
Abstract
Endothelium-derived nitric oxide (NO) is a paracrine factor that controls vascular tone, inhibits platelet function, prevents adhesion of leukocytes, and reduces proliferation of the intima. An enhanced inactivation and/or reduced synthesis of NO is seen in conjunction with risk factors for cardiovascular disease. This condition, referred to as endothelial dysfunction, can promote vasospasm, thrombosis, vascular inflammation, and proliferation of vascular smooth muscle cells. Vascular oxidative stress with an increased production of reactive oxygen species (ROS) contributes to mechanisms of vascular dysfunction. Oxidative stress is mainly caused by an imbalance between the activity of endogenous pro-oxidative enzymes (such as NADPH oxidase, xanthine oxidase, or the mitochondrial respiratory chain) and anti-oxidative enzymes (such as superoxide dismutase, glutathione peroxidase, heme oxygenase, thioredoxin peroxidase/peroxiredoxin, catalase, and paraoxonase) in favor of the former. Also, small molecular weight antioxidants may play a role in the defense against oxidative stress. Increased ROS concentrations reduce the amount of bioactive NO by chemical inactivation to form toxic peroxynitrite. Peroxynitrite—in turn—can “uncouple” endothelial NO synthase to become a dysfunctional superoxide-generating enzyme that contributes to vascular oxidative stress. Oxidative stress and endothelial dysfunction can promote atherogenesis. Therapeutically, drugs in clinical use such as ACE inhibitors, AT1 receptor blockers, and statins have pleiotropic actions that can improve endothelial function. Also, dietary polyphenolic antioxidants can reduce oxidative stress, whereas clinical trials with antioxidant vitamins C and E failed to show an improved cardiovascular outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The endothelial cells of our vasculature—if functional—protect us against thrombosis and atherosclerosis. A key regulator of endothelial function is endothelium-derived nitric oxide (NO) generated by endothelial NO synthase (eNOS) [28]. Vascular NO relaxes blood vessels, prevents platelet aggregation and adhesion, limits oxidation of low-density lipoprotein (LDL) cholesterol, inhibits proliferation of vascular smooth muscle cells, and decreases the expression of pro-inflammatory genes that advance atherogenesis [26–28].
Cardiac risk factors and cardiovascular disease impair endothelial function. An increased production and/or impaired inactivation of reactive oxygen species (ROS), i.e., oxidative stress, leads to reduced bioactivity of NO. A dominant mechanism reducing bioavailability of vascular NO is rapid oxidative inactivation by the ROS superoxide (O −2 ·). In addition, there is evidence that persisting oxidative stress will render eNOS dysfunctional such that it no longer produces NO, but O −2 · [26, 27]. This review discusses the interrelationship between vascular disease and vascular oxidative stress, as well as therapeutic approaches, to reduce oxidative stress and restore endothelial function.
Structure and enzymatic function of eNOS
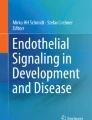
Structurally, all NOS isozymes are homodimers (Fig. 1). In a functional NOS, the C-terminal reductase domain of one monomer (with binding sites for NADPH, FMN, and FAD) is linked to the N-terminal oxygenase domain of the opposite monomer (Fig. 1). This oxygenase domain carries a prosthetic heme group. Theoxygenase domain also binds (6R-)5,6,7,8-tetrahydrobiopterin (BH4), molecular oxygen, and the substrate l-arginine [1, 19]. All NOS isoforms show a zinc thiolate cluster formed by a zinc ion that is tetrahedrally coordinated to two CXXXXC motifs (one contributed by each monomer) at the interface of the NOS dimer [46, 73, 86, 107]. All NOS isozymes catalyze flavin-mediated electron transfer from the C-terminally bound NADPH to the heme in the N-terminal oxygenase domain. Calmodulin (CaM), upon calcium-induced binding to the NOS, increases both the electron transfer within the reductase domain (from NADPH to the flavins; Fig. 1) and the electron transfer from the reductase domain to the heme center in the oxygenase domain (Fig. 1) [45]. At the heme, the electrons are used to reduce and activate O2. In a first step, NOS hydroxylates l-arginine to \( {NG } \) N G-hydroxy-l-arginine (which remains largely bound to the enzyme). In a second step, NOS oxidizes N G-hydroxy-l-arginine to citrulline and NO [96, 123]. In human eNOS, cysteine99 (Cys99, which is part of the zinc thiolate cluster) is thought to represent (or largely contribute to) the binding site for BH4. Mutation of the homologous Cys331 in nNOS to alanine (Cys331Ala) led to an enzyme that lost its binding affinity for BH4 and became catalytically inactive [81]. Interestingly, the estimated K d for l-arginine binding to the Cys331Ala-mutated nNOS was >100 μmol/L [81] compared with 2–3 μmol/L for the wild-type enzyme, suggesting cooperativity between l-arginine and BH4. binding (Fig. 1) [81, 85].

Scheme of a functional eNOS. eNOS is a homodimeric enzyme; each subunit consists of a reductase domain and an oxygenase domain. NADPH donates electrons for NOS; the flow of electrons is only shown from the reductase domain of one monomer (left) to the oxygenase domain of the other monomer. The enzyme contains a zinc (Zn) thiolate cluster at the dimer interface. This site is of major importance for the binding of the cofactor (6R-)5,6,7,8-tetrahydrobiopterin (BH 4 ) and the substrate l-arginine (l -Arg). Interestingly, there is evidence for a mutual enhancement of BH4 and l-arginine binding, which may be of therapeutic relevance in vivo. Electron transfer from the reductase domain (*) enables NOS ferric (Fe3+) heme to bind O2 and form a ferrous (Fe2+)-dioxy species. This species may receive a second electron preferentially from BH4 (or alternatively from the reductase domain) (**). This activates oxygen and allows the catalysis of l-arginine hydroxylation. The oxidized species formed from BH4 is trihydrobiopterin radical (BH3·) or trihydropterin radical cation protonated at N5 (BH3·H+). The BH3· radical (or radical cation) can be recycled to BH4 by eNOS itself (using an electron supplied by the flavins) or by l-ascorbic acid (which is present in cells in millimolar concentrations). This function of l-ascorbic acid can explain its stimulatory effect on eNOS activity. The BH3· radical can be converted to the quinonoid 6,7-[8H]-H2-biopterin (BH2), which can also be reduced by l-ascorbic acid back to BH4. BH4 is likely to also play a redox role in the second reaction cycle, i.e., the conversion of \( {N^\omega } \)-hydroxy-l-arginine to NO. AscH ascorbic acid, Asc ascorbate radical
Regulation of eNOS activity
When intracellular Ca2+ is enhanced, eNOS activity markedly increases; eNOS synthesizes NO in a pulsatile, Ca2+/CaM-dependent manner. Ca2+ induces the binding of CaM to the enzyme, which in turn increases the rate of electron transfer from NADPH to the heme center [45].
However, eNOS can also be activated by stimuli that do not produce sustained increases in intracellular Ca2+, but still induce a long-lasting release of NO. The best established such stimulus is the shear stress of the flowing blood, which can increase enzyme activity at resting Ca2+ levels. This activation is mediated by phosphorylation of the enzyme [25] (Fig. 2).

Regulation of eNOS activity by intracellular Ca2+ and phosphorylation. An increase in intracellular Ca2+ (as produced by agonists such as histamine or bradykinin) leads to an enhanced binding of CaM to the enzyme, which in turn displaces an auto-inhibitory loop and facilitates the flow of electrons from NADPH in the reductase domain to the heme in the oxygenase domain. There are several potential phosphorylation sites in eNOS, but most is known about the functional consequences of phosphorylation of Ser1177 (human eNOS sequence) in the reductase domain and Thr495 (human eNOS sequence) within the CaM-binding domain. In resting endothelial cells, Ser1177 is usually not phosphorylated. Phosphorylation is induced when the cells are exposed to fluid shear stress, estrogens, VEGF, insulin, or bradykinin. The kinases responsible for phosphorylation depend on the primary stimulus. Shear stress elicits the phosphorylation of Ser1177 by activating protein kinase A (PKA), estrogen and VEGF phosphorylate eNOS mainly via Akt, insulin probably activates both Akt and the AMP-activated protein kinase (AMPK), and the bradykinin-induced phosphorylation of Ser1177 is mediated by CaMKII. Phosphorylation of the Ser1177 residue increases the flux of electrons through the reductase domain and thus enzyme activity. The Thr495 residue of human eNOS tends to be constitutively phosphorylated in endothelial cells. Thr495 is a negative regulatory site, and its phosphorylation is associated with a decrease in enzyme activity. The constitutively active kinase that phosphorylates eNOS Thr495 is most probably protein kinase C (PKC). The phosphatase that dephosphorylates Thr495 appears to be protein phosphatase1
The eNOS protein can be phosphorylated on several serine (Ser), threonine (Thr), and tyrosine (Tyr) residues; however, major changes in enzyme function have been reported for the phosphorylation of amino acid residues Ser1177 and Thr495 (in the human eNOS sequence). Phosphorylation of Ser1177 stimulates the flux of electrons within the reductase domain, increases the Ca2+ sensitivity of the enzyme, and represents an additional and independent mechanism of eNOS activation [25]. Several protein kinases can phosphorylate eNOS at Ser1177 can participate in eNOS activation following mechanical and/or hormonal stimulation of endothelial cells. These kinases include Akt/protein kinase B, protein kinase A (PKA), 5′-AMP-activated protein kinase (AMPK), and calmodulin-dependent kinase II (CAMKII) (Fig. 2).
The amino acid residue Thr495, on the other hand, is a negative regulatory site whose phosphorylation decreases enzymatic activity. This site tends to be phosphorylated under non-stimulated conditions (most probably by protein kinase C, PKC). Phosphorylation of Thr495 is likely to interfere with the binding of CaM to the CaM-binding domain. In fact, dephosphorylation of Thr495 is associated with stimuli such as histamine or bradykinin that elevate intracellular Ca2+ concentrations and increase eNOS activity markedly. In endothelial cells stimulated with such Ca2+-elevating agonists, substantially more CaM binds to eNOS when Thr495 is dephosphorylated [25] (Fig. 2).
In vascular disease, oxidative stress reduces the bioavailability of vascular NO
Oxidative stress in vascular disease (i.e., a relative overproduction of ROS), contributes markedly to endothelial dysfunction. In the state of oxidative stress, the production of ROS exceeds the available antioxidant defense systems. As a consequence, bioactivity of NO is reduced. A dominant mechanism reducing bioavailability of vascular NO relates to its rapid oxidative inactivation by the ROS superoxide (O −2 ). In addition, there is evidence that persisting oxidative stress will render eNOS dysfunctional such that it no longer produces NO, but O −2 · (see below).
