
Abstract
Cardiac allograft vasculopathy is regarded as a progressive and diffuse intimal hyperplastic lesion of arteries and veins that leads to insidious vessel narrowing and to allograft ischemic disease, such as acute myocardial infarction or sudden cardiac death. The coronary lesions in transplanted hearts are considered as a particular type of arteriosclerosis with many similarities but also significant differences compared to native coronary atherosclerosis. It is particularly difficult for pathologists to systematically classify the lesions and to elucidate their origins, since over time, the allograft immune responses cause vascular pathology characterized by not only the onset of de novo fibrocellular lesions but also remodeling of already-existing native atherosclerotic lesions in the donor heart. Intraplaque hemorrhages, which result from newly formed leaky microvessels, may cause rapid increase of stenosis and generate a substrate for plaque destabilization. Comparing cardiac allograft vasculopathy from explanted hearts at autopsy with native coronary atherosclerosis from hearts removed at transplantation has revealed that ongoing intraplaque hemorrhages are also an important feature of cardiac allograft vasculopathy and may be important factors in the rapid progression of cardiac allograft vasculopathy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many synonyms, ranging from chronic rejection to transplant atherosclerosis, have been used over the years to identify the progressively stenosing vascular process in transplanted organs that is now most frequently designated as cardiac allograft vasculopathy (CAV; see Table 1) [1–11].
The International Society for Heart Lung Transplantation (ISHLT) has recently published a working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010, recognizing the necessity of clarifying the abundant confusion in terminology and interpretations of various clinical and imaging technologies. This has resulted in a standard language based on best scientific evidence and clinical practice [12–15]. CAV can be defined as a rapidly progressive form of atherosclerosis characterized by an accelerated progressive and diffuse intimal hyperplastic lesions of the vascular tree that leads to insidious vessel narrowing and eventually to allograft ischemia. Clinical presentation is heterogeneous, varying from silent myocardial ischemia to congestive heart failure and sudden death [16, 17]. There are many aspects that are peculiar to CAV compared to classical native atherosclerotic lesions (ATS). CAV is considered a diffuse concentric process, affecting homogeneously the entire coronary vascular tree, with a rapid onset even within months, a mainly immune-mediated process and at histological evaluation characterized by intimal hyperplasia composed by SMC, intact internal elastic lamina, and various mononuclear cell infiltrations and preserved tunica media (see Table 2) [18, 19]. However, this represents a simplistic approach to the CAV lesion evaluation, since the assessment of the vascular tree of re-transplanted hearts or autopsy post-transplanted heart has revealed a series of highly heterogeneous intimal lesions in terms of component makeup, ranging from early diffuse intimal thickening to complicated atheromas [9, 20–22]. Even in these CAV hearts, we can identify non-culprit and culprit lesions (i.e., the lesions that are responsible for the onset of clinical symptoms). Another important feature which can be noticed not only in the heart but also in other solid organ transplants as kidney [23, 24] is the involvement of intramyocardial arteries and arterioles, the so-called microvasculopathy [25], as well as the venous and post-capillary vascular bed in the process of CAV [26]. The latter can be characterized by venulitis with mononuclear inflammatory cells infiltration of the intimal layer or transmural wall or by intimal hyperplastic cell proliferation with cross-sectional luminal stenosis. This is generally considered trivial in terms of hemodynamic graft performance although systematic studies on this subject are lacking. In the definition of terms, “accelerated” atherosclerosis is usually associated to the term CAV, since the rapidly progressive growth of lesions determines many biological and clinical manifestations of CAV. We all know that ATS is a long-life remodeling process affecting the wall of large- and medium-sized arteries, which starts in childhood and manifests in the advanced adult age, and with males being more precociously involved (about 10/15 years earlier than females). On the other hand, CAV develops much more rapidly, affects males and females in a similar degree and proportion, and not only adults but also pediatric patients become symptomatic early after transplantation even within the first year. This accounts for more than 30 % of involvement at 3 years post-transplant (Table 2). The attention has been focused on risk factors both for ATS and CAV in a clear attempt to adopt preventive strategies to reduce morbidity and mortality related to these diseases. However, ATS still represents the main cause of cardiovascular death in the general population, and CAV still represents the second most frequent cause of death among transplanted patients in the long-term follow-up [27]. This is true also when we disaggregate the mortality data considering different era in the follow-up [13].
