
Abstract
The aim of this study was to provide normative data for the onset and tempo of puberty in healthy boys. The analyses are based on data that were collected and evaluated biannually on 1112 Turkish school children aged from 8 to 18 years and a subsample of 30 boys who had reached final height (FH). The data were analyzed cross-sectionally in the total group and longitudinally in the subsample. Mean age and height (Ht) at onset of puberty were 11.6 ± 1.2 years and 146.1 ± 7.7 cm, respectively. Peak height velocity (HtV) was 10.1 ± 1.6 cm. Total pubertal height gain was 26.4 ± 4.3 cm. The duration of puberty was 4.9 ± 0.6 years. Height at onset of puberty was positively correlated with FH (p < 0.0001) and with duration of puberty (p = 0.03). Body mass index at onset of puberty correlated negatively with age at onset of puberty (p < 0.009) and with the duration of puberty (p = 0.05) but not with FH. In conclusion, these results provide normative data for Ht and HtV for each testicular volume stage for boys in puberty. Height at onset of puberty is the most important determinant of FH. There is no secular trend for the onset of puberty. Weight does seem to affect the onset and tempo of puberty but not FH.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The timing of the onset of puberty depends on genetic and environmental factors. While there is ample evidence that the onset of puberty is occurring at increasingly younger ages [31], this finding is primarily based on studies of menarcheal age or breast development of girls [18, 31], and data on sexual maturation of boys analyzed together with the growth pattern throughout puberty are scarce [1, 13, 21, 24] and open to discussion with respect to secular trends [3, 11, 23, 30, 32, 41]. Some studies have reported that there is no notable earlier maturation of boys [3, 11, 30, 32], while a positive secular change has been reported for Swedish [23] and Hong Kong boys [41].
The objective of the present study was to provide normative data for the onset and tempo of puberty in Turkish boys, evaluate height velocity (HtV) at each testicular volume (TV) stage and analyze the growth parameters in puberty. We also compared the findings with those of a previous study on children of a similar background [27]. The analyses presented in this paper are based on findings from a large study on the growth and pubertal development of Turkish school children.
Subjects and methods
Data on height growth and pubertal development were collected between the years 1989 and 1999 by means of biannual visits to six primary and secondary level schools in Istanbul city. Children born in 1975 or in subsequent years were classified by socioeconomic level into groups based on previously reported criteria [28]. Of a total of 2016 boys, 1112 boys aged from 8 to 18 years evaluated as coming from a high socioeconomic class (Class1) were included in the present analysis. Class 1 denotes children whose mother has had more than 8 years of schooling and whose father has had more than 11 years of schooling and is either a businessman, a professional or a high official. Over time, measurements were repeated on these same children, but other children were also included in the study to provide adequate numbers for the older age groups. Thus, our sample consists of a mixture of children followed longitudinally over different periods of time. A total of 5160 measurements were performed on this group.
Approval from the Ministry of Education was obtained for the study. Informed consent was obtained from the parents of each child included in the study.
Chronological age was computed from the birth date reported by the child and from the school files. If a disagreement appeared between these two sources, the child was not included in the analysis. Chronological ages of the children were grouped according to age in years ± 3 months. Chronic or debilitating disease as well as cryptorchidism, epispadias or hypospadias were also reasons for exclusion.
Height (Ht) was measured in a standing position with bare feet, using a portable measuring device (Leicester Height Measure, Invicta Plastics, UK). A portable scale sensitive to 0.1 kg was used for the weight measurements, which were made with the children wearing a minimal amount of underclothes. All measurements were performed by either of the two trained technicians throughout the study. Ht measurements were repeated twice, and the mean value was calculated. In the case of a discrepancy exceeding 0.3 cm, a third measurement was done and the mean of the two closest values was used. Inter-observer error for Ht measurements was assessed by having the same two technicians, independent of one another, measure a random subsample of 30 children (15 girls and 15 boys). Intra-observer error was assessed by having each technician conduct two measurements performed 1 week apart on every child in another random subsample of 15 children (seven girls, eight boys). Inter- and intra-observer measurement errors, expressed as the standard deviation of the differences between these duplicate measurements, were 0.25 cm and 0.21 cm, respectively.
Final height (FH) was defined as the attainment of a HtV less than 0.5 cm/year. The measurement of TV was performed by one observer (RB) throughout the study by means of a Prader orchidometer. Pubic hair and axillary hair development stages were rated in accordance with the Tanner criteria [24]. An evaluation of pubertal stages was also done at 6-monthly intervals. Attainment of a TV of 4 ml was accepted as the onset of puberty. The duration of puberty was taken as the time period from attainment of a TV of 4 ml to final height.
