
Abstract
Purpose
(1) To investigate associations between single nucleotide polymorphisms (SNPs) in osteopontin (OPN) and its receptor—cluster of differentiation 44 (CD44) genes and gastric cancer susceptibility. (2) To explore the correlation of OPN and CD44 expression of gastric cancer.
Methods
We detected 26 SNPs of the genes in gastric cancer patients from the Chinese Han population by Sequenom technique and performed expression of OPN in combination with CD44 in 243 tissues samples of the cases by tissue microarray and immunohistochemistry (IHC).
Results
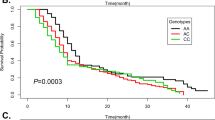
We found that the minor alleles of OPN rs4754C>T and OPN rs9138C>A remained strongly associated with decreased gastric cancer risk (P = 1.53 × 10−4, odds ratio (OR) 0.642, 95 % confidence interval (CI) 0.511–0.808 and P = 1.59 × 10−4, OR 0.642, 95 %CI 0.510–0.809). OPN variant rs1126772A>G and CD44 variant rs353639A>C significantly contributed to elevated risk of gastric cancer (P = 0.042, OR 1.279, 95 % CI 1.008–1.622 and P = 0.047, OR 1.334, 95 % CI 1.003–1.772). Haplotypes of OPN and CD44 variants significantly influenced risk of gastric cancer. Clinical data indicated that rs4754 and rs9138 of OPN were significantly associated with smoking (P = 0.029, OR 0.343, 95 % CI 0.127–0.926 and P = 0.029, OR 0.343, 95 %CI 0.127–0.926) and OPN rs1126772 revealed associations with tumor–node–metastasis (TNM) stage (P = 0.025, OR 1.765, 95 % CI 1.073–2.905) and tumor differentiation (P = 0.031, OR 1.722, 95 % CI 1.049–2.825). OPN expression was observed in 133 of the 243 cases (54.7 %) by IHC and was correlated with serosa invasion (P = 0.013), TNM stage (P = 0.003) and lymph node metastasis (P = 0.002). CD44 expression was found in 92 of the 243 cases (37.9 %) and was associated with tumor size (P = 0.005) and lymph node metastasis (P = 0.023), respectively. The OPN expression displayed a positive association with CD44 (P = 0.01, r s = 0.164).
Conclusions
We found that the polymorphisms rs4754, rs9138 and rs1126772 of OPN gene and rs353639 of CD44 gene were significantly associated with gastric cancer. Our IHC data indicated that interaction of OPN and CD44 protein would promote progression and metastasis of gastric cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gastric cancer is a leading cause of cancer morbidity and mortality worldwide (Catalano et al. 2009). The occurrence and development of gastric cancer is involved in a complicated process and is influenced by integrated effects of genetic and environmental factors (Samson et al. 2002). The precise mechanisms of gastric cancer carcinogenesis remain yet unknown. Some investigations demonstrated associations of cytokines and cell adhesion molecules with susceptibility to gastric cancer (Ando et al. 2009; Xia et al. 2012).
Osteopontin (OPN), also known as secreted phosphoprotein 1 (SPP1), early T lymphocyte activation 1 (Eta-1) and bone sialoprotein I (BSPI), is a member of cytokines and belongs to the small integrin-binding ligand N-liked glycoprotein gene family (Fisher et al. 2004). The OPN gene is located on chromosome 4q24–q25 and consists of seven exons encoding a multifunctional protein that contains a Arg–Gly–Asp (RGD) domain (Young et al. 1990). OPN is involved in multifarious physiological and pathological processes, including inflammatory reaction, wound healing, angiogenesis and immune response (Denhardt et al. 2001; Jansson et al. 2002; Wang et al. 2011). OPN is expressed in a variety of tumor cells, such as stomach (Imano et al. 2009), lung (Jin et al. 2012), colorectum (Likui et al. 2010), esophagus (Wu et al. 2008) and liver (Lin et al. 2011). Previous studies illustrated that OPN signaling could activate anti-apoptosis, survival and invasion of cancer cells via phosphatidylinositol 3-kinase/protein kinase B (PI3K/Akt) and nuclear factor kappa B (NF-κB) signaling pathway (Fong et al. 2009), degrade extracellular matrix (ECM) by regulating the activity of matrix metalloproteinases (MMPs) and urokinase-type plasminogen activator (uPA) (Chen et al. 2011), and modulate angiogenesis by vascular endothelial growth factor (VEGF) (Tang et al. 2008), leading to tumor growth and metastasis. Clinical investigations displayed that OPN mRNA expression was associated with tumor–node–metastasis (TNM) stage in esophageal carcinoma (Wu et al. 2008) and lymph node metastasis and TNM stage in colorectal cancer (Likui et al. 2010). Higashiyama et al. (2007) found that expression of OPN mRNA and protein increased in gastric cancer by semiquantitative reverse transcription polymerase chain reaction (RT-PCR) and Western blot analysis. Dai et al. (2007) revealed that gastric cancer patients with OPN-positive expression held poorer survivals, later TNM stage, invasion and positive lymph node metastasis. Furthermore, elevated plasma OPN level was significantly in association with progressive stage, serosa invasion, lymph node metastasis and liver metastasis in gastric cancer; therefore, plasma OPN level might be of value as diagnostic and prognostic factor in gastric cancer (Wu et al. 2007).
Cluster of differentiation 44 (CD44) is a crucial transmembrane receptor for OPN, which is a member of cell surface adhesion molecule family and exists in various organs and tissues. The CD44 gene is located on chromosome 11p13 and contains 20 exons, 10 of which are expressed in the standard form (CD44s). The remaining 10 exons are expressed in an exceedingly large number of splice variant isoforms of the protein (CD44v) (Tolg et al. 1993). CD44 plays a vital role in cell migration, adhesion, regulation of lymphocyte activation and homing (Ponta et al. 2003). CD44 promotes tumor metastasis by enhancing tumor cell migration and motility (Bourguignon et al. 1999). Increased expression of CD44 was found in gastrointestinal tumors and was associated with tumor invasion, lymph node metastasis and patients’ survival (Bendardaf et al. 2006; Doventas et al. 2012). It was demonstrated that CD44 showed ligand–receptor association and was functionally in concurrent conjunction with OPN in tumor growth and progression (Weber et al. 1996, 1997), promotion of cell proliferation and anti-apoptosis (Lin and Yang-Yen 2001). The C-terminal fragment of OPN contains a heparin-binding domain for variant isoforms of CD44 binding (Weber et al. 1996). Interaction between OPN and CD44 is a way of tumor cells anchoring specific sites of metastasis formation (Weber et al. 1997).
