
Abstract
Hypertrophic cardiomyopathy (HCM) is an inherited myocardial disease with an estimated prevalence of 1:200 caused by mutations in sarcomeric proteins. It is associated with hypertrophy of the left ventricle, increased interstitial fibrosis, and diastolic dysfunction for heterozygous mutation carriers. Carriers of double heterozygous, compound heterozygous, and homozygous mutations often display more severe forms of cardiomyopathies, ultimately leading to premature death. So far, there is no curative treatment against HCM, as current therapies are focused on symptoms relief by pharmacological intervention and not on the cause of HCM. In the last decade, several strategies have been developed to remove genetic defects, including genome editing, exon skipping, allele-specific silencing, spliceosome-mediated RNA trans-splicing, and gene replacement. Most of these technologies have already been tested for efficacy and efficiency in animal- or human-induced pluripotent stem cell models of HCM with promising results. We will summarize recent technological advances and their implication as gene therapy options in HCM with a special focus on treating MYBPC3 mutations and its potential for being a successful bench to bedside example.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is the most common Mendelian-inherited cardiomyopathy and the main cause of sudden cardiac death in individuals below the age of 35, mainly among young athletes (for detailed reviews, see [3, 46]). Its revised estimated prevalence is 1:200 in the general population occurring equally in both genders, whereby recent reports indicate worse survival in women [17, 60]. Clinical manifestations of HCM are variable in terms of disease development, age of onset, and severity of symptoms, causing chest pain, vertigo, syncope, and dyspnea, whereas others patients are in need for early heart transplantation, or die of sudden cardiac death [16, 48, 55]. Causative for these clinical symptoms are structural changes in the heart defined by chaotically oriented cardiac myocytes, so-called myocardial disarray, interstitial fibrosis and hypertrophy, mainly seen in the left ventricle [24]. About 70% of hospitalized HCM patients experience an abnormal thickening of the left ventricle, leading to outflow tract obstruction, which is often associated with normal systolic but impaired diastolic function [49]. If left untreated or undiagnosed, disease progression can result in left ventricular wall thinning, characterized as one of the main risk factors inducing irreversible heart failure and unexpected sudden cardiac death [48]. Current treatment options for HCM are drug-based therapies that aim to relieve associated symptoms and decelerate disease progression, but do not target the genetic cause of HCM (for review, see [70]). Up to now, more than 1400 mutations in over 11 different genes have been identified as a potential cause for HCM (reviewed in [14, 47, 67]). A large majority of these mutations are in genes encoding components of the cardiac sarcomere and are inherited in an autosomal-dominant pattern [64]. Most gene mutations were found in MYBPC3, encoding cardiac myosin-binding protein C (cMyBP-C) and in MYH7, encoding β-myosin heavy chain (for review, see [10]). Individuals carrying homozygous, double or triple mutations have more severe disease progression [18, 25, 28, 58, 75]. Especially, individuals with bi-allelic truncating MYBPC3 mutations were diagnosed with various forms of cardiomyopathy at birth and quickly developed systolic heart failure and died within the first year [40, 75, 78]. For these infants, there is no curative therapy apart from a heart transplant.
Cardiac gene therapy
The idea of gene therapy as a “therapeutic technique achieving permanent correction of hereditary diseases” has been introduced by Clyde Keeler in 1947 [37]. The first trial of human gene therapy has been approved in 1989 for advanced melanoma [65] and in 2004 for heart failure [30]. Today, more than 2300 clinical trials have been completed, are ongoing, or have been approved worldwide [23].
Probably the biggest hurdle for human gene therapy is sufficient and safe delivery of the gene therapy medicinal product into the patient’s body. For gene therapy of cardiac diseases, the currently used viral vectors are adeno-associated virus (AAV). These are small, non-enveloped virus belonging to the parvoviridae family with very low to absent pathogenicity in human host. Features such as the ability to transduce terminally differentiated cells (such as cardiomyocytes), absence of integration in the host genome, and long-lasting gene expression made the AAV attractive for gene therapy. In addition, AAVs naturally occur in different serotypes, which exhibit a distinct tissue tropism (for reviews, see [12, 59]). It has been shown that the serotype 9 (AAV9) is the most efficient for cardiac gene transfer after systemic delivery in mouse and large animal models [29, 52, 57, 62, 79]. The successful completion of a SERCA2a gene therapy phase 2 trial demonstrated safety and feasibility of AAV1-mediated gene transfer in humans [31]. Unfortunately, this study failed in showing beneficial outcomes in treated patients [20]. To further limit the expression of the transgene in cardiomyocytes, a cardiomyocyte-specific promoter such as cardiac troponin T could be used. A limitation of AAV-mediated gene therapy is that humans very frequently present neutralizing antibodies against AAV. These neutralizing antibodies might have a dramatic impact on the outcome of gene therapy and is major a problem in case of re-administration. This could be circumvented by pharmacological modulation of the immune response and/or use of another AAV serotype.
Targeting inherited disorders
Specifically for inherited (or monogenic) disease, there has been major progress in the field of molecular-based interventions to suppress the expression of genetic defects on DNA or RNA level, including genome editing, exon skipping, spliceosome-mediated RNA trans-splicing, allele-specific silencing, and gene replacement therapy. Tools used are clustered regularly interspaced short palindromic repeats (CRISPR)/Cas9, antisense oligonucleotides, RNA interference molecules or wild-type cDNA sequences, often combined with AAV delivery.
