
Abstract
Growth is a dynamic process and has a characteristic pattern with three major growth spurts: the postnatal spurt followed by rapid growth deceleration during infancy and early childhood; the mild mid-growth spurt around the age of 6–7 years that however remains invisible in most velocity charts; and the adolescent growth spurt that parallels full sexual maturation. The maximum peak in height velocity of the adolescent spurt tends to be higher in early than in late-maturing individuals. Body weight follows a very similar pattern. Short-term growth is characterised by irregular sequences of mini growth spurts at random intervals of a few days. Measurements at intervals of less than 24 h are affected by circadian variation.
Growth is the increase of size (amplitude) over time. But individuals differ in developmental tempo: their calendar age may not parallel their biological age. Good clinical practice attempts to separately assess tempo and amplitude. Three techniques are currently available to assess the physical aspect of tempo: (1) assessing skeletal maturity, (2) assessing the state of pubertal maturity and (3) plotting multiple records of height SDS. Human beings follow a cephalocaudal (head-to-tail) gradient of growth. Adolescent growth proceeds in a distal-to-proximal pattern. Sitting height is a useful parameter to estimate the trunk–leg proportion. Particularly in younger children, the increase in body length largely reflects the increase in leg length.
Secular trends in developmental tempo and in adolescent growth exist leading to very characteristic population patterns of growth when recorded at different historic moments.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Tempo
- Amplitude
- Maturity
- Home-made measurements
- Take-off
- Peak height velocity
- Distance curve
- Velocity curve
Introduction
After birth, the human development progresses through several states of maturation [1]. The transition from infancy to childhood by about age 3 years is characterised by the termination of maternal lactation, eating of soft and nutrient dense foods and the completion of deciduous tooth eruption. The juvenile stage spans from age 7 years to onset of the adolescent growth spurt at approximately age 10 for healthy girls and age 12 for boys. Juveniles are sexually immature, but physically and mentally capable of providing for much of their own food and care. The juvenile stage starts with a change in cognitive function, a shift from the preoperational to concrete operational stage. Near the end of the juvenile stage, sexual maturation begins, and one measurable effect is the adolescent growth spurt. The adolescent stage is the period from around the age of 13–14 years in boys, and 11–12 years in girls, to the end of the spurt and the almost complete termination of growth of the skeleton. The end of adolescence usually coincides with the eruption of the third molar (if present). Adulthood and reproductive maturity follow. Body height, weight, BMI and other anthropometric parameter can be plotted on distance curves . Distance curves indicate the amount of height, weight, BMI, etc. achieved at a given age; velocity curves , or rate of growth, indicate the annual increment at a given age. Velocity curves best coincide with the stages of maturation. Age at take-off (ATO) is the age just prior to the onset of the adolescent growth spurt; adolescent growth is the height increment between the ATO and final height.
Some children are short, others are tall. But what is short and tall? Short and tall are statistical terms; their definition is arbitrary. Conventionally a child is considered short, when height is below the third centile, and tall when height is above the 97th centile. The term centile indicates how many percent of the observations have lower values. The third centile indicates that 3 % are smaller/shorter/lighter than children of a reference population. Shortness and tallness per se do not imply a pathological condition, but children with growth disorders are more often found among children who are short or tall. Centiles can be converted into standard deviation scores (SDS) . SDS or Z-values are the differences between the individual measurements and the age- and sex-specific mean values of the reference population, divided by the standard deviation (SD) of the reference population. SDS or Z-values should be given preference over centiles.
At this point it appears necessary to briefly mention a very common, but ill-recognised dilemma. A short child is a child who is short. The statement is trivial and can be made after a single measurement. But a dilemma occurs when a child is repeatedly measured. Children never grow exactly parallel to their centiles. They can be short at one occasion and normal when measured later. When screening for short stature, up to 10 % of longitudinally measured children are temporarily caught at the third centile.