HtV was calculated from the multiple measurements taken on each individual child. To analyze the data, we first grouped the children by their testicular volumes and then calculated the height velocities for each TV group. HtV at a certain TV was designated as the annual velocity following the attainment of that TV. Testicular volume for age was shown as percentile values.
In a subsample of 30 boys who were followed longitudinally until they reached their final height, age of peak height velocity (PHV) for each subject was estimated by plotting the measurements of the child on the growth chart and by taking the midpoint age between the two successive measurements (those preceding and following the most rapid height growth) as the age of PHV. Body mass index (BMI) was calculated as weight (kg)/ height (m2).
The data were entered in a FoxBase program and analyzed by using SPSS-PC (SPSS, Chicago, Ill.). Linear correlations were used to define the relationships between various parameters.
Results
Total group
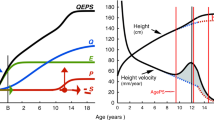
The mean age of onset of puberty was 11.6 ± 1.2 years for the total group. Age of onset of pubic hair was 12.3 ± 0.9 years and that of axillary hair was 13.1 ± 1.0 years. Mean Ht at onset of puberty was 146.1 ± 7.7 cm, and HtV in the year following the onset of puberty was 6.6 ± 3.4 cm/year.
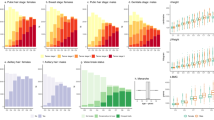
Median, mean values and ranges for TV at each age group are shown in Table 1. Percentile distribution of testicular volumes by age is given in Fig. 1. It will be noted that the median age of attainment of a TV of 4 ml was 11 years and that all boys reached a TV of 25 ml by age 18 years. As seen in Fig. 1, there is quite a large difference between boys of the same age with respect to the attainment of a certain TV. The 50th percentile values of TV given in recent reports [25, 26] have also been plotted in Fig. 1 for comparison of the data.

Testicular volume percentile growth curve in Turkish children and comparison with the Japanese (filled triangle) and Dutch (filled square) 50th percentile for testicular volume
The percentage of boys attaining the various pubic hair stages in each age group are given in Table 2. Pubic hair stage 2 was attained mostly between age 12 and 13 years.
Relationships between TV and age, Ht and HtV are shown in Table 3. Maximal HtV was observed after the testes attained a volume of 10 ml. The testes reached this volume at a mean age of 12.9 ± 0.8 years and at a mean height of 155.9 ± 7.9 cm. The deceleration in height increments noted after the testes reached a volume of 10 ml continued with increasing testis volume. Height continued to increase – albeit at a lower level – after the attainment of 25 ml in TV.
The subsample of longitudinally followed boys
In the subsample of 30 boys who were followed longitudinally to a FH, mean age at onset of puberty was 11.6 ± 0.6 years, and mean Ht at onset of puberty was 147.8 ± 6.8 cm at a mean velocity of 6.0 ± 1.7 cm. These values were similar to those of the total group. PHV was 10.1 ± 1.6 cm at an age of 13.7 ± 0.7 years. Height at PHV was 156.0 ± 8.4 cm. Mean TV at the time of PHV was 11.1 ± 2.0 ml (range 8 to 15 ml). Mean FH was determined to be 174.2 ± 1.6 cm, and mean total pubertal height gain (PHG), when calculated from onset of puberty to FH, was 26.4 ± 4.3 cm (range: 18.8–33.2 cm). The duration of puberty was 4.9 ± 0.6 years (range: 3.6 to 5.6 years) when estimated as the time period from a TV of 4 ml to final height. The time period from a TV of 4 ml to a TV of 25 ml was 3.4 ± 0.7 years (range: 2.1–5.0 years). Total pubertal height gain was 15.2 ± 2.3% of the final height.
Weight at onset of puberty of this subsample of boys was 42.1 ± 9.2 kg (range: 31.5–59.6 kg), and the respective BMI value was 19.1 ± 3.2 (range: 15.0 to 26.3).
Ht at onset of puberty was positively correlated with FH (p < 0.0001; r = 0.9 ) and also showed a positive correlation with duration of puberty (p = 0.03; r = 0.5). PHG during puberty showed correlations with duration of puberty (p < 0.0001; r = 0.7) and with FH (p = 0.03; r = 0.4). There were no significant correlations between age of onset of puberty and FH, total PHG, duration of puberty and PHV. Neither was there a correlation between age and height at onset of puberty. Age at onset of puberty correlated negatively with weight (p < 0.01; r = 0.5) and BMI (p < 0.009; r = 0.5). BMI at onset of puberty showed a weak but significant negative correlation (p = 0,05 ; r = 0.3) with the duration of puberty but not with FH.