Genome editing
CRISPR/Cas9 transformed the field of genome editing by storm. Initially, the CRISPR/Cas9 system was found to be an adaptive immune response in bacteria (for reviews, see [27, 50]). Thirty years later, it has been demonstrated that CRISPR type-2 system proteins, called Cas9, can also function as designer nucleases by associating them with an engineered single guide RNA, which is complementary to a genetic locus of interest [33]. This targeted Cas9 is able to induce a double-strand break that can be resolved by endogenous DNA repair mechanisms such as non-homologous end-joining or by homology-directed repair [13, 38, 45]. Non-homologous end-joining is not desired for gene correction applications because it is prone to introduce additional mutations in the form of insertions and/or deletions. Homology-directed repair corrects the double-strand break site with a supplied exogenous DNA repair template or the non-mutant homologous chromosome, leading to the correction of the mutant allele (Fig. 1a; [42, 77]). Previously used genome editing tools were mostly zinc finger nucleases and transcription activator-like effector nucleases, which proved to be costly and labor intensive (for review, see [26]). CRISPR/Cas9, on the other hand, is a low-priced and quick method for disease modeling in human-induced pluripotent stem cell (hiPSC), mice and larger animal models (for review, see [66]). Recent reports demonstrated successful generation of HCM models or genetic correction in HCM hiPSC with CRISPR/Cas9 genome editing [6, 56, 74].

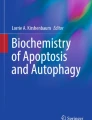
AAV-mediated gene therapy options for inherited disorders. The depicted gene therapy strategies combine a vector (e.g., adeno-associated virus, AAV) containing the gene therapy medicinal product (red circle) under the control of a promoter, which is delivered to the target cell via the most appropriate administration way such as systemic delivery. Viral particles enter the cells via specific receptors and then the nucleus (light blue), where the gene therapy medicinal product is transcribed to target either the DNA (CRISPR/Cas9), the pre-mRNA (antisense oligonucleotide, pre-trans-splicing molecule), the mRNA (RNA interference molecule) or to replace the loss-of-functional endogenous protein (full-length cDNA). a Genome editing with CRISPR/Cas9. Cas9 protein is produced within the cell and then targeted to the gene-of-interest with a specific single guide RNA. Cas9 produces double-strand break and the mutation is repaired by homology-directed repair with a repair template. This leads to a functional full-length mRNA and protein. b Exon skipping with antisense oligonucleotide. Antisense oligonucleotide targets exonic splicing enhancer sequences of an in-frame mutated exon, preventing binding of proteins involved in the splicing process. This induces the skipping of the mutated exon and the production of a shorter, but functional protein. c Exon skipping with CRISPR/Cas9. The specific single guide RNA brings Cas9 towards the targeted DNA sequence to permanently cut in-frame the mutated exon. Consequences are identical as in (b). d Allele-specific silencing. The mutant mRNA is knocked-down by a specific RNA interference molecule. This leads to its degradation and the absence of mutant protein. e RNA trans-splicing. The gene therapy medicinal product is a pre-trans-splicing molecule, encoding wild-type exonic and intronic sequences, including a specific complementary motif for endogenous target pre-mRNA. The pre-trans-splicing molecule hybridizes with the target pre-mRNA to generate a repaired mRNA molecule, devoid of mutation and a full-length functional protein. This process competes with cis-splicing, which gives rise to endogenous mRNA and proteins. f Gene replacement. The gene therapy medicinal product is a full-length cDNA that will be transcribed and translated into a functional full-length protein that compensates loss-of-function mutations. In the specific case of disease of the sarcomere, it also replaces the transcription and translation of endogenous genes. Abbreviations used are: AON, antisense oligonucleotide; Cas9, CRISPR type-2 system proteins; CRISPR, clustered regularly interspaced short palindromic repeats; DSB, double-strand break; HDR, homology-directed repair; RNAi, RNA interference; PTM, pre-trans-splicing molecule; sgRNA, single-guided RNA.
In the context of human gene therapy, much can be learned from the reports in mice, as viral-based delivery vectors of CRISPR/Cas9 components were able to edit postnatal murine hearts [11, 21, 34]. Targeted delivery of CRISPR/Cas9 components, no adverse side effects and efficient genome editing of non-dividing cardiomyocytes are three necessities that need to be ensured before applying this treatment to humans. Additionally, these studies showed that Cas9 overexpression in cardiomyocytes does not alter baseline cardiac function. In general, editing efficiencies and mosaicism are still limitations when using CRISPR/Cas9 in vivo. Indeed, homology-directed repair occurs primarily during the S/G2 phase of the cell cycle and therefore limits its application in (adult) cardiomyocytes. However, a recent study took advantage of the non-homologous end-joining, which is active throughout the cell cycle, including the G0/G1 phase of non-dividing cells, to establish the homology-independent targeted integration for gene targeting [68]. The authors reported an efficiency of ~ 60% after transduction of differentiated neurons and of ~ 3% in heart 2 weeks after AAV9-mediated systemic delivery in neonatal mice.
Moreover, CRISPR/Cas9 is also at the forefront of human germline therapy, since several studies have reported efficient and successful genome editing of human embryos [35, 41, 44, 69]. The study by Ma et al. focused on a male HCM patient with a familial history of HCM caused by a GAGT-deletion in exon 16 of the MYBPC3 gene [44]. The authors reported that correction of germline mutations was achieved by the activation of an endogenous, germline-specific DNA repair response. Therefore, double-strand breaks at the mutant paternal allele were predominantly repaired using the homologous wild-type maternal gene instead of a synthetic DNA template. Induction of double-strand breaks at specific cell cycle stages was able to increase homology-directed repair efficiencies up to 27% among targeted clones, and led to the prevention of mosaicism. Furthermore, no off-targets events were found. However, these findings remain controversial as inter-homologous recombination was never reported before, and already established methods, such as preimplantation genetic diagnosis, could be used to collect and identify eggs without a mutation for further implantation [9]. This would avoid editing of human embryos and therefore potential off-target effects. Nevertheless, these studies show that treatment of human germline mutations can be accomplished with CRISPR/Cas9.
