
Abstract
Aims
To evaluate comparative outcomes of emergency laparotomy closure with and without prophylactic mesh.
Methods
A systematic review was performed via literature databases: PubMed, Cochrane Library, Science Direct, and Google Scholar. Studies were examined for eligibility and included if they compared prophylactic mesh closure to the conventional laparotomy closure following emergency abdominal surgery. Both acute wound failure and incisional hernia (IH) occurence were our primary outcomes. Secondary outcomes included surgical site infection (SSI), seroma/hematoma formation, Clavien-Dindo complications (score ≥ 3), total operative time, and length of hospital stay (LOS).
Results
Two randomised controlled trials (RCTs) and four comparative studies with a total of 817 patients met the inclusion criteria. Overall acute wound failure and incisional hernia rate was significantly lower in the mesh group compared to non-mesh group (odd ratio (OR) 0.23, p = 0.002) and (OR 0.21, p = 0.00001), respectively. There was no significant difference between the two groups regarding the following outcomes: total operative time (mean difference (MD) 21.44, p = 0.15), SSI (OR 1.47, p = 0.06), seroma/haematoma formation (OR 2.74, p = 0.07), grade ≥ 3 Clavien-Dindo complications (OR 2.39, p = 0.28), and LOS (MD 0.26, p = 0.84).
Conclusion
The current evidence for the use of prophylactic mesh in emergency laparotomy is diverse and obscure. Although the data trends towards a reduction in the incidence of IH, a reliable conclusion requires further high-quality RCTs to fully assess the efficacy and safety of mesh use in an emergency setting.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite the widespread use of laparoscopy and minimally invasive approaches in surgery, midline laparotomy remains the commonest surgical approach for abdominal emergencies [1]. It has been evident that complications of emergency laparotomy are more frequent compared to elective laparotomies [2]. Wound failure, defined as ‘impaired wound healing leading to inability to maintain a normal anatomy of the abdominal wall’ is a well-recognised and serious postoperative complication.
The incidence of acute wound dehiscence (AWD) has been reported to be up to 3.5% [3, 4], reaching 14.9% in the emergency setting [5,6,7]. AWD is associated with a high mortality that approximates 45% [8, 9]. Additionally, incisional hernia (IH) occurrence, defined as chronic wound failure, has an adverse impact on an individual’s quality of life and significant cost burden on the healthcare system [10, 11]. IH occurrence ranges from 3 to 20% [12, 13] reaching as high as 50% following emergency surgery [14, 15]. There are several risk factors attributed to wound failure, including patient-related factors, underlying pathology, and surgical technique [16, 17].
Refinements of exisiting closure technique such as employing small-bite closure and the use of retention sutures in the hope of reducing AWD and IH formation have been investigated [18,19,20]. With the evolving technology of surgical mesh implants, the prophylactic use of mesh to reinforce the abdominal wall and prevent wound failure has been proven to be beneficial in both elective laparotomies and ostomy closure, especially in high-risk populations [21,22,23,24,25]. Few studies have investigated the role of mesh during closure of the abdominal wall in emergency laparotomies [26,27,28,29,30,31]. This may be related in part to safety concerns regarding the use of surgical mesh in cases of peritonitis and/or working in contaminated operative fields [32, 33].
Following the recent publication of RCTs in this field, our review aims at providing an up-to-date, well-powered, and inclusive evidence to evaluate the efficacy of mesh closure in reducing early and late post-emergency laparotomy wound failure. We also assess the safety and other postoperative complications associated with this technique.
Methods
Study design
This systematic review was designed and performed in accordance with the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [34], as well as the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [35].
Data sources and search strategy
A systematic online search was conducted on 01/6/2021 using the following databases and clinical trial registers: PubMed, Scopus, Cochrane Database of Systematic Reviews (CENTRAL), clinical trials.gov, ScienceDirect, and VHL (virtual health library). The search was executed by two independent reviewers using the search strategy outlined in Appendix 1. Furthermore, manual search of reference lists in the relevant previously published systematic reviews and studies was performed to identify relevant articles.
