
Abstract
Mastitis, which is generally described as an inflammation of breast tissue, is a common and debilitating disease which frequently results in the cessation of exclusive breastfeeding and affects up to 33% of lactating women. The condition is a primary cause of decreased milk production and results in organoleptic and nutritional alterations in milk quality. Recent studies employing culture-independent techniques, including metagenomic sequencing, have revealed a loss of bacterial diversity in the microbiome of mastitic milk samples compared to healthy milk samples. In those infected, the pathogens Staphylococcus aureus, Staphylococcus epidermidis and members of corynebacteria have been identified as the predominant etiological agents in acute, subacute and granulomatous mastitis, respectively. The increased incidence of antibiotic resistance in the causative species is also a key cause of concern for treatment of the disease, thus leading to the need to develop novel therapies. In this respect, probiotics and bacteriocins have revealed potential as alternative treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the last decade, breastfeeding has been the subject of renewed attention in developed countries because of the demonstrated health benefits to the mother–child dyad [1, 2]. Consequently, international and national health organizations encourage exclusive breastfeeding during the first 6 months of life [3,4,5]. However, in certain cases, exclusive breastfeeding may not be an option for mothers owing to many reasons [6], with mastitis considered as the greatest cause of undesired weaning.
Mastitis, an inflammation of breast tissue, is an acute, devitalizing condition and a potentially serious illness that may lead to breast abscess and septic fever [7]. The main causes of mastitis are milk stasis and infection [3, 8]. Milk stasis is usually the primary cause and occurs when milk is not removed properly from the breast duct due to poor attachment of the infant, fruitless suckling and blockage of the ducts [3, 9]. It is widely accepted that most mastitic cases are related to changes in the microbiome of the mammary gland and that most mastitis-causing bacteria have the ability to form biofilms in the milk ducts which are quite narrow; this results in the impairment of milk flow and the retention of milk [10] (Fig. 1a, b). The incidence of lactational mastitis varies between 2 and 33% of lactating mothers [11, 12] and most episodes occur in the first 6 weeks postpartum [13]. According to epidemiologic studies, there are many factors which might be implicated in its occurrence [13,14,15,16]. Risk factors include age, with mothers under 21 and over 35 years having a decreased incidence [17], mastitis with a previous child [16], cracked or sore nipples, use of ointments, incorrect breastfeeding practices and peripartum antibiotherapy [8, 18, 19].

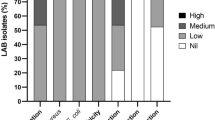
(Fig. 1c is reproduced from Patel et al. [20] which is licensed under the creative commons license http://creativecommons.org/licenses/by/4.0/)
Physiological breast anatomy (a) and mastitic enlarged duct (b). Milk production takes place at the duct system. When mastitis occurs, ducts are blocked due to the formation of bacterial biofilms. c Circos representation of the top most abundant bacterial genera from healthy milk samples and from subacute and acute mastitis milk samples
The aim of this review is to provide an overview of the latest findings in terms of the microbiological load involved in human mastitis, particularly at a time when the advances in sequencing technologies have provided an excellent platform to study both cultivable and non-cultivable microorganisms, giving a more accurate view of the microbiological dysbiosis which shapes this disease. The review also describes the available therapies to treat mastitis, the most common of which is antibiotics. As antibiotic resistance poses a major challenge to the success of this treatment, we examine alternative therapies, namely probiotics and bacteriocins, for which ongoing studies continue to provide promising results.
Source of bacteria in human milk
Traditionally, human milk was considered to be sterile and any bacteria found within were deemed to be contamination either from the mother’s skin or the infant’s mouth [21]. This has since been disproven by several studies which demonstrate that human milk contains its own microbiota [20, 22,23,24,25,26,27,28]. Despite this, the exact mechanisms by which these bacterial populations reach the mammary gland, and subsequently the milk, have not been fully elucidated.
Recent findings indicated that selected bacteria of the maternal gastrointestinal (GI) microbiota can reach the mammary gland through an entero-mammary pathway [23]. The mechanism involves dendritic cells and CD18+ cells which have the ability to transfer bacteria from the GI lumen to the lactating mammary gland [29, 30].
The skin may also be a major source of bacteria for human milk. Indeed, many species of bacteria associated with the skin, namely Staphylococcus and Corynebacterium, have been isolated from healthy human milk [25]. It is possible that these bacteria are relocated to the milk during ejection, specifically from the nipple, mammary areolas and montgomery glands, although it is worth noting that these species are also associated with mucosal surfaces of the body including that of the GI tract. In addition, retrograde flow of milk from the infant oral cavity to the mammary ducts has the potential to lead to cross-contamination of the milk. Moreover, the partner’s bacteria could contribute to bacterial populations in milk as it is known that partners share oral and skin microbiota [31, 32]. Fecal matter can also be a source of contamination in human milk when poor hygienic conditions exist [33,34,35].
All, or some, of these routes of bacterial transfer have the potential to contribute to the microbiota of human milk. As recent studies have indicated, healthy human milk does contain its own populations of bacteria which provide important health benefits not only for the nursing mother but also for the infant, with the suggestion that the microbiota of human milk may aid in establishing the commensal GI microbiota of the infant [11, 35,36,37,38].
How or why the transition from commensal colonization to infection occurs remains to be fully understood, however, several factors have been identified which may predispose women to the development of mastitis. These range from host factors such as genetics, the presence of polymorphisms and even blood grouping, to bacterial factors, e.g., virulence factors of the bacteria present, to medical influences including the use of antibiotics and the widespread administration of iron to prenatal women [10, 37].