Exon skipping
The concept of exon skipping strategies is to remove in-frame the exon(s) containing the gene defect(s), thereby creating a shorter, yet functional protein (for review, see [22]). Most of the studies used antisense oligonucleotides (Fig. 1b), which were designed to mask exonic splicing enhancer motifs to prevent binding of the splicing machinery on the endogenous pre-mRNA, ultimately leading to bounced exon(s) and a shorter mature mRNA. In the last years, a great deal of effort has been dedicated to the optimization of the chemistry of antisense oligonucleotides in order to increase their stability and performance. This therapeutic approach has been especially successful in Duchenne muscular dystrophy with the recent approval by the Food and Drug Administration of eteplirsen, the first ever antisense oligonucleotide-based drug (for review, see [1]). Besides antisense oligonucleotide, CRISPR/Cas9 genome editing (Fig. 1c) has been recently evaluated to permanently skip in-frame mutated exons of the dystrophin gene in myoblasts [61] or hiPSCs [39, 43] derived from patients with Duchenne muscular dystrophy, as well as in skeletal and cardiac muscles of a new mouse model of Duchenne muscular dystrophy generated with CRISPR/Cas9 [2]. Strikingly, in the latter study, 90% of dystrophin protein level was restored in both skeletal muscle and heart after a single systemic delivery of AAV9 encoding Cas9 and single guide RNAs in neonatal mice.
In the context of HCM, our group evaluated antisense oligonucleotide-based exon skipping as a gene therapy option in Mybpc3-targeted knock-in mice [15]. These mice carry a homozygous G>A transition on the last nucleotide of exon 6, which belongs to the highly conserved 5′ splice donor site sequence, resulting in different aberrant mRNAs [72]. This mutation is a founder mutation in Tuscany region in Italy where it accounts for 14% of all HCM cases [19]. In-frame skipping of both exons 5 and 6 of Mybpc3 with specifically designed antisense oligonucleotides and AAV9-mediated delivery in newborn mice abolished cardiac dysfunction and prevented the development of left ventricular hypertrophy. Although the therapeutic effect was transient, this first proof-of-concept study paves the way towards a causal therapy of HCM [15]. We think that AAV-mediated exon skipping with antisense oligonucleotide(s) or CRISPR/Cas9 remains a valuable therapeutic option for MYBPC3 mutation hot spots, such as exon 25 containing 11% of all exonic mutations [5].
Allele-specific silencing
Rapid development in allele-specific silencing by RNA interference (Fig. 1d) has proven to be another option to cure autosomal-dominant diseases by targeting the mutant allele in vitro or in vivo in mice [8, 51, 71].
In the context of HCM, this has been used with success to eliminate the mutant allele and delay the progression of cardiomyopathy in Myh6-targeted knock-in mice [32]. The limitations of this approach are the same as for exon skipping since several molecules should be designed and generated to target every mutation. On the other hand, this strategy could be of interest to target common single nucleotide polymorphisms, which would be co-transmitted with the mutant allele in patients.
RNA trans-splicing
The goal of this approach is to reduce the level of defective transcripts with a repaired full length mRNA. Trans-splicing occurs during mRNA maturation. It is a splicing reaction between two independently transcribed RNA molecules, a target endogenous mutant pre-mRNA and a therapeutic pre-trans-splicing molecule (Fig. 1e; for reviews, see [7, 73]). It is an attractive treatment option, since it uses the endogenous spliceosome machinery in the nucleus, does not require delivery of the complete gene and is restricted to those cells expressing the target pre-mRNA. Upon AAV-mediated delivery and transcription in the nucleus, the pre-trans-splicing molecule hybridizes with the target pre-mRNA to generate a chimeric mRNA molecule. Therefore, the amount of repaired mRNA should rise in comparison to the amount of mutant endogenous mRNA. Depending on the position of the mutation in the pre-mRNA, trans-splicing can occur in 5′- or 3′-mode and pre-trans-splicing molecules will contain a splice donor or acceptor site, respectively. Trans-splicing has already proven its potential as a treatment option for genetic diseases such as Duchenne muscular dystrophy and spinal muscular atrophy in vitro and in vivo (for review, see [5].
First evidence for successful 5′ trans-splicing in the context of HCM was reported by our group both in cardiomyocytes and in vivo in Mybpc3-targeted knock-in mice [53]. Although relatively successful in vitro, the repaired Mybpc3 mRNA represented only 0.14% of the total transcripts in the heart 7 days after AAV9 delivery, which was not enough to prevent the development of cardiac hypertrophy and dysfunction in HCM mice. We recently applied trans-splicing in the 5′- and 3′-mode to hiPSC-derived cardiomyocytes from an HCM patient, carrying a truncating MYBPC3 mutation [63]. Consistently with the report in Mybpc3-targeted knock-in mice, we also found very low trans-splicing efficiencies and therefore no repaired cMyBP-C protein. Low 5′ trans-splicing efficiency was also recently reported in Lmna-targeted knock-in mice with maturation defects in skeletal and cardiac muscles [4].
These studies showed that further optimization is needed to increase trans-splicing efficiencies, so that it can be taken into consideration as a treatment option in humans. Especially patients with HCM-associated MYBPC3 mutations could profit from trans-splicing because all mutations could be repaired with only two PTM molecules, covering the first and the second half of the MYBPC3 mRNA [63]. This treatment would therefore benefit 40–60% of all HCM patients (for reviews, see [5, 10]). In addition, trans-splicing is expected to result in a repaired full-length and functional cMyBP-C protein, in contrast to exon skipping. Furthermore, the authorization for marketing of two pre-trans-splicing molecules as new gene therapy medicinal product would be easier and quicker than for several antisense oligonucleotides, RNA interference or single guide RNA molecules.
Gene replacement
Gene replacement therapy is mainly applied when a mutation results in a low level or absence of the corresponding protein. In this case, full-length wild-type cDNA of the gene-of-interest is packaged and delivered by a vector to the cell of interest (Fig. 1f). Upon successful transduction, the cDNA sequence will find itself in the nucleus and transcription is initiated. The resulting exogenous mRNA is translated into a functional protein that replaces the missing mutant endogenous protein.