Growth is a target-seeking process [2]. Parental height strongly determines this target and, thus, can be used to predict this target. Tanner et al. [3] defined target height (TH) in centimetres as the sex-corrected mean parental height:
As the mean sex difference is typically 13 cm, +6.5 cm should be added for boys and –6.5 cm subtracted for girls. Tanner suggested a 95 % confidence interval of TH ± 10 cm for boys and TH ± 9 cm for girls, independent of the population height. Yet, this approach ignores the parent–parent correlation with r = 0.27: assortative mating describes that tall women tend to choose tall men and vice versa and short women rather tend to choose short men. The approach also ignores that the parent–offspring correlation is not 1.0, but r = 0.57 [4]. It is therefore recommended to replace the traditional Tanner approach by a formula that allows for assortative mating and the parent–offspring correlation.
We propose calculating the conditional target height SDS (cTHSDS) as follows [5]:
This estimate of target height has a 95 % confidence interval of ±1.64 SDS. The formula is independent of sex, and if parental height SDS is obtained from growth charts dating back one generation, the formula is also independent of secular height trends.
Growth is a dynamic process and shows a characteristic pattern with three major growth spurts: the postnatal spurt followed by rapid growth deceleration during infancy and early childhood; the mild mid-growth spurt around the age of 6–7 years that however remains invisible in most velocity charts, this spurt possibly relating to adrenarche and the rise in adrenal steroids; and the adolescent growth spurt that parallels full sexual maturation. The maximum peak in height velocity ( peak height velocity) of the adolescent spurt tends to be higher in early than in late-maturing individuals. Body weight follows a very similar pattern. The majority of children grow non-linearly, but documenting non-linearity is not trivial. Children should preferably be measured at annual or semi-annual intervals, but reality usually differs. In addition semi-annual intervals are still too long to describe short-term growth . Short-term growth is growth at much shorter, at weekly or even daily intervals. Short-term growth patterns are characterised by irregular sequences of mini growth spurts. Measurements at intervals of less than 24 h are affected by circadian variation. Circadian variation by far surpasses the average 24-h increments in height and weight. Height measurements are most reliable when performed in the evening hours; weight measurements are most reliable in the morning shortly after getting up.
Mini growth spurts are chaotic series of rapid height changes [6, 7]. In the American literature, this characteristic pattern of steep rises in height velocity followed by stagnation has been named saltation and stasis [8]. Time series analysis confirmed that mini growth spurts do not occur at strictly periodic intervals but at random intervals of a few days.
The analysis of short-term growth is difficult. It either requires highly accurate measuring techniques such as knemometry (lower leg length measurements [9, 10] for measuring child and infant growth [11]), or in case of conventional height measurements, it requires series of measurements and appropriate statistical analyses. It is good to know that increasing the number of measurements is trivial and that measurements can be obtained at home. Parents are usually very cooperative, and serial home-made measurements [12] are amazingly accurate. Figure 5.1 illustrates daily measures in a growth hormone (GH) deficient girl successfully treated with GH. Recent advances in statistics suggest using jump-preserving smoothing techniques for the analysis of serial height data [13].

Growth in a growth hormone (GH) deficient girl successfully treated with GH, measured daily by her parents. (Reprinted from Hermanussen M (ed). Auxology—studying human growth and development. Schweizerbart, Stuttgart, 2013 with kind permission of Schweizerbart, www.schweizerbart.de)
Tempo and Amplitude
Growth is the increase of size (amplitude) over time. But physical time is not directly relevant to the internal dynamics of growth. Individuals differ in developmental tempo: their calendar age may not parallel their biological age . A slow-maturing child needs more; a fast-maturing child needs less calendar years for reaching the same stage of maturity. The slow-maturing child appears younger and temporarily short; the fast-maturing child appears older and temporarily tall. Good clinical practice attempts to separately assess tempo and amplitude, but developmental tempo is an auxiliary construct. Whereas physical size is immediately measurable in absolute terms by metric scales (centimetres, kilogram, kg/m2, etc.), and physical time by calendars and clocks, there is no apparent metric scale for maturity. Three techniques are currently available to assess the physical aspect of tempo: (1) assessing skeletal maturity, (2) assessing the state of pubertal maturity, and (3) analysing multiple records of height standard deviation scores (SDS).
