated with AF. Li et al. tried to explore whether the above two variants could be expanded to a different ethnic population (Li et al. 2011). They confirmed a significant association between rs2106261 and AF in a Chinese Han cohort consisting of 650 AF patients and 1,447 non-AF controls, providing a cross-race susceptibility of the 16q22 AF locus (Li et al. 2011).
The variants identified on 16q22 located in the zinc finger homeobox 3 (ZFHX3) gene, have been found to play a role in the regulation of cell growth and differentiation in several tissues, including neuron and skeletal muscle (Gudbjartsson et al. 2009; Benjamin et al. 2009). ZFHX3 encodes an AT motif-binding factor 1, which is required for early transcriptional activation of the Pituitary-specific positive transcription factor 1 (POU1F1) (Gudbjartsson et al. 2009; Benjamin et al. 2009). Interestingly, POU1F1 has been found to interact with Pitx2 (Benjamin et al. 2009; Quentien et al. 2010), which is of interest because it is the nearest gene to the previously identified AF variants on chromosome 4q25. A schematic of the interaction of ZFHX3 with Pitx2 is showed in Fig. 3.

A schematic of the interaction of ZFHX3 with Pitx2 ZFH3 zinc finger homeobox 3, POU1F1 pituitary-specific positive transcription factor 1, Pitx2 paired-like homeodomain 2 gene
Common variants on 1q21
Ellinor et al. (Ellinor et al. 2010) identified the association of rs13376333 on chromosome 1q21 to lone AF with an OR = 1.56 from 1,335 lone AF patients and 12,844 unaffected controls from the German AF Network, Heart and Vascular Health Study, the Atherosclerosis Risk in Communities Study, the Cleveland Clinic and Massachusetts General Hospital. This variant is located in the intron between the first and second exon of the potassium intermediate/small conductance calcium-activated channel, subfamily N, member 3 (KCNN3), which encodes a member of a family of voltage-independent calcium-activated potassium channel proteins involved in atrial repolarization (Ellinor et al. 2010). However, there is still no direct evidence indicating that the variants associated with AF lead to a reduction in KCNN3 in the human heart. Blocking of KCNN channels pharmacologically has been found to inhibit pacing-induced shortening of pulmonary venous and atrial action potential duration (APD) in rabbit and it is well-known that APD shortening could reduce the refractory period in atrial myocytes and promotes re-entry, which is an important mechanism for the development and maintenance of AF (Xiao et al. 2011a, b; Ellinor et al. 2010).
Implications for the clinic
Although the common variants identified by recent genome-wide association studies indicate promising novel molecular pathways for AF, the translation into drug development has not yet occurred (Xiao et al. 2011a, b). These common variants, however, have shown great potential in risk prediction, assessment of outcomes, and response to therapies for AF (Fig. 4) (Xiao et al. 2011a, b).

A paradigm for the translation of information of AF’s common variants into clinical practice AF atrial fibrillation, CABG coronary artery bypass graft surgery
Gretarsdottir et al. (Gretarsdottir et al. 2008) genotyped 1,661 Icelandic ischemic stroke patients and 10,815 healthy controls using the Infinium HumanHap300 chip and replicated the most significant signals in two large European ischemic stroke sets composed by 2,224 ischemic stroke patients and 2,583 healthy controls. They discovered that rs2200733 and rs10033464, two common variants previously associated with AF, significantly associate with ischemic stroke, with the strongest risk for cardioembolic stroke (Gretarsdottir et al. 2008). Their study indicated that these variants on chromosome 4q25 might be utilized for identification of subgroups of stroke patients that may benefit from additional efforts to detect AF (Gretarsdottir et al. 2008). However, Lemmens et al. reported that the association of the 4q25 susceptibility variant for AF with stroke was limited to stroke of cardioembolic etiology by performing a large case–control association study in 4,199 ischemic stroke patients and 3,750 controls from 6 studies conducted in Australia, Austria, Belgium, Poland, Spain, and Sweden (Lemmens et al. 2010). Because the genotyping of these variants has become commercially available, whether patients with stroke of cryptogenic etiology should be offered genetic testing deserves further examination by performing larger association study of people of more diverse ancestries (Lemmens et al. 2010).