Design and study selection
The titles, abstracts, and/or full texts of the identified articles have been screened by two authors independently to identify the potentially eligible studies. All studies comparing prophylactic mesh closure versus the conventional suture technique during an emergency laparotomy, including all types of emergency abdominal conditions, were considered. All single-arm and non-emergency studies, case series, and review articles were excluded. Any disagreement between the authors on inclusion and exclusion criteria was resolved through discussion and consensus.
Data collection
The following information was extracted from the included studies: first author, year of publication, study country of origin, study design, study size and description of the study participants, number of patients, patient characteristics, and outcomes. Extracted data were entered into a pre-generated standard Microsoft® Excel (Microsoft Corporation, Redmond, WA, USA) file. Data extraction was performed independently by two authors, and disagreements were resolved by discussion and consensus. If no agreement could be reached, a third author was consulted.
Outcome measures
The primary outcome measure was wound failure, including both AWD and IH. Total operative time, seroma/haematoma formation, surgical site infection (SSI), complications of Clavien-Dindo score ≥ 3, and length of hospital stay (LOS) were the secondary measured outcomes.
Assessment of bias
The methodological quality and risk of bias assessment in the observational studies were carried out by two authors using the Newcastle–Ottawa scale (NOS) [36]. The NOS is a star-based scoring system (maximum score 9) which enables review authors to evaluate an observational study in the following aspects: selection of the study groups, comparability of the groups, and the ascertainment of the outcome of interest. Studies with a score of 9 stars were deemed to be of a low risk of bias, studies with a rating of 7 or 8 stars were at medium risk, and those scoring six or less were judged to be at a high risk of bias.
For RCTs, risk of bias was assessed, independently, by two authors using the Cochrane risk of bias tool [37]. The following categories were classified as high, low, or unclear: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Variations in the risk of bias assessment were resolved by a discussion between authors.
Statistical analysis
Odd ratio (OR) was used as the statistical measure for dichotomous outcomes using the Mantel–Haenszel method. P < 0.05 has been considered significant for all analyses, and 95% confidence interval (CI) was used in this study. For continuous outcomes, mean difference (MD) with 95% CI was estimated. When mean values were not available for continuous outcomes, data of median and interquartile range (IQR) were extracted and subsequently converted to mean and standard deviation (SD) using the well-practised equation described by Hozo et al. [38]. Random-effects modelling was applied for all outcomes analysis.
Furthermore, between-study heterogeneity has been assessed using the I2 and χ2 statistic. Higher values of I2 and the χ2 statistic signify increased levels of heterogeneity, with p < 0.05 or an I2 value exceeding 50% indicating significant heterogeneity [39]. We conducted sensitivity analyses to explore potential sources of heterogeneity and assess the robustness of our results. For each outcome parameter, we repeated the primary analysis using random-effects or fixed-effect models. In addition, for each of our defined dichotomous variables, we calculated the pooled risk ratio (RR) or risk difference (RD).
Finally, we evaluated the effect of each study on the overall effect size and heterogeneity by repeating the analysis following excluding one study at a time. Statistical analyses were undertaken using the Review Manager 5.0 (Nordic Cochrane Centre, Cochrane Collaboration).
Results
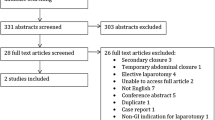
Our search yielded a total of 951 studies, of which 879 were excluded after assessing the titles and abstracts of the published papers. Of the 72 studies included in full-text screening, 67 were excluded as they were not relevant to the scope of this review. Finally, 6 studies were deemed appropriate for inclusion in this meta-analysis [26,27,28,29,30,31]. Figure 1 demonstrates the PRISMA flow chart. The included studies reported a total of 817 patients divided between the mesh group (n = 297) and non-mesh group (n = 520). Table 1 shows characteristics of the included studies.