The heterogeneity of pathological features
The heterogeneity in clinical symptoms from silent ischemia to severe congestive heart failure and even sudden death is paralleled by heterogeneity in the pathological features of CAV lesions. This varies from what is considered the classical CAV fibrocellular lesion characterized by concentric diffuse intimal thickening of epicardial and intramyocardial coronary arteries with preserved tunica media to classical ATS-like lesions characterized by atheromas with focal, eccentric plaques, and a lipid pool (fibrolipid plaques). Inflammatory patterns may range from transmural vasculitis involving epicardial and intramyocardial vessels to a more selective superficial involvement with endothelialitis (Fig. 1) [18–22]. Fibrocellular lesions are present in about two-third of CAV cases in the first years after transplantation, but their incidence drops markedly on the long term when fibrolipid plaques are more frequently detected (Figs. 2, 3, and 4) frequently associated with atrophy or attenuation of the media in a similar pattern as in native ATS [16]. Challenging questions are related to the presence of these fibrolipid plaques in CAV: Are the fibrolipid plaques in CAV pre-existent plaques in the coronary arteries of the donor, or do they arise the novo, superimposed on the classical fibrocellular CAV lesions? And even more: is the rich SMC donor intimal thickening, which is insignificant from a clinical point of view, a predisposing substrate (a “fertile soil”) for CAV development? Many of these questions remain to be elucidated, which could explain why CAV still is the Achilles’ heel of heart transplantation outcomes [16].

Histopathologic characteristic of CAV and ATS. Similarities and differences in phenotypes and biological mechanisms of cardiac allograft vasculopathy (CAV) and atherosclerosis (ATS). This figure reports only the main characteristics of both types of lesions

Coronary allograft vasculopathy: pathological features. View of concentric diffuse intimal thickening of epicardial coronary artery tree in a gross pathology; b concentric lesion, with focal attenuation of tunica media; and c eccentric fibrocellular lesion; d, e concentric diffuse intimal thickening of the small intramyocardial arteries, with focal attenuation of tunica media in (d)

Classic atherosclerosis lesion. a Azan-mallory histo-staining of a classic ATS lesion, showing focal eccentric plaque with thin fibrous cap covering a lipid pool, with atrophy of tunica media; b detailed vision of black inset in (a), showing numerous cholesterol clefts in the lipid pool, with atrophy of tunica media

Coronary allograft vasculopathy: pathological features a epicardial artery showing vasculitis. Power view in the black inset; b H&E showing both the artery (A) and vein (V) affected by vasculitis; c, d endothelialitis of small coronary arteries. All sections H&E stained
Destabilizing factors in plaque tissue of CAV and ATS
In recent years, the attention has been directed to evaluate the microenvironment in atherosclerotic plaque in order to specifically address the issue of inflammation and neoangiogenesis and its role in ATS development and progression and to identify potential substrate of plaque instability [28–31]. Kockx et al. and Virmani et al. showed that intraplaque hemorrhages (IPH) can be seen as a possible plaque destabilizing factor, since hemorrhages were more frequently identified in the vulnerable thin-cap fibroatheromas and in advanced lesions [28, 32, 33]. In addition, IPH occurred in areas of extensive neovascularization, where dilated, very-thin-walled, and leaky microvessels are located, as can be visualized by diffuse perivascular staining for von Willebrand factor [28, 34].
We recently had the opportunity to evaluate the coronary plaques of cardiac transplanted patients who died because of CAV and to compare them with the coronary plaques in their native hearts which were removed at the time of transplantation (i.e., in the same patients) [34]. The results of our study are reported below.
