
Abstract
It has been claimed that infectious agents transmitted by mosquitoes (Diptera: Culicidae) may have a greater connection to cancer then hitherto supposed and that the immune system struggles to recognize and fight some of these infectious agents. One of the claims made is that there is a connection between human malaria and brain cancers in the USA. However, the USA declared itself free of human malaria in the last century, yet cancer incidences remain high, suggesting any overall cancer connection is slight. Two fundamental questions arise from the possible mosquito-cancer connection. Firstly, if mosquitoes are able to vector some pathogens and parasites linked with cancer pathogenesis, why has the fact not been discovered decades ago? Secondly, if there is a connection (other than in relation to Burkett’s lymphoma), what is its extent? The answers may well lie with the various types of malarias known to exist. The discovery in humans of the simian malaria, caused by Plasmodium knowlesi, suggests that other forms of simian or even avian malaria may be capable of survival in humans, albeit at low levels of parasitemia, and humans may be a dead-end host. Other carcinogenic infectious agents transmitted by mosquitoes may also go undetected because either no one is looking for them, or they are looking in wrong anatomical locations and/or with inadequate tools. Research on false negative test results with respect to many infectious agents is sadly lacking, so its extent is unknown. However, electronic and other media provide numerous instances of patients failing to be diagnosed for both human malaria and Lyme’s disease, to take just two examples. This review suggests that to shed light on a potential mosquito-cancer connection, more research is required to establish whether other simian and avian forms of malaria play a part. If so, then they potentially provide unique markers for early cancer detection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
What is really known about mosquito-biting activity and cancer?
Current knowledge on the potential relationship between the spread of cancer and mosquito-borne diseases, with special reference to malaria, is strictly limited (Benelli et al. 2016; Ward et al. 2016). Lehrer (2010a) reported an association between malaria and cancer incidence, based on data sets from 1994, arguing that this may be linked to Plasmodium-triggered suppression of the human immune system. In addition, it has been supposed that Anopheles mosquitoes may be able to vector poorly known viruses, which may be potentially responsible for cancer development (Lehrer 2010b; Benelli 2016). Besides these observations on anopheline, there are some interesting findings also on aedine vectors. Indeed, it has been outlined that Aedes aegypti feeding activity may transfer tumor cells of hamster reticulum cell sarcoma (Banfield et al. 1965, 1966).
Human malaria’s implication in US cancers: a dead end?
However, despite the interesting analysis by Lehrer (2010a,b), in 2016, the USA Centers for Disease Control and Prevention (CDC) declared that US malaria cases had reached a 40-year high of 1925 in 2011 and that malaria had basically been eliminated for decades. The latest figures on US cancer from the CDC are for 2013 when 1,536,119 cases were diagnosed, 584,872 people died and 1 in 4 deaths were attributed to cancer. These figures suggest that human malaria’s implication in present day US cancers has met a dead end. Furthermore, cancers arise in many other countries that have eradicated malaria. What then is driving the large number of present cancer cases? Malaria is only one disease out of many that are attributable to mosquitoes (Benelli 2015; Mehlhorn 2015; Benelli and Mehlhorn 2016), and the latter are still being linked to cancer through their known ability to carry carcinogenic viruses and parasites, many of which can evade immune control (Johansson and Ward 2016; Benelli et al. 2016; Ward et al. 2016).
Simian and avian malaria, overlooked in humans, may still be present?
Zoonoses are recognized to be responsible for 60% of emerging infectious diseases (Jones et al. 2008), and the simian Plasmodium knowlesi has been shown to infect humans and is commonly misdiagnosed as benign Plasmodium malariae (Cox-Singh et al. 2008). Unknown lineages of simian Plasmodium to which humans may be susceptible have recently been reported (Krief et al. 2010). This raises the intriguing possibility that other forms of malaria, for example avian ones, may, contrary to previously accepted opinion, be capable of survival in humans. Indeed, generally accepted opinion may be a myth, due to unreliable tests in the past failing to detect either simian or avian malaria in humans, or that low levels of parasitemia have been found and deemed to have no known adverse health consequences and that humans are dead-end hosts.