Cardiovascular risk factors and vascular disease are associated with an increased production of reactive oxygen species in the vascular wall
Risk factors for cardiovascular disease include (but are not limited to) hypertension [75], diabetes mellitus [48], hypercholesterolemia [142], and atherosclerosis [115]. These risk factors lead to dramatic increases in reactive ROS in the vascular wall, a situation that culminates into oxidative stress. ROS include free oxygen radicals, oxygen ions, and peroxides (Fig. 3a). There are several enzyme systems that can potentially produce ROS in the vessel wall, with four systems being of major importance. These include NADPH oxidase, xanthine oxidase, a dysfunctional eNOS (in which oxygen reduction is uncoupled from NO synthesis), and enzymes of the mitochondrial respiratory chain [92] (Fig. 3a).

Enzymes involved in the generation and inactivation of reactive oxygen species (ROS). There are numerous enzyme systems that generate and degrade ROS; a relative overproduction of ROS results in oxidative stress (light red box, a). Molecular oxygen (O 2) reacts with an impaired electron (e −) to form the superoxide anion (O 2 − ·). Numerous studies implicate NADPH oxidases, xanthine oxidase, “uncoupled” eNOS (in which oxygen reduction has been uncoupled from NO synthesis), and the “leakage” of activated oxygen from mitochondria during oxidative respiration as important sources of O −2 · in the cardiovascular system (red boxes). O −2 · can be converted to hydrogen peroxide (H2O2, the two-electron reduction state of O2) by the enzyme superoxide dismutase. H2O2 can undergo spontaneous conversion to hydroxyl radical (OH·, the three-electron reduction state of O2) via the Fenton reaction. OH· is extremely reactive and will attack most cellular components. H2O2 can be detoxified via glutathione peroxidase, catalase, or thioredoxin (Trx) peroxidase to H2O and O2 (green boxes). The enzyme myeloperoxidase can use H2O2 to oxidize chloride to the strong oxidizing agent hypochlorous acid (HOCl). Blood levels of myeloperoxidase have been found to correlate with endothelial dysfunction and the risk for myocardial infarction. HOCl can chlorinate and thereby inactivate various biomolecules, including lipoproteins and the eNOS substrate l-arginine. Besides HOCl generation, MPO can oxidize NO to nitrite (NO −2 ) in the vasculature. Also inducible heme oxygenase 1 and its products function as adaptive molecules against oxidative stress (b). Heme oxygenase is the first rate-limiting enzyme in heme breakdown to generate equimolar quantities of carbon monoxide (CO), biliverdin, and free ferrous iron. For mechanisms by which heme oxygenase reduces oxidative stress, see text. Other enzymes with antioxidant properties are paraoxonases. Paraoxonase isoforms 1 and 3 are circulating in serum residing on high-density lipoprotein, decreasing high- and low-density lipoprotein lipid peroxidation. Paraoxonase 2 is cell-associated and seems to represent a novel endogenous defense mechanism against vascular oxidative stress. The biochemical mechanism is still largely unclear
NADPH oxidases
NADPH oxidases are multicomponent enzymes functional in membranes of various cell types including endothelial cells, smooth muscle cells, and fibroblasts. Several isoforms of O −2 ·-producing NADPH oxidase exist in the vascular wall. Evidence for an activation of NADPH oxidase in the vasculature has been provided in animal models of vascular disease such as angiotensin II-induced hypertension [31, 83], genetic hypertension [76], diabetes mellitus [48], and hypercholesterolemia [142]. In atherosclerotic arteries, there is evidence for increased expression of the NADPH oxidase subunits gp91phox (Nox2) and Nox4 [115]; angiotensin II leads to an overexpression of Nox1 [83]. A confirmation of the role of NADPH oxidase-derived ROS in hypertension and atherosclerosis came from studies with genetic disruption of subunits of the enzyme. Knockout of the p47phox subunit reduced blood pressure responses to angiotensin II and diminished atherogenesis in apolipoprotein E (apoE)−/− mice [6, 65]. Similarly, Nox1-deficient mice show smaller blood pressure increases to angiotensin II [83], whereas mice overexpressing Nox1 in smooth muscle showed greater blood pressure responses to angiotensin II and increased O −2 · production [21].
Involvement of the renin–angiotensin system
The inflammatory cells present in the atherosclerotic vessel wall are capable of producing angiotensin II. Angiotensin-converting enzyme activity, as well as local angiotensin II concentrations, is increased in atherosclerotic plaques [20, 100]. In addition, in hypercholesterolemia, local renin–angiotensin systems may be activated. The stimulating effects of angiotensin II on the activity of NADPH oxidases suggests that an activated renin–angiotensin system could cause increased vascular O −2 · production and thus vascular dysfunction [35]. In vessels from hypercholesterolemic animals [133] and in platelets from hypercholesterolemic patients [95], the angiotensin II receptor subtype AT1 has been found to be upregulated.
Xanthine oxidase
The enzyme xanthine oxidase is generated from xanthine dehydrogenase by proteolysis. Xanthine oxidase readily donates electrons to molecular oxygen, thereby producing O −2 · and hydrogen peroxide. Oxypurinol, an inhibitor of xanthine oxidase, has been shown to reduce O −2 · production and improve endothelium-dependent vascular relaxations to acetylcholine in blood vessels from hyperlipidemic animals [98]. This suggests a contribution of xanthine oxidase to endothelial dysfunction in early hypercholesterolemia. The source of xanthine oxidase is not completely clear, but increased cholesterol levels have been shown to stimulate the release of the enzyme from the liver into the circulation. This circulating xanthine oxidase can then associate with endothelial glycosaminoglycans [147]. Unlike NADPH oxidases, the relative importance of xanthine oxidase for endothelial dysfunction is less certain. Recent experimental evidence has suggested that endothelial cells themselves can express xanthine dehydrogenase (and thus xanthine oxidase) and that this expression is regulated in a redox-sensitive way, dependent on the endothelial NADPH oxidase [84]. However clinical data relative to xanthine oxidase are controversial. Whereas some investigators reported an improvement of endothelial dysfunction in hypercholesterolemic and diabetic patients with xanthine oxidase inhibitors such as oxypurinol and allopurinol [14, 15], others failed to show an effect with allopurinol [97].
Respiratory chain of the mitochondria
About 1% of the O2 consumed by mitochondria is reduced by only a single electron thereby forming O −2 ·. O −2 · can be produced in at least two locations within the respiratory chain; in the NADH dehydrogenase (complex I) and in the ubiquinone–cytochrome b–c1 region (complex III) [129]. However, the actual amount of O −2 · released by the mitochondria also depends on the activity of Mn-containing superoxide dismutase2 (SOD2) located in the mitochondrial matrix (see below). There is evidence to suggest that some cardiovascular diseases are associated with mitochondrial dysfunction [106] and that mitochondrial production of ROS may be linked to the development of early atherosclerotic lesions [5]. Mitochondrial dysfunction, e.g., resulting from SOD2 deficiency, increases mitochondrial DNA (mtDNA) damage and accelerates atherosclerosis in apoE−/− mice [99]. However, a causal role of mitochondrial O −2 · for vascular disease in vivo remains to be established.
eNOS itself can be a source of superoxide
NOS enzymes contain four redox active prosthetic groups (FAD, FMN, heme, and BH4) that could—in principle—pass electrons to O2 [40, 82, 104, 150]. Thus, electron transfer in NOS enzymes needs to be tightly controlled to prevent uncoupling of O2 reduction from NO synthesis that will turn a functional NOS into a dysfunctional O −2 ·-generating enzyme [123].
Evidence for eNOS uncoupling has been obtained in peroxynitrite-treated rat aorta [69], in endothelial cells treated with low-density lipoprotein [105], and in isolated blood vessels from animals with pathophysiological conditions such as SHR [18], stroke-prone spontaneously hypertensive rats (SHRSP) [60], angiotensin II-induced hypertension [90], deoxycorticosterone acetate (DOCA)–salt hypertension [66], streptozotocin-induced diabetes [48], or nitroglycerin tolerance [43].
eNOS uncoupling has also been seen in patients with endothelial dysfunction due to hypercholesterolemia [121], diabetes mellitus [41] or essential hypertension [47], and in chronic smokers [43].
Antioxidant enzymes potentially protecting against vascular oxidative stress
Important antioxidant enzymes include superoxide dismutase (SOD), glutathione peroxidase (GPx), catalase, heme oxygenase (HO), and the thioredoxin (Trx) peroxidase (Fig. 3a, b) and perhaps also paraoxonases (PON).
Superoxide dismutase
SOD catalyzes the dismutation of O −2 · into oxygen and hydrogen peroxide, thereby serving a key antioxidant role (Fig. 3a). In humans, three forms of the enzyme are present. SOD1 (Cu–Zn–SOD) is located in the cytoplasm, SOD2 (Mn–SOD, see above) in the mitochondria, and SOD3 (Cu–Zn–SOD) is extracellular. In the cardiovascular system, the action of SOD3 lowers O −2 · and maintains vascular NO levels [59]. Mice with a deleted SOD1 gene develop normally and show no marked phenotype under normal conditions. However, they are more susceptible to myocardial ischemia–reperfusion injury [155]. A common gene variant of human SOD3, present in approximately 5% of humans, shows decreased SOD activity, oxidative stress, and accelerated NO inactivation. This variant is indeed associated with an increased risk of ischemic heart disease [55].
Catalase
The enzyme catalase catalyzes the decomposition of hydrogen peroxide to water and oxygen (Fig. 3a). The overall biological significance of catalase is not completely clear. Homozygous catalase knockout mice develop normally and show no gross abnormalities, indicating that this enzyme is dispensable for animal life [50]. Interestingly, overexpression of catalase has protective effects in the cardiovascular system such as delayed development of atherosclerosis [154] and inhibition of angiotensin II-induced aortic wall hypertrophy [161].
Glutathione peroxidase
GPx reduces free hydrogen peroxide to water and lipid hydroperoxides to their corresponding alcohols (Fig. 3a). There are several isozymes, and GPx1 is the most abundant version, found in the cytoplasm of many mammalian tissues. Mice genetically engineered to lack GPx1 are apparently healthy and fertile, but exhibit a pronounced susceptibility to myocardial ischemia–reperfusion injury [156]. In patients with coronary artery disease, the activity of red blood cell GPx1 is inversely associated with the risk of cardiovascular events [10]. In apoE-deficient mice, the deficiency of GPx1 accelerates and modifies atherosclerotic lesion progression [127]. GPx4 knockout mice are not viable; they die during early embryonic development.