Inflammatory patterns in CAV and ATS
Immunohistochemical studies have characterized the inflammatory profile of lesions and showed that CAV fibrocellular lesions display a pattern of inflammation similar to the inflamed myocardium during an acute cellular rejection. In this type of inflammatory response, CD3+ T cells dominate the infiltrate, accounting for about 70–75 % of the inflammatory cells, CD20+ B cells for about 10 %, and CD68+ macrophages for about 15 % [35]. By contrast, macrophages are the dominant cell type in ATS plaques accounting for more than 55 % of the plaque cells, CD3+ cells as the second important cell type (40–45 %), but almost no B-lymphocytes [36]. Our attempts to characterize the inflammatory cells subtypes in CAV showed similarly that fibrocellular plaques of CAV presented overall low numbers of macrophages and more lymphocytes compared to ATS, but that fibrolipid plaques in CAV and in ATS had the same inflammatory patterns (Table 2).
Plaque microvessels and intraplaque hemorrhages in CAV
Overall, we investigated 24 hearts of 12 patients, evaluating 70 plaques of which 35 lesions were taken from native hearts and 35 from the transplanted heart at autopsy [34]. Microvessels, which are an important feature of the advanced fibro lipid plaques in ATS, were detected in our study in 74.3 % of the 35 CAV lesions and showed perivascular leakage of von Willebrand factor as sign of endothelial damage. In these CAV lesions, presence of microvessels was strongly associated with IPH and plaque inflammatory cells.
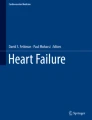
These intraplaque hemorrhages were even more frequently encountered in CAV lesions than in ATS, (60 % of plaques versus 20 % of plaques respectively, p = 0.0016). Not only fresh hemorrhages but also older (lytic or organized) hemorrhages could be detected frequently in the same plaque (40 % of plaques were positive both for fresh and old hemorrhages) (Fig. 5). This implies that, similar to the situation in advanced native plaques, plaque hemorrhage appears to be an ongoing phenomenon and hence may contribute significantly to lesion progression and/or degree of lumen stenosis. Interestingly, these hemorrhages were not only found in fibrolipid plaques, as one would expect, but also in the “typical” fibrocellular lesions of CAV (Fig. 3) [34].

Intraplaque hemohrrage (IPH) in CAV and ATS. a The graph reports the distribution of incidence of IPH in CAV and ATS plaques and divided by different types of lesions as: early, fibrocellular, and fibrolipidic lesions. Note as in both CAV and ATS early lesions, no IPH was identified. CAV shows more incidence of IPH in both fibrocellular and fibrolipidic lesion compared to ATS (p < 0.01); b,c,d immunohistology (Gycophorin A, panels b and c) and iron stain (panel d) of plaque hemorrhage
The remodeling process of CAV is time dependent, and one might expect a dramatic reduction in the numbers of fibrocellular plaques over the years concomitant with their transition into fibroatheromas, which is due to the exposure to atherosclerotic risk factors such as hypercholesterolemia or immunologic risk factors. However, in the long term, we observed that about half of the plaques still were fibrocellular in nature. Moreover, one would expect that in post-transplant patients, the plaques would have been more inflamed, but instead, we detected lack of inflammation in some of CAV plaques several years after transplantation. These differences are probably also risk factors related (Table 2).
Adventitia
Since the adventitia of arteries is supposed to be actively involved in the process of tissue remodeling of atherosclerosis affected arteries, we have recently further explored patterns of inflammation, microvessels, and leakage in the adventitia and perivascular tissues of CAV versus ATS. Lesions containing plaque hemorrhages had more adventitial inflammation in CAV than in ATS, but the abundant infiltrations diminished on the long term (post-transplant intervals of several years).
CAV lesions showed more adventitial inflammation and particularly more fibrosis compared to ATS. Inflammation followed a pattern of diffusely distributed inflammatory cells which was present in nearly all lesions early after transplantation, but in the late observations (years after transplantation), some plaques were completely devoid of adventitial inflammation (Table 2).
Distinct perivascular fibrosis appears to be an early complication of CAV-affected arteries, which may contribute importantly to remodeling phenomena, particularly in terms of shrinkage. The presence of adventitial fibrosis and microvessels seemed not to be influenced by time [37, 38].