In recent researches, the functions of the mutated genes of OPN and CD44 were investigated. For example, Hep-3B (hepatocelluar carcinoma cell line) transfected with OPN 3′-untranslated regions (UTR) mutation would modify OPN expression (Bhattacharya et al. 2010). Polymorphisms in the OPN promoter region could affect its transcriptional activity (Giacopelli et al. 2004). Knockout of CD44 gene could prevent tumor metastasis in the mice model (Weber et al. 2002). CD44 rs13347C>T polymorphism might influence nasopharyngeal carcinoma development by increasing CD44 expression (Xiao et al. 2013). In addition, genetic analyses on CD44 and OPN with regard to susceptibility in gastrointestinal tumors were described. Winder et al. found that in gastric adenocarcinoma, CD44 rs187116 (AG, GG vs. AA) was associated with shorter time to tumor recurrence (TTR), rs7116432 (AG, AA vs. GG) correlated with shorter TTR and overall survival (OS); patients harboring CD44 rs187115T–rs187116A haplotype were at the lowest risk of developing tumor recurrence (Winder et al. 2011). Gerger et al. (2011) demonstrated the wild-type genotype CC of CD44 rs8193 led to a shorter TTR in colon cancer. Also, polymorphisms in the OPN promoter region were associated with gastric carcinoma risk (Lee et al. 2013; Zhao et al. 2012). Zhao et al. (2012) detected that nucleotide −443 (T → C) variants of OPN increased metastasis and subsequent death of gastric carcinoma. Lee et al. (2013) confirmed −443 CC and −616 TT were significantly associated with gastric cancer susceptibility. Single nucleotide polymorphisms (SNPs) of OPN and CD44 might become of predictive for high expression levels of the proteins in gastric cancer progression. However, association study of genetic polymorphisms in the OPN coding and 3′-UTR with susceptibility to gastric cancer remains yet absent.
We aimed at evaluation of whether genetic variants of OPN and CD44 in the coding and untranslated regions were associated with gastric cancer susceptibility. We performed a genetic analysis in a case–control study by Sequenom technique and analyzed potential associations of these genetic polymorphisms as well as expression of OPN and CD44 in gastric cancer tissue with clinicopathological characteristics of gastric cancer.
Materials and methods
Study population
Three hundred and eleven cases with advanced gastric carcinoma and 425 cancer-free controls were investigated in this study. Patients with gastric carcinoma were collected from the First Affiliated Hospital of Anhui Medical University between March 2008 and July 2009 and received no chemotherapy or radiotherapy before surgical gastrectomy. The patients were comprised 246 men and 65 women with an average age of 60.4 ± 10.4 years (ranging from 24 to 83 years). Of which, two hundred and forty-three cases with full clinical pathological data were used for IHC analysis, including 187 men and 56 women with an average age of 60.3 ± 10.2 years (ranging from 24 to 83 years). Additional 24 samples of normal gastric mucosal tissues were used as IHC controls. In addition, a total of 336 men and 89 women control subjects were matched with an average age of 60.6 ± 8.4 years (ranging from 30 to 86 years). These control subjects without a history of cancers were recruited from patients who visited hospital for a conventional cancer-screening program. Information on demographic characteristics, such as gender, age, smoking habits, alcohol consumption and family history of cancer were obtained from a personal interview administered by trained personnel. Smoking habit was defined as non-smoker and smoker. Individuals who smoked one cigarette per day for over 1 year were defined as smokers. Alcohol consumption was defined as non-drinker and drinker. Individuals who consumed more than 200 mL alcohol per day were defined as drinker. The intake of salted food was defined as no or occasional and yes. Individuals who took salt in diet over 6 g per day were defined as high salt. Clinical diagnosis and staging of gastric carcinoma were assessed by two pathologists according to the World Health Organization classifications and TNM classifications issued in 2006. Informed consents were obtained from all the participants. This study was approved by the ethics committee for genome research of the Anhui Medical University of China.
Extraction of peripheral blood DNA
Total blood sample was collected from each subject before treatment and stored at −80 °C until analysis. Genomic DNA was extracted from peripheral blood using QIAamp DNA Blood Midi Kit (Qiagen Inc., Germany) according to the manufacturer’s protocol. The quantitative concentration of DNA was measured by the Nanodrop Spectrophotometer (ND-1000, USA) of full wavelength and standardized to 50 ng/μl.
SNP selection and sequenom assay
Based on the Hapmap Chinese Han population database, we checked SNPs of OPN and CD44 genes by Haploview software. We preferentially chose tag SNPs and potentially significant SNPs which located in the exon or 3′-UTR. Thus, a panel of 26 SNPs were selected with the minor allele frequency (MAF) >0.05 and were in Hardy–Weinberg equilibrium (HWE). They included (1) OPN SNPs: rs11728697, rs4754, rs1126772 and rs9138 and (2) CD44 SNPs: rs2785172, rs2553808, rs353619, rs187115, rs353644, rs353639, rs353630, rs353647, rs7937602, rs4756195, rs3794107, rs1071695, rs16927042, rs996076, rs16927061, rs11033021, rs7110737, rs12577007, rs8193, rs11821102, rs10836347 and rs13347. Genotyping analysis of the SNPs for fast-track validation analysis was performed using the Sequenom Mass Array system. Fifteen ng of genomic DNA was standardized for genotyping of each sample. Locus-specific PCR and detection primers were designed using the Mass ARRAY Assay Design 3.0 software (Sequenom, San Diego, California, USA) following the manufacturer’s instructions. The DNA samples were amplified by multiplex PCRs. The PCR products were then used for locus-specific single-base extension reactions. The resulting products were desalted and transferred to a 384-element SpectroCHIP array. Allele detection was performed using MALDI-TOF MS. The mass spectrograms were analyzed by the Mass ARRAY Typer software (Sequenom).