Gene replacement is particularly interesting for HCM-associated MYBPC3 mutations, because they usually result in a low level or absence of mutant proteins, causing haploinsufficiency (for review, see [10]). Additional expression of any sarcomeric protein is expected to replace the endogenous protein level and to prevent haploinsufficiency, because the sarcomere is a tightly regulated system with a preserved protein stoichiometry [70]. We previously showed that delivery of full-length wild-type Mybpc3 cDNA prevents the development of cardiac hypertrophy and dysfunction by increasing the amount of cMyBP-C protein in Mybpc3-targeted knock-in mice [52]. This successful proof-of-concept study in mice was achieved with a single systemic delivery of AAV9 encoding Mybpc3 under the control of human cardiac troponin T promoter in 1-day-old mice. For the observation period of 34 weeks, Mybpc3 mRNA and cMyBP-C protein levels increased in an AAV dose-dependent manner. Additionally, Mybpc3 gene therapy also suppressed accumulation of mutant mRNAs and consequently the production of poison peptides. In agreement to this, we showed that AAV-mediated MYBPC3 gene transfer dose-dependently restores the force of contraction to wild-type level in engineered heart tissue derived from cardiac cells of neonatal Mybpc3-targeted knock-out mice [76]. As an intermediate step towards humans, we further tested this concept in hiPSCs, which were retrieved from an HCM patient carrying a truncating MYBPC3 mutation in [63]. MYBPC3 mRNA and cMyBP-C protein levels were ~ 50% lower in patient-specific than in control hiPSC-derived cardiomyocytes. Additionally, patient-specific hiPSC-derived cardiomyocytes exhibited higher cell area and altered gene expression, reproducing human HCM features. AAV-mediated delivery of the human full-length MYBPC3 cDNA in patient-specific hiPSC-derived cardiomyocytes resulted in higher amounts of MYBPC3 mRNA and cMyBP-C protein 7 days after transduction. Furthermore, restoration of cMyBP-C haploinsufficiency was sufficient to suppress hypertrophy. Stoichiometry of the sarcomere was also preserved in the unrelated control hiPSC-derived cardiomyocytes, where MYBPC3 gene transfer resulted in higher levels of mRNA without changes in the level of cMyBP-C protein. Beneficial outcomes using gene replacement therapy were also reported in human embryonic stem cell-derived cardiomyocytes carrying a truncating MYBPC3 mutation [54]. In this study, adenoviral-mediated gene transfer of full-length MYBPC3 prevented hypertrophy, sarcomeric disarray and improved calcium impulse propagation in HCM cardiomyocytes 7 days after treatment. Additionally, Western blot analyses suggested more exogenous cMyBP-C protein in HCM than in control cardiomyocytes, which fits to preserved stoichiometry of the sarcomere as described above. No clinical study has been initiated yet using gene replacement therapy for HCM. Therefore, these studies represent an intermediate step towards clinical application.
Conclusion—future directions
Gene therapy targeting the cause of HCM is particularly attractive for the rare, severe forms with bi-allelic truncating mutations in MYBPC3 leading to heart failure and premature death in infants [75]. Among the different gene therapy options tested, gene replacement with AAV9-mediated delivery of functional MYBPC3 cDNA has already proven to be the most successful in mice [52] and in human pluripotent stem cell-derived cardiomyocytes [54, 63]. Gene replacement therapy is attractive for cardiomyopathy of the sarcomere, which is a tightly regulated protein complex with a preserved stoichiometry. Thus, any addition of a functional full-length cDNA should replace, at least in part if not all, the expression of the endogenous protein. Using AAV with a high cardiac tropism and a cardiomyocyte-specific promoter, any kind of sarcomere mutation can theoretically be corrected. Besides gene replacement therapy, AAV9-mediated delivery of Cas9 and single guide RNAs has already proven to be successful to induce in-frame exon skipping and reframing of dystrophin in a mouse model of Duchenne muscular dystrophy [2]. This exciting study certainly paves the way towards first-in-man and may also be a good strategy to address mutation hot spots in sarcomeric genes. However, in all cases, still novel technologies should be tested to augment AAV accumulation in the heart of large animal models and humans such as nanomaterial-coated capsids [36], to further increase the efficiency of CRISPR/Cas9-mediated homology-directed repair or homology-independent targeted integration in the heart in vivo, and to advance knowledge for the best AAV serotype for human heart. Finally, a joint effort between families, (pediatric) cardiologists and cardiac surgeons, gynecologists, geneticists, and basic scientists is necessary to form a basis to advance gene therapy towards first-in-patient, at least for the severe forms of inherited cardiomyopathy.