Heme oxygenase
HO catalyzes the first step in heme breakdown to generate equimolar quantities of carbon monoxide, biliverdin, and free ferrous iron (Fig. 3b). There is ample evidence that HO1 can protect against vascular remodeling and atherogenesis [119]. HO1 is induced by oxidative stress, probably as an adaptive response. The proposed mechanisms by which HO1 may protect cells include its abilities to degrade the pro-oxidative heme to biliverdin. This gets subsequently converted to bilirubin, which has radical-scavenging properties. Moreover, bilirubin seems to directly inhibit fully functional NADPH oxidase and can also interrupt assembly and activation of the enzyme [57]. In addition, a decrease in heme content caused by HO1 limits heme availability for maturation of the Nox2 subunit of NADPH oxidase prevents assembly of a functional enzyme and reduces cellular ROS generation [126]. Carbon monoxide generated by HO has antiproliferative and anti-inflammatory as well as vasodilator properties [91]. The potential cytotoxic effects of iron (e.g., stimulation of the Fenton reaction; Fig. 3a) are limited by the simultaneous enhancement of intracellular ferritin [91]. Genetic models of HO1 deficiency or overexpression of HO1 suggest that the actions of HO1 are important in modulating the severity of atherosclerosis [51].
Thioredoxin
Also Trx has been recognized as critical protective system acting via direct (antioxidant) and indirect (regulation of signal transduction) effects [153]. Trx is present in endothelial cells and vascular smooth muscle. Trx seems to exert most of its ROS-scavenging properties through Trx peroxidase (peroxiredoxin), which uses endogenous SH groups as reducing equivalents (Fig. 3a). Trx reduces the oxidized form of Trx peroxidase and the reduced Trx peroxidase scavenges ROS (such as H2O2; Fig. 3a) and also ONOO− [153].
Paraoxonase
The PON family of enzymes (Fig. 3b) seems to contribute to vascular antioxidant defense and protect against coronary artery disease [3]. The PON1 and PON3 enzymes are synthesized in the liver and circulate in plasma associated with the high-density lipoprotein (HDL) fraction. The capacity of HDL in decreasing HDL and LDL lipid peroxidation largely depends on its PON1 content [3]. Deletion of the PON1 gene increases oxidative stress in mouse macrophages and aortae [110], and apoE−/− mice overexpressing PON1 developed fewer atherosclerotic lesions [130]. PON2 is expressed in many cell types. Polymorphisms of the PON2 gene have been reported to be associated with cardiovascular diseases [70]. The enzyme has been shown to reduce ROS in human endothelial cells, vascular smooth muscle cells, and fibroblasts [53]. The ROS species removed by PON2 is O −2 , not H2O2 (Horke and Förstermann, unpublished). PON2-deficient mice with an apoE−/− background developed more atherosclerotic lesions, whereas PON2-overexpressing mice were protected against those lesions [93].
Molecular mechanisms contributing to reduced levels of bioactive NO in vascular disease
Endothelial dysfunction is largely equivalent to the inability of the endothelium to generate adequate amounts of bioactive NO (and to produce NO-mediated vasodilation). Endothelial dysfunction has been shown for patients with all common types of cardiovascular risk factors. Several possible defects could account for reductions in bioactive NO. These include an increased depletion of NO due to its reaction with O −2 , a decreased NO production due to changes in the activity of eNOS (e.g., eNOS uncoupling), or a decreased NO production due to changes in the expression of the enzyme. Also, a depletion of the NOS substrate l-arginine, e.g., due to enhanced arginase activity, could contribute to endothelial dysfunction.
Oxidative stress produced by NADPH oxidase induces eNOS uncoupling
There is a growing body of evidence that vascular NADPH oxidase plays a crucial role in the phenomenon of eNOS uncoupling (Fig. 4a). An important hint came from experiments with NADPH oxidase (p47phox) knockout animals [66]. When hypertension was induced in normal mice with a combination of the mineralocorticoid DOCA and salt, these animals showed an increased production of vascular ROS. This was significantly reduced by the NOS inhibitor l-NAME, demonstrating a marked contribution of uncoupled eNOS to oxidative stress in vascular tissue. p47phox knockout animals showed much less oxidative stress upon DOCA–salt treatment, and levels of ROS could no longer be reduced with l-NAME [66]. These findings demonstrate that NADPH oxidase-derived ROS can indeed represent the trigger leading to eNOS uncoupling and that uncoupled eNOS significantly contributes to oxidative stress [66]. The detailed mechanism of how NADPH oxidase-derived ROS can trigger eNOS uncoupling is described below (Fig. 4a).

a Potential mechanisms by which risk factors for atherosclerosis and various cardiovascular diseases lead to eNOS uncoupling and endothelial dysfunction. In many types of vascular disease, NADPH oxidases are upregulated in the vascular wall and generate superoxide (O −2 ·). In experimental diabetes mellitus and angiotensin II-induced hypertension, this has been shown to be mediated by protein kinase C (PKC) [48, 90]. Expression of eNOS is also increased in vascular disease. H2O2, the dismutation product of O −2 ·, can increase eNOS expression via transcriptional and post-transcriptional mechanisms (SOD superoxide dismutase) [23]. In addition, also PKC activation can enhance eNOS expression [74], and PKC inhibitors reduce eNOS expression levels in vascular disease [48]. The products of NADPH oxidases and eNOS, O −2 · and NO, rapidly recombine to form peroxynitrite (ONOO−). This can oxidize the essential cofactor of eNOS (6R-)5,6,7,8-tetrahydrobiopterin (BH4) to trihydrobiopterin radical (BH3.) [7, 33]. BH3. can disproportionate to the quinonoid 6,7-[8H]-H2-biopterin (BH2). As a consequence, oxygen reduction and O2 reduction by eNOS are uncoupled from NO formation, and a functional NOS is converted into a dysfunctional O −2 ·-generating enzyme that contributes to vascular oxidative stress. The enhanced eNOS expression (see above) aggravates the situation. Under oxidative stress, concentrations of asymmetric dimethyl-l-arginine (ADMA) increase in cells because arginine N-methyltransferase (PRMT, type I) is upregulated [11], and the ADMA-degrading enzyme dimethylarginine dimethylaminohydrolase (DDAH) is downregulated [78]. ADMA in turn may contribute to eNOS uncoupling [124]. b Scheme of an endothelial NO synthase (eNOS) whose oxygen reduction is uncoupled from NO synthesis. Oxidative stress is associated with endothelial dysfunction. ONOO− can oxidize BH4 to biologically inactive products such as trihydrobiopterin radical (BH3·) or trihydropterin radical cation protonated at N5 (BH3·H+). The BH3· radical can be converted to the quinonoid 6,7-[8H]-H2-biopterin (BH2), which also lacks biological activity. When ONOO− overwhelms the cell’s capacity to re-reduce these products to BH4, eNOS “uncouples” and reduces oxygen to O −2 ·, but does not synthesize NO anymore. eNOS then contributes to oxidative stress in the cell
Molecular mechanisms triggering eNOS uncoupling
Oxidation of BH4 is likely to represent a major mechanism for eNOS uncoupling
NO and l-citrulline production by eNOS in endothelial cells correlates closely with the intracellular concentration of BH4 [108, 146]. In isolated arteries [17] or rats in vivo [152], a BH4 depletion produced endothelial dysfunction. Conversely, supplementation with BH4 is capable of correcting eNOS dysfunction in several types of pathophysiology: In isolated aortas from prehypertensive SHR, BH4 supplementation diminished the NOS-dependent generation of O −2 · [18]. Administration of BH4 restored endothelial function in animal models of diabetes [102] and insulin resistance [113], as well as in patients with hypercholesterolemia [121], diabetes mellitus [41], essential hypertension [47], and in chronic smokers [43].
Intracellular BH4 levels depend on the balance of its de novo synthesis and its degradation or oxidation. BH4 is one of the most potent naturally occurring reducing agents. It is therefore reasonable to hypothesize that oxidative stress may lead to excessive oxidation and depletion of BH4 [69, 87]. As oxidative stress occurs in cardiovascular pathophysiology (see above), oxidation of BH4 may be the common cause of eNOS dysfunction in these situations. In agreement with this concept, BH4 levels have been found decreased in the aorta from insulin-resistant rats [112], in plasma of SHR compared with age-matched WKY rats [52], in aorta of hypercholesterolemic–apoE-knockout mice [69] and in DOCA–salt-treated hypertensive rats [66]. Conversely, an infusion of the eNOS cofactor BH4 can restore eNOS functionality as demonstrated by studies in chronic smokers [43], diabetics [41], hypercholesterolemic patients [121], and hypertensive individuals [47].
ONOO−—the direct reaction product of NO. and O −2 —is able to oxidize BH4 (Fig. 4b). Published data show that ONOO− oxidizes BH4 to the BH3· radical, which is re-reduced to BH4 by NOS itself or when enough reducing equivalents such as vitamin C are available [63, 145] (Fig. 1). BH3. radical can also disproportionate to the quinonoid 6,7-[8H]-H2-biopterin, which again can be reduced by vitamin C back to BH4 [44, 145]. The exact mechanism of action of l-ascorbic acid is unknown, but as detailed below, the improvement of endothelial dysfunction by vitamin C may be due to enhanced regeneration of BH4 rather than the scavenging of O −2 · (see Fig. 1).
Potential role of l-arginine levels for eNOS uncoupling
Beneficial effects of l-arginine supplementation have been documented in both animal studies and humans under pathophysiological conditions such as hypercholesterolemia and hypertension [22, 49, 56, 109]. This raises the question as to whether l-arginine concentrations can become critical as a substrate in vivo. At first glance, this appears unlikely. The K m of eNOS for l-arginine is ∼3 μmol/L [103], normal l-arginine plasma concentrations are ∼100 μmol/L (even in pathophysiology they hardly fall below 60 μmol/L), and there is an up to 10-fold accumulation of l-arginine within cells [16]. In addition, human endothelial cells are not even dependent on l-arginine uptake from the extracellular space; they can effectively recycle l-citrulline to l-arginine and can also obtain l-arginine from proteolysis [38, 114].