Inflammation in ATS and CAV and in vivo imaging
ATS is recognized as an inflammatory disease of the arteries; although, the inflammatory component in the plaques is usually present multifocally instead of diffusely [39–41]. Inflammation is recognized to be a destabilizing factor in the natural history of the plaque and eventually may lead to plaque disruption complicated by thrombosis [41]. CAV also has a strong inflammatory component but usually in relation to the concomitant presence of acute cellular rejection in the myocardium. The role of ACR in CAV development and progression is still controversial. Some authors reported a strong association with CAV progression and worse outcomes [17], while others had been unable to obtain similar results [42]. High rejection score was an independent predictor for CAV onset suggesting an immune basis for CAV onset and nonimmune modulation for progression [17]. Moreover, so-called endothelialitis has now been recognized as a common feature of the microvascular inflammatory burden associated to antibody-mediated rejection (AMR). Symptomatic antibody-mediated rejection has been recognized as a risk factor for development of CAV and worse outcome [43–45]. Recently, Wu et al. demonstrated that also asymptomatic AMR is associated with development of CAV at 5 years follow-up [46]. Evidence of strong correlation between complement activation (C4d and C3d) on EMBs and development of CAV exists [47, 48], supporting the concept of donor specific antibodies damage to endothelium and activation of m-TOR proliferative pathway [49–51].
The production of antibodies to donor HLA antigens before or after cardiac transplantation is a major risk factor for the development of AMR. The pathological effect of DSA binding to the transplanted organ is likely to involve signaling pathways. Engagement of HLA class I molecules by anti-HLA antibodies increased the activation of ERK1-2, S6K, and S6RP through target of rapamycin (mTOR) complexes 1 and 2 (mTORC1 and mTORC2) [52]. Recent multicenter trials have evaluated the outcomes of immunosuppressive therapies with the mTOR-derived antiproliferative signal inhibitors such as everolimus [53]. These studies were performed using in vivo imaging techniques evaluation of CAV by means of virtual histology (VH). These techniques have previously been used also for identification of ATS plaque characteristics in an attempt to identify plaques at risk of complications such as plaque rupture. They have been used also in CAV assessment, among patients treated with everolimus and low-dose calcineurin inhibitor (CNI) compared to standard CNI therapy [54]. Among these techniques, VH represents a novel technological tool that utilizes backscatter radiofrequency data obtained during IVUS (intra-vascular ultrasound) pullback to construct a tissue map providing a qualitative assessment of plaque and intimal wall composition. It has been demonstrated that VH possesses 94–97 % ex vivo and 87–97 % in vivo accuracy for characterization of four basic tissue components (fibrous, fibrofatty, calcified, and necrotic core components) among patients with ischemic heart disease [55]. Moreover, another technique—namely, contrast ultrasound imaging and dynamic contrast-enhanced MR (DCE-MR)—was applied by Dong et al. group to study also the vasa vasorum in the adventitia of the plaques [56]. DCR-MR allows the assessment of neovascular architecture and functional characteristics, such as fractional plasma volume and permeability, also providing high spatial resolution that allows localization of the measurements, including the adventitial boundary and the source of the vasa vasorum [56].
Thanks to application of virtual histology in CAV assessment of patients treated with everolimus and low-dose calcineurin inhibitor (CNI), the investigators were able to identify four morphologic components of plaques—namely, fibrous tissue, fibro fatty tissue, calcifications, and necrotic cores, in which the last two have been considered as surrogates of inflammation into the plaque. Moreover, the results showed that the progression of CAV in the treated group was characterized by a statistically significant increase in the calcified and necrotic components. These gave new insights in the detailed morphology of CAV lesions; although, we question the interpretation given by the authors to consider calcified and necrotic components as surrogate markers for inflammation in plaques [57–59]. Nowadays, imaging techniques are still unable to detect reliably sites of inflammation in plaques (Table 2) [60].
Conclusions
Cardiac allograft vasculopathy can be considered a particular type of atherosclerosis with many similarities but also significant differences compared to ATS, which makes it difficult for pathologists to systematically classify the lesions and to elucidate their origins. With donation, the patients receive a heart, which already has its own history of coronary atherosclerosis and in which all the phenotypes of ATS lesions are potentially already present. The immunological/inflammatory- and microvessel-derived hemorrhagic responses over time after transplantation cause coronary arterial pathology that is characterized by the onset of de novo lesions but also remodeling of already existing lesions (Fig. 5). Detailed knowledge of the entire spectrum of plaque types in CAV is not only important for understanding the pathogenesis of disease but also clinically for the interpretation of in vivo imaging techniques.