Microorganisms detected in lactational mastitis
Lactational mastitis is classified into different categories depending on the course (acute, subacute and granulomatous, which is explained later) or the clinical manifestations (clinical or subclinical) [10]. Mastitis is a multifactorial disease caused by a range of different pathogens and is characterized by an alteration in the mammary microbiota [27, 38, 39]. Indeed, a metagenomic analysis of 20 milk samples (half from women with mastitis, while the other half were taken from healthy women) showed a noteworthy loss of bacterial diversity in the mastitic milk samples [26]. The latter is illustrated in Table 1 which records the genera detected in healthy human milk and mastitic human milk via culture-dependent and culture-independent analyses. The majority of the available literature is based on culture-independent approaches, however, the scientific community should be handling this data with precaution as there is some argument as to the appropriate controls for such studies. Salter et al. [40] and Glassing et al. [41] have both described the potential for incorrect results in low bacterial count samples owing to contamination or other artefacts which could explain the discrepancies between the healthy core microbiome reported by Hunt et al. [25] and Murphy et al. [28]. In a more recent study, the healthy core milk microbiome consisted of the genera Pseudomonas, Staphylococcus, Streptococcus, Elizabethkingia, Variovorax, Bifidobacterium, Flavobacterium, Stenotrophomonas, Brevundimonas, Chryseobacterium, Lactobacillus and Enterobacter [28], whereas Staphylococcus species dominated the mastitic milk samples with S. aureus and S. epidermidis being the dominant species in the microbiome of women diagnosed with acute and subacute mastitis, respectively [26]. In another study, sequencing of 16S rDNA of 32 human mastitic milk samples revealed the presence of 17 genera and 30 distinct species [42]. Proteobacteria was the predominant phylum accounting for 51.3% of the total followed by Firmicutes (37.8%) and included representatives from the classes Gammaproteobacteria, Alphaproteobacteria and Bacilli. The most frequently isolated genera included Pseudomonas (6 species) and Staphylococcus (4 species). The following species were frequently isolated; Staphylococcus species (87.5% of mastitic samples), S. aureus (75.0%), P. aeruginosa (53.1%) Klebsiella pneumoniae (43.8%) and Brevundimonas diminuta (38.0%). Recently, Mediano et al. [27] identified 5009 isolates from 1849 mastitic milk samples by classical, biochemical and/or molecular methods. Mean total bacterial count was 4.11 log10 colony forming units (cfu)/mL with Staphylococcus being the most commonly isolated bacterial group (97.57%) and S. epidermidis being the dominant species (91.56%) followed by S. aureus (29.74%). Streptococci and corynebacteria comprised the second (70.20%) and third (16.60%) most dominant groups, respectively. Most recently, a 16S rRNA gene-sequencing method of 50 human milk samples (16 subacute mastitic, 16 acute mastitic and 18 healthy control samples) revealed an enrichment of genera including Aeromonas, Staphylococcus, Ralstonia, Klebsiella, Serratia, Enterococcus and Pseudomonas in subacute and acute mastitic samples, while Acinetobacter, Ruminococcus, Clostridium, Faecalibacterium and Eubacterium were consistently depleted [20] (Fig. 1c). Moreover, dramatic enrichment of aerotolerant bacteria and depletion of obligate anerobes was observed during the infection. Lower microbial diversity was also a feature of the mastitic milk samples along with increased abundance of opportunistic pathogens including S. aureus, S. epidermidis, S. hominis, K. pneumoniae, Ser. marcescens, P. aeruginosa, E. faecalis, Bacillus subtilis, B. cereus and Escherichia coli. Marín et al. [43] analyzed the cultivable microbial diversity of 647 human mastitic milk samples using Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS) technology. The total staphylococcal count was 3.7 log10 cfu/mL with Staphylococcus genus being the most frequently isolated (94.1%) and S. epidermidis being the predominant species (87.6%) followed by S. aureus (22.1%), S. hominis (5.3%) and S. lugdunensis (3.3%). In agreement with the findings of Mediano et al. [27], streptococci were the second-most abundant group with a mean count of 3.47 log10 cfu/mL. Strep. mitis/oralis was the most common species (40.8%), while Strep. salivarius and Strep. parasanguinis were detected with frequencies of 36.8 and 14.4%, respectively. Corynebacteria occurred in 11% of the analyzed samples with the populations of C. tuberculostearicum and C. kropenstedtii reaching ratios of 3.6 and 2%, respectively. Similarly, Delgado et al. [44, 45] identified Staphylococcus as the predominant genus in mastitic milk samples using a combination of culture and molecular techniques where S. epidermidis was found to be the dominant species. Moreover, antibiotic resistance and the presence of the biofilm-related icaD gene were significantly higher in S. epidermidis strains isolated from mastitic milk samples [45].
Acute mastitis
Acute mastitis is characterized by breast redness, fever, pain and malaise [10]. Due to the intensity of these symptoms, acute mastitis is typically the sole type of mastitis that is accurately diagnosed despite representing a relatively small proportion of human mastitis cases. A metagenomic study of human milk samples by Jimenez et al. [26] analyzed the microbiome of 20 milk samples including 10 healthy, 5 acute and 5 subacute mastitic samples. Variation in the predominant bacterial genus was observed in milk samples obtained from healthy women (Pseudomonas, Bacteroides), however, Staphylococcus was the dominant genus in both acute and subacute mastitis samples. Women who presented with acute mastitis were found to have higher levels of S. aureus (approximately 106 cfu/mL) in their milk compared to those with subacute mastitis. The wide range of toxins produced by strains of S. aureus have previously been implicated in bovine mastitis and may also be responsible for the symptoms observed in acute mastitis in humans [56]. Comparatively, S. epidermidis was found to be the most abundant staphylococcal species in women with subacute mastitis. Interestingly, Patel et al. [20] recently reported that acute mastitis samples harbored significantly more Aeromonas, Klebsiella, Ralstonia, Proteus and Leptospira at genus level and significantly higher levels of Aeromonadaceae, Burkholderiaceae, Brucellaceae and Streptococcaceae at family level when acute mastitis, subacute mastitis and healthy milk samples were compared (Fig. 1c).
Subacute mastitis
The symptoms of subacute mastitis are distinctly more subtle than acute resulting in a lower rate of diagnosis, whether this is due to misdiagnosis or a lack of understanding by women experiencing these symptoms is not described. Where an official diagnosis has been established, the symptoms of subacute mastitis include a sharp, needling pain and a burning sensation in the breast [10].
As indicated previously, Jimenez et al. [26] proposed that S. epidermidis was the predominant species of Staphylococcus present in subacute mastitic milk samples (n = 5). An additional, and more extensive study of 20 women with subacute mastitis also found S. epidermidis to be the most dominant species (by 85%). Other species of Staphylococcus including S. hominis, S. pasteuri, S. warneri and S. haemolyticus, were also identified in subacute mastitic samples albeit at much lower levels than S. epidermidis [44]. At genus level, Staphylococcus was also found to be more enriched in subacute mastitis milk samples along with Erwinia, Bacillus, Pantoea, Cronobacter and Pseudomonas when compared to acute mastitic and healthy milk samples [20].
Collectively, the species of Staphylococcus found in subacute mastitic milk samples can be referred to as coagulase-negative staphylococci (CNS). Many species of CNS are healthy skin commensals; however, they can also be implicated in nosocomial infections, particularly S. epidermidis [63].
In addition to CNS, streptococci, more specifically viridans streptococci, may play a role in mastitis although the strains involved appear to be host-dependent. For example, Strep. uberis and Strep. dysgalactiae have been identified in bovine mastitis [50], yet they are not involved in human mastitis. On the other hand, Strep. mitis and Strep. salivarius prevail in human mastitis [57]. The combination of viridans streptococci and CNS have the potential to form thick biofilms leading to confinement of the lumen through which the milk passes. This pressure leads to the symptoms of subacute mastitis described previously [10].