Endothelial cells, however, also express arginases that can compete with eNOS for substrate and—if highly expressed—“starve” eNOS. In porcine coronary and rat aortic endothelial cells, arginase I is constitutively expressed [13, 159], whereas arginase II can be induced by lipopolysaccharide [13]. In human endothelial cells, arginase II seems to be the predominant isozyme [4, 88]. An upregulated expression and activity of arginase II has been found in human diabetic corpus cavernosum [9] and in endothelium from patients with pulmonary hypertension [151]. Evidence for a role of increased enzymatic activity of arginase in endothelial dysfunction has also been provided in animal models of cardiovascular disease such as aging [8], atherosclerosis [88], endothelial dysfunction following ischemia–reperfusion [39], and hypertension induced by aortic coarctation or high salt [58, 160]. In apoE-knockout mice, the expression of arginase II was unchanged compared with wild-type mice, but the activity of the enzyme was markedly increased [88]. Similarly, in human umbilical vein endothelial cells, arginase II enzymatic activity, but not protein expression, was enhanced after an 18- to 24-h exposure to thrombin [88] or a 24-h stimulation with inflammatory cytokines [4].
Thus, a relative l-arginine deficiency in the vicinity of eNOS caused by excessive arginase activity is conceivable and could explain part of the beneficial effects of l-arginine supplementation. However, also non-substrate effects of l-arginine could contribute to these effects. These include potential direct radical-scavenging properties of the guanidino nitrogen group, the cooperativity between l-arginine and BH4 binding sites of NOS [34, 81] (see Fig. 1), or the competition of l-arginine with the derivative asymmetric dimethyl-l-arginine (ADMA), which is an endogenous inhibitor of eNOS activity [125].
Contribution of ADMA to eNOS uncoupling?
ADMA represents an independent predictor for all-cause cardiovascular mortality. The activities (not the expression) of both protein arginine N-methyltransferase (PRMT), type I [11], and of the ADMA-degrading enzyme dimethylarginine dimethylaminohydrolase (DDAH) [78] are redox sensitive (Fig. 4a). In cultured endothelial cells, rat models and man, oxidative stress has been shown to increase the activity of PRMT(s) and decrease that of DDAH, thereby leading to increased ADMA concentrations [11, 78, 125]. Thus, an increased production of ROS could be the reason for increased ADMA levels. Elevated ADMA inhibits NO synthesis by eNOS or could even uncouple the enzyme [125] (Fig. 4). However, it remains to be established whether ADMA concentrations reached in vivo (even in pathophysiology) are sufficient to effectively interact with eNOS.
A reduced eNOS expression is unlikely to contribute to endothelial dysfunction
Several studies have shown that cardiovascular risk factors are associated with an increase rather than a decrease in eNOS expression [37, 48, 69, 72, 76, 90, 132]. The increased expression of eNOS in vascular disease is likely to be a consequence of an increased production of the ROS H2O2, the dismutation product of O −2 ·. H2O2. can increase eNOS expression through transcriptional and post-transcriptional mechanisms [23] (see Fig. 4a).
Vascular oxidative stress and endothelial dysfunction predispose to atherosclerosis
Most risk factors favoring the development of atherosclerosis (such as hypertension, hypercholesterolemia, diabetes, cigarette smoking, or a positive family history of premature coronary artery disease) are associated with vascular oxidative stress and endothelial dysfunction [137]. Pathophysiological mechanisms are probably best established for hypertension. Angiotensin II—through stimulation of AT1 receptors—leads to an upregulation and activation of NADPH oxidases in the vascular wall resulting in oxidative stress [90, 94, 158]. Angiotensin II can increase NADPH oxidase activity by inducing a rapid translocation of the small GTPase rac1 to the cell membrane [143] or by phosphorylation and translocation of the NADPH oxidase subunit p47phox to the membrane [128]. Also, mechanical stretch, characteristic of hypertension, can induce p47phox membrane translocation and NADPH oxidase activation [36]; stretch-induced NADPH oxidase activation was absent in p47phox-deficient cells. A critical role for oxidative stress has been demonstrated in hypertensive rats. Treatment of these rats with statins decreased O −2 · production and reduced blood pressure [144].
Endothelial dysfunction is already found in the preclinical stage of atherosclerosis and can be detected much earlier than angiographic or ultrasound evidence of structural coronary artery disease. In fact, coronary endothelial vasodilator dysfunction has been described as an independent predictor of the progression of atherosclerosis and the risk of cardiovascular events [111]. Interestingly, patients with impaired endothelium-dependent vasodilation in a peripheral vascular bed (the human forearm) have a higher risk for cardiovascular events over a follow-up period of 4.5 years [42].
However, it ought to be mentioned that hard evidence that oxidative stress is both necessary and sufficient for atherosclerosis has been difficult to find. Only if tools become available that limit oxidative stress at its source (and ameliorate its secondary phenomena) will we be able to finally decide what components of atherosclerosis are directly caused by oxidative stress.
Pharmacological approaches to reduce oxidative stress and prevent or reverse eNOS uncoupling
Angiotensin-converting enzyme inhibitors and AT1 receptor antagonists
Angiotensin II activates NADPH oxidases via AT1 receptor stimulation [35]. In addition, the AT1 receptor is upregulated in vitro by LDL [142]. Therefore, ACE inhibitors and AT1 receptor antagonists may have indirect antioxidant effects by preventing the activation of NADPH oxidase [61, 142] and/or increasing the activity of SOD3 [54]. Indeed, there is clinical evidence for a beneficial effect of inhibition of the renin–angiotensin system. ACE inhibitors improve endothelial function in patients with coronary artery disease and in hypertensive patients. Further, the Heart Outcome Prevention Evaluation (HOPE) trial [157] showed that treatment with ramipril greatly reduced the incidence of death, myocardial infarction, and stroke in high risk patients without heart failure. Also, the European Trial on Reduction of Cardiac Events with Perindopril in Stable Coronary Artery Disease (EUROPA) [29] demonstrated a 20% reduction with perindopril of the relative risk for cardiovascular endpoints in a patient population with stable coronary heart disease. In contrast, the Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) trial [12] could not show that patients with stable coronary artery disease and largely intact ventricular function have a therapeutic benefit from the addition of ACE inhibitors to modern conventional therapy. The failure of ACE inhibitors to reduce the cardiovascular events in this trial may have been attributable to the low overall event rate of hard endpoints, such as myocardial infarction or death in this patient population.
Statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors)
Much of the clinical benefit obtained with statins is clearly related to their cholesterol-lowering properties, but effects unrelated to this effect seem to be beneficial on various aspects of cardiovascular disease [77]. Statins can inhibit endothelial O −2 · formation by preventing the isoprenylation of p21 Rac, which is critical for the assembly of NADPH oxidase after activation of PKC [138]. In addition, SOD3 activity was more than doubled by simvastatin, and simvastatin treatment also increased the number of functionally active endothelial progenitor cells [67]. Finally, statins increase the expression of eNOS by inhibition of Rho isoprenylation [68], and statins can also directly activate eNOS via post-translational mechanisms involving activation of the phosphatidylinositol 3-kinase/protein kinase Akt pathway [62]. Taken together, statin treatment improves endothelial function at least in part by reducing oxidant stress and improving eNOS function.
Folic acid and 5-methyltetrahydrofolate
Folic acid and its active form 5-methyltetrahydrofolate have been used successfully to restore endothelial function in patients with hypercholesterolemia [135], diabetes mellitus [131], or hyperhomocysteinemia [149] and in healthy volunteers with postprandial endothelial dysfunction [148].
In cultured endothelial cells and with recombinant eNOS enzyme, 5-methyltetrahydrofolate, NO synthesis was enhanced and O −2 · production was reduced [122]. This provides a reasonable explanation for the clinical reports of positive effects of 5-methyltetrahydrofolate on endothelial function in vivo. The molecular mechanism by which folate or 5-methyltetrahydrofolate increase eNOS activity is not completely clear. It has been reported that folic acid reverses endothelial dysfunction by direct effects on the eNOS enzyme and independently of either the regeneration or stabilization of BH4 [89, 122], whereas others have postulated that folates possess antioxidant properties and may recouple eNOS by BH4 stabilization or BH4 regeneration from quinonoid BH2 [134].
Polyphenolic antioxidants
Dietary polyphenolic antioxidants are likely to assist in preventing ROS damage. Epidemiological evidence suggests a negative correlation between the consumption of polyphenol-rich foods (fruits, vegetables, and cocoa contained in chocolate) or beverages (wine, especially red wine, grape juice, green tea, etc.) and the incidence of cardiovascular disease [2, 80, 120, 136]. Most polyphenols are only mild antioxidants, but some can reduce the activity of pro-oxidative NADPH oxidases, and others can stimulate anti-oxidative enzymes and eNOS [71, 117, 118, 139–141]. Current evidence suggests that small molecular weight compounds with indirect mechanisms of action, such as some dietary antioxidants, may offer more long-term benefit than directly acting radical scavengers or antioxidant vitamins (see below).
(6R-)5,6,7,8-tetrahydrobiopterin (BH4)
Acute intraarterial infusion of the eNOS cofactor BH4 can restore eNOS functionality (i.e., “recouple” eNOS) in clinical situations as demonstrated by studies in chronic smokers [43], diabetics [41], hypercholesterolemic [121], and hypertensive [47] patients. Also, in coronary arteries of patients with hypercholesterolemia, BH4 restored endothelial function [30]. However, the need for parenteral administration, the short half-life, and the high cost of BH4 restrict its therapeutic use.
Vitamin C
In cultured endothelial cells, ascorbic acid (vitamin C) increased eNOS enzyme activity via regeneration of BH4. Long-term in vivo treatment with vitamin C restored endothelial function and endothelial NOS activity in aortae of apoE-deficient mice. Also, in patients, acute infusions of high doses of vitamin C have been found to improve endothelial function [42, 64]. Some studies in patients also demonstrated improvements of endothelial function/endothelial NO production [32] or reduced levels of ROS in the vascular wall [24] after longer-term oral treatment with vitamin C. The exact mechanism of action of l-ascorbic acid in improving endothelial dysfunction is not clear, but the most important mechanism may be the enhanced regeneration or stabilization of BH4 and eNOS “recoupling” rather than the scavenging of O −2 · (Fig. 1). Disappointingly, however, long-term epidemiological trials with oral vitamin C have been ambiguous at best and do not support an important role for vitamin C in reducing the risk of coronary disease or other types of cardiovascular morbidity or mortality [101].
Vitamin E
Because of its antioxidant properties, also vitamin E has been believed to help prevent diseases associated with oxidative stress. However, large-scale randomized clinical trials undertaken to prove this hypothesis failed to verify a consistent benefit in terms of prevention of coronary heart disease and death [116]. In fact, there is enough evidence from large, well-designed studies to discourage the use of vitamin E in primary prevention of cardiovascular disease [79].