If it can be proven that different forms of avian malaria can survive in humans, it would add strength to the argument that cancers may be more intricately connected with mosquitoes than supposed. Avian malaria parasites have a worldwide distribution except for Antarctica (Braga et al. 2011). While no mosquito species are present in Iceland, cancers there may be partially due to mosquito-biting activity experienced abroad. These other “non-human” malarias may be non-virulent strains behaving as innocent bystanders or guilty in a way yet to be determined and proven. Mosquito viruses are present in healthy UK birds but are either non-virulent or the birds have developed herd immunity, as they show no clinical signs of infection (Buckley et al. 2003). If such malarias are present, but asymptomatic in humans, should we be concerned or interested? We would argue yes, because not only would their discovery enable an assessment of the percentage of total cancers attributable to mosquitoes to be made, but also hold out the prospect of a single universal cancer test. In addition, if avian or simian malaria are involved in an active way with cancer, then it would need to be screened for in blood donors (Allain et al. 2009; Dodd 2010).
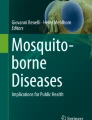
It is known that mosquito species carrying, or capable of being bridge vectors for both simian and avian malaria, can not only bite humans but give them serious infections. For example, Culex mosquitoes infected with Plasmodium relictum killed birds, horses, and humans through transmission of West Nile virus (Fig. 1) (Spielman and D’Antonio 2001 p. 184; Buckley et al. 2003; Hughes et al. 2010; Petersen et al. 2013). West Nile viruses can be designated into five phylogenetic lineages with sub-lineages, and new genotypes may increase efficiency and rapidity of viral transmission in mosquito vectors. Most human patients with West Nile virus-related illnesses are unrecognized clinically, with a study showing only 58% of patients had a positive MAC-ELISA result at clinical presentation (Petersen et al. 2013). Seasonality also has an effect with different Plasmodium species varying asynchronously across the season in mosquitoes and birds (Medeiros et al. 2016).

The potential connection between mosquito-biting activity and cancer remains debated. International Agency for Research on Cancer highlighted that infection by P. falciparum in holoendemic areas is “probably carcinogenic to humans” and placed it in “Group 2A.” The discovery in humans of simian malaria, caused by Plasmodium knowlesi, suggests that other forms of simian or even avian malaria may be capable of survival in humans, albeit at low levels of parasitemia, and humans may be a dead-end host. Other carcinogenic infectious agents transmitted by mosquitoes may also go undetected. Here, a under a magnification of ×1125, is a mature simian malarial schizont and gametocyte in simian blood (photo credit: Dr. W.A. Rogers, Jr., Centers for Disease Control and Prevention, PHIL). b Giemsa-stained blood smear from a bird infected with P. relictum: intracellular parasites (indicated by arrows) develop within nucleated red blood cells, potentially leading to anemia (photo credit: U.S. Geological Survey—Biological Resources Division, courtesy of Global Invasive Species Database, ISSG). c Two developing oocysts containing densely packed sporozoites (indicated by arrows) of P. relictum on the stomach wall of Culex quinquefasciatus, which at maturation will invade mosquito salivary glands, being vectors to other vertebrate hosts during further mosquito-biting activity (photo credit: U.S. Geological Survey—Biological Resources Division, courtesy of Global Invasive Species Database, ISSG)
In this scenario, the present review examines the possibility of non-human malarias being sustained in humans, without recognition and identification, as well as possible reasons why infectious agents linked with cancer may be under-reported. It considers whether there is a standard cancer-seeking protocol that looks for such infectious agents, whether any tests used for detection are prone to false negatives, particularly if such tests as are used are based on cost (both with respect to labor and equipment) rather than superior and more expensive detection tests. Our review continues with a brief look at the history of malaria. Then, we provide an examination of past and current detection methods for class 1 carcinogenic infectious agents, followed by conclusions and challenges for a future research agenda.
A brief history of Plasmodium: overlooked issues
The origin of human Plasmodium has been debated extensively, being attributed at different times to both avian and simian sources, with hypotheses that Plasmodium species switch from birds to African great apes and vice versa (Waters et al. 1991; Cox 2010; Prugnolle et al. 2011; Pick et al. 2011; Perkins 2014; Molina-Cruz et al. 2016). Although regarded as unusual, Culiseta melanura can transport malaria agents from a bird reservoir to the human bloodstream (Spielman and D’Antonio 2001 p. 109). Furthermore, within human malaria, there are numerous slightly different strains; therefore, travellers from one district may have immunity against the strain in their local environment, while they can be infected as soon as they encounter a neighboring strain (Spielman and D’Antonio 2001, p. 168).