Tissue microarray block preparation and IHC
Typical areas of cancers on HE-stained section slides were selected under microscope. Circles were drawn on the slides around the representative areas of the section. Using the slides as guides, core samples (0.6 mm in diameter) were punched out from each corresponding paraffin-embedded block using a tissue microarray (TMA) sampling tool. Duplicated cores were applied in order to avoid shedding. Fifty-four cores were embedded in a TMA block with 8 × 7 alignments. Thus, a total of nine TMA blocks were produced creating a panel of TMAs for the 243 tumor samples. In addition, we selected 24 cases of normal gastric mucosal tissues as the controls.
Histological sections (4 µm) from the nine TMA blocks were used for the study. The TMA sections were deparaffinized in xylene and rehydrated through descending concentrations of ethanol. After washing twice in phosphate-buffered saline (PBS) for 5 min, the slides were exposed to 3 %H2O2 at room temperature for 10 min. Antigen retrieval was achieved by microwave treatment in 0.01 mol/L citrate buffer (pH 6.0) for 2 min, followed by cooling for 2 h. After washing in PBS and exposure to normal goat serum to reduce non-specific binding, the slides were incubated with rabbit monoclonal antibody against human of OPN and CD44 (abcam, USA) at a diluted solution of 1:200 at 4 °C for 20 h and then with secondary antibody and SABC agent at 37 °C for 20 min, respectively. After further PBS washing, slides were then incubated with substrate diaminobenzidine and hydrogen peroxide for 10 min. Finally, sections were counterstained with hematoxylin. All reagents were purchased from Zhongshan Biotechnology Co., Ltd. (Beijing, P.R. China).
Evaluation IHC staining
Immunoreactivity of tumor TMA was evaluated according to both of the proportion of stained cells and/or ECM as well as their intensities. Area of stained cells and/or ECM was semiquantitatively scored as follows: 0 = negative, 1 = 1–25 %, 2 = 26–50 %, 3 = 51–75 % and 4 = 76–100 %. Staining intensity was scored as 0 = negative, 1 = weak, 2 = medium and 3 = strong. The sum of the intensity and extent score was used as the final staining score. A score of ≥4 was considered as a positive expression.
Data analysis
We used a logistic regression model with age and gender adjustment to analyze the association of SNPs with risk of gastric cancer. HWE proportion was tested in control samples to ensure genotyping quality. The differences in frequency distributions of the genotypes between the cases and the controls and the stratified association analysis between the clinicopathological parameters and the SNPs and protein expression of OPN and CD44 were tested using chi-squared test, while if there was the number of genotype ≤5, Fishers’ exact test was used. When the number of one mutant genotype (Dd or DD) was 0 in one of the clinicopathological parameters, we combined two mutant genotypes and analyzed as dominant model (DD plus Dd vs. dd). All analyses for P values were two-sided. The statistical software Plink v1.07 (http://pngu.mgh.harvard.edu/purcell/plink/) and Stata/SE version 10 were used for statistical analyses (StataCorp LP, College Station, TX). The Haploview 4.2 was used to calculate the linkage disequilibrium (LD) and the haplotype analysis. Those haplotypes with the frequency of <0.05 were ignored in the analysis.
Results
Association analysis of 26 SNPs of OPN and CD44
Minor alleles, P values, estimated odds ratios (ORs) and 95 % confidence intervals (CIs) of the 26 SNPs of OPN and CD44 genes between the cases and the controls are summarized in Table 1. We found that three of four SNPs (rs4754, rs1126772 and rs9138) of OPN tested were associated with the risk of gastric cancer. Of which, the minor alleles of rs4754C>T and rs9138C>A remained strongly associated with decreased gastric cancer risk (P = 1.53 × 10−4, OR 0.642, 95 % CI 0.511–0.808; P = 1.59 × 10−4, OR 0.642, 95 % CI 0.510–0.809), while the minor allele of rs1126772A>G significantly presented increased gastric cancer risk (P = 0.042, OR 1.279, 95 % CI 1.008–1.622). One individual SNP (rs353639A>C) of 22 CD44 variants detected was identified to increase the risk of gastric cancer (P = 0.047, OR 1.334, 95 % CI 1.003–1.772). We further analyzed the four SNPs using alternative models, such as codominant, dominant and recessive models. As shown in Table 2, in the codominant model, heterozygous genotypes TC (rs4754) and CA (rs9138) and the homozygous genotypes TT (rs4754) and AA (rs9138) of OPN were significantly of higher proportion in the controls and had the benefit of decreased risk of gastric cancer compared to the wild-type genotype CC (P = 0.000, OR 0.547, 95 % CI 0.400–0.746; P = 0.000, OR 0.547, 95 % CI 0.400–0.747; P = 0.014, OR 0.503, 95 % CI 0.289–0.876; and P = 0.014, OR 0.503, 95 % CI 0.289–0.876), respectively. OPN heterozygous genotype AG of rs1126772 bore increased risk of gastric cancer (P = 0.040, OR 1.381, 95 % CI 1.015–1.879). In the dominant model, TC + TT (rs4754) and CA + AA (rs9138) showed significantly reduced risk of gastric cancer compared to the CC genotype (P = 0.000, OR 0.539, 95 % CI 0.401–0.725; and P = 0.000, OR 0.539, 95 % CI 0.400–0.726, respectively), while the genotype AG + GG of rs1126772 elevated the risk of gastric cancer compared to the wild-type AA (P = 0.030, OR 1.386, 95 % CI 1.032–1.863).