Conclusions
Endothelial dysfunction and oxidative stress has been identified as a common denominator of many cardiovascular risk factors. They support pro-inflammatory, prothrombotic, proliferative, and vasoconstrictor mechanisms that are involved in the initiation, progression, and complications of atherosclerosis. Diagnostically, a deficiency in bioactive NO in coronary or peripheral arteries appears to be predictive of future cardiovascular events. The pathophysiologic causes of oxidative stress are likely to involve changes in a number of different enzyme systems; most importantly, there is an upregulation of NADPH oxidases and eNOS (Fig. 5). Together, they lead to an increased production of ONOO−. This conveys oxidative damage to eNOS and/or its cofactor BH4 leading to “uncoupling” of the enzyme (Figs. 4 and 5). As a consequence, an increased production of ROS by uncoupled eNOS is likely to contribute significantly to vascular oxidative stress and endothelial dysfunction (Fig. 4).

Scheme viewing vascular oxidative stress as a cause of atherogenesis. Cardiovascular risk factors activate ROS-producing enzyme systems and/or weaken ROS-detoxifying systems. Many of the underlying mechanisms are still unclear. The resulting oxidative stress promotes atherogenesis through a number of different mechanisms, including the activation of redox-sensitive transcription factors (which stimulate the expression of pro-inflammatory genes) and the activation of signaling cascades (activation of kinases, inhibition of phosphatases). Elevated levels of ROS can also stimulate mitochondrial and nuclear DNA damage (and activate reactive DNA repair systems). Enhanced DNA damage is found associated with various types of vascular disease and may be involved in atherogenesis. However, despite important evidence in favor of the above hypothesis, the possibility remains that inflammation is the primary process of atherogenesis and oxidative stress the detrimental secondary response. The dashed blue arrows indicate this possibility
Therapeutically, cardiovascular drugs in clinical use such as ACE inhibitors, AT1 receptor blockers, and statins have pleiotropic actions that improve endothelial function. In addition, dietary polyphenolic antioxidants may prevent or reverse eNOS uncoupling and restore its normal function. Such compounds either block pathways leading to oxidative stress and/or upregulate antioxidant enzymes. Despite promising initial observations, clinical trials with antioxidant vitamins C and E failed to show an improved cardiovascular outcome.
References
Alderton WK, Cooper CE, Knowles RG (2001) Nitric oxide synthases: structure, function and inhibition. Biochem J 357:593–615
Arts IC, Hollman PC (2005) Polyphenols and disease risk in epidemiologic studies. Am J Clin Nutr 81:317S–325S
Aviram M, Rosenblat M, Bisgaier CL, Newton RS, Primo-Parmo SL, La Du BN (1998) Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J Clin Invest 101:1581–1590
Bachetti T, Comini L, Francolini G, Bastianon D, Valetti B, Cadei M, Grigolato P, Suzuki H, Finazzi D, Albertini A, Curello S, Ferrari R (2004) Arginase pathway in human endothelial cells in pathophysiological conditions. J Mol Cell Cardiol 37:515–523
Ballinger SW, Patterson C, Knight-Lozano CA, Burow DL, Conklin CA, Hu Z, Reuf J, Horaist C, Lebovitz R, Hunter GC, McIntyre K, Runge MS (2002) Mitochondrial integrity and function in atherogenesis. Circulation 106:544–549
Barry-Lane PA, Patterson C, van der Merwe M, Hu Z, Holland SM, Yeh ET, Runge MS (2001) p47phox is required for atherosclerotic lesion progression in ApoE(−/−) mice. J Clin Invest 108:1513–1522
Bec N, Gorren AFC, Mayer B, Schmidt PP, Andersson KK, Lange R (2000) The role of tetrahydrobiopterin in the activation of oxygen by nitric-oxide synthase. J Inorg Biochem 81:207–211
Berkowitz DE, White R, Li D, Minhas KM, Cernetich A, Kim S, Burke S, Shoukas AA, Nyhan D, Champion HC, Hare JM (2003) Arginase reciprocally regulates nitric oxide synthase activity and contributes to endothelial dysfunction in aging blood vessels. Circulation 108:2000–2006
Bivalacqua TJ, Hellstrom WJ, Kadowitz PJ, Champion HC (2001) Increased expression of arginase II in human diabetic corpus cavernosum: in diabetic-associated erectile dysfunction. Biochem Biophys Res Commun 283:923–927
Blankenberg S, Rupprecht HJ, Bickel C, Torzewski M, Hafner G, Tiret L, Smieja M, Cambien F, Meyer J, Lackner KJ (2003) Glutathione peroxidase 1 activity and cardiovascular events in patients with coronary artery disease. N Engl J Med 349:1605–1613
Boger RH, Sydow K, Borlak J, Thum T, Lenzen H, Schubert B, Tsikas D, Bode-Boger SM (2000) LDL cholesterol upregulates synthesis of asymmetrical dimethylarginine in human endothelial cells: involvement of S-adenosylmethionine-dependent methyltransferases. Circ Res 87:99–105
Braunwald E, Domanski MJ, Fowler SE, Geller NL, Gersh BJ, Hsia J, Pfeffer MA, Rice MM, Rosenberg YD, Rouleau JL (2004) Angiotensin-converting-enzyme inhibition in stable coronary artery disease. N Engl J Med 351:2058–2068
Buga GM, Singh R, Pervin S, Rogers NE, Schmitz DA, Jenkinson CP, Cederbaum SD, Ignarro LJ (1996) Arginase activity in endothelial cells: inhibition by NG-hydroxy-l-arginine during high-output NO production. Am J Physiol 271:H1988–H1998
Butler R, Morris AD, Belch JJ, Hill A, Struthers AD (2000) Allopurinol normalizes endothelial dysfunction in type 2 diabetics with mild hypertension. Hypertension 35:746–751
Cardillo C, Kilcoyne CM, Cannon RO 3rd, Quyyumi AA, Panza JA (1997) Xanthine oxidase inhibition with oxypurinol improves endothelial vasodilator function in hypercholesterolemic but not in hypertensive patients. Hypertension 30:57–63
Closs EI, Scheld JS, Sharafi M, Forstermann U (2000) Substrate supply for nitric-oxide synthase in macrophages and endothelial cells: role of cationic amino acid transporters. Mol Pharmacol 57:68–74
Cosentino F, Katusic ZS (1995) Tetrahydrobiopterin and dysfunction of endothelial nitric oxide synthase in coronary arteries. Circulation 91:139–144
Cosentino F, Luscher TF (1998) Tetrahydrobiopterin and endothelial function. Eur Heart J 19(Suppl G):G3–G8
Crane BR, Arvai AS, Ghosh DK, Wu C, Getzoff ED, Stuehr DJ, Tainer JA (1998) Structure of nitric oxide synthase oxygenase dimer with pterin and substrate. Science 279:2121–2126
Diet F, Pratt RE, Berry GJ, Momose N, Gibbons GH, Dzau VJ (1996) Increased accumulation of tissue ACE in human atherosclerotic coronary artery disease. Circulation 94:2756–2767
Dikalova A, Clempus R, Lassegue B, Cheng G, McCoy J, Dikalov S, San Martin A, Lyle A, Weber DS, Weiss D, Taylor WR, Schmidt HH, Owens GK, Lambeth JD, Griendling KK (2005) Nox1 overexpression potentiates angiotensin II-induced hypertension and vascular smooth muscle hypertrophy in transgenic mice. Circulation 112:2668–2676
Drexler H, Zeiher AM, Meinzer K, Just H (1991) Correction of endothelial dysfunction in coronary microcirculation of hypercholesterolaemic patients by l-arginine. Lancet 338:1546–1550
Drummond GR, Cai H, Davis ME, Ramasamy S, Harrison DG (2000) Transcriptional and posttranscriptional regulation of endothelial nitric oxide synthase expression by hydrogen peroxide. Circ Res 86:347–354
Ellis GR, Anderson RA, Lang D, Blackman DJ, Morris RH, Morris-Thurgood J, McDowell IF, Jackson SK, Lewis MJ, Frenneaux MP (2000) Neutrophil superoxide anion-generating capacity, endothelial function and oxidative stress in chronic heart failure: effects of short- and long-term vitamin C therapy. J Am Coll Cardiol 36:1474–1482
Fleming I, Busse R (2003) Molecular mechanisms involved in the regulation of the endothelial nitric oxide synthase. Am J Physiol Regul Integr Comp Physiol 284:R1–R12
Förstermann U (2008) Oxidative stress in vascular disease: causes, defense mechanisms and potential therapies. Nat Clin Pract Cardiovasc Med 5:338–349
Förstermann U, Münzel T (2006) Endothelial nitric oxide synthase in vascular disease: from marvel to menace. Circulation 113:1708–1714
Förstermann U, Nakane M, Tracey WR, Pollock JS (1993) Isoforms of nitric oxide synthase: functions in the cardiovascular system. Eur Heart J 14(Suppl I):10–15
Fox KM (2003) Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet 362:782–788
Fukuda Y, Teragawa H, Matsuda K, Yamagata T, Matsuura H, Chayama K (2002) Tetrahydrobiopterin restores endothelial function of coronary arteries in patients with hypercholesterolaemia. Heart 87:264–269
Fukui T, Ishizaka N, Rajagopalan S, Laursen JB, Qt C, Taylor WR, Harrison DG, de Leon H, Wilcox JN, Griendling KK (1997) p22phox mRNA expression and NADPH oxidase activity are increased in aortas from hypertensive rats. Circ Res 80:45–51
Gokce N, Keaney JF Jr, Frei B, Holbrook M, Olesiak M, Zachariah BJ, Leeuwenburgh C, Heinecke JW, Vita JA (1999) Long-term ascorbic acid administration reverses endothelial vasomotor dysfunction in patients with coronary artery disease. Circulation 99:3234–3240
Gorren AC, Kungl AJ, Schmidt K, Werner ER, Mayer B (2001) Electrochemistry of pterin cofactors and inhibitors of nitric oxide synthase. Nitric Oxide 5:176–186