Granulomatous mastitis
Idiopathic granulomatous mastitis (IGM) is a relatively rare, inflammatory disease which presents as a painful, tender lump or mass in the breast. The presence of a mass and the secondary symptoms of IGM, skin thickness, abscess formation and nipple retraction, often lead to a clinical misdiagnosis of breast malignancy [64, 65]. IGM is predominantly observed in women of reproductive age, approximately 2–6 years following pregnancy, however, it has also been reported in prepubescent girls, elderly women and men [66].
The causes of IGM may vary and several factors have been proposed that predispose to IGM including diabetes mellitus, the use of the oral contraceptive pill and undetected organisms amongst others [66, 67]. However, Taylor et al. [68] suggested that the presence of species of corynebacteria was linked to the development of IGM. A subsequent study by Dobinson et al. [65] demonstrated the successful isolation of several strains of corynebacteria from breast masses, namely C. kroppenstedii, C. tuberculostearicum and C. freneyi. Despite the strong suggestion that corynebacteria is a major causative agent of IGM, a successful treatment has not yet been established [67]. This is principally due to the fact that corynebacteria exist in lipid-filled vacuoles within the granuloma as opposed to the tissue itself thus treatment requires agents that are effective against corynebacteria as well as active in lipid environments. However, most antimicrobials are hydrophilic with weak distribution to lipid environments. A combination of these agents, e.g., clarithromycin or rifampin, with corticosteroids and/or other immunomodulatory modalities has shown some success in treating IGM [65].
Effects on milk quality
Lactational mastitis is a primary cause of decreased milk production and is also related to alterations in the cellular composition of milk. Changes in the metabolic activity of milk-producing cells along with diminished milk synthesis in the mammary gland is normally a direct result of inflammatory mediators [3, 69]. Edema of the interstitial tissues is caused by opening of the paracellular pathways during lactation as a result of protein leakage from blood and milk. Moreover, due to the opening of the paracellular pathways, levels of sodium and chloride increase, while at the same time the levels of potassium and lactose decrease [3]. Due to milk stasis, white granules may be observed in the milk which are formed from caseins hardened by salts, mainly consisting of calcium [3]. Fatty or fibrous-looking material, sometimes brown or green, is occasionally forced out from blocked ducts accompanied by alleviation of symptoms [3]. Furthermore, during mastitis, a change in the organoleptic properties can occur, in that the milk becomes salty. Generally, the saltiness is provisional and lasts approximately 1 week [70].
A recent study conducted by Say et al. [69] focused on the effects of mastitis on the macronutrient content of milk. A total of 30 lactating women were divided into two groups; one diagnosed with mastitis and one consisting of healthy women. Fat, carbohydrate and energy levels were significantly lower in the mastitic milk samples. The authors concluded that the observed differences may have emerged from reduced milk synthesis, compromised permeability of the blood–milk barrier and an increase in enzymatic or proteolytic activity associated with the inflammatory process [71, 72]. We speculate that the reduced levels of fat, carbohydrates and energy could have a negative effect on the health of the infant with the prerequisite that the mother still breastfeeds.
Perez et al. [73] concentrated on the impact of mastitis on the biogenic amine (BAs) profile in human milk. BAs are defined as low molecular weight nitrogenous organic compounds with distinct biological activities. In the study, two groups of women participated; one (n = 40) healthy group and the other (n = 30) diagnosed with mastitis. Putrescine, spermidine and spermine were the predominant BAs identified in both cases, however, the concentrations of BAs in mastitic milk were higher compared to healthy milk. BAs have been shown to contribute to gut maturation and the increased levels seen in mastitic milk may potentially negatively affect the development of the infants’ GI microbiota [74, 75].
Therapies
An overview of current therapies for mastitis treatment are presented in Table 2.
Antibiotics
Prior to 1948, the management of lactational mastitis consisted of binding, ice packs and discontinuance of nursing, in the hope that symptoms would not develop further. Penicillin was considered the most appropriate antibacterial available yet proved to be limited in treatment of the disease [81]. As stated already, S. aureus and S. epidermidis are found to be the main causative microorganisms of lactational mastitis with Strep. mitis and Strep. salivarius being the second and third most reported causative agents, respectively [27]. However, multidrug resistance to antibiotics and/or formation of biofilms is typical among clinical isolates of these two staphylococcal species. Accordingly, it is not surprising that 70–90% of the cases of staphylococcal mastitis in cattle are immune to antibiotherapy [82]. Resistance to methicillin and a high ability to form biofilms explains why mastitis tends to be a recurrent or chronic infection. Indeed, it has been reported that 25% of mothers who discontinue breast-feeding as a result of mastitis [3] have already received antibiotherapy (cloxacillin, clindamycin, amoxicillin-clavulanic acid and/or erythromycin) for 2–4 weeks with little success [11].
Penicillinase-resistant penicillins such as dicloxacillin or flucloxacillin are the most suitable antibiotic therapies for treatment of the disease (Table 2). First-generation cephalosporins are also approved as a first-line therapy. More specifically, cephalexin can be administered in cases of penicillin intolerance, while in cases of allergy to penicillin, clindamycin is preferred [4, 83]. Dicloxacillin has lesser hepatic inimical effects than flucloxacillin [76]. However, dicloxacillin can cause phlebitis when applied intravenously; so, it should be taken orally when symptoms persist [4]. A later study demonstrated that chloramphenicol, gentamicin, oflaxacin and ciprofloxacin were the most efficacious antibiotics against mastitis pathogens [43]. With regards to duration of antibiotic therapy, there is no consensus with recommendations varying between 7 and 14 days. As outlined by Reddy et al. [84], where symptoms endure, culturing of the milk and an assessment of the antibiotic resistance of the microbes should be performed due to the escalation of penicillin-resistant, methicillin-resistant (MRSA) and oxacillin-resistant S. aureus (ORSA); although it would be of greater benefit if milk cultures were performed as soon as possible to establish a proper diagnosis and to establish the most adequate treatment depending on the main bacterial agent(s) involved. This would greatly help to avoid misuse of antibiotics.
It is broadly acknowledged that antibiotics are the culprit for the disruption in human microbiota which can result in antibiotic-associated diarrhea, urogenital and oral infections [37]. Studies have demonstrated an increased vulnerability to infectious, allergic and inflammatory diseases because of the dysregulation of host immune homeostasis due to altered microbiota. The latter is attributed to the excessive use of antibiotics [85, 86]. The administration of antibiotics during pre- and post-delivery stages, has been proven to adversely affect breastfed infants as antibiotics can modify the maternal microbiota which is of critical importance to the human GI microbiota in early life [87]. Arvola et al. [88] demonstrated that infants with deferred colonization or low bifidobacterial counts may be at risk of further gastrointestinal or allergic conditions, while de Weerth et al. [89] found low Bifidobacterium and Lactobacillus counts in the stools of infants diagnosed with colic. Moreover, Kummeling et al. [90] reported that antibiotic exposure via breastfeeding in infants was associated with a higher risk of recurrent wheeze during the first 2 years of life. Consequently, there is a need to develop strategies to replace antibiotics and in this context, probiotics may provide a feasible solution.