Skeletal maturity of the bones of the hand and wrist is assessed by several methods; the Greulich–Pyle method [14] in combination with the growth prediction tables of Bayley and Pinneau [15] and the Tanner–Whitehouse method [16, 17] are the most commonly used. Thodberg [18] suggested replacing the manual assessment of skeletal maturity by automatic techniques.
Pubertal maturity can be rated by pubertal signs but only in healthy individuals. In disorders of sexual development, these signs often fail to reflect the tempo of maturation.
Height measurements can be described in absolute terms, or they can be related to a reference population. This can be done by plotting measurements on centile charts or by transforming measurements into standard deviation or Z-scores (SDS) [12]. A suitable reference population may be the same ethnic group, or people from the same regional area, or a population that lives under similar conditions.
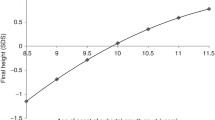
Multiple records of height standard deviation score (SDS) allow rough, but quick estimates of tempo. Figure 5.2 illustrates the height SDS of nine healthy boys (blue) and nine healthy girls (pink) from the first Zürich longitudinal study and shows the association between developmental tempo and patterns of SDS [19]. Delays in developmental tempo tend to result in steadily declining height SDS and a downward peak shortly before the individual’s peak height velocity and a rise thereafter, resembling a flat V. Tempo acceleration leads to upward rising in height SDS, with a characteristic peak in height SDS shortly after peak height velocity and a decline thereafter, resembling a roof.

Height SDS of nine healthy boys (blue colour) and nine healthy girls (pink colour) from the Zürich study (numbers correspond to the original numbering of the study population). The upper two rows of the graphs indicate children with average developmental tempo, the central rows show children with delayed developmental tempo, and the lower rows show children with accelerated developmental tempo. Vertical bars denote the age at peak height velocity (APHV) in years. (Reprinted from Hermanussen M (ed). Auxology—studying human growth and development. Schweizerbart, Stuttgart, 2013 with kind permission of Schweizerbart, www.schweizerbart.de)
Tempo is a very persistent characteristic throughout an individual’s development: fast-maturing children tend to be fast from early childhood onwards and remain accelerated until maturity. Slow-maturing children tend to be slow from the very beginning and usually remain delayed. Differences in developmental tempo become particularly apparent during adolescence—40 % (girls) and 50 % (boys) of adolescent height variation is variation in tempo [20, 21]. The tempo of physical maturation may grossly differ from the tempo of mental, emotional or social maturation.
Developmental tempo is influenced by a variety of factors of which malnutrition, illness and stress are only a few. Catch-up growth after short intermittent illnesses in otherwise healthy children is catch up in tempo. Even chronically ill patients are usually not short because of losses in amplitude, but because of delay in tempo. Aswani et al. [22] provide an excellent example in patients suffering from cystic fibrosis (CF) . CF patients grow poorly at all ages, they are short up to early adulthood, but they achieve normal final height in their mid-20s. Wiedemann et al. [23] stated that in a group of 4306 CF patients, the initially low height SDS increased with age and normal height was achieved by almost all patients when reaching the adult age.
Migrants and Adoptees
Migrants are persons who transitorily or permanently change residency. In Europe, migrants mainly originate from the Mediterranean region, the Near and Middle East, and Africa. Migration occurs in the direction of improvement in socioeconomic circumstances and usually exhibits significant effects on growth and development in children and adolescents. Migrants tend to become as tall as their host population. When two populations merge, the shorter population tends to catch up in height towards the taller target. Maya children born to families from Guatemala who migrated to the USA are 11.5 cm taller than Maya children living in Guatemala [24]. Non-adult migrants tend to mature early and reach taller adult height than their nonmigrant relatives. Migrants are prone to obesity [25, 26]. Growth references need to consider migration. Separate references for native and migrant populations have been published, e.g. for Turkish- and Moroccan-born Dutch [27, 28] and Turkish-born German children [29].