Gorren AC, List BM, Schrammel A, Pitters E, Hemmens B, Werner ER, Schmidt K, Mayer B (1996) Tetrahydrobiopterin-free neuronal nitric oxide synthase: evidence for two identical highly anticooperative pteridine binding sites. Biochemistry 35:16735–16745
Griendling KK, Sorescu D, Ushio-Fukai M (2000) NAD(P)H oxidase: role in cardiovascular biology and disease. Circ Res 86:494–501
Grote K, Flach I, Luchtefeld M, Akin E, Holland SM, Drexler H, Schieffer B (2003) Mechanical stretch enhances mRNA expression and proenzyme release of matrix metalloproteinase-2 (MMP-2) via NAD(P)H oxidase-derived reactive oxygen species. Circ Res 92:e80–e86
Guzik TJ, Mussa S, Gastaldi D, Sadowski J, Ratnatunga C, Pillai R, Channon KM (2002) Mechanisms of increased vascular superoxide production in human diabetes mellitus: role of NAD(P)H oxidase and endothelial nitric oxide synthase. Circulation 105:1656–1662
Hecker M, Sessa WC, Harris HJ, Anggard EE, Vane JR (1990) The metabolism of l-arginine and its significance for the biosynthesis of endothelium-derived relaxing factor: cultured endothelial cells recycle l-citrulline to l-arginine. Proc Natl Acad Sci U S A 87:8612–8616
Hein TW, Zhang C, Wang W, Chang CI, Thengchaisri N, Kuo L (2003) Ischemia–reperfusion selectively impairs nitric oxide-mediated dilation in coronary arterioles: counteracting role of arginase. FASEB J 17:2328–2330
Heinzel B, John M, Klatt P, Bohme E, Mayer B (1992) Ca2+/calmodulin-dependent formation of hydrogen peroxide by brain nitric oxide synthase. Biochem J 281(Pt 3):627–630
Heitzer T, Krohn K, Albers S, Meinertz T (2000) Tetrahydrobiopterin improves endothelium-dependent vasodilation by increasing nitric oxide activity in patients with type II diabetes mellitus. Diabetologia 43:1435–1438
Heitzer T, Schlinzig T, Krohn K, Meinertz T, Munzel T (2001) Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation 104:2673–2678
Heitzer T, Brockhoff C, Mayer B, Warnholtz A, Mollnau H, Henne S, Meinertz T, Munzel T (2000) Tetrahydrobiopterin improves endothelium-dependent vasodilation in chronic smokers: evidence for a dysfunctional nitric oxide synthase. Circ Res 86:E36–E41
Heller R, Werner-Felmayer G, Werner ER (2006) Antioxidants and endothelial nitric oxide synthesis. Eur J Clin Pharmacol 62(Suppl 13):21–28
Hemmens B, Mayer B (1998) Enzymology of nitric oxide synthases. Methods Mol Biol 100:1–32
Hemmens B, Goessler W, Schmidt K, Mayer B (2000) Role of bound zinc in dimer stabilization but not enzyme activity of neuronal nitric-oxide synthase. J Biol Chem 275:35786–35791
Higashi Y, Sasaki S, Nakagawa K, Fukuda Y, Matsuura H, Oshima T, Chayama K (2002) Tetrahydrobiopterin enhances forearm vascular response to acetylcholine in both normotensive and hypertensive individuals. Am J Hypertens 15:326–332
Hink U, Li H, Mollnau H, Oelze M, Matheis E, Hartmann M, Skatchkov M, Thaiss F, Stahl RA, Warnholtz A, Meinertz T, Griendling K, Harrison DG, Forstermann U, Munzel T (2001) Mechanisms underlying endothelial dysfunction in diabetes mellitus. Circ Res 88:E14–E22
Hishikawa K, Nakaki T, Suzuki H, Kato R, Saruta T (1993) Role of l-arginine nitric oxide pathway in hypertension. J Hypertension 11:639–645
Ho YS, Xiong Y, Ma W, Spector A, Ho DS (2004) Mice lacking catalase develop normally but show differential sensitivity to oxidant tissue injury. J Biol Chem 279:32804–32812
Hoekstra KA, Godin DV, Cheng KM (2004) Protective role of heme oxygenase in the blood vessel wall during atherogenesis. Biochem Cell Biol 82:351–359
Hong H-J, Hsiao G, Cheng T-H, Yen M-H (2001) Supplementation with tetrahydrobiopterin suppresses the development of hypertension in spontaneously hypertensive rats. Hypertension 38:1044–1048
Horke S, Witte I, Wilgenbus P, Kruger M, Strand D, Forstermann U (2007) Paraoxonase-2 reduces oxidative stress in vascular cells and decreases endoplasmic reticulum stress-induced caspase activation. Circulation 115:2055–2064
Hornig B, Landmesser U, Kohler C, Ahlersmann D, Spiekermann S, Christoph A, Tatge H, Drexler H (2001) Comparative effect of ace inhibition and angiotensin II type 1 receptor antagonism on bioavailability of nitric oxide in patients with coronary artery disease: role of superoxide dismutase. Circulation 103:799–805
Iida S, Chu Y, Weiss RM, Kang YM, Faraci FM, Heistad DD (2006) Vascular effects of a common gene variant of extracellular superoxide dismutase in heart failure. Am J Physiol Heart Circ Physiol 291:H914–H920
Imaizumi T, Hirooka Y, Masaki H, Harada S, Momohara M, Tagawa T, Takeshita A (1992) Effects of l-arginine on forearm vessels and responses to acetylcholine. Hypertension 20:511–517
Jiang F, Roberts SJ, Datla S, Dusting GJ (2006) NO modulates NADPH oxidase function via heme oxygenase-1 in human endothelial cells. Hypertension 48:950–957
Johnson FK, Johnson RA, Peyton KJ, Durante W (2005) Arginase inhibition restores arteriolar endothelial function in Dahl rats with salt-induced hypertension. Am J Physiol Regul Integr Comp Physiol 288:R1057–R1062
Jung O, Marklund SL, Xia N, Busse R, Brandes RP (2007) Inactivation of extracellular superoxide dismutase contributes to the development of high-volume hypertension. Arterioscler Thromb Vasc Biol 27:470–477
Kerr S, Brosnan MJ, McIntyre M, Reid JL, Dominiczak AF, Hamilton CA (1999) Superoxide anion production is increased in a model of genetic hypertension: role of the endothelium. Hypertension 33:1353–1358
Klingbeil AU, John S, Schneider MP, Jacobi J, Handrock R, Schmieder RE (2003) Effect of AT1 receptor blockade on endothelial function in essential hypertension. Am J Hypertens 16:123–128
Kureishi Y, Luo Z, Shiojima I, Bialik A, Fulton D, Lefer DJ, Sessa WC, Walsh K (2000) The HMG-CoA reductase inhibitor simvastatin activates the protein kinase Akt and promotes angiogenesis in normocholesterolemic animals. Nat Med 6:1004–1010
Kuzkaya N, Weissmann N, Harrison DG, Dikalov S (2003) Interactions of peroxynitrite, tetrahydrobiopterin, ascorbic acid, and thiols: implications for uncoupling endothelial nitric-oxide synthase. J Biol Chem 278:22546–22554
Landmesser U, Merten R, Spiekermann S, Buttner K, Drexler H, Hornig B (2000) Vascular extracellular superoxide dismutase activity in patients with coronary artery disease: relation to endothelium-dependent vasodilation. Circulation 101:2264–2270
Landmesser U, Cai H, Dikalov S, McCann L, Hwang J, Jo H, Holland SM, Harrison DG (2002) Role of p47(phox) in vascular oxidative stress and hypertension caused by angiotensin II. Hypertension 40:511–515
Landmesser U, Dikalov S, Price SR, McCann L, Fukai T, Holland SM, Mitch WE, Harrison DG (2003) Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J Clin Invest 111:1201–1209
Landmesser U, Bahlmann F, Mueller M, Spiekermann S, Kirchhoff N, Schulz S, Manes C, Fischer D, de Groot K, Fliser D, Fauler G, Marz W, Drexler H (2005) Simvastatin versus ezetimibe: pleiotropic and lipid-lowering effects on endothelial function in humans. Circulation 111:2356–2363
Laufs U, La Fata V, Plutzky J, Liao JK (1998) Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation 97:1129–1135
Laursen JB, Somers M, Kurz S, McCann L, Warnholtz A, Freeman BA, Tarpey M, Fukai T, Harrison DG (2001) Endothelial regulation of vasomotion in apoE-deficient mice: implications for interactions between peroxynitrite and tetrahydrobiopterin. Circulation 103:1282–1288
Leus FR, Zwart M, Kastelein JJ, Voorbij HA (2001) PON2 gene variants are associated with clinical manifestations of cardiovascular disease in familial hypercholesterolemia patients. Atherosclerosis 154:641–649
Li H, Forstermann U (2009) Resveratrol: a multifunctional compound improving endothelial function. Editorial to: “Resveratrol supplementation gender independently improves endothelial reactivity and suppresses superoxide production in healthy rats” by S. Soylemez et al. Cardiovasc Drugs Ther 23:425–429
Li H, Wallerath T, Munzel T, Forstermann U (2002) Regulation of endothelial-type NO synthase expression in pathophysiology and in response to drugs. Nitric Oxide 7:149–164
Li H, Raman CS, Glaser CB, Blasko E, Young TA, Parkinson JF, Whitlow M, Poulos TL (1999) Crystal structures of zinc-free and -bound heme domain of human inducible nitric-oxide synthase. Implications for dimer stability and comparison with endothelial nitric-oxide synthase. J Biol Chem 274:21276–21284
Li H, Oehrlein SA, Wallerath T, Ihrig-Biedert I, Wohlfart P, Ulshofer T, Jessen T, Herget T, Forstermann U, Kleinert H (1998) Activation of protein kinase C alpha and/or epsilon enhances transcription of the human endothelial nitric oxide synthase gene. Mol Pharmacol 53:630–637
Li H, Witte K, August M, Brausch I, Godtel-Armbrust U, Habermeier A, Closs EI, Oelze M, Munzel T, Forstermann U (2006) Reversal of endothelial nitric oxide synthase uncoupling and up-regulation of endothelial nitric oxide synthase expression lowers blood pressure in hypertensive rats. J Am Coll Cardiol 47:2536–2544
Li H, Witte K, August M, Brausch I, Gödtel-Armbrust U, Habermeier A, Closs EI, Oelze M, Münzel T, Förstermann U (2006) Reversal of eNOS uncoupling and upregulation of eNOS expression lowers blood pressure in hypertensive rats. J Amer Coll Cardiol 47:2536–2544