Probiotics
The WHO/FAO describes probiotics as “live microorganisms that when administered in adequate amounts confer a health benefit on the host” [91, 92]. It is now known that the infant gut is colonized by bacteria from human milk [28, 38, 47, 48, 93]. Consequently, modulation of maternal gut microbiota during pregnancy and lactation could have a direct impact on infant health [94]. Indeed, recent studies illustrate that the mammary gland accommodates its own microbiota during late pregnancy and lactation [94]. More specifically, strains isolated from breast milk can be good candidates for use as probiotics [11, 77] as they fulfill several criteria including human origin, adaptation to mucosal substrates and a history of safe extended consumption by sensitive individuals such as infants [78].
An initial study by Jimenez et al. [11] investigated the potential of two lactobacilli strains as an alternative therapy for staphylococcal mastitis, namely L. salivarius CECT5713 and L. gasseri CECT5714 [Table 2]. Of a total of 20 women presenting with the condition, ten received the two Lactobacillus strains (10 log10 cfu of each) for a 4-week period and ten received the excipent only for the same period. On day 0, mean staphylococcal counts in both groups were similar, but by day 30, the mean staphylococcal count in the probiotic group was lower when compared to the control group (2.96 log10 cfu/mL versus 4.79 log10 cfu/mL, respectively). By day 14, clinical signs were no longer observed in the probiotic group although mastitis persisted in the control group. A subsequent study by Arroyo et al. [77] also investigated the potential of L. salivarius CECT5713 and the strain L. fermentum CECT5716 in a much larger group of subjects, 352 women presenting with infectious mastitis. Women received either L. salivarius CECT5713 (n = 127, 9 log10 cfu), or L. fermentum CECT5716 (n = 124, 9 log10 cfu) or antibiotic therapy (n = 101) for 3 weeks. By day 21, milk bacterial counts were lower in women receiving probiotics compared to those on antibiotic therapy. The authors state that women in the probiotic groups ‘improved more’ and had lower recurrence of mastitis than those receiving antibiotic therapy. The outcomes of both these studies are further discussed by Fernandez et al. [10].
A more recent study examined the potential of L. salivarius PS2 to hinder infectious mastitis in pregnant women who were previously diagnosed with mastitis [78]—108 women were divided into two groups. Those in the probiotic group ingested 9 log10 cfu/day of L. salivarius PS2 from approximately week 30 of pregnancy until delivery while those in the control group received a placebo. Following the end of the study, 41% of the participating women were diagnosed with mastitis; although the number of women from the probiotic group suffering from mastitis (25%) was significantly lower than the placebo group (57%). The bacterial counts of women with subacute mastitis from the placebo group were significantly higher when compared to the probiotic group (4.61 and 3.83 log10 cfu/mL, respectively). Comparable results were noted in the group of women with acute mastitis where those who belonged in the placebo group had higher bacterial mean counts (4.51–5.53 log10 cfu/mL) than those who belonged in the probiotic group (3.29–4.29 log10 cfu/mL). This study demonstrates that L. salivarius PS2 could be an effective alternative to forestall infectious mastitis.
Espinosa-Martos et al. [79] endeavored to correlate microbiological, biochemical or immunological markers in milk, blood or urine with the beneficial outcome observed during probiotic treatment of mastitis. A total of 31 women took part in the study. Among them, 23 women had clinical symptoms of mastitis while the remaining (n = 8) were healthy. Over a period of 21 days, both groups received three daily doses (109 cfu) of L. salivarius PS2. In the mastitic group, the probiotic intake resulted in a notable reduction of mean bacterial (1.1 log10 cfu/mL) counts in milk. Moreover, clinical symptoms were alleviated in the probiotic group after day 7 while the somatic cell count significantly declined after the intake of probiotics. The effect of the probiotic strain on the total bacterial counts in human milk is in agreement with previous studies [11, 77].
Bacteriocins
Bacteriocins are antimicrobial peptides produced by bacteria and exhibit potent activity against other bacteria including antibiotic-resistant strains [95]. They are generally stable, have low toxicity and can exhibit a narrow or broad spectrum of activity. Certain bacteriocins such as nisin have already gained acceptance as antimicrobials in the food industry where they provide protection against pathogen and food spoilage microorganisms. The lantibiotics describe a group of bacteriocins which undergo post-translational modifications and have exhibited a high potency to hinder various multidrug-resistant bacteria combined with a low propensity to generate resistance. The food-grade lantibiotic, nisin, is produced by certain strains of Lactococcus lactis, a common species in the breast milk of healthy women [10, 49]. Indeed, approximately 30% of isolates of this origin can produce nisin [96]. During the past 2 decades, there has been a revived interest in the use of this lantibiotic as a therapeutic agent in bovine mastitis [10]. Furthermore, another bacteriocin, i.e., lacticin 3147 has generated promising results in the treatment of bovine mastitis [97, 98]. Like nisin, lacticin 3147 is a lantibiotic with a broad spectrum of activity. Indeed, the potential of nisin in treating infectious mastitis in lactating mothers has already been demonstrated (Table 2). In a 2-week study, nisin was investigated as an alternative treatment for staphylococcal mastitis in women who had already received antibiotics for 2–4 weeks but which failed to ameliorate their condition [80]. More specifically, eight women diagnosed with staphylococcal mastitis were divided in two groups. The first group received a solution of nisin which was applied to the nipple and mammary areola, while the second group received a solution lacking nisin. On day 0, the staphylococcal counts were similar in the bacteriocin and placebo groups (5.0 ± 0.2 and 4.9 ± 0.2 log10 cfu/mL, respectively), while on day 14, the average counts in the nisin group (3.2 ± 0.4 log10 cfu/mL) were significantly lower compared with the placebo group (5.0 ± 0.2 log10 cfu/mL). At the end of the study, no clinical signs were observed in the bacteriocin group.
Conclusion and future prospects
While the number of studies addressing the microbiological load of human lactational mastitis is limited, those which have been completed provide an insight into the microbiological dysbiosis associated with the disease and hence shed light on potential new therapies. One study which employed metagenomic analysis of mastitic milk samples clearly identified a loss of bacterial diversity [26]. Unsurprisingly, Staphylococcus is the dominant genus associated with the disease where S. aureus is the main etiological agent in acute mastitis and S. epidermidis is associated with subacute mastitis. In addition, Corynebacterium species are now recognized as the causative agents of human granulomatous mastitis.