Notably, our knowledge of human malaria is still expanding, as recently as 2010, it was proposed that Plasmodium ovale comprises two non-recombining species and that morbidity caused by it has been underestimated (Sutherland et al. 2010). For some time, only four Plasmodium species have been associated with human malaria, namely P. malariae, Plasmodium vivax, P. ovale, and Plasmodium falciparum. However, in this century, the simian malaria agent P. knowlesi has been added to this list. Rare malarial cases have been linked with the presence of Plasmodium cynomolgi, and there is possible transmission to humans of Plasmodium bastianelli, Plasmodium inui, Plasmodium rodiani, Plasmodium schwetzi, Plasmodium semiovale, Plasmodium simium, and Plasmodium eylesi (Ta et al. 2014).
With over 3000 known species/subspecies of mosquitoes, it would seem quite possible that further forms of Plasmodium could exist in humans, and remain unidentified, particularly if the human host remains asymptomatic. Tests for avian and simian malaria are constantly evolving (Richard et al. 2002; Ta et al. 2014). More recently, loop-mediated isothermal amplification tests have increased accuracy, reduced testing costs and time for human malaria diagnosis (Bousema and Drakeley 2011). It has recently been shown that tests for identification of avian Plasmodium may produce false negatives in birds due to different elution protocols (Niebuhr and Blasco-Costa 2016). Parasite genetic information obtained from cultures is likely to be different from the natural infection parasites (Yeda et al. 2016). General PCR protocols may favor detection of parasites with higher parasitemia, and sensitivity of different PCR assays in detection of mixed infections has been insufficiently tested (Zehtindjiev et al. 2012; Bernotiene et al. 2016). It would be realistic, therefore, to assume any tests for the presence of avian Plasmodium in humans may have produced false negatives for the same reason. However, a Medline search for humans actually being tested for avian Plasmodium failed to produce any evidence. This is perhaps not surprising as over 50 species of avian Plasmodium have been identified and diversity is greater than realized (Njabo et al. 2009; Outlaw et al. 2016). P. knowlesi and P. cynomolgi, both agents of simian malaria, have been detected in humans and are commonly misidentified (Vythilingam et al. 2008; Cox-Singh et al. 2008; Ta et al. 2014). Huff (1951) records how Plasmodium gallinaceum and P. relictum could go through pre-erythrocytic stages in ducks, geese, canaries, and domestic pigeons without parasitemia. As the number of avian Plasmodium species is substantial, it would require such a huge study that it would be hard to justify on both cost and ethical grounds if humans were themselves to be tested for each type.
Since zoonoses are believed to account for up to 60% of emerging infectious diseases, and 71.8% of these originate in wildlife (Jones et al. 2008), this suggests that any infectious agent affecting primates or birds has a reasonable chance of affecting humans. The World Bank has estimated that zoonoses have cost global economies more than $20 BN in direct and $200 BN in indirect costs between 2000 and 2010. Zoonoses provide opportunities for host switching or genetic exchange giving rise to novel genetic combinations (Webster et al. 2016).
Mosquitoes are well placed to transfer zoonoses to humans. There are known to be numerous types of Plasmodium parasites, and in the case of human malaria, dengue fever, chikungunya, and Zika virus, different mosquito species are potential vectors (see Benelli and Mehlhorn 2016 for a recent review), raising the prospect that any simian or avian Plasmodium that could affect humans may be carried by a vector not previously suspected.
Based on laboratory studies, it has been shown that Aedes albopictus is a competent vector for at least 22 arboviruses (Malcolm 2009). In addition, it is known that some mosquito species can carry more than one type of Plasmodium (Alavi et al. 2003; Perez-Tris and Bensch 2005). Avian malaria parasites are present in numerous mosquito species, for example, Culex, Aedes, Culiseta, Anopheles, Mansonia, Aedeomya, and Coquillettidia; the “parasite-vector-vertebrate host” interactions remain understudied, as do reasons for the pathogenicity of different species and few experts have the knowledge required to identify avian Plasmodium spp. (Braga et al. 2011; Inci et al. 2012). Additionally, host-parasite interactions are complex, and host/vector ecology may be of crucial importance to shed light on parasite diversification (Lauron et al. 2014). To properly identify Plasmodium species, all the main blood stages of the parasite should be examined with samples containing relatively intensive parasitemia (Braga et al. 2011). Furthermore, hybrids may occur (Ramiro et al. 2015). In addition to malaria parasites, there are numerous tests for arbovirus recognition in mosquitoes (Anderson et al. 2010).