Adopting infants from a third-world environment may be considered a particular form of child migration. In Sweden, over 6800 children from India have been adopted during the last four decades [30]. Many were severely undernourished and suffered from infectious illnesses upon arrival, but their health improved when they were integrated in their foster families, and they usually caught up in height and weight. Only the severely stunted children caught up less. Low birth weight appears to be a limiting factor for later catch-up growth. Adopted girls tend to prematurely start pubertal development at 11.6 years (range of 7.3–14.6) which was earlier than Swedish (13.0 years) and wealthy Indian girls (12.4–12.9 years). The adolescent growth component was on average 1.5 years earlier, but the final height was reduced to 154 cm. Eight percent of the adopted Indian girls even remained 145 cm or shorter. It is not known why this phenomenon is not so frequently observed in adopted boys.
Proportions
Humans follow a cephalocaudal (head-to-tail) gradient of growth . A special feature of the human pattern is that between birth and puberty, legs grow relatively faster than other body segments. This gives the human species a distinctive body shape. Adolescent growth proceeds in a distal-to-proximal pattern. Body proportions change with age. First, the feet, the hands and the distal parts of the lower and upper extremities start to grow, thereafter the proximal, then the central parts of the skeleton. The peak height velocity of total body height may precede the peak height velocity of sitting height by several months. Rump growth can proceed into the third decade of life. The adolescent spurt is larger in early than in late-maturing children [31].
Proportional age defines the biological age by the change of head–trunk–extremity proportions. Sitting height is a useful parameter to estimate the trunk–leg proportion. Particularly in younger children, the increase in body length largely reflects the increase in leg length.
Also skeletal robustness (e.g. pelvic or relative elbow breadth) is subject to distinct changes both during individual life and in populations over periods of several decades. Skeletal robustness is associated with daily physical activity. A recent analysis of elbow breadth, pelvic breadth (bicristal) and thoracic depth and breadth of up to 28,975 healthy females and 28,288 healthy males aged 3–18 years from cross-sectional anthropological surveys performed between 1980 and 2012 by the Universities of Potsdam and Berlin, Germany, showed that relative elbow breadth and, to an even greater extent, absolute and relative pelvic breadth significantly decreased in both sexes since 1980 [32]. The trend towards slighter built coincides with the modern decline in physical activity and underscores the phenotypic plasticity of humans while adapting to new environmental conditions.
The Historic Aspect
The aspect of tempo and amplitude is not limited to individual growth, but it is obvious also in the population data as exemplified in Fig. 5.3. During World War II, Oslo schoolgirls suffered from marked growth impairment during the German occupation [33], but caught up later and achieved normal adult height. The Oslo growth impairment was impairment in tempo, limited to the time of hardship; it was not impairment in amplitude.

Oslo schoolgirls suffered from marked growth impairment during the German occupation [33], but caught up later and finally achieved normal adult height. (Reprinted from Hermanussen M (ed). Auxology—studying human growth and development. Schweizerbart, Stuttgart, 2013 with kind permission of Schweizerbart, www.schweizerbart.de)
Measuring tempo in a population is not easy. Menarcheal age has been used for this purpose. There is a marked secular trend in menarche. In most European countries, the average age at menarche decreases [34] from some 18 years in the mid-nineteenth century to about 16 years around 1900 and to modern values in the urban centres already in the 1930s, e.g. in Germany: 12.6 years in Leipzig 1934 and 13.3 years in Halle 1939 [35]. At present, the mean menarcheal age in Germany is 12.7 years (low social class), 13.0 years (high class), 12.5 years (migration background) and 12.9 years (no migration background) [36]. Menarcheal age in Mediterranean countries is about 1 year earlier than in Northern Europe. Menarcheal age in the USA has mildly declined over the past 40 years, with black girls maturing 0.5–1 year earlier [37].
The average age at onset of the adolescent growth spurt may also be taken as a substitute for adolescent maturation in a population. The faster a given population matures, the earlier the adolescents start their adolescent growth spurt. Quantifying the pattern of adolescent growth in a population needs some mathematical modelling. Among several models we preferentially use the Preece–Baines model [38] for this purpose. The model explicitly calculates the height and age at take-off ( HTO and ATO) and age at peak height velocity (APHV) and thus provides two useful parameters for estimating the state of maturation. The Preece–Baines model can be applied to population data, and it is mathematically not very sophisticated.