While the treatment of mastitis with antibiotics has, in the past, been met with mixed results, the looming threat of antibiotic resistance has significantly increased the need to identify alternative therapies. In addition, antibiotics are known to impart deleterious effects on the microbiota of human milk. In this regard, probiotics offer a viable alternative and the limited number of studies available, would seem to indicate that they can be effective against human mastitis both as prophylactics and therapeutics and in the latter case have generated similar or superior results to antibiotics in certain instances. Some of the probiotic strains tested to date have in fact been isolated from breast milk and it is now accepted that the mammary gland has its own microbiota in late pregnancy and during lactation. In this regard, it may be conceivable in the near future to generate ‘personalized’ probiotics for those at particular risk of mastitis, such as women with a known history of the disease.
The preliminary success of the bacteriocin nisin in the management of human mastitis, as well as the promising results with lacticin 3147 for the treatment of bovine mastitis may pave the way for other bacteriocins or bacteriocin-producing live strains in the treatment of human mastitis in the future. For such alternative therapies to be accepted as preventative agents or for treatment of this condition, randomized controlled trials in healthy and diseased lactating women are required to confirm efficacy, and furthermore to demonstrate that no negative effects of treatment are imparted on the quality of milk for nutrition of the nursing infant.
Undoubtedly, continued investigation into the microbiology of human mastitis is essential and will help in the identification and development of successful therapies. In this regard, there is an onus on researchers, health agencies and biotechnology companies to work in unison towards reducing the incidence of this devitalizing disease.
References
Martin CR, Ling PR, Blackburn GL (2016) Review of infant feeding: key features of breast milk and infant formula. Nutrients 8(5):279. https://doi.org/10.3390/nu8050279
Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J et al (2016) Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 387(10017):475–490. https://doi.org/10.1016/S0140-6736(15)01024-7
WHO (2000) Mastitis: causes and management. World Health Organization, Geneva, pp 1–45
Abou-Dakn M, Richardt A, Schaefer-Graf U, Wockel A (2010) Inflammatory breast diseases during lactation: milk stasis, puerperal mastitis, abscesses of the breast and malignant tumors–current and evidence-based strategies for diagnosis and therapy. Breast Care 5(1):33–37. https://doi.org/10.1159/000272223
Amir LH, Cullinane M, Garland SM, Tabrizi SN, Donath SM, Bennett CM et al (2011) The role of micro-organisms (Staphylococcus aureus and Candida albicans) in the pathogenesis of breast pain and infection in lactating women: study protocol. BMC Pregnancy Childbirth 11:54. https://doi.org/10.1186/1471-2393-11-54
Li R, Fein SB, Chen J, Grummer-Strawn LM (2008) Why mothers stop breastfeeding: mothers’ self-reported reasons for stopping during the first year. Pediatrics 122(Suppl 2):S69–S76. https://doi.org/10.1542/peds.2008-1315i
Osterman KL, Rahm VA (2000) Lactation mastitis: bacterial cultivation of breast milk, symptoms, treatment, and outcome. J Hum Lact 16(4):297–302. https://doi.org/10.1177/089033440001600405
Betzold CM (2007) An update on the recognition and management of lactational breast inflammation. J Midwifery Womens Health 52(6):595–605. https://doi.org/10.1016/j.jmwh.2007.08.002
Cullinane M, Amir LH, Donath SM, Garland SM, Tabrizi SN, Payne MS et al (2015) Determinants of mastitis in women in the CASTLE study: a cohort study. BMC Fam Pract 16(1):181. https://doi.org/10.1186/s12875-015-0396-5
Fernández L, Arroyo R, Espinosa I, Marín M, Jiménez E, Rodríguez JM (2014) Probiotics for human lactational mastitis. Benef Microb 5(2):169–183. https://doi.org/10.3920/bm2013.0036
Jiménez E, Fernández L, Maldonado A, Martín R, Olivares M, Xaus J et al (2008) Oral administration of Lactobacillus strains isolated from breast milk as an alternative for the treatment of infectious mastitis during lactation. Appl Environ Microbiol 74(15):4650–4655. https://doi.org/10.1128/aem.02599-07
Civardi E, Garofoli F, Tzialla C, Paolillo P, Bollani L, Stronati M (2013) Microorganisms in human milk: lights and shadows. J Matern Fetal Neonatal Med 26(Suppl 2):30–34. https://doi.org/10.3109/14767058.2013.829693
Foxman B, D’Arcy H, Gillespie B, Bobo JK, Schwartz K (2002) Lactation mastitis: occurrence and medical management among 946 breastfeeding women in the United States. Am J Epidemiol 155(2):103–114. https://doi.org/10.1093/aje/155.2.103
Kinlay JR, O’Connell DL, Kinlay S (2001) Risk factors for mastitis in breastfeeding women: results of a prospective cohort study. Aust N Z J Public Health 25(2):115–120. https://doi.org/10.1111/j.1753-6405.2001.tb01831.x
Scott JA, Robertson M, Fitzpatrick J, Knight C, Mulholland S (2008) Occurrence of lactational mastitis and medical management: a prospective cohort study in Glasgow. Int Breastfeed J 3(1):21. https://doi.org/10.1186/1746-4358-3-21
Mediano P, Fernández L, Rodríguez JM, Marín M (2014) Case-control study of risk factors for infectious mastitis in Spanish breastfeeding women. BMC Pregnancy Childbirth 14:195. https://doi.org/10.1186/1471-2393-14-195
Jonsson S, Pulkkinen MO (1994) Mastitis today: incidence, prevention and treatment. Ann Chir Gynaecol Suppl 208:84–87
Amir LH, Forster DA, Lumley J, McLachlan H (2007) A descriptive study of mastitis in Australian breastfeeding women: incidence and determinants. BMC Public Health 7(1):62. https://doi.org/10.1186/1471-2458-7-62
Spencer JP (2008) Management of mastitis in breastfeeding women. Am Fam Phys 78(6):727–731