The LD and haplotypes analysis
We performed a LD analysis. The results were shown in Fig. 1. The SNPs of CD44 (1#–22#) were separately located in Block 1–Block 5. Block 6 contained 3 SNPs (rs4754, rs1126772 and rs9138) of OPN. We performed a haplotype analysis further (Table 3) and found that haplotypes TAA (rs4754, rs1126772 and rs9138) and CTAA (rs11728697, rs4754, rs1126772 and rs9138) of OPN significantly conferred reduced risk of gastric cancer (P = 1.0 × 10−4, OR 0.640, 95 % CI 0.509–0.805; P = 0.003, OR 0.685, 95 % CI 0.535–0.877), respectively, while haplotypes CGC (rs4754, rs1126772 and rs9138) and CCAC (rs11728697, rs4754, rs1126772 and rs9138) of OPN endued elevated risk of gastric cancer (P = 0.044, OR 1.279, 95 % CI 1.008–1.622; P = 0.013, OR 1.306, 95 % CI 1.056–1.617). Also, the haplotype GCC of CD44 consisting of rs353644, rs353639 and rs353630 (Block 3) endued elevated risk of gastric cancer (P = 0.044, OR 1.436, 95 % CI 1.015–2.031).

Pairwise LD (r 2) in the study population
Association analysis of SNPs and clinicopathological characteristics of gastric cancer
We conducted a stratified genetic association analysis with regard to the 26 SNPs and clinicopathological characteristics, such as gender, age, tumor location, tumor size, histological type, grade of tumor differentiation, serosa invasion, lymph node metastasis, TNM stage, smoking, alcohol drinking, family history and salted food. There were significant correlations of the genotype TT of rs8193 to tumor size (P = 0.029, OR 0.438, 95 % CI 0.204–0.925) and serosa invasion (P = 0.019, OR 0.394, 95 % CI 0.180–0.865), rs4756195 AA to serosa invasion (P = 0.028, OR 0.099, 95 % CI = 0.011–0.904), rs1071695 CT + TT to serosa invasion (P = 0.033, OR 2.371, 95 % CI 1.054–5.331) and TNM stage (P = 0.022, OR 2.121, 95 % CI 1.103–4.080), rs1126772 AG to TNM stage (P = 0.025, OR 1.765, 95 % CI 1.073–2.905) and differentiation (P = 0.031, OR 1.722, 95 % CI 1.049–2.825), rs353644 GG (P = 0.029, OR 3.061, 95 % CI 1.082–8.661) and rs3794107 AT + TT to histological type (P = 0.000, OR 4.086, 95 % CI 1.852–9.012), rs16927042 CG to histological type (P = 0.003, OR 3.370, 95 % CI 1.452–7.822) and salted food (P = 0.034, OR 2.057, 95 % CI 1.045–4.050), rs16927061 GA + AA to gender (P = 0.023, OR 0.479, 95 % CI 0.252–0.912), rs4754 TT, rs 9138 AA and rs11821102 AG + AA to smoking (P = 0.029, OR 0.343, 95 % CI 0.127–0.926; P = 0.029, OR 0.343, 95 % CI 0.127–0.926; P = 0.014, OR 0.438, 95 % CI 0.224–0.856), rs353619 TC + TT to family history (P = 0.007, OR 2.932, 95 % CI 1.311–6.557) and tumor location (P = 0.029, OR 2.117, 95 % CI 1.074–14.171), respectively (Table 4). In addition, genetic changes of the four SNPs in OPN and CD44 genes did not affect expression of OPN and CD44 in tumor tissues (Table 5).
Correlation of OPN and CD44 expression with clinicopathological characteristics of gastric cancer
We detected expression of OPN and CD44 in gastric carcinoma by means of TMA and IHC. The specific immunostaining of OPN and CD44 proteins was cytoplasmic and/or membranous. None of OPN and CD44 expression was found in normal mucosa and gastric glands (Fig. 2a, b). We found OPN-positive expression in 133 of the 243 cases (54.7 %) and CD44 expression in 92 of the cases (37.9 %), respectively. Stronger immunoreactivities of both OPN and CD44 were found in adenocarcinomas (Fig. 2c, d) and invasive adenocarcinoma cells in the serosa (Fig. 2e).

OPN and CD44 IHC staining. a Normal gastric glands were OPN negative, ×400; b normal gastric glands were CD44 negative, ×400; c positive immunoreactivity of OPN was observed in tubular adenocarcinoma cells, ×200; d positive immunoreactivity of CD44 was located in tubular adenocarcinoma cells, ×400; e invasive adenocarcinoma cells in the serosa were OPN positive, ×200
We performed a case-only logistic regression association analysis and found protein expression significantly correlated with serosa invasion (P = 0.013), TNM stage (P = 0.003) and lymph node metastasis (P = 0.002) in OPN and with tumor size (P = 0.005) and lymph node metastasis (P = 0.023) in CD44, respectively (Table 6). OPN+/CD44+ were 60 cases (24.7 %), OPN+/CD44− were 73 cases (30.0 %), OPN−/CD44− were 78 cases (32.1 %) and OPN−/CD44+ were 32 cases (13.2 %). OPN in tumor tissues was significantly expressed with a positive correlation of CD44 (P = 0.01) with an acceptable rs of 0.164.
Discussion
In this study, we detected 26 SNPs of OPN and CD44 genes with regard to evaluating gastric cancer susceptibility. We found that the polymorphisms rs4754, rs9138 and rs1126772 of OPN gene and rs353639 of CD44 gene were significantly associated with gastric cancer in the Chinese population. To our knowledge, these four genetic variants were never reported in relation to susceptibility of gastric cancer.