Besides mosquitoes, other bloodsucker insects may be responsible of arbovirus spreading. For example, Santiago-Alarcon et al. (2012) have shown that Culicoides (Diptera: Ceratopogonidae) are susceptible to Plasmodium infection, with some of their abdomens containing human blood and infected with avian Plasmodium, illustrating how little we know about numerous vectors affecting humans. Furthermore, they mention that an avian parasite (Plasmodium lophurae) can be experimentally adapted to a mammal host.
Carcinogenic infectious agents
The International Agency for Research on Cancer (IARC) highlighted that infection with P. falciparum in holoendemic areas is “probably carcinogenic to humans” and placed it in “Group 2A” (Bouvard et al. 2012). Besides this, IARC recognizes the following as group 1 carcinogens: Epstein-Barr virus (EBV), a member of the Herpes family, Kaposi sarcoma herpesvirus (HHV-8), human papilloma virus (HPV), hepatitis B and C viruses (HBV and HCV), human T cell lymphotropic virus type 1, the bacterium Helicobacter pylori, and the parasites Schistosoma haematobium, Clonorchis sinensi, and Opisthorchis viverrini. Their main features are summarized in the paragraphs below.
Herpes viruses
HHV-6A, a member of the Herpes family, has for the first time been implicated in female unexplained infertility development and possibly able to infect cervical cells (Marci et al. 2016). HHV-6A either in latent form or during acute infection can also activate the human endogenous retrovirus K-18 that can cause deregulation of the immune system (Tai et al. 2009). PCR analysis of peripheral blood mononuclear cells and saliva failed to find HHV-6A DNA, illustrating that blood and saliva tests may produce false negatives (Higashimoto et al. 2012). The UK National Health Service (NHS) has a range of information sheets. With respect to an EBV diagnosis, common symptoms are listed as a high temperature, severely sore throat, swollen neck glands, and fatigue and after infection, lifelong immunity is developed. Exposure to the virus in childhood causes few symptoms and often goes non-recognized. If after a mosquito bite the person bitten is asymptomatic, then EBV is unlikely to be suspected and not routinely looked for as 95% of people in the UK are thought to be infected by the time they are 40 years old.
An NHS information sheet for cytomegalovirus (CMV) also part of the Herpes family and under investigation by the IARC as a possible group 1 carcinogen states that most cases of CMV do not cause symptoms, and it is thought that 50–80% of adults in the UK are infected. HHV-8 will be looked for in potential cancer patients if they have the characteristic discolored patches. No mention is made of possible linkages with mosquitoes despite their presence in some species (Ward et al. 2016).
Hepatitis B and C
Initial assessment of these viruses is based not on tests but on discussions with the patient. For example, is the patient migrating or returning from holiday from a country where such infections are rife? Simple tests on skin stretch may be used, although there is no reported validation of stiffness cut-offs and non-invasive tests are poor for fibrosis (Degos et al. 2010; Tsochatzis et al. 2011). However, HCV often has no noticeable symptoms until the liver has been significantly damaged. Symptoms for both HBV and HCV can be flu-like, tiredness, loss of appetite, feeling and being sick, and abdominal pain. When suspected, a blood test is carried out; however, diagnosis of HBV-positive hepatocellular carcinoma (HCC) is difficult (independent of cirrhosis etiology, because of a lack of biomarkers, see Li et al. 2010). There is no suggestion of a routine test, if cancer is identified elsewhere in the body, i.e., if the patient remains asymptomatic for these viruses. There is no suggestion, either that these viruses may be picked up from mosquitoes, despite their linkage (Ward et al. 2016). Estimates of their contributions to worldwide disease have been lacking (Perz et al. 2006).
Human T cell lymphotropic virus (HTLV)
UK NHS factsheets only refer to this virus in the context of non-Hodgkin lymphoma. It is detected when there is lymph node swelling, but in some cases, non-Hodgkin lymphoma first develops in an organ or somewhere else outside the lymphatic system. Risk factors include a Helicobacter infection or EBV infection. However, as EBV infection is regarded as widespread and H. pylori reasonably common, it is unlikely that finding either of these would lead to HTLV tests.