AF is among the most common adverse events after cardiac surgery, with an estimated incidence of 27–40% (Body et al. 2009). Body et al. (Body et al. 2009) found that variations (rs2200733, and rs13143308) in 4q25 could predict postoperative AF after coronary artery bypass graft (CABG) surgery in two independently cardiac surgery cohorts. They defined postoperative AF as the occurrence of AF identified from physician, nursing, or perioperative ECG records, during the postoperative time of primary hospitalization, or the duration of contiguous hospitalization in the institution where the surgery was conducted. The discovery cohort was comprised of 1,583 patients from the CABG Genomics Program and the validation cohort was composed of 1,288 patients from the VCRS. However, the previous association of rs10033464 with AF in ambulatory populations was not seen for postoperative AF (Body et al. 2009). Their study indicated that AF after CABG risk prediction might be improved by the incorporation of genetic findings. Recently, Virani et al. performed genotyping for rs2200733 and rs10033464 on 4q25 in 1,166 white participants from the TexGen genetic registry. They found that both variants were associated with postoperative AF with odds ratios of 1.41 and 1.47, respectively (Virani et al. 2011). These findings are consistent with the report from Body et al. (Body et al. 2009). They also found that the two variants were also associated with long-term AF with hazard ratios of 1.32 and 1.28, respectively. Based on the results of the above two studies, we can conclude that using these common variants can predict the short-term risk of AF after CABG surgery and as well as the long-term AF risk. Using this information, one might like to plan the post-surgery management by, for example, defining those at high risk of postoperative AF and trying to identify and treat them at an early stage. Husser et al. (Husser et al. 2010) genotyped the two common variants including rs2200733 and rs10033464) in 195 consecutive patients with drug-refractory paroxysmal or persistent AF who underwent AF catheter ablation. All participants in their study were followed up for 6 months. Seven-day Holter recordings were conducted immediately after the ablation and at 3 and 6 months after the ablation. Early recurrence of AF was defined as an AF episode during the first 7 days after the ablation and late recurrence of AF was defined as any AF episode between 3 and 6 months after the ablation. They found that the presence of any variant allele increased the risk for both early recurrence of AF (OR 1.994) and late recurrence of AF (OR 4.182) (Husser et al. 2010). Their study points to a potential role for these common variants in stratification of AF ablation therapy or peri-interventional management. This information could be used to predict the risk or anticipated success rate before the procedure and to plan the ablation strategy and post-ablation management accordingly. In short, common variants of AF have showed great potential in outcomes assessment and therapies response determination (Xiao et al. 2011a, b).
In conclusion, several common variants have been identified on the 4q25, 16q22, and 1q21 chromosomes. These common variants provided novel molecular pathways for AF. Rarely does such an opportunity arise to use these common variants for risk prediction, assessment of outcomes, or response to therapies for AF.
References
Anselmi CV, Novelli V, Roncarati R et al (2008) Association of rs2200733 at 4q25 with atrial flutter/fibrillation diseases in an Italian population. Heart 94:1394–1396
Benjamin EJ, Rice KM, Arking DE et al (2009) Variants in ZFHX3 are associated with atrial fibrillation in individuals of European ancestry. Nat Genet 41:879–881
Bhuiyan ZA, van den Berg MP, van Tintelen JP et al (2007) Expanding spectrum of human RYR2-related disease: new electrocardiographic, structural, and genetic features. Circulation 116:1569–1576