References
Aartsma-Rus A, Straub V, Hemmings R, Haas M, Schlosser-Weber G, Stoyanova-Beninska V, Mercuri E, Muntoni F, Sepodes B, Vroom E, Balabanov P (2017) Development of exon skipping therapies for Duchenne muscular dystrophy: a critical review and a perspective on the outstanding issues. Nucleic Acid Ther 27:251–259
Amoasii L, Long C, Li H, Mireault AA, Shelton JM, Sanchez-Ortiz E, McAnally JR, Bhattacharyya S, Schmidt F, Grimm D, Hauschka SD, Bassel-Duby R, Olson EN (2017) Single-cut genome editing restores dystrophin expression in a new mouse model of muscular dystrophy. Sci Transl Med 9:eaan8081
Ashrafian H, Watkins H (2007) Reviews of translational medicine and genomics in cardiovascular disease: new disease taxonomy and therapeutic implications cardiomyopathies: therapeutics based on molecular phenotype. J Am Coll Cardiol 49:1251–1264
Azibani F, Brull A, Arandel L, Beuvin M, Nelson I, Jollet A, Ziat E, Prudhon B, Benkhelifa-Ziyyat S, Bitoun M, Lorain S, Bonne G, Bertrand AT (2018) Gene therapy via trans-splicing for LMNA-related congenital muscular dystrophy. Mol Ther Nucleic Acids 10:376–386
Behrens-Gawlik V, Mearini G, Gedicke-Hornung C, Richard P, Carrier L (2014) MYBPC3 in hypertrophic cardiomyopathy: from mutation identification to RNA-based correction. Pflugers Arch 466:215–223
Ben Jehuda R, Eisen B, Shemer Y, Mekies LN, Szantai A, Reiter I, Cui H, Guan K, Haron-Khun S, Freimark D, Sperling SR, Gherghiceanu M, Arad M, Binah O (2018) CRISPR correction of the PRKAG2 gene mutation in the patient's induced pluripotent stem cell-derived cardiomyocytes eliminates electrophysiological and structural abnormalities. Heart Rhythm 15:267–276
Berger A, Maire S, Gaillard MC, Sahel JA, Hantraye P, Bemelmans AP (2016) mRNA trans-splicing in gene therapy for genetic diseases. Wiley Interdiscip Rev RNA 7:487–498
Bongianino R, Denegri M, Mazzanti A, Lodola F, Vollero A, Boncompagni S, Fasciano S, Rizzo G, Mangione D, Barbaro S, Di Fonso A, Napolitano C, Auricchio A, Protasi F, Priori SG (2017) Allele-specific silencing of mutant mRNA rescues ultrastructural and arrhythmic phenotype in mice carriers of the R4496C mutation in the ryanodine receptor gene (RYR2). Circ Res 121:525–536
Brezina PR, Kutteh WH (2015) Clinical applications of preimplantation genetic testing. BMJ 350:g7611
Carrier L, Mearini G, Stathopoulou K, Cuello F (2015) Cardiac myosin-binding protein C (MYBPC3) in cardiac pathophysiology. Gene 573:188–197
Carroll KJ, Makarewich CA, McAnally J, Anderson DM, Zentilin L, Liu N, Giacca M, Bassel-Duby R, Olson EN (2016) A mouse model for adult cardiac-specific gene deletion with CRISPR/Cas9. Proc Natl Acad Sci U S A 113:338–343
Chamberlain K, Riyad JM, Weber T (2017) Cardiac gene therapy with adeno-associated virus-based vectors. Curr Opin Cardiol 32:275–282
Cong L, Ran FA, Cox D, Lin S, Barretto R, Habib N, Hsu PD, Wu X, Jiang W, Marraffini LA, Zhang F (2013) Multiplex genome engineering using CRISPR/Cas systems. Science 339:819–823
Friedrich FW, Carrier L (2012) Genetics of hypertrophic and dilated cardiomyopathy. Curr Pharm Biotechnol 13:2467–2476
Gedicke-Hornung C, Behrens-Gawlik V, Reischmann S, Geertz B, Stimpel D, Weinberger F, Schlossarek S, Precigout G, Braren I, Eschenhagen T, Mearini G, Lorain S, Voit T, Dreyfus PA, Garcia L, Carrier L (2013) Rescue of cardiomyopathy through U7snRNA-mediated exon skipping in Mybpc3-targeted knock-in mice. EMBO Mol Med 5:1128–1145
Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW (2011) 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J Thorac Cardiovasc Surg 142:e153–e203
Geske JB, Ong KC, Siontis KC, Hebl VB, Ackerman MJ, Hodge DO, Miller VM, Nishimura RA, Oh JK, Schaff HV, Gersh BJ, Ommen SR (2017) Women with hypertrophic cardiomyopathy have worse survival. Eur Heart J 38:3434–3440
Girolami F, Ho CY, Semsarian C, Baldi M, Will ML, Baldini K, Torricelli F, Yeates L, Cecchi F, Ackerman MJ, Olivotto I (2010) Clinical features and outcome of hypertrophic cardiomyopathy associated with triple sarcomere protein gene mutations. J Am Coll Cardiol 55:1444–1453
Girolami F, Olivotto I, Passerini I, Zachara E, Nistri S, Re F, Fantini S, Baldini K, Torricelli F, Cecchi F (2006) A molecular screening strategy based on beta-myosin heavy chain, cardiac myosin binding protein C and troponin T genes in Italian patients with hypertrophic cardiomyopathy. J Cardiovasc Med (Hagerstown) 7:601–607
Greenberg B, Butler J, Felker GM, Ponikowski P, Voors AA, Desai AS, Barnard D, Bouchard A, Jaski B, Lyon AR, Pogoda JM, Rudy JJ, Zsebo KM (2016) Calcium upregulation by percutaneous administration of gene therapy in patients with cardiac disease (CUPID 2): a randomised, multinational, double-blind, placebo-controlled, phase 2b trial. Lancet 387:1178–1186