Our study revealed that OPN rs4754 with the minor allele T and rs9138 with the minor allele A were significantly associated with reduced gastric cancer risk (P = 1.53 × 10−4, OR 0.642, 95 % CI 0.511–0.808; P = 1.59 × 10−4, OR 0.642, 95 % CI 0.510–0.809, respectively). Previous investigation demonstrated a statistical difference in the synonymous SNP rs4754 (+282C/T, Asp80Asp) with CC homozygotes in the sarcoidosis patients in Slovenian (Maver et al. 2009). Presumably, C to T transition at the SNP rs4754 might be harmful to OPN pre-mRNA alternative splicing via modifying exonic splicing enhancer or exonic splicing silencer binding to the polymorphic region of the gene (Cartegni et al. 2002). The SNP rs9138 (+1239C/A) located in the 3′-UTR region of OPN gene and might affect transcribed mRNAs stability and translational activity (Conne et al. 2000). It was reported that OPN mRNA expression in the individuals carrying the C allele of rs9138 was 4.4-fold higher than in those carrying the A allele (D’Alfonso et al. 2005). Functional data revealed that the A allele of rs9138 might promote OPN mRNA degradation, thus contributing to decreasing gastric cancer risk (Castelli et al. 2009). In addition, we found that genotypes TT of rs4754 and AA of rs9138 in OPN were significantly associated with smoking (P = 0.029, OR 0.343, 95 % CI 0.127–0.926 and P = 0.029, OR 0.343, 95 % CI 0.127–0.926, respectively). It was reported that smoking might initiate inflammatory response to facilitate development of gastric carcinoma (Ladeiras-Lopes et al. 2008). OPN might be involved in pathogenesis of inflammation of gastric mucosa through other proinflammatory cytokines (Hamajima et al. 2006). So we deduced that the two genetic variants and smoking could play synergetic roles in gastric cancer. We supposed that the Chinese population harboring at least one T allele of OPN rs4754 and/or at least one A allele of OPN rs9138 benefited protective effects on gastric carcinogenesis.
Intriguingly, OPN rs1126772 with the minor allele G was also associated with the risk of gastric cancer (P = 0.042, OR 1.279, 95 % CI 1.008–1.622). The SNP rs1126772 (+1083A/G) located in the 3′-UTR region. By means of the database of polymorphic microRNA target site (PolymiRTS) (Ziebarth et al. 2012), we predicted the A to G transition of rs1126772 of OPN interrupted a non-conservative microRNA binding site in the 3′-UTR of the OPN gene. MicroRNAs restrained proteins expression at the translation levels and affected their target mRNAs stability (Baek et al. 2008); thus, OPN expression was deregulated. Our clinical data also indicated that heterozygous genotype AG of rs1126772 revealed associations with TNM (III + IV) stage (P = 0.025) and poorly differentiation (P = 0.031), suggesting this genetic polymorphism played an essential role in progression of gastric cancer. Further analysis of OPN gene rs1126772 would be a valuable indicator for predicting occurrence and development of gastric cancer.
In our study, we found that the TAA haplotype of OPN containing the minor alleles of rs4754 and rs9138 and the major allele of rs1126772 significantly reduced risk of gastric cancer (P = 1.0 × 10−4, OR 0.640, 95 %CI 0.509–0.805), while the CGC haplotype of the three variants conferred increased risk of gastric cancer (P = 0.044, OR 1.279, 95 % CI 1.008–1.622). These results demonstrated the three SNPs felt into a strong linkage in combination to affect susceptibility to gastric cancer. The SNP rs11728697 locating in the exon 3 region exhibited strong linkage with rs1126772 (5.2 kb to rs11728697, D′ = 0.951, r 2 = 0.525, data not shown). Also, when we combined rs11728697, rs4754, rs9138 and rs1126772 to analyze the combination effect of haplotypes, we found that the haplotypes of CTAA and CCAC of the four SNPs were significantly associated with gastric cancer risk (P = 0.003 and P = 0.013, respectively). The force of the unfavorable C allele at rs4754 as well as rs9138 was stronger far beyond the protective A allele at rs1126772; thus, the overall effect of this haplotype was prone to elevating gastric cancer risk (P = 0.013, OR 1.306, 95 % CI 1.056–1.617). Haplotype analysis might provide more valuable evidence to explore genetic association of these polymorphic sites with gastric cancer.
CD44 belongs to cell surface adhesion molecule family and is a crucial receptor for OPN. Our study displayed the SNP rs353639 minor allele C of CD44 was associated with elevated risk of gastric cancer (P = 0.047, OR 1.334, 95 % CI 1.003–1.772). The SNP rs353639 locates in the intron region, which is close to the transcriptional start position of CD44. According to the F-SNP database, this variant was predicted to regulate transcriptional level of CD44 (Lee and Shatkay 2008). We hypothesized that the A to C variation of rs353639 might change transcriptional factor binding to the polymorphic region of the CD44 gene. Haplotype analysis of rs353644-G, rs353639-C and rs353630-C further verified that the C allele of rs353639 would increase the risk of gastric cancer (P = 0.044, OR 1.436, 95 % CI 1.015–2.031). It would be helpful to discover which transcriptional factor binding site was affected as a result of change of this polymorphism.
Previous investigation showed the wild-type genotype CC of CD44 rs8193 was correlated with a shorter TTR in colon cancer (Gerger et al. 2011). Likewise, our study revealed patients carrying the mutant homozygous genotype TT of the SNP rs8193 were associated with smaller tumor size and no serosa invasion compared to the CC genotype carriers (P = 0.029 and P = 0.019, respectively). We speculated that the wild type of rs8193 might be a potential indicator for tumor growth and progression. A recent study in the Chinese population suggested the GG and AG genotype of CD44 rs4756195 increased the risk of breast cancer, and patients carrying the GG genotype might hold poor prognosis (Zhou and Wu 2012), in accordance with our data that the AA genotype of the SNP rs4756195 carriers was correlated with no serosa invasion compared to the GG genotype (P = 0.028). These data provided such a evidence that rs4756195 polymorphism was closely associated with tumor development, at least in the Chinese Han population. Besides, we found correlations between other CD44 polymorphisms and clinicopathological subgroups, including rs1071695 CT + TT to serosa invasion (P = 0.033) and TNM (III + IV) stage (P = 0.022), rs353644 GG and rs3794107 AT + TT to histological type (P = 0.029 and P = 0.000, separately), rs16927042 CG to histological type (P = 0.003) and salted food (P = 0.034), rs16927061 GA + AA to female (P = 0.023), rs11821102 AG + AA to no smoking (P = 0.014), rs353619 TC + TT to family history (P = 0.007) and tumor location (P = 0.029), separately, indicating that these SNPs of the CD44 gene might lead to development of gastric cancer and were significantly associated with risk factors for gastric cancer. Hence, functional and biological significance of these SNPs should be elucidated under future consideration.