Body SC, Collard CD, Shernan SK et al (2009) Variation in the 4q25 chromosomal locus predicts atrial fibrillation after coronary artery bypass graft surgery. Circ Cardiovasc Genet 2:499–506
Brugada R, Hong K, Dumaine R et al (2004) Sudden death associated with short-QT syndrome linked to mutations in HERG. Circulation 109:30–35
Chen YH, Xu SJ, Bendahhou S et al (2003) KCNQ1 gain-of-function mutation in familial atrial fibrillation. Science 299:251–254
Cheng Y, Zhan Q, Zhao J, Xiao J (2010) Stabilizing ryanodine receptor type 2: a novel strategy for the treatment of atrial fibrillation. Med Sci Monit 16:HY23–HY26
Chinchilla A, Daimi H, Lozano-Velasco E et al (2011) Pitx2 insufficiency leads to atrial electrical and structural remodeling linked to arrhythmogenesis. Circ Cardiovasc Genet 4:269–279
Ellinor PT, Nam EG, Shea MA, Milan DJ, Ruskin JN, MacRae CA (2008) Cardiac sodium channel mutation in atrial fibrillation. Heart Rhythm 5:99–105
Ellinor PT, Lunetta KL, Glazer NL et al (2010) Common variants in KCNN3 are associated with lone atrial fibrillation. Nat Genet 42:240–244
Gollob MH, Jones DL, Krahn AD et al (2006) Somatic mutations in the connexin 40 gene (GJA5) in atrial fibrillation. N Engl J Med 354:2677–2688
Gretarsdottir S, Thorleifsson G, Manolescu A et al (2008) Risk variants for atrial fibrillation on chromosome 4q25 associate with ischemic stroke. Ann Neurol 64:402–409
Gudbjartsson DF, Arnar DO, Helgadottir A et al (2007) Variants conferring risk of atrial fibrillation on chromosome 4q25. Nature 448:353–357
Gudbjartsson DF, Holm H, Gretarsdottir S et al (2009) A sequence variant in ZFHX3 on 16q22 associates with atrial fibrillation and ischemic stroke. Nat Genet 41:876–878
Hodgson-Zingman DM, Karst ML, Zingman LV et al (2008) Atrial natriuretic peptide frameshift mutation in familial atrial fibrillation. N Engl J Med 359:158–165
Hong K, Piper DR, Diaz-Valdecantos A et al (2005) De novo KCNQ1 mutation responsible for atrial fibrillation and short QT syndrome in utero. Cardiovasc Res 68:433–440
Husser D, Adams V, Piorkowski C, Hindricks G, Bollmann A (2010) Chromosome 4q25 variants and atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol 55:747–753
Kaab S, Darbar D, van Noord C et al (2009) Large scale replication and meta-analysis of variants on chromosome 4q25 associated with atrial fibrillation. Eur Heart J 30:813–819
Kirchhof P, Kahr PC, Kaese S et al (2011) Pitx2c is expressed in the adult left atrium, and reducing pitx2c expression promotes atrial fibrillation inducibility and complex changes in gene expression. Circ Cardiovasc Genet 4:123–133
Lee KT, Yeh HY, Tung CP et al (2010) Association of RS2200733 but not RS10033464 on 4q25 with atrial fibrillation based on the recessive model in a Taiwanese population. Cardiology 116:151–156
Lemmens R, Buysschaert I, Geelen V et al (2010) The association of the 4q25 susceptibility variant for atrial fibrillation with stroke is limited to stroke of cardioembolic etiology. Stroke 41:1850–1857
Li C, Wang F, Yang Y et al (2011) Significant association of SNP rs2106261 in the ZFHX3 gene with atrial fibrillation in a Chinese Han GeneID population. Hum Genet 129:239–246
Lubitz SA, Sinner MF, Lunetta KL et al (2010) Independent susceptibility markers for atrial fibrillation on chromosome 4q25. Circulation 122:976–984
Makiyama T, Akao M, Shizuta S et al (2008) A novel SCN5A gain-of-function mutation M1875T associated with familial atrial fibrillation. J Am Coll Cardiol 52:1326–1334
Olson TM, Michels VV, Ballew JD et al (2005) Sodium channel mutations and susceptibility to heart failure and atrial fibrillation. Jama 293:447–454
Olson TM, Alekseev AE, Liu XK et al (2006) Kv1.5 channelopathy due to KCNA5 loss-of-function mutation causes human atrial fibrillation. Hum Mol Genet 15:2185–2191