References
Rahmani M, Cruz RP, Granville DJ, McManus BM (2006) Allograft vasculopathy versus atherosclerosis. Circ Res 99:801–815
Mitchell NR (2013) Learning from rejection: what transplantation teaches us about (other) vascular pathologies. J Autoimmun 45:80–89
Suzuki J, Isobe M, Morishita R, Nagai R (2010) Characteristics of chronic rejection in heart transplantation: important elements of pathogenesis and future treatments. Circ J 74:233–239
Ardehali A (1995) Heart transplantation: accelerated graft atherosclerosis. Adv Card Surg 6:195–205
Grant SC, Brooks NH (1993) Accelerated graft atherosclerosis after heart transplantation. Br Heart J 69:469–470
Rossignol DA, Kipreos B, Akosah K, Mohanty PK (1999) Accelerate transplant coronary artery disease and massive silent acute myocardial infarction in a heart transplant patient—a case report and brief review of literature. Angiology 50:947–953
Johnson MR (1992) Transplant coronary disease: nonimmunologic risk factor. J Heart Lung Transplant 11:S124–S132
Mitchell RN, Libby P (2007) Vascular remodeling in transplant vasculopathy. Circ Res 100:967–978
McManus BM, Horley KJ, Wilson JE, Malcom GT, Kendall TJ, Miles RR, Winters GL, Costanzo MR, Miller LL, Radio SJ (1995) Prominence of coronary arterial wall lipids in human heart allograft. Implication for pathogenesis of allograft arteriopathy. Am J Pathol 147:293–308
Bundy RE, Marczin N, Birks EF, Chester AH, Yacoub MH (2000) Transplant atherosclerosis: role of phenotypic modulation of vascular smooth muscle by nitric oxide. Gen Pharmacol 34:73–84
Weis M, von Sheidt W (1997) Cardiac allograft vasculopathy: a review. Circulation 96:2069–2077
Fishbein GA, Fishbein MC (2009) Arteriosclerosis: rethinking the current classification. Arch Pathol Lab Med 133:1309–1316
Mehra MR, Crespo-Leiro MG, Dipchand A, Ensminger SM, Hiemann NE, Kobashigawa JA, Madsen J, Parameshwar J, Starling RC, Uber PA (2010) International society for heart and lung transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010. J Heart Lung Transplant 29:717–727
Stary HC, Chandler AB, Glagov S, Guyton JR, Insull W Jr, Rosenfeld ME, Schaffer SA, Schwartz CJ, Wagner WD, Wissler RW (1994) A definition of initial, fatty streak and intermediate lesions of atherosclerosis. A report from committee on vascular lesions of the council on atherosclerosis American heart association. Circulation 89:2462–2478
Stary HC, Chandler AB, Dinsmore RE, Fuster V, Glagov S, Insull W Jr, Rosenfeld ME, Schwartz CJ, Wagner WD, Wissler RW (1995) A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from committee on vascular lesions of the council on atherosclerosis American heart association. Artherioscler Thromb Vasc Biol 15:1512–1531
Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, Dobbels F, Kirk R, Rahmel AO, Hertz MI, International Society of Heart and Lung Transplantation (2012) The registry of the international society for heart and lung transplantation: 29th official adult heart transplant report-2012. J Heart Lung Transplant 31:1052–1064
Caforio AL, Tona F, Fortina AB, Angelini A, Piaserico S, Gambino A, Feltrin G, Ramondo A, Valente M, Iliceto S, Thiene G, Gerosa G (2004) Immune and nonimmune predictors of cardiac allograft vasculopathy onset and severity: multivariate risk factor analysis and role of immunosuppression. Am J Transplant 4:962–970
Schmauss D, Weis M (2008) Cardiac allograft vasculopathy. Recent developments. Circulation 117:2131–2141
Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM (2000) Lessons from sudden coronary death. A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 20:1262–1275