Patel SH, Vaidya YH, Patel RJ, Pandit RJ, Joshi CG, Kunjadiya AP (2017) Culture independent assessment of human milk microboal community in lactational mastitis. Sci Rep 7:7804. https://doi.org/10.1038/s41598-017-08451-728
West PA, Hewitt JH, Murphy OM (1979) The influence of methods of collection and storage on the bacteriology of human milk. J Appl Microbiol 46(2):269–277. https://doi.org/10.1111/j.1365-2672.1979.tb00820.x
Heikkila MP, Saris PE (2003) Inhibition of Staphylococcus aureus by the commensal bacteria of human milk. J Appl Microbiol 95(3):471–478. https://doi.org/10.1046/j.1365-2672.2003.02002.x
Perez PF, Doré J, Leclerc M, Levenez F, Benyacoub J, Serrant P et al (2007) Bacterial imprinting of the neonatal immune system: lessons from maternal cells? Pediatrics 119(3):e724. https://doi.org/10.1542/peds.2006-1649
Collado MC, Delgado S, Maldonado A, Rodríguez JM (2009) Assessment of the bacterial diversity of breast milk of healthy women by quantitative real-time PCR. Lett Appl Microbiol 48(5):523–528. https://doi.org/10.1111/j.1472-765X.2009.02567.x
Hunt KM, Foster JA, Forney LJ, Schütte UME, Beck DL, Abdo Z et al (2011) Characterization of the diversity and temporal stability of bacterial communities in human milk. PLOS One 6(6):e21313. https://doi.org/10.1371/journal.pone.0021313
Jiménez E, de Andrés J, Manrique M, Pareja-Tobes P, Tobes R, Martínez-Blanch JF et al (2015) Metagenomic analysis of milk of healthy and mastitis-suffering women. J Jum Lact 31(3):406–415. https://doi.org/10.1177/0890334415585078
Mediano P, Fernández L, Jiménez E, Arroyo R, Espinosa-Martos I, Rodríguez JM et al (2017) Microbial diversity in milk of women with mastitis: potential role of coagulase-negative staphylococci, viridans group streptococci, and corynebacteria. J Jum Lact 33(2):309–318. https://doi.org/10.1177/0890334417692968
Murphy K, Curley D, O’Callaghan TF, O’Shea C-A, Dempsey EM, O’Toole PW et al (2017) The Composition of human milk and infant faecal microbiota over the first three months of life: a pilot study. Sci Rep 7:40597. https://doi.org/10.1038/srep40597
Rescigno M, Urbano M, Valzasina B, Francolini M, Rotta G, Bonasio R et al (2001) Dendritic cells express tight junction proteins and penetrate gut epithelial monolayers to sample bacteria. Nat Immunol 2(4):361–367. https://doi.org/10.1038/86373
Macpherson AJ, Uhr T (2004) Induction of protective IgA by intestinal dendritic cells carrying commensal bacteria. Science 303(5664):1662–1665. https://doi.org/10.1126/science.1091334
Kort R, Caspers M, van de Graaf A, van Egmond W, Keijser B, Roeselers G (2014) Shaping the oral microbiota through intimate kissing. Microbiome 2(1):41. https://doi.org/10.1186/2049-2618-2-41
Ross AA, Doxey AC, Neufeld JD (2017) The skin microbiome of cohabiting couples. mSystems 2 (4)
Wyatt RG, Mata LJ (1969) Bacteria in colostrum and milk of Guatemalan Indian women. J Trop Pediatr 15(4):159–162
Eidelman AI, Szilagyi G (1979) Patterns of bacterial colonization of human milk. Obstet Gynecol 53:550–552
Serafini ÁB, André MCDPB., Rodrigues MAV, Kipnis A, Carvalho CO, Campos MRH et al (2003) Qualidade microbiológica de leite humano obtido em banco de leite. Rev Saúde Pública 37:775–779
Martín R, Jiménez E, Heilig H, Fernández L, Marín ML, Zoetendal EG et al (2009) Isolation of bifidobacteria from breast milk and assessment of the bifidobacterial population by PCR-denaturing gradient gel electrophoresis and quantitative real-time PCR. Appl Environ Microbiol 75:965–969. https://doi.org/10.1128/AEM.02063-08
Martín V, Maldonado-Barragán A, Moles L, Rodriguez-Banõs M, del Campo R, Fernández L et al (2012) Sharing of bacterial strains between breast milk and infant feces. J Hum Lact 28:36–44. https://doi.org/10.1177/0890334411424729
Jost T, Lacroix C, Braegger CP, Rochat F, Chassard C (2014) Vertical mother-neonate transfer of maternal gut bacteria via breastfeeding. Environ Microbiol 16(9):2891–2904. https://doi.org/10.1111/1462-2920.12238
Rodríguez JM, Fernández L (2017) Infectious mastitis during lactation: a mammary dysbiosis model in McGuire M. In: McGuire M, Bode L (eds) Prebiotics and probiotics in human milk, 2nd edn. Academic Press, San Diego, pp 401–428
Salter SJ, Cox MJ, Turek EM, Calus ST, Cookson WO, Moffatt MF et al (2014) Reagent and laboratory contamination can critically impact sequence-based microbiome analyses. BMC Biol 12:87. https://doi.org/10.1186/s12915-014-0087-z
Glassing A, Dowd SE, Galandiuk S, Davis B, Chiodini RJ (2016) Inherent bacterial DNA contamination of extraction and sequencing reagents may affect interpretation of microbiota in low bacterial biomass samples. Gut Pathog 8:24. https://doi.org/10.1186/s13099-016-0103-7
Patel SH, Vaidya YH, Joshi CG, Kunjadia AP (2016) Culture-dependent assessment of bacterial diversity from human milk with lactational mastitis. Comp Clin Path 25:437–443. https://doi.org/10.1007/s00580-015-2205-x
Marín M, Arroyo R, Espinosa-Martos I, Fernández L, Rodríguez JM (2017) Identification of emerging human mastitis pathogens by MALDI-TOF and assessment of their antibiotic resistance patterns. Front Microbiol 8:1258. https://doi.org/10.3389/fmicb.2017.01258
Delgado S, Arroyo R, Martín R, Rodríguez JM (2008) PCR-DGGE assessment of the bacterial diversity of breast milk in women with lactational infectious mastitis. BMC Infect Dis 8:51. https://doi.org/10.1186/1471-2334-8-51
Delgado S, Arroyo R, Jiménez E, Marín ML, del Campo R, Fernández L et al (2009) Staphylococcus epidermidis strains isolated from breast milk of women suffering infectious mastitis: potential virulence traits and resistance to antibiotics. BMC Microbiol 9::82. https://doi.org/10.1186/1471-2180-9-82
Alexandraki V, Kazou M, Angelopoulou A, Arena MP, Capozzi V, Russo P et al (2016) The microbiota of non-cow milk and products. In: Tsakalidou E, Papadimitriou K (eds) Non-bovine Milk and Milk Products, 1st edn. Academic Press, San Diego, pp 117–159