Discussion
In this study, attainment of a TV of 4 ml was taken as the criterion for an assessment of age of onset of puberty in boys, as has classically been proposed [4]. However, the majority of reports on onset of puberty in boys refer to the G2 stage, which includes testis size, penile size and texture of scrotal skin [26]. There are also a number of authors who report that a TV of 3.0 ml should be the cut-off value for onset of puberty in boys [3, 42]. Despite these difficulties in comparing our results with other studies, age of onset of puberty in our study is in compliance with most European and American studies [5, 9, 15, 23, 24, 30, 32–34, 37, 40].
A previous study on sexual maturation in Turkish boys [27] born in 1955–1960 did not include measurements of TV, and the appearance of pubic hair was taken as the criterion for the assessment of onset of puberty. Mean age at onset of pubic hair development in that study was 11.8 years, as compared to 12.3 years in this present study. While it may not be totally appropriate to compare the two studies because of differences in methodology, these findings suggest that there appears to be no secular trend for early maturation in boys in our population. One explanation for the absence of a secular trend in pubertal development may be that the children in both studies were taken from amongst the higher socioeconomic levels of the Turkish population. The difficulties inherent in producing normative data in a developing country are well known, and only a sample from the upper strata of the population will suit the recommendations of the World Health Organization (WHO) for obtaining reference values [8, 14, 29]. It must be added that the mixed population of Istanbul city is quite representative of the whole of Turkey [7, 10, 39]. Thus, the results of our study are in agreement with those from most of the studies from the Western world reporting no secular trend for boys [3, 11, 30, 32]. Indeed, reported ages for onset of puberty in boys in different studies throughout the decades do not show a consistent pattern for a secular trend through these years among different populations. Interestingly, the age at onset of puberty in Turkish children living in the Netherlands [12] seemed to be somehow older than those in the present study. One explanation may be that those children were of a lower socioeconomic class. On the other hand, the mean FH of these children from the Netherlands was similar to the FH in this study.
To our knowledge, this is the first study to report Ht and height velocity for each successive testicular volume stage in healthy boys (Table 3). HtV was highest after attainment of testicular volume of 10 ml. This is also shown in the data of longitudinally followed children where PHV was observed at a TV of 11.1 ± 2.0 ml. This study also presents TV growth charts between 8 and 18 years with seven percentile lines. The 50th centile line of our study parallels almost exactly recently published TV curves [25, 26], but is somewhat steeper and skewed to the left, indicating faster maturation in our children.
The different growth parameters, such as age at PHV, magnitude of PHV and FH, in the longitudinally followed boys in our study were within the ranges of corresponding values reported in most European and American studies [2, 3, 16, 20, 38]. The attainment of FH depends on several factors at interplay. One factor may be the differences in Ht at onset of puberty. The positive correlations found in our study between Ht at onset of puberty and FH indicate that the smaller the child is at onset of puberty, the smaller the FH will be, a finding which has been reported in other studies as well [35] .This result emphasizes the importance of Ht at the onset of puberty for the prediction of FH. Height at onset of puberty in our study –147.8 ± 6.8 cm – is similar to that reported by Tanner et al, as is the value for FH [38]. Another factor affecting FH may be the duration of puberty. The duration of puberty in our study is similar to values reported in previous studies [21, 24]. In the present study there was a positive correlation between Ht at onset of puberty and duration of puberty as well as a positive correlation between duration of puberty and total height gain in puberty. This may provide the explanation for the shorter child at onset of puberty having a shorter duration of puberty and a lesser pubertal height gain ending up with a reduced FH.
A number of studies have shown that age at onset of puberty is not correlated to the duration of puberty [21, 24], a finding which has been confirmed in our study as well. This result implies that the duration of puberty does not change with respect to age at onset of puberty.
It has been reported that there is no difference in FH between early and late maturers [13, 22, 36]. We also found no evident correlation between age at onset of puberty and PHV, total pubertal height gain or FH. These results are in agreement with those obtained in a study with Swiss children [20]. Thus, it may be concluded that height attained at onset of puberty is the main factor affecting FH.