Johnson DE, Gao SZ, Schroeder JS, DeCampli WM, Billingham ME (1989) The spectrum of coronary artery pathological findings in human cardiac allograft. J Heart Transplant 8:349–359
Lu W, Palatnik K, Fishbein GA, Lai C, Levi DS, Perens G, Alejos J, Kobashigawa J, Fishbein MC (2011) Diverse morphologic manifestation of cardiac allograft vasculopathy: a pathological study of 64 allograft hearts. J Heart Lung Transplant 30:1044–1050
Pucci AM, Forbes RD, Billingham ME (1990) Pathological features in long-term cardiac allograft. J Heart Transplant 9:339–345
Haas M (2012) Pathological features of antibody-mediated rejection in renal allografts: an expanding spectrum. Curr Opin Nephrol Hypertens 21:264–271
Stegall MD, Park WD, Larson TS, Gloor JM, Cornell LD, Sethi S, Dean PG, Prieto M, Amer H, Textor S, Schwab T, Cosio FG (2011) The histology of solitary renal allografts at 1 and 5 years after transplantation. Am J Transplant 11:698–707
Tona F, Caforio AL, Montisci R, Angelini A, Ruscazio M, Gambino A, Ramondo A, Thiene G, Gerosa G, Iliceto S (2006) Coronary flow reserve by contrast-enhanced echocardiography: a new noninvasive diagnostic tool for cardiac allograft vasculopathy. Am J Transplant 6:998–1003
Angelini A, Castellani C, Tona F, Gambino A, Caforio AP, Feltrin G, Della Barbera M, Valente M, Gerosa G, Thiene G (2007) Continous engraftment and differentiation of male recipient Y-chromosome-positive cardiomyocytes in donor female human heart transplants. J Heart Lung Transplant 26:1110–1118
Gallo P, Agozzino L, Angelini A, Arbustini E, Bartoloni G, Bernucci P, Bonacina E, Bosman C, Catani G, di Gioia C, Giordana C, Leone O, Motta T, Pucci A, Rocco M (1997) Causes of late failure after heart transplantation: a ten-year survey. J Heart Lung Transplant 16:1113–1121
Virmani R, Kolodgie FD, Burke AP, Finn AV, Gold HK, Tulenko TN, Wrenn SP, Narula J (2005) Atherosclerotic plaque progression and vulnerability to rupture: angiogenesis as a source of intraplaque hemorrhage. Arterioscler Thromb Vasc Biol 25:2054–2061
Yeagle PL (1985) Cholesterol and the cell membrane. Biochim Biophys Acta 822:267–287
Kockx MM, Cromheeke KM, Knaapen MW, Bosmans JM, De Meyer GR, Herman AG, Bult H (2003) Phagocytosis and macrophage activation associated with hemorrhagic microvessels in human atherosclerosis. Arterioscler Thromb Vasc Biol 23:440–446
Koole D, Heyligers J, Moll F, Pasterkamp G (2012) Intraplaque neovascularization and hemorrhage: markers for cardiovascular risk stratification and therapeutic monitoring. J Cardiovasc Med (Hagerstown) 13:635–639. doi:10.2459/JCM.0b013e3283590cd2
Kolodgie FD, Gold HK, Burke AP, Fowler DR, Kruth HS, Weber DK, Farb A, Guerrero LJ, Hayase M, Kutys R, Narula J, Finn AV, Virmani R (2003) Intraplaque hemorrhage and progression of coronary atheroma. N Engl J Med 349:2316–2325
Takaya N, Yuan C, Chu B, Saam T, Polissar NL, Jarvik GP, Isaac C, McDonough J, Natiello C, Small R, Ferguson MS, Hatsukami TS (2005) Presence of intraplaque hemorrhage stimulates progression of carotid atherosclerotic plaques: a high resolution magnetic resonance imaging study. Circulation 111:2768–2775
Castellani C, Angelini A, de Boer OJ, van der Loos CM, Fedrigo M, Frigo AC, Meijer-Jorna LB, Li X, Ploegmakers HJ, Tona F, Feltrin G, Gerosa G, Valente M, Thiene G, van der Wal AC (2013) Intraplaque hemorrhage in cardiac allograft vasculopathy. Am J Transplant 14:184–192
van Loosdregt J, van Oosterhout MF, Bruggink AH, van Wichen DF, van Kuik J, de Koning E, Baan CC, de Jonge N, Gmelig-Meyling FH, de Weger RA (2006) The chemokine and chemokine receptor profile of infiltrating. Cells in the wall of arteries with cardiac allograft vasculopathy is indicative of a memory T–helper 1 response. Circulation 14:1599–1607