Numerous studies identified the biological significances of OPN and its interaction with CD44 in normal cellular activities, including adhesion, migration and proliferation (Raheja et al. 2008; Weber et al. 1996; Zohar et al. 2000). The interaction of OPN and CD44 contributed to malignant phenotypes, such as tumorigenesis, tumor progression, invasiveness and metastasis (Lee et al. 2007; Teramoto et al. 2005). In this study, we observed gastric mucosal tissues showed negative immunoreactivity of OPN and CD44. Positive expression of OPN was significantly correlated with serosa invasion of tumor cells (P = 0.013) and advanced TNM stage of gastric cancer (P = 0.003). The possible mechanisms that OPN correlated with invasion and progression of gastric cancer might be involved in that: (1) ECM degradation and migration through up-regulating MMPs and uPA (Chen et al. 2011); (2) NF-κB and/or PI3K/Akt signal pathways activated, inhibiting tumor cell apoptosis and promoting cell proliferation (Fong et al. 2009); and (3) OPN induced VEGF to facilitate tumor angiogenesis (Tang et al. 2008). The activations described above took place via binding of OPN to integrin and/or CD44. In view of our study, there was a significant correlation of CD44 expression with larger size of tumor growth (P = 0.005). We also detected that predominant expression of OPN and CD44 simultaneously associated with lymph node metastasis in gastric cancer (P = 0.002 and P = 0.023, respectively). Taking into consideration of the results that OPN expression was significantly correlated with CD44 (P = 0.01), we supposed that OPN, via its interaction with CD44 and subsequent downstream signaling, conduced to tumor cell migration and metastasis in gastric cancer. One previous study revealed OPN could contribute enhancement of survival and proliferation in gastric carcinoma cells through the interaction with CD44 variant isoforms (Lee et al. 2007). The fundamental mechanism of this effect was via Src kinase signaling pathway upon OPN binding to CD44, followed by inside out integrin activation. Another investigation demonstrated that OPN existed as an integral component of CD44–erzin/radixin/moesin (ERM) complex involved in metastatic cells (Zohar et al. 2000). Besides, Teramoto et al. (2005) showed that OPN, in interaction with CD44, motivated tumorigenesis in transformed fibroblast cells. In accordance with these investigations, our data might suggest that strong effects of OPN and CD44 interaction would aggravate the malignant phenotypes and aggressiveness in gastric cancer cells.
In this study, we demonstrated that gastric cancer expressed OPN and CD44. However, we failed to find statistically significant effect of OPN and CD44 variants on protein expressions in the gastric cancer cells. OPN was expressed in a variety of immune cells, including macrophages, dendritic cells and T lymphocytes, and modulated both innate and adaptive immune responses (Wang and Denhardt 2008). Polarization of Th cells to the Th2 phenotypes, a critical aspect of cell-mediated immunity, was influenced by production of OPN (Ashkar et al. 2000). OPN interacted with CD44 to inhibit Th2 cytokine IL-10 expression (Ashkar et al. 2000) and probably participated in chronic inflammatory reaction, such as autoimmune atrophic gastritis which was a potential risk factor for gastric carcinogenesis (Neumann et al. 2013). In addition, previous investigations indicated that increased serum OPN and CD44 levels were, respectively, associated with progression of non-small cell lung cancer (Rud et al. 2013) and gastric carcinoma (Saito et al. 1998). Therefore, we supposed that the polymorphisms in OPN and CD44 genes might induce potential gastric carcinogenesis via altering the protein expression in immune cells, rather than in epithelial cells. The aforementioned hypotheses remained to be investigated.
In conclusion, our investigation indicated that variations of OPN and CD44 exhibited significant associations with susceptibility, progression and metastasis in advanced gastric cancer. Expression of OPN might contribute to aggressive and malignant phenotypes of gastric cancer cells in interaction with CD44. Our data provided new insight into clinical implications in treatment and prognosis of gastric cancer. Blocking OPN and CD44 expression might become potential therapeutic strategies for gastric cancer in the Chinese Han population.
References
Ando T, Ishikawa T, Kato H et al (2009) Synergistic effect of HLA class II loci and cytokine gene polymorphisms on the risk of gastric cancer in Japanese patients with Helicobacter pylori infection. Int J Cancer 125:2595–2602. doi:10.1002/ijc.24666
Ashkar S, Weber GF, Panoutsakopoulou V et al (2000) Eta-1 (osteopontin): an early component of type-1 (cell-mediated) immunity. Science 287:860–864
Baek D, Villen J, Shin C, Camargo FD, Gygi SP, Bartel DP (2008) The impact of microRNAs on protein output. Nature 455:64–71. doi:10.1038/nature07242
Bendardaf R, Algars A, Elzagheid A et al (2006) Comparison of CD44 expression in primary tumours and metastases of colorectal cancer. Oncol Rep 16:741–746
Bhattacharya SD, Garrison J, Guo H, Mi Z, Markovic J, Kim VM, Kuo PC (2010) Micro-RNA-181a regulates osteopontin-dependent metastatic function in hepatocellular cancer cell lines. Surgery 148:291–297. doi:10.1016/j.surg.2010.05.007