Table 5.1 illustrates the forward displacement of ATO, the rise of HTO , the adolescent growth and the adult height in six male Japanese growth surveys published in 1955, 1960, 1970, 1980, 1990 and 2000. Japanese boys in 2000 spurt about 1 year earlier than in 1955, and their adolescent growth is 6 cm larger than in 1955. The table illustrates that the secular trend in height is both a trend in tempo and a trend in amplitude.
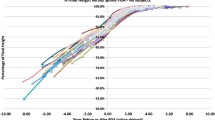
The intermingling of tempo and amplitude often leads to misinterpretation when analysing secular trends in populations. When depicting differences between average height and a reference for height, for the same populations at different historic moments, populations behave similar to individuals. Figure 5.4 exemplifies the differences between average height and the WHO standards/references for height [41] in modern and historic Japanese children [39, 40] (Satake, 2012, personal communication). At all ages, Japanese are shorter than WHO standards/references—Japanese differ in amplitude at all ages. But the patterns also show that the historic cohorts steadily decline in height compared with WHO height, with a downward peak at mid-adolescence and a rise thereafter, and that the modern cohorts (though still shorter than the reference at all ages) partially resemble the accelerated pattern in Fig. 5.2, with a characteristic peak in height SDS at mid-adolescence. Modern children are taller and they mature faster. At 12 years, modern boys are taller and biologically older than their fathers at age 12. The trend in tempo superimposes the trend in amplitude. The superimposition of the two trends needs to be disentangled. This is important for the understanding of secular changes in growth.

The rise in adult height observed in recent history is spectacular. Old World Europeans increased in height by some 11–19 cm since the mid-nineteenth century [42]. Interestingly this was different in Europeans who lived abroad. Late-nineteenth century white US conscripts were already almost as tall as today [43]. White South African males reached an average body height of near 172 cm at the turn of the nineteenth to twentieth century, with no remarkable trend since [44]. European Australians reached 175 cm at the beginning of the twentieth century [45]. The discrepancy in growth of white Europeans born within and outside the European continent strongly contrasts the notion that adult height is one of the most heritable human phenotypes [46]. The data rather support the vision that adult height depends on environmental cues.
This contradicts traditional concepts of growth as a target-seeking process [2]. Since decades, growth has been considered being regulated by genes, nutrition, health and the state of an individual’s social and economic environment. Social, economic and demographic history has produced multiple evidence for interactions between living conditions, technology, economy and body height [43, 47]: optimal conditions lead to marked improvements in the average height of populations; poor populations are short. But this evidence appears to only hold true at the population level. This concept fails to provide convincing explanations why the healthy and well-nourished members of poor populations are also short. Well-nourished and healthy people should be tall, but they are not when living among short and poor people. Growth appears to seek its target at the community level. Tall stature communities appear to generate tall people; short stature communities appear to generate short people. We named this the community effect in height [48–50].
At first view this idea appears bizarre, and it has already generated vivid debates. But evidence has accumulated that social and psychological phenomena are directly involved in the regulation of adult height. The pathomechanism of this regulation is still far from being understood. But it appears that self-determination, autonomy, democracy and happiness of the modern people tend to correlate with the recent trends in adolescent growth (Fig. 5.4). At this moment it is too early for any conclusive statements, but new evidence may provide more insights into the complex regulation of adolescent growth and lead to a better understanding of the plasticity of adult height [49].
References
Bogin BA. Patterns of human growth. 2nd ed. Cambridge: Cambridge University Press; 1999.
Tanner JM. Growth as a mirror of the condition of society: secular trends and class distinctions. In: Demirjian A, editor. Human growth: a multidisciplinary review. London: Taylor & Francis; 1986. pp. 3–34.
Tanner JM, Goldstein H, Whitehouse RH. Standards for children’s height at age 2–9 years allowing for height of parents. Arch Dis Child. 1970;45:755–62.
Luo ZC, Albertsson-Wikland K, Karlberg J. Target height as predicted by parental heights in a population- based study. Pediatr Res. 1998;44:563–71.