Human papilloma virus
UK NHS factsheets state that genital HPV is part of cervical screening, which is offered to 25–64-year-old women. However, for men, there is currently no reliable test, it is difficult to diagnose and usually there are no symptoms. No mention is made of mosquitoes although the virus has been found in them (Ward et al. 2016). Different types of test can produce different outcomes (Ronco et al. 2013).
H. pylori
UK NHS factsheets are not available but is available for Campylobacter (food poisoning agent). It lists symptoms such as sickness, vomiting and diarrhea, lack of energy, loss of appetite, a high temperature, aching muscles, and chills. It states that in most cases these symptoms will pass in a few days and a sufferer will make a full recovery. It makes no mention of a cancer connection, and there is no suggestion it would be looked for in cancer patients.
Schistosomiasis
NHS information factsheets describe this as an infection caused by parasitic worms that live in fresh water in subtropical and tropical regions (see Mehlhorn 2016 for a recent review). First-infected patients often do not have symptoms, although in the long term it can cause carcinogenesis and organ damage (Figueiredo et al. 2015; Machicado and Marcos 2016). Diagnosis usually requires an expert in tropical diseases (Akpata et al. 2015; Botelho et al. 2016). It is unlikely that cancer patients residing outside of the tropics and subtropics would be routinely tested for this, despite increased travel and migration.
C. sinensi and O. viverrini
UK NHS has no information sheets for either of these, suggesting they would not be routinely tested for in cancer patients. It should be noted that the “gold standard” detection method for O. viverrini has limited diagnostic sensitivity and diagnostic specificity (Worasith et al. 2015).
UK cancer tests
Notably, the UK NHS list tests for a multitude of different cancers and also list a large set of symptoms. However, there is no single test and it does not appear to systematically test for all the IARC recognized carcinogens, outlining the urgency of further research efforts.
Conclusions
This review posed two questions, firstly, if there is a mosquito-cancer connection, why has it not been already identified (with the relevant exception for Burkett’s lymphoma), and secondly, what is its extent. With respect to the first question, one answer would appear to be that no one has seriously looked for it so far due to an absence of human, simian, or avian malarias being identified in many of the countries where cancers are present. There may in fact be no avian malaria in humans or a cancer connection with human and simian malarias, or maybe most patients with cancer are asymptomatic for these malarias and are, therefore, not tested for them.
It is possible that at some time humans have been tested for avian malarias, although we could not find any significant evidence for this. If they have been tested at some time in the past, then unreliable tests (in the light of newly discovered tests) may have produced false negatives or the tests may have been made on a limited number of avian Plasmodium parasites. There are currently huge difficulties regarding the proper identification of avian malaria parasites, highlighting the crucial importance of research in this field.
Other carcinogenic infectious agents do not appear to be part of a routine cancer testing protocol as most of the population is assumed to have had, for example, EBV and/or CMV. Even when a cancer test is positive, there does not appear to be a protocol that looks for each and all of these infectious agents as possible secondary cancer sites. Due to a lack of systematic testing, the answer to the second question is that we have no means of knowing the extent of known or potentially carcinogenic infectious agents transmitted by mosquito vectors, as well as by other generalist bloodsuckers Diptera, such as those belonging to the Culicoides genus.
While recent hypotheses suggesting a mosquito-cancer connection seem logical, any evidence remains circumstantial, leaving the mosquito as a possible suspect requiring greater interrogation. In a human murder trial, a suspect is often seen on CCTV and described in the broadest terms, for example 6 ft tall and wearing a hoodie. Likewise with mosquitoes, there are so many species that recognizing a suspect is equally if not more difficult. To complicate matters further, if they are guilty as charged, they will have left the scene years beforehand and with, so far, no recognizable DNA left behind.