Bourguignon LY, Zhu H, Shao L, Zhu D, Chen YW (1999) Rho-kinase (ROK) promotes CD44v(3,8-10)-ankyrin interaction and tumor cell migration in metastatic breast cancer cells. Cell Motil Cytoskeleton 43:269–287. doi:10.1002/(SICI)1097-0169(1999)43:4<269::AID-CM1>3.0.CO;2-5
Cartegni L, Chew SL, Krainer AR (2002) Listening to silence and understanding nonsense: exonic mutations that affect splicing. Nat Rev Genet 3:285–298. doi:10.1038/nrg775
Castelli EC, Moreau P, Oya e Chiromatzo A et al (2009) In silico analysis of microRNAS targeting the HLA-G 3′ untranslated region alleles and haplotypes. Hum Immunol 70:1020–1025. doi:10.1016/j.humimm.2009.07.028
Catalano V, Labianca R, Beretta GD, Gatta G, de Braud F, Van Cutsem E (2009) Gastric cancer. Crit Rev Oncol Hematol 71:127–164. doi:10.1016/j.critrevonc.2009.01.004
Chen RX, Xia YH, Xue TC, Zhang H, Ye SL (2011) Down-regulation of osteopontin inhibits metastasis of hepatocellular carcinoma cells via a mechanism involving MMP-2 and uPA. Oncol Rep 25:803–808. doi:10.3892/or.2010.1116
Conne B, Stutz A, Vassalli JD (2000) The 3′ untranslated region of messenger RNA: a molecular ‘hotspot’ for pathology? Nat Med 6:637–641. doi:10.1038/76211
Dai N, Bao Q, Lu A, Li J (2007) Protein expression of osteopontin in tumor tissues is an independent prognostic indicator in gastric cancer. Oncology 72:89–96. doi:10.1159/000111108
D’Alfonso S, Barizzone N, Giordano M et al (2005) Two single-nucleotide polymorphisms in the 5′ and 3′ ends of the osteopontin gene contribute to susceptibility to systemic lupus erythematosus. Arthritis Rheum 52:539–547. doi:10.1002/art.20808
Denhardt DT, Noda M, O’Regan AW, Pavlin D, Berman JS (2001) Osteopontin as a means to cope with environmental insults: regulation of inflammation, tissue remodeling, and cell survival. J Clin Invest 107:1055–1061. doi:10.1172/JCI12980
Doventas A, Bilici A, Demirell F, Ersoy G, Turna H, Doventas Y (2012) Prognostic significance of CD44 and c-erb-B2 protein overexpression in patients with gastric cancer. Hepatogastroenterology 59:2196–2201. doi:10.5754/hge10498
Fisher LW, Jain A, Tayback M, Fedarko NS (2004) Small integrin binding ligand N-linked glycoprotein gene family expression in different cancers. Clin Cancer Res 10:8501–8511. doi:10.1158/1078-0432.CCR-04-1072
Fong YC, Liu SC, Huang CY et al (2009) Osteopontin increases lung cancer cells migration via activation of the alphavbeta3 integrin/FAK/Akt and NF-kappaB-dependent pathway. Lung Cancer 64:263–270. doi:10.1016/j.lungcan.2008.09.003
Gerger A, Zhang W, Yang D et al (2011) Common cancer stem cell gene variants predict colon cancer recurrence. Clin Cancer Res 17:6934–6943. doi:10.1158/1078-0432.CCR-11-1180
Giacopelli F, Marciano R, Pistorio A, Catarsi P, Canini S, Karsenty G, Ravazzolo R (2004) Polymorphisms in the osteopontin promoter affect its transcriptional activity. Physiol Genomics 20:87–96. doi:10.1152/physiolgenomics.00138.2004
Hamajima N, Naito M, Kondo T, Goto Y (2006) Genetic factors involved in the development of Helicobacter pylori-related gastric cancer. Cancer Sci 97:1129–1138. doi:10.1111/j.1349-7006.2006.00290.x
Higashiyama M, Ito T, Tanaka E, Shimada Y (2007) Prognostic significance of osteopontin expression in human gastric carcinoma. Ann Surg Oncol 14:3419–3427. doi:10.1245/s10434-007-9564-8
Imano M, Satou T, Itoh T et al (2009) Immunohistochemical expression of osteopontin in gastric cancer. J Gastrointest Surg 13:1577–1582. doi:10.1007/s11605-009-0955-y
Jansson M, Panoutsakopoulou V, Baker J, Klein L, Cantor H (2002) Cutting edge: attenuated experimental autoimmune encephalomyelitis in eta-1/osteopontin-deficient mice. J Immunol 168:2096–2099
Jin Y, Tong DY, Tang LY, Chen JN, Zhou J, Feng ZY, Shao CK (2012) Expressions of osteopontin (OPN), alphanubeta3 and Pim-1 associated with poor prognosis in non-small cell lung cancer (NSCLC). Chin J Cancer Res 24:103–108. doi:10.1007/s11670-012-0103-1
Ladeiras-Lopes R, Pereira AK, Nogueira A, Pinheiro-Torres T, Pinto I, Santos-Pereira R, Lunet N (2008) Smoking and gastric cancer: systematic review and meta-analysis of cohort studies. Cancer Causes Control 19:689–701. doi:10.1007/s10552-008-9132-y
Lee PH, Shatkay H (2008) F-SNP: computationally predicted functional SNPs for disease association studies. Nucleic Acids Res 36:D820–D824. doi:10.1093/nar/gkm904
Lee JL, Wang MJ, Sudhir PR, Chen GD, Chi CW, Chen JY (2007) Osteopontin promotes integrin activation through outside-in and inside-out mechanisms: OPN-CD44 V interaction enhances survival in gastrointestinal cancer cells. Cancer Res 67:2089–2097. doi:10.1158/0008-5472.CAN-06-3625
Lee TY, Lin JT, Wu CC et al (2013) Osteopontin promoter polymorphisms are associated with susceptibility to gastric cancer. J Clin Gastroenterol 47:e55–e59. doi:10.1097/MCG.0b013e31827b9325
Likui W, Hong W, Shuwen Z (2010) Clinical significance of the upregulated osteopontin mRNA expression in human colorectal cancer. J Gastrointest Surg 14:74–81. doi:10.1007/s11605-009-1035-z
Lin YH, Yang-Yen HF (2001) The osteopontin-CD44 survival signal involves activation of the phosphatidylinositol 3-kinase/Akt signaling pathway. J Biol Chem 276:46024–46030. doi:10.1074/jbc.M105132200