Liao JK (2002) Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol 86:5–18
Lin KY, Ito A, Asagami T, Tsao PS, Adimoolam S, Kimoto M, Tsuji H, Reaven GM, Cooke JP (2002) Impaired nitric oxide synthase pathway in diabetes mellitus: role of asymmetric dimethylarginine and dimethylarginine dimethylaminohydrolase. Circulation 106:987–992
Lonn E, Bosch J, Yusuf S, Sheridan P, Pogue J, Arnold JM, Ross C, Arnold A, Sleight P, Probstfield J, Dagenais GR (2005) Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial. Jama 293:1338–1347
Manach C, Mazur A, Scalbert A (2005) Polyphenols and prevention of cardiovascular diseases. Curr Opin Lipidol 16:77–84
Martasek P, Miller RT, Liu Q, Roman LJ, Salerno JC, Migita CT, Raman CS, Gross SS, Ikeda-Saito M, Masters BS (1998) The C331A mutant of neuronal nitric-oxide synthase is defective in arginine binding. J Biol Chem 273:34799–34805
Masters BS, McMillan K, Sheta EA, Nishimura JS, Roman LJ, Martasek P (1996) Neuronal nitric oxide synthase, a modular enzyme formed by convergent evolution: structure studies of a cysteine thiolate-liganded heme protein that hydroxylates l-arginine to produce NO. as a cellular signal. FASEB J 10:552–558
Matsuno K, Yamada H, Iwata K, Jin D, Katsuyama M, Matsuki M, Takai S, Yamanishi K, Miyazaki M, Matsubara H, Yabe-Nishimura C (2005) Nox1 is involved in angiotensin II-mediated hypertension: a study in Nox1-deficient mice. Circulation 112:2677–2685
McNally JS, Davis ME, Giddens DP, Saha A, Hwang J, Dikalov S, Jo H, Harrison DG (2003) Role of xanthine oxidoreductase and NAD(P)H oxidase in endothelial superoxide production in response to oscillatory shear stress. Am J Physiol Heart Circ Physiol 285:H2290–H2297
Miller RT, Martasek P, Omura T, Siler Masters BS (1999) Rapid kinetic studies of electron transfer in the three isoforms of nitric oxide synthase. Biochem Biophys Res Commun 265:184–188
Miller RT, Martasek P, Raman CS, Masters BS (1999) Zinc content of Escherichia coli-expressed constitutive isoforms of nitric-oxide synthase. Enzymatic activity and effect of pterin. J Biol Chem 274:14537–14540
Milstien S, Katusic Z (1999) Oxidation of tetrahydrobiopterin by peroxynitrite: implications for vascular endothelial function. Biochem Biophys Res Commun 263:681–684
Ming XF, Barandier C, Viswambharan H, Kwak BR, Mach F, Mazzolai L, Hayoz D, Ruffieux J, Rusconi S, Montani JP, Yang Z (2004) Thrombin stimulates human endothelial arginase enzymatic activity via RhoA/ROCK pathway: implications for atherosclerotic endothelial dysfunction. Circulation 110:3708–3714
Moat SJ, Clarke ZL, Madhavan AK, Lewis MJ, Lang D (2006) Folic acid reverses endothelial dysfunction induced by inhibition of tetrahydrobiopterin biosynthesis. Eur J Pharmacol 530:250–258
Mollnau H, Wendt M, Szocs K, Lassegue B, Schulz E, Oelze M, Li H, Bodenschatz M, August M, Kleschyov AL, Tsilimingas N, Walter U, Forstermann U, Meinertz T, Griendling K, Munzel T (2002) Effects of angiotensin II infusion on the expression and function of NAD(P)H oxidase and components of nitric oxide/cGMP signaling. Circ Res 90:E58–E65
Morita T (2005) Heme oxygenase and atherosclerosis. Arterioscler Thromb Vasc Biol 25:1786–1795
Mueller CF, Laude K, McNally JS, Harrison DG (2005) Redox mechanisms in blood vessels. Arterioscler Thromb Vasc Biol 25:274–278
Ng CJ, Bourquard N, Grijalva V, Hama S, Shih DM, Navab M, Fogelman AM, Lusis AJ, Young S, Reddy ST (2006) Paraoxonase-2 deficiency aggravates atherosclerosis in mice despite lower apolipoprotein-B-containing lipoproteins: anti-atherogenic role for paraoxonase-2. J Biol Chem 281:29491–29500
Nickenig G, Harrison DG (2002) The AT(1)-type angiotensin receptor in oxidative stress and atherogenesis: part I: oxidative stress and atherogenesis. Circulation 105:393–396
Nickenig G, Baumer AT, Temur Y, Kebben D, Jockenhovel F, Bohm M (1999) Statin-sensitive dysregulated AT1 receptor function and density in hypercholesterolemic men. Circulation 100:2131–2134
Noble MA, Munro AW, Rivers SL, Robledo L, Daff SN, Yellowlees LJ, Shimizu T, Sagami I, Guillemette JG, Chapman SK (1999) Potentiometric analysis of the flavin cofactors of neuronal nitric oxide synthase. Biochemistry 38:16413–16418
O’Driscoll JG, Green DJ, Rankin JM, Taylor RR (1999) Nitric oxide-dependent endothelial function is unaffected by allopurinol in hypercholesterolaemic subjects. Clin Exp Pharmacol Physiol 26:779–783
Ohara Y, Peterson TE, Harrison DG (1993) Hypercholesterolemia increases endothelial superoxide anion production. J Clin Invest 91:2546–2551
Ohashi M, Runge MS, Faraci FM, Heistad DD (2006) MnSOD deficiency increases endothelial dysfunction in ApoE-deficient mice. Arterioscler Thromb Vasc Biol 26:2331–2336
Ohishi M, Ueda M, Rakugi H, Naruko T, Kojima A, Okamura A, Higaki J, Ogihara T (1997) Enhanced expression of angiotensin-converting enzyme is associated with progression of coronary atherosclerosis in humans. J Hypertens 15:1295–1302
Paolini M, Sapone A, Canistro D, Chieco P, Valgimigli L (2003) Antioxidant vitamins for prevention of cardiovascular disease. Lancet 362:920, author reply 921
Pieper GM (1997) Acute amelioration of diabetic endothelial dysfunction with a derivative of the nitric oxide synthase cofactor, tetrahydrobiopterin. J Cardiovasc Pharmacol 29:8–15
Pollock JS, Forstermann U, Mitchell JA, Warner TD, Schmidt HH, Nakane M, Murad F (1991) Purification and characterization of particulate endothelium-derived relaxing factor synthase from cultured and native bovine aortic endothelial cells. Proc Natl Acad Sci U S A 88:10480–10484
Pou S, Keaton L, Surichamorn W, Rosen GM (1999) Mechanism of superoxide generation by neuronal nitric-oxide synthase. J Biol Chem 274:9573–9580
Pritchard KA Jr, Groszek L, Smalley DM, Sessa WC, Wu M, Villalon P, Wolin MS, Stemerman MB (1995) Native low-density lipoprotein increases endothelial cell nitric oxide synthase generation of superoxide anion. Circ Res 77:510–518
Ramachandran A, Levonen AL, Brookes PS, Ceaser E, Shiva S, Barone MC, Darley-Usmar V (2002) Mitochondria, nitric oxide, and cardiovascular dysfunction. Free Radic Biol Med 33:1465–1474
Raman CS, Li H, Martasek P, Kral V, Masters BS, Poulos TL (1998) Crystal structure of constitutive endothelial nitric oxide synthase: a paradigm for pterin function involving a novel metal center. Cell 95:939–950
Rosenkranz-Weiss P, Sessa WC, Milstien S, Kaufman S, Watson CA, Pober JS (1994) Regulation of nitric oxide synthesis by proinflammatory cytokines in human umbilical vein endothelial cells. Elevations in tetrahydrobiopterin levels enhance endothelial nitric oxide synthase specific activity. J Clin Invest 93:2236–2243
Rossitch E, Alexander E, Black PM, Cooke JP (1991) l-arginine normalizes endothelial function in cerebral vessels from hypercholesterolemic rabbits. J Clin Invest 87:1295–1299
Rozenberg O, Shih DM, Aviram M (2005) Paraoxonase 1 (PON1) attenuates macrophage oxidative status: studies in PON1 transfected cells and in PON1 transgenic mice. Atherosclerosis 181:9–18
Schachinger V, Britten MB, Zeiher AM (2000) Prognostic impact of coronary vasodilator dysfunction on adverse long-term outcome of coronary heart disease. Circulation 101:1899–1906
Shinozaki K, Kashiwagi A, Nishio Y, Okamura T, Yoshida Y, Masada M, Toda N, Kikkawa R (1999) Abnormal biopterin metabolism is a major cause of impaired endothelium- dependent relaxation through nitric oxide/O2- imbalance in insulin-resistant rat aorta. Diabetes 48:2437–2445
Shinozaki K, Nishio Y, Okamura T, Yoshida Y, Maegawa H, Kojima H, Masada M, Toda N, Kikkawa R, Kashiwagi A (2000) Oral administration of tetrahydrobiopterin prevents endothelial dysfunction and vascular oxidative stress in the aortas of insulin-resistant rats. Circ Res 87:566–573
Simon A, Plies L, Habermeier A, Martine U, Reining M, Closs EI (2003) Role of neutral amino acid transport and protein breakdown for substrate supply of nitric oxide synthase in human endothelial cells. Circ Res 93:813–820
Sorescu D, Weiss D, Lassegue B, Clempus RE, Szocs K, Sorescu GP, Valppu L, Quinn MT, Lambeth JD, Vega JD, Taylor WR, Griendling KK (2002) Superoxide production and expression of nox family proteins in human atherosclerosis. Circulation 105:1429–1435
Stanner SA, Hughes J, Kelly CN, Buttriss J (2004) A review of the epidemiological evidence for the ’antioxidant hypothesis’. Public Health Nutr 7:407–422
Steinkamp-Fenske K, Bollinger L, Xu H, Yao Y, Horke S, Forstermann U, Li H (2007) Reciprocal regulation of endothelial nitric-oxide synthase and NADPH oxidase by betulinic acid in human endothelial cells. J Pharmacol Exp Ther 322:836–842
Steinkamp-Fenske K, Bollinger L, Voller N, Xu H, Yao Y, Bauer R, Forstermann U, Li H (2007) Ursolic acid from the Chinese herb danshen (Salvia miltiorrhiza L.) upregulates eNOS and downregulates Nox4 expression in human endothelial cells. Atherosclerosis 195:e104–e111
Stocker R, Perrella MA (2006) Heme oxygenase-1: a novel drug target for atherosclerotic diseases? Circulation 114:2178–2189