Martín R, Langa S, Reviriego C, Jimínez E, Marín ML, Xaus J et al (2003). Human milk is a source of lactic acid bacteria for the infant gut. J Pediatr 143(6):754–758. https://doi.org/10.1016/j.jpeds.2003.09.028
Albesharat R, Ehrmann MA, Korakli M, Yazaji S, Vogel RF (2011) Phenotypic and genotypic analyses of lactic acid bacteria in local fermented food, breast milk and faeces of mothers and their babies. Syst Appl Microbiol 34:148–155. https://doi.org/10.1016/j.syapm.2010.12.001
Martín R, Heilig HGHJ., Zoetendal EG, Jiménez E, Fernández L, Smidt H et al (2007) Cultivation-independent assessment of the bacterial diversity of breast milk among healthy women. Res Microbiol 158:31–37. https://doi.org/10.1016/j.resmic.2006.11.004
Riffon R, Sayasith K, Khalil H, Dubreuil P, Drolet M, Lagace J (2001) Development of a rapid and sensitive test for identification of major pathogens in bovine mastitis by PCR. J Clin Microbiol 39:2584–2589. https://doi.org/10.1128/jcm.39.7.2584-2589.2001
Gavin A, Ostovar K (1977) Microbiological characterization of human milk. J Food Prot 40:614–616. https://doi.org/10.4315/0362-028X-40.9.614
Martín R, Jiménez E, Olivares M, Marin ML, Fernández L, Xaus J et al (2006) Lactobacillus salivarius CECT 5713, a potential probiotic strain isolated from infant feces and breast milk of a mother–child pair. Int J Food Microbiol 112:35–43. https://doi.org/10.1016/j.ijfoodmicro.2006.06.011
Gonzalez R, Mandomando I, Fumado V, Sacoor C, Macete E, Alonso PL et al (2013) Breast milk and gut microbiota in African mothers and infants from an area of high HIV prevalence. PloS One 8:e80299. https://doi.org/10.1371/journal.pone.0080299
Thompson N, Pickler RH, Munro C, Shotwell J (1997). Contamination in expressed breast milk following breast cleansing. J Hum Lact 13:127–130. https://doi.org/10.1177/089033449701300213
Cabrera-Rubio R, Mira-Pascual L, Mira À, Collado MC (2016) Impact of mode of delivery on the milk microbiota composition of healthy women. J Dev Orig Health Dis 7:54–60. https://doi.org/10.1017/S2040174415001397
Delgado S, Garcia P, Fernández L, Jiménez E, Rodriguez-Banõs M, del Campo R et al (2011) Characterization of Staphylococcus aureus strains involved in human and bovine mastitis. FEMS Immunol Med Microbiol 62:225–235. https://doi.org/10.1111/j.1574-695X.2011.00806.x
Delgado S, Collado C, Fernández L, Rodríguez JM (2009) Bacterial analysis of breast milk: a tool to differentiate Raynaud’s phenomenon from infectious mastitis during lactation. Curr Microbiol 59:59–64. https://doi.org/10.1007/s00284-009-9393-z
Martín R, Langa S, Reviriego C, Jiménez E, Marín ML, Olivares M et al (2004) The commensal microflora of human milk: new perspectives for food bacteriotherapy and probiotics. Trends Food Sci Technol 15 (3):121–127. https://doi.org/10.1016/j.tifs.2003.09.010
Jost T, Lacroix C, Braegger C, Chassard C (2013) Assessment of bacterial diversity in breast milk using culture-dependent and culture-independent approaches. Br J Nutr 110(7):1253–1262. https://doi.org/10.1017/s0007114513000597
Ward TL, Hosid S, Ioshikhes I, Altosaar I (2013) Human milk metagenome: a functional capacity analysis. BMC Microbiol 13:116. https://doi.org/10.1186/1471-2180-13-116
Gueimonde M, Laitinen K, Salminen S, Isolauri E (2007) Breast milk: a source of bifidobacteria for infant gut development and maturation? Neonatology 92:64–66. https://doi.org/10.1159/000100088
Grice EA, Kong HH, Conlan S, Deming CB, Davis J, Young AC et al (2009) Topographical and temporal diversity of the human skin microbiome. Science 324(5931):1190–1192. https://doi.org/10.1126/science.1171700
Otto M (2014) Staphylococcus epidermidis pathogenesis. Methods Mol Biol 1106:17–31. https://doi.org/10.1007/978-1-62703-736-5_2
Sabel MS (2009) Infectious and inflammatory diseases of the breast in essentials of breast surgery. Mosby, Philadelphia, pp 83–90
Dobinson HC, Anderson TP, Chambers ST, Doogue MP, Seaward L, Werno AM (2015) Antimicrobial treatment options for granulomatous mastitis caused by Corynebacterium species. J Clin Microbiol 53:2895–2899. https://doi.org/10.1128/jcm.00760-15
Korkut E, Akcay MN, Karadeniz E, Subasi ID, Gursan N (2015) Granulomatous mastitis: a ten-year experience at a university hospital. Eurasian J Med 47(3):165–173. https://doi.org/10.5152/eurasianjmed.2015.118
Kiyak G, Dumlu EG, Kilinc I, Tokaç M, Akbaba S, Gurer A et al (2014) Management of idiopathic granulomatous mastitis: dilemmas in diagnosis and treatment. BMC Surg 14(1):66. https://doi.org/10.1186/1471-2482-14-66
Taylor GB, Paviour SD, Musaad S, Jones WO, Holland DJ (2003) A clinicopathological review of 34 cases of inflammatory breast disease showing an association between corynebacteria infection and granulomatous mastitis. Pathology 35:109–119
Say B, Dizdar EA, Degirmencioglu H, Uras N, Sari FN, Oguz S et al (2016) The effect of lactational mastitis on the macronutrient content of breast milk. Early Hum Dev 98:7–9. https://doi.org/10.1016/j.earlhumdev.2016.03.009
Prentice A, Prentice AM, Lamb WH (1985) Mastitis in rural Gambian mothers and the protection of the breast by milk antimicrobial factors. Trans R Soc Trop Med Hyg 79:90–95
Nommsen LA, Lovelady CA, Heinig MJ, Lonnerdal B, Dewey KG (1991) Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 months of lactation: the DARLING study. Am J Clin Nutr 53:457–465
Le Roux Y, Laurent F, Moussaoui F (2003) Polymorphonuclear proteolytic activity and milk composition change. Vet Res 34:629–645. https://doi.org/10.1051/vetres:2003021
Perez M, Ladero V, Redruello B, Del Rio B, Fernández L, Rodríguez JM et al (2016) Mastitis modifies the biogenic amines profile in human milk, with significant changes in the presence of histamine, putrescine and spermine. PLoS One 11:e0162426. https://doi.org/10.1371/journal.pone.0162426
Thomas T, Thomas TJ (2001) Polyamines in cell growth and cell death: molecular mechanisms and therapeutic applications. Cell Molec Life Sci 58(2):244–258. https://doi.org/10.1007/pl00000852