Lin F, Li Y, Cao J et al (2011) Overexpression of osteopontin in hepatocellular carcinoma and its relationships with metastasis, invasion of tumor cells. Mol Biol Rep 38:5205–5210. doi:10.1007/s11033-010-0671-4
Maver A, Medica I, Salobir B, Tercelj M, Peterlin B (2009) Genetic variation in osteopontin gene is associated with susceptibility to sarcoidosis in Slovenian population. Dis Markers 27:295–302. doi:10.3233/DMA-2009-0675
Neumann WL, Coss E, Rugge M, Genta RM (2013) Autoimmune atrophic gastritis–pathogenesis, pathology and management. Nat Rev Gastroenterol Hepatol 10:529–541. doi:10.1038/nrgastro.2013.101
Ponta H, Sherman L, Herrlich PA (2003) CD44: from adhesion molecules to signalling regulators. Nat Rev Mol Cell Biol 4:33–45. doi:10.1038/nrm1004
Raheja LF, Genetos DC, Yellowley CE (2008) Hypoxic osteocytes recruit human MSCs through an OPN/CD44-mediated pathway. Biochem Biophys Res Commun 366:1061–1066. doi:10.1016/j.bbrc.2007.12.076
Rud AK, Boye K, Oijordsbakken M et al (2013) Osteopontin is a prognostic biomarker in non-small cell lung cancer. BMC Cancer 13:540. doi:10.1186/1471-2407-13-540
Saito H, Tsujitani S, Katano K, Ikeguchi M, Maeta M, Kaibara N (1998) Serum concentration of CD44 variant 6 and its relation to prognosis in patients with gastric carcinoma. Cancer 83:1094–1101
Samson PS, Escovidal LA, Yrastorza SG, Veneracion RG, Nerves MY (2002) Re-study of gastric cancer: analysis of outcome. World J Surg 26:428–433. doi:10.1007/s00268-001-0243-9
Tang H, Wang J, Bai F et al (2008) Positive correlation of osteopontin, cyclooxygenase-2 and vascular endothelial growth factor in gastric cancer. Cancer Invest 26:60–67. doi:10.1080/07357900701519279
Teramoto H, Castellone MD, Malek RL, Letwin N, Frank B, Gutkind JS, Lee NH (2005) Autocrine activation of an osteopontin-CD44-Rac pathway enhances invasion and transformation by H-RasV12. Oncogene 24:489–501. doi:10.1038/sj.onc.1208209
Tolg C, Hofmann M, Herrlich P, Ponta H (1993) Splicing choice from ten variant exons establishes CD44 variability. Nucleic Acids Res 21:1225–1229
Wang KX, Denhardt DT (2008) Osteopontin: role in immune regulation and stress responses. Cytokine Growth Factor Rev 19:333–345. doi:10.1016/j.cytogfr.2008.08.001
Wang Y, Yan W, Lu X et al (2011) Overexpression of osteopontin induces angiogenesis of endothelial progenitor cells via the avbeta3/PI3 K/AKT/eNOS/NO signaling pathway in glioma cells. Eur J Cell Biol 90:642–648. doi:10.1016/j.ejcb.2011.03.005
Weber GF, Ashkar S, Glimcher MJ, Cantor H (1996) Receptor–ligand interaction between CD44 and osteopontin (Eta-1). Science 271:509–512
Weber GF, Ashkar S, Cantor H (1997) Interaction between CD44 and osteopontin as a potential basis for metastasis formation. Proc Assoc Am Physicians 109:1–9
Weber GF, Bronson RT, Ilagan J, Cantor H, Schmits R, Mak TW (2002) Absence of the CD44 gene prevents sarcoma metastasis. Cancer Res 62:2281–2286
Winder T, Ning Y, Yang D et al (2011) Germline polymorphisms in genes involved in the CD44 signaling pathway are associated with clinical outcome in localized gastric adenocarcinoma. Int J Cancer 129:1096–1104. doi:10.1002/ijc.25787
Wu CY, Wu MS, Chiang EP et al (2007) Elevated plasma osteopontin associated with gastric cancer development, invasion and survival. Gut 56:782–789. doi:10.1136/gut.2006.109868
Wu IC, Wu MT, Chou SH et al (2008) Osteopontin expression in squamous cell cancer of the esophagus. World J Surg 32:1989–1995. doi:10.1007/s00268-008-9609-6
Xia HZ, Du WD, Wu Q et al (2012) E-selectin rs5361 and FCGR2A rs1801274 variants were associated with increased risk of gastric cancer in a Chinese population. Mol Carcinog 51:597–607. doi:10.1002/mc.20828
Xiao M, Hu S, Zhang L, Huang J, Jiang H, Cai X (2013) Polymorphisms of CD44 gene and nasopharyngeal carcinoma susceptibility in a Chinese population. Mutagenesis 28:577–582. doi:10.1093/mutage/get035
Young MF, Kerr JM, Termine JD, Wewer UM, Wang MG, McBride OW, Fisher LW (1990) cDNA cloning, mRNA distribution and heterogeneity, chromosomal location, and RFLP analysis of human osteopontin (OPN). Genomics 7:491–502
Zhao F, Chen X, Meng T, Hao B, Zhang Z, Zhang G (2012) Genetic polymorphisms in the osteopontin promoter increases the risk of distance metastasis and death in Chinese patients with gastric cancer. BMC Cancer 12:477. doi:10.1186/1471-2407-12-477
Zhou X, Wu CY (2012) Association of CD44 polymorphisms with genetic susceptibilities and clinico-pathologic characteristics in breast cancer. Sichuan Da Xue Xue Bao Yi Xue Ban 43:807–811
Ziebarth JD, Bhattacharya A, Chen A, Cui Y (2012) PolymiRTS Database 2.0: linking polymorphisms in microRNA target sites with human diseases and complex traits. Nucleic Acids Res 40:D216–D221. doi:10.1093/nar/gkr1026
Zohar R, Suzuki N, Suzuki K, Arora P, Glogauer M, McCulloch CA, Sodek J (2000) Intracellular osteopontin is an integral component of the CD44-ERM complex involved in cell migration. J Cell Physiol 184:118–130. doi:10.1002/(SICI)1097-4652(200007)184:1<118:AID-JCP13>3.0.CO;2-Y
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Qiu, Y., Hu, Y., Zhang, ZY. et al. Genetic association of osteopontin (OPN) and its receptor CD44 genes with susceptibility to Chinese gastric cancer patients. J Cancer Res Clin Oncol 140, 2143–2156 (2014). https://doi.org/10.1007/s00432-014-1761-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-014-1761-9