References
Akpata R, Neumayr A, Holtfreter MC, Krantz I, Singh DD, Mota R, Hatz C, Richter J (2015) The WHO-ultrasonography protocol for assessing morbidity due to Schistosoma haematobium. Acceptance and evolution over 14 years. Systematic review. Parasitol res 114:1279–1289
Alavi Y, Arai M, Mendoza M, Tufet-Bayona M, Sinha R, Fowler K et al (2003) The dynamics of interactions between Plasmodium and the mosquito: a study of the infectivity of Plasmodium berghei and Plasmodium gallinaceum, and their transmission by Anopheles stephensi, Anopheles gambiae and Aedes aegypti. Int j parasitol 33:933–943
Allain J-P, Stramer SL, Carneiro-Proietti ABF, Martins ML, Lopes Da Silva SN, Ribeiro M et al (2009) Transfusion-transmitted infectious diseases. Biologicals 37:71–77
Anderson SL, Richards SL, Smartt CT (2010) A simple method for determining arbovirus transmission in mosquitoes. J am mosq control assoc 26:108–111
Banfield WG, Woke PA, MacKay CM, Cooper HL (1965) Mosquito transmission of a reticulum cell sarcoma of hamsters. Science 148:1239–1240
Banfield WG, Woke PA, MacKay CM (1966) Mosquito transmission of lymphomas. Cancer 19:1333–1336
Benelli G (2015) Research in mosquito control: current challenges for a brighter future. Parasitol res 114:2801–2805
Benelli G (2016) Green synthesized nanoparticles in the fight against mosquito-borne diseases and cancer—a brief review. Enzyme microbial technol 95:58–68
Benelli G, Mehlhorn H (2016) Declining malaria, rising dengue and Zika virus: insights for mosquito vector control. Parasitol res 115:1747–1754
Benelli G, Lo Iacono A, Canale A, Melhorn H (2016) Mosquito vectors and the spread of cancer: an overlooked connection? Parasitol res 115:2131–2137
Bernotiene R, Palinauskas V, Iezhova T, Murauskaite D, Valkiunas G (2016) Avian haemosporidian parasites (Haemosporida): a comparative analysis of different polmerase chain reaction assays in detection of mixed infections. Exp parasitol 163:31–37
Botelho MC, Machado A, Carvalho A, Vilaca M, Conceicao O, Rosa F et al (2016) Schistosoma haematobium in Guinea-Bissau: unacknowledged morbidity due to a particularly neglected parasite in a particularly neglected country. Parasitol res 115(4):1567–1572
Bousema T, Drakeley C (2011) Epidemiological and infectivity of Plasmodium falciparum and Plasmodium vivax gametocytes in relation to malaria control and elimination. Clin microbiol rev 24:377–410
Bouvard V, Baan RA, Grosse Y, Lauby-Secretan B, Ghissassi FE, Benbrahim-Talias L et al (2012) Carcinogernity of malaria and of some polyomaviruses. Lancet oncol 13:339–340
Braga EM, Silveira P, Belo NO, Valkiunas G (2011) Recent advances in the study of avian malaria: an overview with an emphasis on the distribution of Plasmodium spp. in Brazil. Mem Inst Oswaldo Cruz 106:S1 doi.org/10.1590/S0074-02762011000900002
Buckley A, Dawson A, Moss SR, Hinsley SA, Bellamy PE, Gould EA (2003) Serological evidence of West Nile virus, Usutu virus and Sindbis virus infection of birds in the UK. J gen virol 84:2807–2817
Cox FEG (2010) History of the discovery of the malaria parasites and their vectors. Parasit vectors 3:5. doi:10.1186/1756-3305-3-5
Cox-Singh J, Davis TM, Lee KS, Shamsui SS, Matusop A, Ratnam S et al (2008) Plasmodium knowlesi malaria in humans is widely distributed and potentially life threatening. Clin infect dis 46(2):165–171
Degos F, Perez P, Roche B, Mahmoodi A, Asselineau J, Voitot H et al (2010) Diagnostic accuracy of FibroScan and comparison to liver fibrosis biomarkers in chronic viral hepatitis: a multicenter prospective study (the FIBROSTIC study). J hepatol 53:1013–1021
Dodd RY (2010) Emerging pathogens in transfusion medicine. Clin lab med 30:499–509
Figueiredo JC, Richter J, Borja N, Balaca A, Costa S, Belo S, Grácio MA (2015) Prostate adenocarcinoma associated with prostatic infection due to Schistosoma haematobium. Case report and systematic review. Parasitol res 114(2):351–358
Higashimoto Y, Ohta A, Nishiyama Y, Ihira M, Sugata K, Asano Y et al (2012) Development of a human herpesvirus 6 species specific immunoblotting assay. J clin microbiol 50:1245–1251
Huff CG (1951) Observations on the pre-erythrocytic stages of Plasmodium relictum, Plasmodium cathermerium, and Plasmodium gallinaceum in various birds. J infect dis 88:17–26
Hughes T, Irwin P, Hofmeister E, Paskewitz SM (2010) Occurrence of avian Plasmodium and West Nile virus in Culex species in Wisconsin. J am mosq control assoc 26:24–31
Inci A, Yildirim A, Njabo KY, Duzlu O, Biskin Z, Ciloglu A (2012) Detection and molecular characterization of avian Plasmodium from mosquitoes in central Turkey. Vet parasitol 188:179–84
Jones EK, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL (2008) Global trends in emerging infectious diseases. Nature 451:990–993
Johansson O, Ward M (2016) The human immune system’s response to carcinogenic and other infectious agents transmitted by mosquito vectors. Parasitol Res doi: 10.1007/s00436-016-5272-2.