De Boer OJ, Becker AE, van der Wal AC (2003) T lymphocytes in atherogenesis—functional aspects and antigenic repertoire. Cardiovasc Res 60:78–86
Siow RCM, Churchman AT (2007) Adventitial growth factor signalling and vascular remodelling: potential perivascular gene transfer from outside-in. Cardiovasc Res 75:659–668
Baikoussis N, Apostolakis EE, Papakonstantinou NA, Siminelakis SN, Arnaoutoglou H, Papadopoulos G, Goudevenos J, Dougenis D (2011) The implication of vasa vasorum in surgical diseases of the aorta. Eur J Cardiothorac Surg 40:412–417
van der Wal AC, Becker AE, van der Loos CM, Das PK (1994) Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation 89:36–44
Hosono M, de Boer OJ, van der Wal AC, van der Loos CM, Teeling P, Piek JJ, Ueda M, Becker AE (2003) Increased expression of T cell activation markers (CD25, CD26, CD40L and CD69) in atherectomy speciments of patients with unstable angina and acute myocardial infarction. Atherosclerosis 168:73–80
Raichlin E, Bae JH, Kushwaha SS, Lennon RJ, Prasad A, Rihal CS, Lerman A (2009) Inflammatory burden of cardiac allograft coronary atherosclerotic plaque is associated with early recurrent cellular rejection and predicts a higher risk of vasculopathy progression. J Am Coll Cardiol 53:1279–1286
Stocin PGI, Sharples LD, Schofield PM, Cary NR, Mullins PA, English TA, Wallwoek J, Large SR (1993) Lack of association between endomyocardial evidence of rejection in the first six months and the later development of transplant-related coronary artery disease. J Heart Lung Transplant 12:110–116
Kfouri AG, Hammond ME, Snow GL, Drakos SG, Stehlik J, Fischer PW, Reid BB, Everitt MD, Bader FM, Renlund DG (2009) Cardiovascular mortality among heart transplant recipients with asymptomatic antibody-mediated or stable mixed cellular and antibody-mediated rejection. J Heart Transplant 28:781–784
Petrossian GA, Nichols AB, Marboe CC, Sciacca R, Rose EA, Smith CR, Cannon PJ, Reemtsma K, Powers ER (1989) Relation between survival and development of coronary artery disease and anti-HLA antibodies after cardiac transplantation. Circulation 80(III):122–125
Cherry R, Nielsen H, Reed E, Reemtsma K, Suciu-Foca N, Marboe CC (1992) Vascular (humoral) rejection in human cardiac allograft biopsies: relation to circulating anti-HLA antibodies. J Heart Lung Transplant 11:24–29
Wu GW, Kobashigawa JA, Fishbein MC, Patel JK, Kittleson MM, Reed EF, Kiyosaki KK, Ardehali A (2009) Asymptomatic antibody-mediated rejection after heart transplantation predicts poor outcomes. J Heart Lung Transplant 28:417–422
Poelzl G, Ullrich R, Huber A, Ulmer H, Antretter H, Hoefer D, Mairinger T, Laufer G, Pachinger O, Schwarzacher S (2005) Capillary deposition of the complement fragment C4d in cardiac allograft biopsies is associated with allograft vasculopathy. Transpl Int 18:313–317
Loupy A, Cazes A, Guillemain R, Amrein C, Hedjoudje A, Tible M, Pezzella V, Fabiani JN, Suberbielle C, Nochy D, Hill GS, Empana JP, Jouven X, Bruneval P, Duong Van Huyen JP (2011) Very late heart transplant rejection is associated with microvascular injury, complement deposition and progression to cardiac allograft vasculopathy. Am J Transplant 11:1478–1487
Tible M, Loupy A, Vernerey D, Suberbielle C, Beuscart T, Cazes A, Guillemain R, Amrein C, Pezzella V, Fabiani JN, Nochy D, Hill G, Empana JP, Jouven X, Charron D, Bruneval P, Duong Van Huyen JP (2013) Pathologic classification of antibody-mediated rejection correlates with donor-specific antibodies and endothelial cell activation. J Heart Lung Transplant 32:769–776