Olson TM, Alekseev AE, Moreau C et al (2007) KATP channel mutation confers risk for vein of Marshall adrenergic atrial fibrillation. Nat Clin Pract Cardiovasc Med 4:110–116
Postma AV, van de Meerakker JB, Mathijssen IB et al (2008) A gain-of-function TBX5 mutation is associated with atypical Holt-Oram syndrome and paroxysmal atrial fibrillation. Circ Res 102:1433–1442
Qi J, Xiao J, Zhang Y et al (2009) Effects of potassium channel blockers on changes in refractoriness of atrial cardiomyocytes induced by stretch. Exp Biol Med (Maywood) 234:779–784
Quentien MH, Vieira V, Menasche M et al (2010) Truncation of PITX2 differentially affects its activity on physiological targets. J Mol Endocrinol 46:9–19
Ravn LS, Aizawa Y, Pollevick GD et al (2008) Gain of function in IKs secondary to a mutation in KCNE5 associated with atrial fibrillation. Heart Rhythm 5:427–435
Shi L, Li C, Wang C et al (2009) Assessment of association of rs2200733 on chromosome 4q25 with atrial fibrillation and ischemic stroke in a Chinese Han population. Hum Genet 126:843–849
Sinner MF, Ellinor PT, Meitinger T, Benjamin EJ, Kaab S (2011) Genome-wide association studies of atrial fibrillation: past, present, and future. Cardiovasc Res 89:701–709
Thibodeau IL, Xu J, Li Q et al (2010) Paradigm of genetic mosaicism and lone atrial fibrillation: physiological characterization of a connexin 43-deletion mutant identified from atrial tissue. Circulation 122:236–244
Virani SS, Brautbar A, Lee W et al (2011) Usefulness of single nucleotide polymorphism in chromosome 4q25 to predict in-hospital and long-term development of atrial fibrillation and survival in patients undergoing coronary artery bypass grafting. Am J Cardiol 107:1505–1509
Wang J, Klysik E, Sood S, Johnson RL, Wehrens XH, Martin JF (2010) Pitx2 prevents susceptibility to atrial arrhythmias by inhibiting left-sided pacemaker specification. Proc Natl Acad Sci USA 107:9753–9758
Watanabe H, Darbar D, Kaiser DW et al (2009) Mutations in sodium channel beta1- and beta2-subunits associated with atrial fibrillation. Circ Arrhythm Electrophysiol 2:268–275
Xia M, Jin Q, Bendahhou S et al (2005) A Kir2.1 gain-of-function mutation underlies familial atrial fibrillation. Biochem Biophys Res Commun 332:1012–1019
Xiao J, Liang D, Zhao H et al (2010a) 2-Aminoethoxydiphenyl borate, a inositol 1, 4, 5-triphosphate receptor inhibitor, prevents atrial fibrillation. Exp Biol Med (Maywood) 235:862–868
Xiao J, Zhang H, Liang D et al (2010b) Taxol, a microtubule stabilizer, prevents atrial fibrillation in in vitro atrial fibrillation models using rabbit hearts. Med Sci Monit 16:BR353–BR360
Xiao JJ, Liang DD, Chen YH (2011) The genetics of atrial fibrillation: from the bench to the besides. Annu Rev Genomics Hum Genet 12:6.1–6.24
Xiao J, Liang D, Zhang Y, et al. (2011) MicroRNA expression signature in atrial fibrillation with mitral stenosis. Physiol Genomics 43:655–664
Yang Y, Xia M, Jin Q et al (2004) Identification of a KCNE2 gain-of-function mutation in patients with familial atrial fibrillation. Am J Hum Genet 75:899–905
Zhang DF, Liang B, Lin J, Liu B, Zhou QS, Yang YQ (2005) KCNE3 R53H substitution in familial atrial fibrillation. Chin Med J (Engl) 118:1735–1738
Zhang X, Chen S, Yoo S et al (2008) Mutation in nuclear pore component NUP155 leads to atrial fibrillation and early sudden cardiac death. Cell 135:1017–1027
Acknowledgments
This work was supported by the Shanghai Municipal Natural Science Foundation (10ZR1433100, to Xingyuan Liu).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding authors
Additional information
X. Liu, F. Wang, J. Xiao and J. Zhao contributed equally to this work.
Rights and permissions
About this article
Cite this article
Liu, X., Wang, F., Knight, A.C. et al. Common variants for atrial fibrillation: results from genome-wide association studies. Hum Genet 131, 33–39 (2012). https://doi.org/10.1007/s00439-011-1052-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-011-1052-3