Krief S, Escalente AA, Pacheco MA, Mugisha L, Andre C, Halbwax M (2010) On the diversity of malaria parasites in African apes and the origin of Plasmodium falciparum from Bonobos. Plos pathog 6(2):e1000765. doi:10.1371/journal.ppat.1000765
Lauron EJ, Loiseau C, Bowie RCK, Spicer GS, Smith TB, Melo M et al (2014) Coevolutionary patterns and diversification of avian malaria parasites in African sunbirds (Family Nectariniidae). Parasitology 142:635–647
Lehrer S (2010a) Association between malaria incidence and all cancer mortality in fifty U.S. states and the district of Columbia. Anticancer res 30:1371–1373
Lehrer S (2010b) Anopheles mosquito transmission of brain tumor. Med hypotheses 74:167–168
Li LM, Hu ZB, Zhou ZX, Liu FY, Zhang JF, Shen HB (2010) Serum microRNA profiles serve as novel biomarkers for HBV infection and diagnosis of HBV-positive hepatocarcinoma. AA cancer res 70(23):9798–807
Machicado C, Marcos LA (2016) Carcinogenesis associated with parasites other than Schistosoma, Opisthorchis and Clonorchis: a systematic review. Int j cancer 138(12):2915–2921
Malcolm CA (2009) Public health issues posed by mosquitoes. An independent report for the Chartered Institute of Environmental Health, London
Marci R, Gentili V, Bortolotti D, Lo Monte G, Caselli E, Bolzani S et al (2016) Presence of HHV-6A in endometrial epithelial cells from women with primary unexplained infertility. Plos one 11(7):e0158304. doi:10.1371/journal.pone.0158304
Medeiros MC, Ricklefs RE, Brawn JD, Ruiz MO, Goldberg TL, Hamer GL (2016) Overlap in the seasonal infection patterns of avian malaria parasites and West Nile virus in vectors and hosts. Am j trop med hyg 95:1121–1129
Mehlhorn H (ed) (2015) Encyclopedia of parasitology, 4th edn. Springer, New York
Mehlhorn H (2016) Worms of humans. In: Human parasites (Ed. H. Mehlhorn), Springer, pp. 135–298, doi: 10.1007/978-3-319-32802-7_4
Molina-Cruz A, Zilversmit MM, Neafsey DE, Harti DL, Barillas-Mury C (2016) Mosquito vectors and the globalization of Plasmodium falciparum malaria. Annu rev genet 50:447–465
Niebuhr CN, Blasco-Costa I (2016) Improving detection of avian malaria from host blood: a step towards a standardised protocol for diagnostics. Parasitol res 115:3905–3911
Njabo KY, Cornel A, Sehgal RNM, Loiseau C, Buermann W, Harrigan R et al (2009) Coquillettidia (Culicidae, Diptera) mosquitoes are natural vectors of avian malaria in Africa. Malaria j 8:193
Outlaw DC, Harvey JA, Nagle MS, Drovetski SV, Voelker G (2016) Diversity and distribution of avian haemosporidians in sub-Saharan Africa: an inter-regional biographic overview. Parasitology doi: 10.1017/S0031182016001979
Perez-Tris J, Bensch S (2005) Daignosing genetically diverse avian malarial infections using mixed-sequence analysis and TA-cloning. Parasitology 131:15–23
Perkins SL (2014) Malaria’s many mates: past, present, and future of the systematics of the order Haemosporida. J parasitol 100:11–25
Perz JF, Armstrong GL, Farrington LA, Hutin YJF, Bell BP (2006) The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J hepatol 45:529–538
Petersen LR, Brault AC, Nasci RS (2013) West Nile virus: review of the literature. JAMA 310(3):308–315. doi:10.1001/jama.2013.8042
Pick C, Ebersberger I, Spielmann T, Bruchhaus I, Burmaster T (2011) Phyogenomic analyses of malaria parasites and evolution of their exported proteins. BMC evol biol 11:167. doi:10.1186/1471-2148-11-167