Hermanussen M, Cole TJ. The calculation of target height reconsidered. Horm Res. 2003;59:180–3.
Hermanussen M, Rol de Lama MA, F-Tresguerres JA, Grasedyck L, Burmeister J. Short-term growth: evidence for chaotic series of mini growth spurts in rat growth. Physiol Behav. 1998;64:7–13.
Hermanussen M. The analysis of short-term growth. Horm Res. 1998;49:53–64.
Lampl M, Johnson ML, Frongillo Jr EA. Mixed distribution analysis identifies saltation and stasis growth. Ann Hum Biol. 2001;28:403–11.
Hermanussen M, Geiger-Benoit K, Burmeister J, Sippell WG. Knemometry in childhood: accuracy and standardization of a new technique of lower leg length measurement. Ann Hum Biol. 1988;15:1–16.
Hermanussen M, Geiger-Benoit K, Burmeister J, Sippell WG. Periodical changes of short term growth velocity (“mini growth spurts”) in human growth. Ann Hum Biol. 1988;15:103–9.
Kaempf DE, Pflüger MS, Thiele AM, Hermanussen M, Linderkamp O. Influence of nutrition on growth in premature infants: assessment by knemometry. Ann Hum Biol. 1998;25:127–36.
Hermanussen M (ed). Auxology: studying human growth and development. Stuttgart: Schweizerbart; 2013.
Caino S, Kelmansky D, Adamo P, Lejarraga H. Short-term growth in healthy infants, schoolchildren and adolescent girls. Ann Hum Biol. 2006;33:213–26.
Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist. 2nd ed. Stanford: Stanford. Stanford University Press; 1959.
Bayley N, Pinneau SR. Tables for predicting adult height from skeletal age: revised for use with the Greulich-Pyle hand standards. J Pediatr. 1952;40:423–41, Erratum J Pediatr. 41:371.
Tanner JM, Goldstein H, Cameron N, Saunders WB, Healy MJR. Assessment of skeletal maturity and prediction of adult height. 3rd ed. Philadelphia: WB Saunders; 2001.
Tanner JM, Whitehouse RH, Marshall WA, Healy MJR, Goldstein H. Assessment of skeletal maturity and prediction of adult height (TW2 method). 2nd ed. London, New York, Paris, San Diego, San Francisco, Sidney, Tokyo, Toronto: Academic; 1983.
Thodberg HH. Clinical review: an automated method for determination of bone age. J Clin Endocrinol Metab. 2009;94:2239–44.
Hermanussen M. Auxology: an update. Horm Res Paediatr. 2010;74:153–64.
Hermanussen M, Meigen C. Phase variation in child and adolescent growth. Int J Biostat. 2007;3:1–16.
Molinari L, Hermanussen M. The effect of variability in maturational tempo and midparent height on variability in linear body measurements. Ann Hum Biol. 2005;32:679–82.
Aswani N, Taylor CJ, McGaw J, Pickering M, Rigby AS. Pubertal growth and development in cystic fibrosis: a retrospective review. Acta Paediatr. 2003;92:1029–32.
Wiedemann B, Steinkamp G, Sens B, Stern M. German cystic fibrosis quality assurance group: the German cystic fibrosis quality assurance project: clinical features in children and adults. Eur Respir J. 2001;17:1187–94.
Bogin B, Smith P, Orden AB, Varela Silva MI, Loucky J. Rapid change in height and body proportions of Maya American children. Am J Hum Biol. 2002;14:753–61.
Fredriks AM, van Buuren S, Hira Sing RA, Wit JM, Verloove-Vanhorick SP. Alarming prevalence of overweight and obesity for children of Turkish, Moroccan and Dutch origin in The Netherlands according to international standards. Acta Paediatr. 2005;94:496–8.
Kirchengast S, Schober E. Obesity among female adolescents in Vienna, Austria: the impact of childhood weight status and ethnicity. Br J Obstet Gynaecol. 2006;113:1188–94.
Fredriks AM, Buuren SV, Burgmeijer RJF, Meulmeester JF, Beuker RJ, Brugman E, Roede MJ, Verloove-Vanhorick SP, Wit JM. Continuing positive secular growth change in the Netherlands 1955–1997. Pediatr Res. 2000;47:316–23.