Guo Y, VanDusen NJ, Zhang L, Gu W, Sethi I, Guatimosim S, Ma Q, Jardin BD, Ai Y, Zhang D, Chen B, Guo A, Yuan GC, Song LS, Pu WT (2017) Analysis of cardiac myocyte maturation using CASAAV, a platform for rapid dissection of cardiac myocyte gene function in vivo. Circ Res 120:1874–1888
Hammond SM, Wood MJ (2011) Genetic therapies for RNA mis-splicing diseases. Trends Genet 27:196–205
Hanna E, Remuzat C, Auquier P, Toumi M (2017) Gene therapies development: slow progress and promising prospect. J Mark Access Health Policy 5:1265293
Ho CY (2010) Hypertrophic cardiomyopathy. Heart Fail Clin 6:141–159
Ho CY, Lever HM, DeSanctis R, Farver CF, Seidman JG, Seidman CE (2000) Homozygous mutation in cardiac troponin T: implications for hypertrophic cardiomyopathy. Circulation 102:1950–1955
Hockemeyer D, Jaenisch R (2016) Induced pluripotent stem cells meet genome editing. Cell Stem Cell 18:573–586
Hsu PD, Lander ES, Zhang F (2014) Development and applications of CRISPR-Cas9 for genome engineering. Cell 157:1262–1278
Ingles J, Doolan A, Chiu C, Seidman J, Seidman C, Semsarian C (2005) Compound and double mutations in patients with hypertrophic cardiomyopathy: implications for genetic testing and counselling. J Med Genet 42:e59
Ishikawa K, Fish KM, Tilemann L, Rapti K, Aguero J, Santos-Gallego CG, Lee A, Karakikes I, Xie C, Akar FG, Shimada YJ, Gwathmey JK, Asokan A, McPhee S, Samulski J, Samulski RJ, Sigg DC, Weber T, Kranias EG, Hajjar RJ (2014) Cardiac I-1c overexpression with reengineered AAV improves cardiac function in swine ischemic heart failure. Mol Ther 22:2038–2045
Jaski BE, Jessup ML, Mancini DM, Cappola TP, Pauly DF, Greenberg B, Borow K, Dittrich H, Zsebo KM, Hajjar RJ (2009) Calcium upregulation by percutaneous administration of gene therapy in cardiac disease (CUPID trial), a first-in-human phase 1/2 clinical trial. J Card Fail 15:171–181
Jessup M, Greenberg B, Mancini D, Cappola T, Pauly DF, Jaski B, Yaroshinsky A, Zsebo KM, Dittrich H, Hajjar RJ (2011) Calcium upregulation by percutaneous administration of gene therapy in cardiac disease (CUPID): a phase 2 trial of intracoronary gene therapy of sarcoplasmic reticulum Ca2+-ATPase in patients with advanced heart failure. Circulation 124:304–313
Jiang J, Wakimoto H, Seidman JG, Seidman CE (2013) Allele-specific silencing of mutant Myh6 transcripts in mice suppresses hypertrophic cardiomyopathy. Science 342:111–114
Jinek M, Chylinski K, Fonfara I, Hauer M, Doudna JA, Charpentier E (2012) A programmable dual-RNA-guided DNA endonuclease in adaptive bacterial immunity. Science 337:816–821
Johansen AK, Molenaar B, Versteeg D, Leitoguinho AR, Demkes C, Spanjaard B, de Ruiter H, Akbari Moqadam F, Kooijman L, Zentilin L, Giacca M, van Rooij E (2017) Postnatal cardiac gene editing using CRISPR/Cas9 with AAV9-mediated delivery of short guide RNAs results in mosaic gene disruption. Circ Res 121:1168–1181
Kang X, He W, Huang Y, Yu Q, Chen Y, Gao X, Sun X, Fan Y (2016) Introducing precise genetic modifications into human 3PN embryos by CRISPR/Cas-mediated genome editing. J Assist Reprod Genet 33:581–588
Kasala D, Yoon AR, Hong J, Kim SW, Yun CO (2016) Evolving lessons on nanomaterial-coated viral vectors for local and systemic gene therapy. Nanomedicine (Lond) 11:1689–1713
Keeler CE (1947) Gene therapy. J heredity 38:294–298
Kim S, Kim D, Cho SW, Kim J, Kim JS (2014) Highly efficient RNA-guided genome editing in human cells via delivery of purified Cas9 ribonucleoproteins. Genome Res 24:1012–1019
Kyrychenko V, Kyrychenko S, Tiburcy M, Shelton JM, Long C, Schneider JW, Zimmermann WH, Bassel-Duby R, Olson EN (2017) Functional correction of dystrophin actin binding domain mutations by genome editing. JCI Insight 2(18). https://doi.org/10.1172/jci.insight.95918
Lekanne Deprez RH, Muurling-Vlietman JJ, Hruda J, Baars MJ, Wijnaendts LC, Stolte-Dijkstra I, Alders M, van Hagen JM (2006) Two cases of severe neonatal hypertrophic cardiomyopathy caused by compound heterozygous mutations in the MYBPC3 gene. J Med Genet 43:829–832
Liang P, Xu Y, Zhang X, Ding C, Huang R, Zhang Z, Lv J, Xie X, Chen Y, Li Y, Sun Y, Bai Y, Songyang Z, Ma W, Zhou C, Huang J (2015) CRISPR/Cas9-mediated gene editing in human tripronuclear zygotes. Protein Cell 6:363–372
Lin S, Staahl BT, Alla RK, Doudna JA (2014) Enhanced homology-directed human genome engineering by controlled timing of CRISPR/Cas9 delivery. Elife 3:e04766
Long C, Li H, Tiburcy M, Rodriguez-Caycedo C, Kyrychenko V, Zhou H, Zhang Y, Min YL, Shelton JM, Mammen PPA, Liaw NY, Zimmermann WH, Bassel-Duby R, Schneider JW, Olson EN (2018) Correction of diverse muscular dystrophy mutations in human engineered heart muscle by single-site genome editing. Sci Adv 4:eaap9004
Ma H, Marti-Gutierrez N, Park SW, Wu J, Lee Y, Suzuki K, Koski A, Ji D, Hayama T, Ahmed R, Darby H, Van Dyken C, Li Y, Kang E, Park AR, Kim D, Kim ST, Gong J, Gu Y, Xu X, Battaglia D, Krieg SA, Lee DM, Wu DH, Wolf DP, Heitner SB, Belmonte JCI, Amato P, Kim JS, Kaul S, Mitalipov S (2017) Correction of a pathogenic gene mutation in human embryos. Nature 548:413–419