Prugnolle F, Durand P, Ollamo B, Duval L, Ariey F et al (2011) A fresh look at the origin of Plasmodium falciparum, the most malignant malaria agent. Plos pathog 7(2):e1001283. doi:10.1371/journal.ppat.1001283
Ramiro RS, Khan SM, Franke-Fayard B, Janse CJ, Obbard DJ, Reece SE (2015) Hybridization and pre-zygotic reproductive barriers in Plasmodium. Proc biol sci 282(1806):20143027. doi:10.1098/rspb.2014.3027
Richard FA, Sehgal RNM, Jones HI, Smith TB (2002) A comparative analysis of PCR-based detection methods for avian malaria. J parasitol 88:819–822
Ronco G, Dillner J, Elfstrom KM, Tunesi S, Snijders PJF, Arbyn M (2013) Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet 383(9916):524–532
Santiago-Alarcon D, Havelka P, Schaefer HM, Segelbacher G (2012) Bloodmeal analysis reveals avian Plasmodium infections and broad host preferences of Culicoides (Diptera: Ceratopogonidae) vectors. Plos one 7(2):e31098. doi:10.1371/journal.pone.0031098
Spielman A, D’Antonio M (2001) Mosquito: the story of man’s deadliest foe. Hyperion, New York
Sutherland CJ, Tanomsing N, Nolder D, Oguike M, Jennison C, Pukrittayakamee S et al (2010) Two non recombining sympatric forms of the human malaria parasite Plasmodium ovale occur globally. J infect dis 201:1544–1550
Ta TH, Hisam S, Lanza M, Jiram AI, Ismail N, Rubio JM (2014) First case of a naturally acquired human infection with Plasmodium cynomolgi. Malaria j 413:68
Tai AK, Luka J, Ablashi D, Huber BT (2009) HHV-6A infection induces expression of HERV-K18-encoded superantigen. J clin virol 46:47–48
Tsochatzis EA, Gurusamy KS, Ntaoula S, Cholongitas E, Davidson BR, Burroughs AK (2011) Elastography for the diagnosis of severity of fibrosis in chronic liver disease: a meta-analysis of diagnostic accuracy. J hepatol 54:650–659
Vythilingam I, Noorazian YM, Huat TC, Jiram AI, Yusri YM, Azahari AH (2008) Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia. Parasit vectors 1:26. doi:10.1186/1756-3305-1-26
Ward M, Ward A, Johansson O (2016) Does the mosquito have more of a role in certain cancers than is currently appreciated?—The mosquito cocktail hypothesis. Med hypotheses 86:85–91
Waters AP, Higgins DG, McCutchan TF (1991) Plasmodium falciparum appears to have arisen as a result of lateral transfer between avian and human hosts. Proc natl acad sci U S A 88:3140–3144
Webster JP, Gower CM, Knowles SCL, Molyneux DH, Fenton A (2016) One-health: an ecological and evolutionary framework for tackling Neglected Zoonotic Diseases. Evol appl 9(2):313–33
Worasith C, Kamamia C, Yakovleva A, Duenngai K, Wangboon C, Sithithaworn J et al (2015) Advances in the diagnosis of human Opisthorchiasis: development of Opisthorchiasis viverrini antigen detection in urine. Plos negl trop dis 9:e0004157
Yeda R, Ingasia LA, Cheruiyot AC, Okudo C, Chebon LJ, Cheruiyot J (2016) The Genotypic and phenotypic stability of Plasmodium falciparum field isolates in continuous in vitro culture. Plos one 11:e0143565. doi:10.1371/journal.pone.0143565
Zehtindjiev P, Krizanauskiene A, Bensch S, Palinauskas V, Asghar M, Dimitrov D (2012) A new morphologically distinct malaria parasite that fails detection by established polymerase chain reaction-based protocols for amplification of the cytochrome B gene. J parasitol 98:657–665
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Ward, M., Benelli, G. Avian and simian malaria: do they have a cancer connection?. Parasitol Res 116, 839–845 (2017). https://doi.org/10.1007/s00436-016-5352-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00436-016-5352-3