Chanphai P, Thomas TJ, Tajmir-Riahi HA (2016) Conjugation of biogenic and synthetic polyamines with serum proteins: a comprehensive review. Int J Biol Macromo. 92:515–522. https://doi.org/10.1016/j.ijbiomac.2016.07.049
Jahanfar S, Ng CJ, Teng CL (2013) Antibiotics for mastitis in breastfeeding women. Cochrane Database Syst Rev 2:CD005458. https://doi.org/10.1002/14651858.CD005458.pub3
Arroyo R, Martín V, Maldonado A, Jiménez E, Fernández L, Rodríguez JM (2010) Treatment of infectious mastitis during lactation: antibiotics versus oral administration of lactobacilli isolated from breast milk. Clin Infect Dis 50:1551–1558. https://doi.org/10.1086/652763
Fernández L, Cardenas N, Arroyo R, Manzano S, Jiménez E, Martín V et al (2016) Prevention of infectious mastitis by oral administration of Lactobacillus salivarius PS2 during late pregnancy. Clin Infect Dis 62:568–573. https://doi.org/10.1093/cid/civ974
Espinosa-Martos I, Jiménez E, de Andrés J, Rodríguez-Alcalá LM, Tavárez S, Manzano S et al (2016) Milk and blood biomarkers associated to the clinical efficacy of a probiotic for the treatment of infectious mastitis. Benef Microbes 7(3):305–318. https://doi.org/10.3920/bm2015.0134
Fernández L, Delgado S, Herrero H, Maldonado A, Rodríguez JM (2008) The bacteriocin nisin, an effective agent for the treatment of staphylococcal mastitis during lactation. J Hum Lact 24:311–316. https://doi.org/10.1177/0890334408317435
Devereux WP (1969) Acute puerperal mastitis. Am J Obstet Gynecol 108:78–81. https://doi.org/10.1016/0002-9378(70)90208-5
Wall RJ, Powell AM, Paape MJ, Kerr DE, Bannerman DD, Pursel VG et al (2005) Genetically enhanced cows resist intramammary Staphylococcus aureus infection. Nat Biotechnol 23:445–451. https://doi.org/10.1038/nbt1078
Schoenfeld EM, McKay MP (2010) Mastitis and methicillin-resistant Staphylococcus aureus (MRSA): the calm before the storm? J Emerg Med 38:e31–34. https://doi.org/10.1016/j.jemermed.2008.11.021
Reddy P, Qi C, Zembower T, Noskin GA, Bolon M (2007) Postpartum mastitis and community-acquired methicillin-resistant Staphylococcus aureus. Emerg Infect Dis 13::298–301. https://doi.org/10.3201/eid1302.060989
Joffe TH, Simpson NA (2009) Cesarean section and risk of asthma. The role of intrapartum antibiotics: a missing piece? J Pediatr 154:154. https://doi.org/10.1016/j.jpeds.2008.08.039
Willing BP, Vacharaksa A, Croxen M, Thanachayanont T, Finlay BB (2011) Altering host resistance to infections through microbial transplantation. PLOS One 6:e26988. https://doi.org/10.1371/journal.pone.0026988
Mueller NT, Bakacs E, Combellick J, Grigoryan Z, Dominguez-Bello MG (2015) The infant microbiome development: mom matters. Trends Mol Med 21:109–117. https://doi.org/10.1016/j.molmed.2014.12.002
Arvola T, Ruuska T, Keränen J, Hyöty H, Salminen S, Isolauri E (2006) Rectal bleeding in infancy: clinical, allergological, and microbiological examination. Pediatrics 117:e760. https://doi.org/10.1542/peds.2005-1069
de Weerth C, Fuentes S, Puylaert P, de Vos WM (2013) Intestinal microbiota of infants with colic: development and specific signatures. Pediatrics 131:e550–e558. https://doi.org/10.1542/peds.2012-1449
Kummeling I, Stelma FF, Dagnelie PC, Snijders BEP, Penders J, Huber M et al (2007) Early life exposure to antibiotics and the subsequent development of eczema, wheeze and allergic sensitization in the first 2 years of life: the KOALA birth cohort study. Pediatrics 119:e225. https://doi.org/10.1542/peds.2006-0896
FAO/WHO (2001); Report of joint FAO/WHO expert consultation on the health and nutritional properties of powder milk with live lactic acid bacteria. http://www.fao.org/3/a-a0512e.pdf
Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B et al (2014) Expert consensus document: The international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol 11:506–514. https://doi.org/10.1038/nrgastro.2014.66
Pacheco AR, Barile D, Underwood MA, Mills DA (2015) The impact of the milk glycobiome on the neonate gut microbiota. Annu Rev Anim Biosci 3:419–445. https://doi.org/10.1146/annurev-animal-022114-111112
Fernández L, Langa S, Martín V, Maldonado A, Jiménez E, Martín R et al (2013) The human milk microbiota: origin and potential roles in health and disease. Pharmacol Res 69:1–10. https://doi.org/10.1016/j.phrs.2012.09.001
Cotter PD, Hill C, Ross RP (2005) Bacteriocins: developing innate immunity for food. Nat Rev Microbiol 3:777–788. https://doi.org/10.1038/nrmicro1273
Beasley SS, Saris PE (2004) Nisin-producing Lactococcus lactis strains isolated from human milk. Appl Environ Microbiol 70:5051–5053. https://doi.org/10.1128/aem.70.8.5051-5053.2004
Crispie F, Twomey D, Flynn J, Hill C, Ross P, Meaney W (2005) The lantibiotic lacticin 3147 produced in a milk-based medium improves the efficacy of a bismuth-based teat seal in cattle deliberately infected with Staphylococcus aureus. J Dairy Res 72:159–167. https://doi.org/10.1017/S0022029905000816
Klostermann K, Crispie F, Flynn J, Meaney WJ, Ross PR, Hill C (2010) Efficacy of a teat dip containing the bacteriocin lacticin 3147 to eliminate Gram-positive pathogens associated with bovine mastitis. J Dairy Res 77:231–238. https://doi.org/10.1017/s0022029909990239
Acknowledgements
This work was funded by APC Microbiome Ireland, a Centre for Science and Technology (CSET) funded by the Science Foundation Ireland (SFI), grant number SFI/12/RC/2273, Toddlerfood (14/F/821) and Infamilk (15/F/721) projects funded through the Irish Department of Agriculture, Food and the Marine (DAFM).
Author information
Authors and Affiliations
Contributions
AA drafted the manuscript. DF, AR, CS, CH and PR revised and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Rights and permissions
About this article

Cite this article
Angelopoulou, A., Field, D., Ryan, C.A. et al. The microbiology and treatment of human mastitis. Med Microbiol Immunol 207, 83–94 (2018). https://doi.org/10.1007/s00430-017-0532-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00430-017-0532-z