It is also noteworthy that weight and BMI at onset of puberty are negatively correlated to age at onset of puberty, implying that the heavier the child is, the earlier the puberty. This relation that body fat or BMI influences the timing of puberty has been shown in several studies [17, 19], mostly in girls, but has not been a consistent finding in boys [6]. In Dutch children [11], while weight and Ht showed an increase over the years, no secular trend was noted for the onset of puberty in boys. In fact, age of attainment of genital stage 2 showed a tendency to increase over the years, as was also noted in our study. This shows that the underlying factors for the secular trend for puberty are multifactorial and cannot simply be explained only by the trend in weight increase. On the other hand, the negative correlation that we found between BMI at onset of puberty and the duration of puberty implies that BMI is possibly effective on the tempo of puberty.
In conclusion, there does not seem to be a secular trend for the onset of puberty for the boys in our population. Weight at onset of puberty does seem to affect the age of onset and tempo of puberty – namely, that the heavier the boy is at onset of puberty, the earlier and faster the puberty will be, but this does not appear to affect the FH. This is the first study to give Ht and HtV for each testicular volume stage for boys in puberty. The HtV calculated for each testicular volume may have a clinical implication in guiding the clinicians to evaluate the HtV of the adolescents at follow-up. As also confirmed by the findings in this study, the most important determinant of FH appears to be height at onset of puberty.
Abbreviations
- BMI:
-
body mass index
- Ht:
-
height
- HtV:
-
height velocity
- FH:
-
final height
- PGS:
-
pubertal growth spurt
- PHG:
-
pubertal height gain
- PHV:
-
peak height velocity
- TV:
-
testicular volume
References
Abbasi V (1998) Growth and normal puberty. Pediatrics 102:7–11
Berkey CS, Dockery DW, Wang X, Wypij D, Ferris B Jr (1993) Longitudinal height velocity Standard for US adolescents. Stat Med 12:403–414
Biro FM, Lucky AW, Huster GA, Morrison JA (1995) Pubertal staging in boys. J Pediatr 127:100–102
Bourguignon JP (2004) Control of the onset of puberty. In:Pescovitz OH, Eugster EA (eds) Pediatric endocrinology: mechanisms, manifestations, and management. Lippincott Williams and Wilkins, New York, London, pp 285–298
Buckler J (1990) A longitudinal study of adolescent growth. Springer, London
Buckler J (1998) Growth at adolescence. In: Kelnar CJH, Savage MO, Stirling HF, Saenger P (eds) Growth disorders: pathophysiology and treatment. Chapman and Hall Medical, London, pp 179–193
Devlet Istatistik Enstitusu (2003) 2000 Census of population: social and economic characteristics, Devlet Istatistik Enstitusu, Ankara
Dibley MJ, Goldsby JB, Staehling NW, Trombridge FL (1987) Development of normalized curves for the international growth reference: historical and technical. Am J Clin Nutr 46:736–748
Dober I, Kiralfalvi L (1993) Pubertal development in South-Hungarian boys and girls. Ann Hum Biol 20:71–74
Duben A, Behar C (1991) Istanbul households. Marriage, family and fertility 1880–1990. Cambridge University Press, Cambridge, pp 24–25
Fredriks AM, Van Buuren S, Burgmeijer RJ, Meulmeester JF, Beuker RJ, Brugman E, Roede MJ, Verloove-Vanhorick SP, Wit JM (2000) Continuing positive secular growth change in the Netherlands 1955–1997. Pediatr Res 47:316–323
Fredriks AM, Van Buuren S, Jeurissen SER, Dekker FW, Verloove-Vanhorick SP, Wit JM (2003) Height, weight, body mass index and pubertal development reference values for children of Turkish origin in the Netherlands. Eur J Pediatr 162:788–793
Gasser T, Sheehy A, Molinari L, Largo RH (2001) Growth of early and late matures. Ann Hum Biol 28:328–336
Garza C, Onis de M for the WHO Multicentre Growth Reference Study Group (2004) Rationale for developing a new international growth reference. Food Nutr Bull 25[Suppl 1]:S5–S14
Hagg U, Taranger J (1991) Height and height velocity in early, average and late maturers followed to the age of 25: a prospective longitudinal study of Swedish urban children from birth to adulthood. Ann Hum Biol 18:47–56