Mali P, Yang L, Esvelt KM, Aach J, Guell M, DiCarlo JE, Norville JE, Church GM (2013) RNA-guided human genome engineering via Cas9. Science 339:823–826
Maron BJ (2010) Contemporary insights and strategies for risk stratification and prevention of sudden death in hypertrophic cardiomyopathy. Circulation 121:445–456
Maron BJ, Maron MS (2013) Hypertrophic cardiomyopathy. Lancet 381:242–255
Maron BJ, Olivotto I, Spirito P, Casey SA, Bellone P, Gohman TE, Graham KJ, Burton DA, Cecchi F (2000) Epidemiology of hypertrophic cardiomyopathy-related death: revisited in a large non-referral-based patient population. Circulation 102:858–864
Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG, Kuvin JT, Nistri S, Cecchi F, Udelson JE, Maron BJ (2006) Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation 114:2232–2239
Marraffini LA (2015) CRISPR-Cas immunity in prokaryotes. Nature 526:55–61
Matsa E, Dixon JE, Medway C, Georgiou O, Patel MJ, Morgan K, Kemp PJ, Staniforth A, Mellor I, Denning C (2014) Allele-specific RNA interference rescues the long-QT syndrome phenotype in human-induced pluripotency stem cell cardiomyocytes. Eur Heart J 35:1078–1087
Mearini G, Stimpel D, Geertz B, Weinberger F, Krämer E, Schlossarek S, Mourot-Filiatre J, Stöhr A, Dutshc A, Wijnker PJM, Braren I, Katus HA, Müller OJ, Voit T, Eschenhagen T, Carrier L (2014) Mybpc3 gene therapy for neonatal cardiomyopathy enables longterm disease prevention in mice. Nat Commun 5:5515
Mearini G, Stimpel D, Kramer E, Geertz B, Braren I, Gedicke-Hornung C, Precigout G, Muller OJ, Katus HA, Eschenhagen T, Voit T, Garcia L, Lorain S, Carrier L (2013) Repair of Mybpc3 mRNA by 5′-trans-splicing in a mouse model of hypertrophic cardiomyopathy. Mol Ther Nucleic Acids 2:e102
Monteiro da Rocha A, Guerrero-Serna G, Helms A, Luzod C, Mironov S, Russell M, Jalife J, Day SM, Smith GD, Herron TJ (2016) Deficient cMyBP-C protein expression during cardiomyocyte differentiation underlies human hypertrophic cardiomyopathy cellular phenotypes in disease specific human ES cell derived cardiomyocytes. J Mol Cell Cardiol 99:197–206
Moolman JC, Corfield VA, Posen B, Ngumbela K, Seidman CE, Brink PA, Watkins H (1997) Sudden death due to troponin T mutations. J Am Coll Cardiol 29:549–555
Mosqueira D, Mannhardt I, Bhagwan JR, Lis-Slimak K, Katili P, Scott E, Hassan M, Prondzynski M, Harmer SC, Tinker A, Smith JGW, Carrier L, Williams PM, Gaffney D, Eschenhagen T, Hansen A, Denning C (2018) CRISPR/Cas9 editing in human pluripotent stem cell-cardiomyocytes highlights arrhythmias, hypocontractility, and energy depletion as potential therapeutic targets for hypertrophic cardiomyopathy. Eur Heart J. https://doi.org/10.1093/eurheartj/ehy249
Murrey DA, Naughton BJ, Duncan FJ, Meadows AS, Ware TA, Campbell KJ, Bremer WG, Walker CM, Goodchild L, Bolon B, La Perle K, Flanigan KM, McBride KL, McCarty DM, Fu H (2014) Feasibility and safety of systemic rAAV9-hNAGLU delivery for treating mucopolysaccharidosis IIIB: toxicology, biodistribution, and immunological assessments in primates. Hum Gene Ther Clin Dev 25:72–84
Nanni L, Pieroni M, Chimenti C, Simionati B, Zimbello R, Maseri A, Frustaci A, Lanfranchi G (2003) Hypertrophic cardiomyopathy: two homozygous cases with "typical" hypertrophic cardiomyopathy and three new mutations in cases with progression to dilated cardiomyopathy. Biochem Biophys Res Commun 309:391–398
Naso MF, Tomkowicz B, Perry WL 3rd, Strohl WR (2017) Adeno-associated virus (AAV) as a vector for gene therapy. BioDrugs 31:317–334
Olivotto I, Maron MS, Adabag AS, Casey SA, Vargiu D, Link MS, Udelson JE, Cecchi F, Maron BJ (2005) Gender-related differences in the clinical presentation and outcome of hypertrophic cardiomyopathy. J Am Coll Cardiol 46:480–487
Ousterout DG, Kabadi AM, Thakore PI, Majoros WH, Reddy TE, Gersbach CA (2015) Multiplex CRISPR/Cas9-based genome editing for correction of dystrophin mutations that cause Duchenne muscular dystrophy. Nat Commun 6(6244):6244
Pleger ST, Shan C, Ksienzyk J, Bekeredjian R, Boekstegers P, Hinkel R, Schinkel S, Leuchs B, Ludwig J, Qiu G, Weber C, Raake P, Koch WJ, Katus HA, Muller OJ, Most P (2011) Cardiac AAV9-S100A1 gene therapy rescues post-ischemic heart failure in a preclinical large animal model. Sci Transl Med 3:92ra64
Prondzynski M, Kramer E, Laufer SD, Shibamiya A, Pless O, Flenner F, Muller OJ, Munch J, Redwood C, Hansen A, Patten M, Eschenhagen T, Mearini G, Carrier L (2017) Evaluation of MYBPC3 trans-splicing and gene replacement as therapeutic options in human iPSC-derived cardiomyocytes. Mol Ther Nucleic Acids 7:475–486
Richard P, Charron P, Carrier L, Ledeuil C, Cheav T, Pichereau C, Benaiche A, Isnard R, Dubourg O, Burban M, Gueffet JP, Millaire A, Desnos M, Schwartz K, Hainque B, Komajda M (2003) Hypertrophic cardiomyopathy: distribution of disease genes, spectrum of mutations and implications for molecular diagnosis strategy. Circulation 107:2227–2232