Jindra PT, Jin YP, Rozengurt E, Reed EF (2008) HLA class I antibody-mediated endothelial cell proliferation via the mTOR pathway. J Immunol 180:2357–2366
Valenzuela NM, Reed EF (2013) Antibodies in transplantation: the effects of HLA and non-HLA antibody binding and mechanisms of injury. Methods Mol Biol 1034:41–70
Kaczmarek I, Deutsch MA, Kauke T, Beiras-Fernandez A, Schmoeckel M, Vicol C, Sodian R, Reichart B, Spannagl M, Ueberfuhr P (2008) Donor-specific HLA alloantibodies:long term impact on cardiac allograft vasculopathy and mortality after heart transplant. Exp Clin Transplant 6:229–235
Eisen HJ, Tuzcu EM, Dorent R, Kobashigawa J, Mancini D, Valantine-von Kaeppler HA, Starling RC, Sørensen K, Hummel M, Lind JM, Abeywickrama KH, Bernhardt P, RAD B253 Study Group (2003) Everolimus for the prevention of allograft rejection and vasculopathy in cardiac-transplant recipients. N Engl J Med 349:847–858
Arora S, Erikstad I, Ueland T, Sigurdardottir V, Ekmehag B, Jansson K, Eiskjer H, Botker HE, Mortensen S-A, Saunamaki K, Gude E, Ragnarsson A, Solbu D, Aukrust P, Gullestad L (2012) Virtual Histology assessment of Cardiac Allograft vasculopathy following introduction of everolimus—results of a multicenter trial. Am J Transplant 12:2700–2709
Nasu K, Tsuchikane E, Katoh O, Vince DG, Virmani R, Surmely JF, Murata A, Takeda Y, Ito T, Ehara M, Matsubara T, Terashima M, Suzuki T (2006) Accuracy of in vivo coronary plaque morphology assessment: a validation study of in vivo virtual histology compared with in vitro histopathology. J Am Coll Cardiol 47:2405–2412
Dong L, Kerwin WS, Chen H, Chu B, Underhill HR, Neradilek MB, Hatsukami TS, Yuan C, Zhao XQ (2011) Carotid artery atherosclerosis: effect of intensive lipid therapy on the vasa vasorum—evaluation by using dynamic contrast-enhanced MR imaging. Radiology 260:224–231
Moguillansky D, Leng X, Carson A, Lavery L, Schwartz A, Chen X, Villanueva FS (2011) Quantification of plaque neovascularization using contrast ultrasound: a histologic validation. Eur Heart J 32:646–653
ten Kate GL, Sijbrands EJ, Valkema R, ten Cate FJ, Feinstein SB, van der Steen AF, Daemen MJ, Schinkel AF (2010) Molecular imaging of inflammation and intraplaque vasa vasorum: a step forward to identification of vulnerable plaques? J Nucl Cardiol 17:897–912
Narula J, Nakano M, Virmani R, Kolodgie FD, Petersen R, Newcomb R, Malik S, Fuster V, Finn AV (2013) Histopathologic characteristics of atherosclerotic coronary disease and implication of the findings for the invasive and noninvasive detection of vulnerable plaques. J Am Coll Cardiol 61:1041–1051
Castellani C, van der Wal AC, De Boer OJ, Fedrigo M, Thiene G, Valente M, Angelini A (2013) Virtual histology and the morphologic assessment of cardiac allograft vasculopathy. Am J Transplant 13:1109
Acknowledgments
The authors thank the Association for European Cardiovascular Pathology (AECVP). The authors thank Marco Pizzigolotto, Elisabetta Baliello, and Daniele Iannazzone for skillful technical assistance. This work was also supported by a research grant from University of Padua: PDR099073, CPDA108809, 60A07-5074, and 60A07-8587
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Angelini, A., Castellani, C., Fedrigo, M. et al. Coronary cardiac allograft vasculopathy versus native atherosclerosis: difficulties in classification. Virchows Arch 464, 627–635 (2014). https://doi.org/10.1007/s00428-014-1586-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-014-1586-6