Stoclet JC, Chataigneau T, Ndiaye M, Oak MH, El Bedoui J, Chataigneau M, Schini-Kerth VB (2004) Vascular protection by dietary polyphenols. Eur J Pharmacol 500:299–313
Stroes E, Kastelein J, Cosentino F, Erkelens W, Wever R, Koomans H, Luscher T, Rabelink T (1997) Tetrahydrobiopterin restores endothelial function in hypercholesterolemia. J Clin Invest 99:41–46
Stroes ES, van Faassen EE, Yo M, Martasek P, Boer P, Govers R, Rabelink TJ (2000) Folic acid reverts dysfunction of endothelial nitric oxide synthase. Circ Res 86:1129–1134
Stuehr D, Pou S, Rosen GM (2001) Oxygen reduction by nitric-oxide synthases. J Biol Chem 276:14533–14536
Sydow K, Munzel T (2003) ADMA and oxidative stress. Atheroscler Suppl 4:41–51
Sydow K, Schwedhelm E, Arakawa N, Bode-Boger SM, Tsikas D, Hornig B, Frolich JC, Boger RH (2003) ADMA and oxidative stress are responsible for endothelial dysfunction in hyperhomocyst(e)inemia: effects of l-arginine and B vitamins. Cardiovasc Res 57:244–252
Taille C, El-Benna J, Lanone S, Dang MC, Ogier-Denis E, Aubier M, Boczkowski J (2004) Induction of heme oxygenase-1 inhibits NAD(P)H oxidase activity by down-regulating cytochrome b558 expression via the reduction of heme availability. J Biol Chem 279:28681–28688
Torzewski M, Ochsenhirt V, Kleschyov AL, Oelze M, Daiber A, Li H, Rossmann H, Tsimikas S, Reifenberg K, Cheng F, Lehr HA, Blankenberg S, Forstermann U, Munzel T, Lackner KJ (2007) Deficiency of glutathione peroxidase-1 accelerates the progression of atherosclerosis in apolipoprotein E-deficient mice. Arterioscler Thromb Vasc Biol 27:850–857
Touyz RM, Yao G, Schiffrin EL (2003) c-Src induces phosphorylation and translocation of p47phox: role in superoxide generation by angiotensin II in human vascular smooth muscle cells. Arterioscler Thromb Vasc Biol 23:981–987
Turrens JF, Alexandre A, Lehninger AL (1985) Ubisemiquinone is the electron donor for superoxide formation by complex III of heart mitochondria. Arch Biochem Biophys 237:408–414
Tward A, Xia YR, Wang XP, Shi YS, Park C, Castellani LW, Lusis AJ, Shih DM (2002) Decreased atherosclerotic lesion formation in human serum paraoxonase transgenic mice. Circulation 106:484–490
van Etten RW, de Koning EJ, Honing ML, Stroes ES, Gaillard CA, Rabelink TJ (2002) Intensive lipid lowering by statin therapy does not improve vasoreactivity in patients with type 2 diabetes. Arterioscler Thromb Vasc Biol 22:799–804
Vaziri ND, Ni Z, Oveisi F (1998) Upregulation of renal and vascular nitric oxide synthase in young spontaneously hypertensive rats. Hypertension 31:1248–1254
Vergnani L, Hatrik S, Ricci F, Passaro A, Manzoli N, Zuliani G, Brovkovych V, Fellin R, Malinski T (2000) Effect of native and oxidized low-density lipoprotein on endothelial nitric oxide and superoxide production: key role of l-arginine availability. Circulation 101:1261–1266
Verhaar MC, Stroes E, Rabelink TJ (2002) Folates and cardiovascular disease. Arterioscler Thromb Vasc Biol 22:6–13
Verhaar MC, Wever RM, Kastelein JJ, van Dam T, Koomans HA, Rabelink TJ (1998) 5-Methyltetrahydrofolate, the active form of folic acid, restores endothelial function in familial hypercholesterolemia. Circulation 97:237–241
Vita JA (2005) Polyphenols and cardiovascular disease: effects on endothelial and platelet function. Am J Clin Nutr 81:292S–297S
Vita JA, Treasure CB, Nabel EG, McLenachan JM, Fish RD, Yeung AC, Vekshtein VI, Selwyn AP, Ganz P (1990) Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circulation 81:491–497
Wagner AH, Kohler T, Ruckschloss U, Just I, Hecker M (2000) Improvement of nitric oxide-dependent vasodilatation by HMG-CoA reductase inhibitors through attenuation of endothelial superoxide anion formation. Arterioscler Thromb Vasc Biol 20:61–69
Wallerath T, Poleo D, Li H, Forstermann U (2003) Red wine increases the expression of human endothelial nitric oxide synthase: a mechanism that may contribute to its beneficial cardiovascular effects. J Am Coll Cardiol 41:471–478
Wallerath T, Li H, Godtel-Ambrust U, Schwarz PM, Forstermann U (2005) A blend of polyphenolic compounds explains the stimulatory effect of red wine on human endothelial NO synthase. Nitric Oxide 12:97–104
Wallerath T, Deckert G, Ternes T, Anderson H, Li H, Witte K, Forstermann U (2002) Resveratrol, a polyphenolic phytoalexin present in red wine, enhances expression and activity of endothelial nitric oxide synthase. Circulation 106:1652–1658
Warnholtz A, Nickenig G, Schulz E, Macharzina R, Brasen JH, Skatchkov M, Heitzer T, Stasch JP, Griendling KK, Harrison DG, Bohm M, Meinertz T, Munzel T (1999) Increased NADH-oxidase-mediated superoxide production in the early stages of atherosclerosis: evidence for involvement of the renin–angiotensin system. Circulation 99:2027–2033
Wassmann S, Laufs U, Baumer AT, Muller K, Konkol C, Sauer H, Bohm M, Nickenig G (2001) Inhibition of geranylgeranylation reduces angiotensin II-mediated free radical production in vascular smooth muscle cells: involvement of angiotensin AT1 receptor expression and Rac1 GTPase. Mol Pharmacol 59:646–654
Wassmann S, Laufs U, Baumer AT, Muller K, Ahlbory K, Linz W, Itter G, Rosen R, Bohm M, Nickenig G (2001) HMG-CoA reductase inhibitors improve endothelial dysfunction in normocholesterolemic hypertension via reduced production of reactive oxygen species. Hypertension 37:1450–1457
Werner ER, Gorren AC, Heller R, Werner-Felmayer G, Mayer B (2003) Tetrahydrobiopterin and nitric oxide: mechanistic and pharmacological aspects. Exp Biol Med 228:1291–1302
Werner-Felmayer G, Werner ER, Fuchs D, Hausen A, Reibnegger G, Schmidt K, Weiss G, Wachter H (1993) Pteridine biosynthesis in human endothelial cells. Impact on nitric oxide-mediated formation of cyclic GMP. J Biol Chem 268:1842–1846
White CR, Darley-Usmar V, Berrington WR, McAdams M, Gore JZ, Thompson JA, Parks DA, Tarpey MM, Freeman BA (1996) Circulating plasma xanthine oxidase contributes to vascular dysfunction in hypercholesterolemic rabbits. Proc Natl Acad Sci U S A 93:8745–8749
Wilmink HW, Stroes ES, Erkelens WD, Gerritsen WB, Wever R, Banga JD, Rabelink TJ (2000) Influence of folic acid on postprandial endothelial dysfunction. Arterioscler Thromb Vasc Biol 20:185–188
Woo KS, Chook P, Lolin YI, Sanderson JE, Metreweli C, Celermajer DS (1999) Folic acid improves arterial endothelial function in adults with hyperhomocystinemia. J Am Coll Cardiol 34:2002–2006
Xia Y, Tsai AL, Berka V, Zweier JL (1998) Superoxide generation from endothelial nitric-oxide synthase. A Ca2+/calmodulin-dependent and tetrahydrobiopterin regulatory process. J Biol Chem 273:25804–25808
Xu W, Kaneko FT, Zheng S, Comhair SA, Janocha AJ, Goggans T, Thunnissen FB, Farver C, Hazen SL, Jennings C, Dweik RA, Arroliga AC, Erzurum SC (2004) Increased arginase II and decreased NO synthesis in endothelial cells of patients with pulmonary arterial hypertension. FASEB J 18:1746–1748
Yamashiro S, Kuniyoshi Y, Arakaki K, Miyagi K, Koja K (2002) The effect of insufficiency of tetrahydrobiopterin on endothelial function and vasoactivity. Jpn J Thorac Cardiovasc Surg 50:472–477
Yamawaki H, Haendeler J, Berk BC (2003) Thioredoxin: a key regulator of cardiovascular homeostasis. Circ Res 93:1029–1033
Yang H, Roberts LJ, Shi MJ, Zhou LC, Ballard BR, Richardson A, Guo ZM (2004) Retardation of atherosclerosis by overexpression of catalase or both Cu/Zn-superoxide dismutase and catalase in mice lacking apolipoprotein E. Circ Res 95:1075–1081
Yoshida K, Okamura T, Kimura H, Bredt DS, Snyder SH, Toda N (1993) Nitric oxide synthase-immunoreactive nerve fibers in dog cerebral and peripheral arteries. Brain Res 629:67–72
Yoshida T, Maulik N, Engelman RM, Ho YS, Magnenat JL, Rousou JA, Flack JE 3rd, Deaton D, Das DK (1997) Glutathione peroxidase knockout mice are susceptible to myocardial ischemia reperfusion injury. Circulation 96(Flack JE):II-216–II-220
Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P (2000) Vitamin E supplementation and cardiovascular events in high-risk patients. The heart outcomes prevention evaluation study investigators. N Engl J Med 342:154–160
Zalba G, San Jose G, Moreno MU, Fortuno MA, Fortuno A, Beaumont FJ, Diez J (2001) Oxidative stress in arterial hypertension: role of NAD(P)H oxidase. Hypertension 38:1395–1399
Zhang C, Hein TW, Wang W, Chang CI, Kuo L (2001) Constitutive expression of arginase in microvascular endothelial cells counteracts nitric oxide-mediated vasodilatory function. FASEB J 15:1264–1266
Zhang C, Hein TW, Wang W, Miller MW, Fossum TW, McDonald MM, Humphrey JD, Kuo L (2004) Upregulation of vascular arginase in hypertension decreases nitric oxide-mediated dilation of coronary arterioles. Hypertension 44:935–943
Zhang Y, Griendling KK, Dikalova A, Owens GK, Taylor WR (2005) Vascular hypertrophy in angiotensin II-induced hypertension is mediated by vascular smooth muscle cell-derived H2O2. Hypertension 46:732–737
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Förstermann, U. Nitric oxide and oxidative stress in vascular disease. Pflugers Arch - Eur J Physiol 459, 923–939 (2010). https://doi.org/10.1007/s00424-010-0808-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-010-0808-2