Hauspie R (1979) Adolescent growth. In: Johnston FE, Roche AF, Susanne C (eds) Human Physical growth and maturation. Nato Advanced Study Institutes Series. Plenum Press, New York, pp 161–175
He Q, Karlberg J (2001) BMI in childhood and its association with height gain, timing of puberty and final height. Pediatr Res 49:244–251
Kaplowitz PB, Oberfield SE and the Drug and Therapeutics and Executive Committees of the Lawson Wilkins Pediatric Endocrine Society (1999) Re-examination of the age limit for defining when puberty is precocious in girls in the Unites States: implications for evaluation and treatment. Pediatrics 104:936–941
Karlberg J (2002) Secular trends in pubertal development. Horm Res 47[Suppl 2]:19–30
Largo RH, Gasser TH, Prader A, Stuetzle W, Huber PJ (1978) Analysis of the adolescent growth spurt using smoothing spline functions. Ann Hum Biol 5:421–434
Largo RH, Prader A (1983) Pubertal development in Swiss boys. Helv Paediat Acta 38:211–228
Lindgren G (1978) Growth of school children with early, average and late ages of peak height velocity. Ann Hum Growth 5:253–267
Lindgren G (1996) Pubertal stages 1980 of Stockholm children. Acta Paediatr 85:1365–1367
Marshall WA, Tanner JM (1970) Variations in the pattern of pubertal changes in boys. Arch Dis Child 45:13–23
Matsuo N, Anzo M, Sato S, Ogata T, Kamimaki T (2000) Testicular volume in Japanese boys up to the age of 15 years. Eur J Pediatr 159:843–845
Mul D, Fredriks AM, Van Buuren S, Oostdijk W, Verloove-Vanhorick SP, Wit JM (2001) Pubertal development in the Netherlands 1965–1997. Pediatr Res 50:479–486
Neyzi O, Alp H, Yalçindag A, Yakacikli S, Orphon A (1975) Sexual maturation in Turkish boys. Ann Hum Biol 2:251–259
Neyzi O, Furman A, Bundak R, Gunoz H,Darendeliler F, Bas F (2006) Growth references for Turkish children aged 6 to 18 years. Acta Pediatr 1–8 (preview article)
Onis de M, Garza C (2006) Foreword. Acta Pediatr 450[Suppl]:5–6
Papadimitriou A, Stephanou N, Papantzimas K, Glynos G, Philippidis P (2002) Sexual maturation of Greek boys. Ann Hum Biol 29:105–108
Rees M (1993) Menarche when and why? Lancet 342:375–376
Roche AF, Wellens R, Attie KM, Siervogel RM (1995) The timing of sexual maturation in a group of US white youths. J Pediatr Endocrinol Metab 8:11–18
Roede MJ (1990) The secular trend in the Netherlands. The third nation wide growth study. Arztl Jugendkd 81:330–336
Roy MP (1972) Evolution clinique de la puberte du garson (Etude longitudinale somatique de adolescents). In: C.R. 11th Reunion des Equipes chargees des etudes sur la Croissance et le developpement de l’Enfant normal. C.I.E, Paris, London, pp 185–190
Tanaka T, Komatsu K, Takada G, Miyashita M, Ohno T (1996) Prediction of adult height in healthy Japanese children. Acta Paediatr 417[Suppl 1]:57–60
Tanner JM (1987) Issues and advances in adolescent growth and development. J Adolesc Health Care 8:470–478
Tanner JM, Davies PSW (1985) Clinical longitudinal standards for height and height velocity for North American children. J Pediatr 107:317–329
Tanner JM, Whitehouse RH (1976) The adolescent growth spurt of boys and girls of the Harpenden growth study. Ann Hum Biol 3:109–126
Turkish Demographic and Health Survey (2003) Preliminary Report (2004). Hacettepe University Institute of Population Studies and Ministry of Health, Ankara
Willers B, Engelherdt L, Pelz L (1996) Sexual maturation in East German boys. Acta Paediatr 85:785–788
Wong GW, Leung SS, Law WY, Yeung VT, Lau JT, Yeung WK (1996) Secular trend in the sexual maturation of southern Chinese boys. Acta Paediatr 85:620–662
Zachmann M, Prader A, Kind HP, Hafliger H, Budliger H (1974) Testicular volume during adolescence cross-sectional and longitudinal studies. Helv Paediatr Acta 29:61–72
Acknowledgements
We would like to thank our technicians Mine Şükür and Sibel Balaban for doing the measurements; Şükran Poyrazoğlu MD and Sema Eryílmaz MD for performing the physical examination of the children.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bundak, R., Darendeliler, F., Gunoz, H. et al. Analysis of puberty and pubertal growth in healthy boys. Eur J Pediatr 166, 595–600 (2007). https://doi.org/10.1007/s00431-006-0293-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-006-0293-y