Fredriks AM. Growth diagrams. Fourth Dutch nation-wide survey. Doctorial dissertation. Leiden; 2004. pp. 91–104.
Redlefsen T, Commentz J, Meigen C, Hermanussen M. Reference values for height, weight and body mass index of German born Turkish children. Anthropol Anz. 2007;65:263–74.
Proos LA. Growth and development of Indian children adopted in Sweden. Indian J Med Res. 2009;130:646–50.
Shuttleworth FK. Sexual maturation and the physical growth of girls age six to nineteen. Monogr Soc Res in Child Develop. vol 2, no 5. Washington, DC: National Research Council; 1937.
Scheffler C, Hermanussen M. Is there an influence of modern life style on skeletal build? Am J Hum Biol. 2014;26:590–7.
Brundtland GH. Height, weight and menarcheal age of Oslo schoolchildren during the last 60 years. Ann Hum Biol. 1980;7:307–22.
van Wieringen JC. Secular growth changes. In: Falkner F, Tanner JM, editors. Human growth. vol 3, 2nd ed. New York, London: Plenum Press; 1986. pp. 307–31.
Lehmann A, Scheffler C, Hermanussen M. Evidence of seasonal variation in longitudinal growth of height in a sample of boys from Stuttgart Carlsschule, 1771–1793, using combined principal component analysis and maximum likelihood principle. Homo. 2010;61:59–63.
Kahl H, Schaffrath Rosario A, Schlaud M. Sexual maturation of children and adolescents in Germany. Results of the German. Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2007;50:677–85.
Kaplowitz P. Pubertal development in girls: secular trends. Curr Opin Obstet Gynecol. 2006;18:487–91.
Preece MA, Baines MJ. A new family of mathematical models describing the human growth curve. Ann Hum Biol. 1978;5:1–24.
Takahashi E, Atsumi H. Age differences in thoracic form as indicated by thoracic index. Hum Biol. 1955;27:65–74.
Technology. Report on school health survey 2003. Tokyo: National Printing Bureau; 2004. pp. 130–3.
WHO multicentre growth reference study group. WHO child growth standards. Acta Paediatr Suppl. 2006;95 Suppl 450:1–104.
Bodzsar BE, Susanne C. Secular growth changes in Europe. Budapest: Eotvos University Press; 1998.
Komlos J. Height and social status in eighteenth-century Germany. J Interdisciplinary Hist. 1990;20:607–21.
Henneberg M, van den Berg ER. Test of socioeconomic causation of secular trend: stature changes among favored and oppressed South Africans are parallel. Am J Phys Anthropol. 1990;83:459–65.
Henneberg M. Possible causes of secular trends in body size: lessons from the Southern Hemisphere. In: Schulze M, et al. editors. Homo: unsere Herkunft und Zukunft. Goettingen: Cuvillier Verlag; 2001. pp. 234–7.
Lettre G. Recent progress in the study of the genetics of height. Hum Genet. 2011;129:465–72.
Fogel RW. The escape from hunger and premature death, 1700–2100. Cambridge, New York, Melbourne: Cambridge University Press; 2004.
Aßmann C, Hermanussen M. Modeling determinants of growth: evidence for a community-based target in height? Pediatr Res. 2013;74:88–95.
Bogin B, Hermanussen M, Blum WF, Aßmann C. Sex, sport, IGF-1 and the community effect in height hypothesis. Int J Environ Res Public Health. 2015;12:4816–32.
Hermanussen M, Alt C, Staub K, Aßmann C, Groth D. The impact of physical connectedness on body height in Swiss conscripts. Anthropol Anz. 2014;71:313–27.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Hermanussen, M. (2016). Growth in Childhood and Puberty. In: Kumanov, P., Agarwal, A. (eds) Puberty. Springer, Cham. https://doi.org/10.1007/978-3-319-32122-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-32122-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-32120-2
Online ISBN: 978-3-319-32122-6
eBook Packages: MedicineMedicine (R0)