Rosenberg SA, Aebersold P, Cornetta K, Kasid A, Morgan RA, Moen R, Karson EM, Lotze MT, Yang JC, Topalian SL et al (1990) Gene transfer into humans—immunotherapy of patients with advanced melanoma, using tumor-infiltrating lymphocytes modified by retroviral gene transduction. N Engl J Med 323:570–578
Sander JD, Joung JK (2014) CRISPR-Cas systems for editing, regulating and targeting genomes. Nat Biotechnol 32:347–355
Schlossarek S, Mearini G, Carrier L (2011) Cardiac myosin-binding protein C in hypertrophic cardiomyopathy: mechanisms and therapeutic opportunities. J Mol Cell Cardiol 50:613–620
Suzuki K, Tsunekawa Y, Hernandez-Benitez R, Wu J, Zhu J, Kim EJ, Hatanaka F, Yamamoto M, Araoka T, Li Z, Kurita M, Hishida T, Li M, Aizawa E, Guo S, Chen S, Goebl A, Soligalla RD, Qu J, Jiang T, Fu X, Jafari M, Esteban CR, Berggren WT, Lajara J, Nunez-Delicado E, Guillen P, Campistol JM, Matsuzaki F, Liu GH, Magistretti P, Zhang K, Callaway EM, Zhang K, Belmonte JC (2016) In vivo genome editing via CRISPR/Cas9 mediated homology-independent targeted integration. Nature 540:144–149
Tang L, Zeng Y, Du H, Gong M, Peng J, Zhang B, Lei M, Zhao F, Wang W, Li X, Liu J (2017) CRISPR/Cas9-mediated gene editing in human zygotes using Cas9 protein. Mol Gen Genomics 292:525–533
Tardiff JC, Carrier L, Bers DM, Poggesi C, Ferrantini C, Coppini R, Maier LS, Ashrafian H, Huke S, van der Velden J (2015) Targets for therapy in sarcomeric cardiomyopathies. Cardiovasc Res 105:457–470
Trochet D, Prudhon B, Beuvin M, Peccate C, Lorain S, Julien L, Benkhelifa-Ziyyat S, Rabai A, Mamchaoui K, Ferry A, Laporte J, Guicheney P, Vassilopoulos S, Bitoun M (2018) Allele-specific silencing therapy for dynamin 2-related dominant centronuclear myopathy. EMBO Mol Med 10:239–253
Vignier N, Schlossarek S, Fraysse B, Mearini G, Kramer E, Pointu H, Mougenot N, Guiard J, Reimer R, Hohenberg H, Schwartz K, Vernet M, Eschenhagen T, Carrier L (2009) Nonsense-mediated mRNA decay and ubiquitin-proteasome system regulate cardiac myosin-binding protein C mutant levels in cardiomyopathic mice. Circ Res 105:239–248
Wally V, Murauer EM, Bauer JW (2012) Spliceosome-mediated trans-splicing: the therapeutic cut and paste. J Invest Dermatol 132:1959–1966
Wang L, Kim K, Parikh S, Cadar AG, Bersell KR, He H, Pinto JR, Kryshtal DO, Knollmann BC (2018) Hypertrophic cardiomyopathy-linked mutation in troponin T causes myofibrillar disarray and pro-arrhythmic action potential changes in human iPSC cardiomyocytes. J Mol Cell Cardiol 114:320–327
Wessels MW, Herkert JC, Frohn-Mulder IM, Dalinghaus M, van den Wijngaard A, de Krijger RR, Michels M, de Coo IF, Hoedemaekers YM, Dooijes D (2015) Compound heterozygous or homozygous truncating MYBPC3 mutations cause lethal cardiomyopathy with features of noncompaction and septal defects. Eur J Hum Genet 23:922–928
Wijnker PJ, Friedrich FW, Dutsch A, Reischmann S, Eder A, Mannhardt I, Mearini G, Eschenhagen T, van der Velden J, Carrier L (2016) Comparison of the effects of a truncating and a missense MYBPC3 mutation on contractile parameters of engineered heart tissue. J Mol Cell Cardiol 97:82–92
Wu Y, Liang D, Wang Y, Bai M, Tang W, Bao S, Yan Z, Li D, Li J (2013) Correction of a genetic disease in mouse via use of CRISPR-Cas9. Cell Stem Cell 13:659–662
Xin B, Puffenberger E, Tumbush J, Bockoven JR, Wang H (2007) Homozygosity for a novel splice site mutation in the cardiac myosin-binding protein C gene causes severe neonatal hypertrophic cardiomyopathy. Am J Med Genet A 143A:2662–2667
Ziegler T, Kraus M, Husada W, Gesenhues F, Jiang Q, Pinkenburg O, Trenkwalder T, Laugwitz KL, le Noble F, Weber C, Kupatt C, Hinkel R (2017) Steerable induction of the Thymosin beta4/MRTF-A pathway via AAV-based overexpression induces therapeutic neovascularization. Hum Gene Ther
Acknowledgements
We would like to thank Suellen Lopes Oliveira for graphic design of the figure.
Funding
This work was supported by the DZHK (German Centre for Cardiovascular Research) and the German Ministry of Research Education (BMBF).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
L.C. and G.M. are co-applicants and holders of a provisional patent no. PCT/EP2014/057984 (WO 2014/170470 A1; EP2792742 A1; CA2944186 A1), Priority date Apr 17, 2013, Filling date Apr 17, 2014, publication date Oct 23, 2014. The authors declare no competing financial interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the special issue on Sarcomeric Mutations in Pflügers Archiv—European Journal of Physiology
Rights and permissions
About this article

Cite this article
Prondzynski, M., Mearini, G. & Carrier, L. Gene therapy strategies in the treatment of hypertrophic cardiomyopathy. Pflugers Arch - Eur J Physiol 471, 807–815 (2019). https://doi.org/10.1007/s00424-018-2173-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-018-2173-5