PRISMA flow chart
To clarify, mesh position was stated as ‘on-lay’ in three studies [26, 28, 29], intraperitoneal in two [27, 30], and retro-muscular in one study [31]. The mesh was fixed in position in all patients who received mesh closure. IH assessment was carried out through a combination of clinical examination and imaging (ultrasound or computed tomography). Moreover, a polydioxanone suture was used for closure of the fascia in five studies [26,27,28,29,30], whilst in one study, a polypropylene material was employed [31].
Four studies included only those patients who underwent emergency GI laparotomy [27, 29,30,31] whilst the other two expanded their inclusion criteria and included all emergency laparotomy patients [26, 28]. Characteristics of the included populations and surgical techniques are demonstrated in Tables 2 and 3, respectively.
Methodological appraisal of included studies
The methodological appraisal of the included observational studies is illustrated in Appendix 2. The risk of bias was judged as moderate in all included studies. Regarding the RCTs, both included RCTs reported random sequence generation and allocation concealment [29, 30]. However, performance bias and detection bias were assessed to be high in one study [29] and unclear in the other [30]. An overview of the risk of bias is shown in Fig. 2.

Risk of bias assessment of included RCTs. (a) Risk of bias summary of included RCTs. (b) Risk of bias graph of included RCTs
Primary outcome
Wound failure
Wound failure, which includes AWD and IH, was reported in all included studies with a total number of 817 patients (Fig. 3). Wound failure rate was significantly higher in the non-mesh group when compared to the mesh group (5.4% in mesh group vs. 22.3% in non-mesh group, OR 0.23, 95% CI (0.09, 0.58), p = 0.002).

Forest plots of the measured outcomes
The subgroup analysis for AWD, which was mentioned in three studies, showed a higher incidence in the non-mesh group. However, the difference was not statistically significant (2.9% in mesh group vs. 11.6% in non-mesh group, OR 0.36, 95% CI (0.02, 6.09), p = 0.48). Interestingly, these two RCTs reported contradictory results with one RCT favouring mesh use to lower AWD occurrence (inexistence of AWD in mesh group vs. AWD of 13.5% in non-mesh group, p = 0.003) and the other concluding failure of mesh closure to prevent AWD (14.3% in mesh group vs. 3.7% in non-mesh, p = 0.292).
The were 114 patients who developed IH as reported in three of the included studies (Fig. 3). The rate of IH was statistically higher in the non-mesh group than mesh group (6.6% in mesh group vs. 25.8% in non-mesh group, OR 0.21, 95% CI (0.11, 0.40), p = 0.00001). The level of heterogeneity was deemed to be high between the included studies (I2 = 57%, p = 0.05).
Secondary outcomes
Operative time
Operative time was reported in four studies including 562 patients in total (Fig. 3). There was no statistically significant difference between the mesh group and non-mesh group regarding duration of the procedure (187.8 ± 71.04 min vs. 169.2 ± 59.67 min respectively, MD 21.44, 95% CI (− 7.63, 50.51), p = 0.15). A high level of heterogeneity was noted among included studies (I2 = 66%, p = 0.03).
Surgical site infection (SSI)
The number of patients who developed SSI was mentioned in all the six studies (Fig. 3). The rate of SSI was higher in the mesh group when compared to the non-mesh group; however, the difference was not statistically significant (29.9% in mesh vs 21.7% in non-mesh, OR 1.47, 95% CI (0.99, 2.17), P = 0.06). The level of heterogeneity of the studies in this case was low (I2 = 11%, P = 0.34).
Seroma/haematoma formation
Seroma and haematoma occurrence was reported in two studies with a total number of 163 patients (Fig. 3). There was no statistically significant difference between the two groups regarding seroma/haematoma formation (16.6% in mesh group vs. 6.3% in non-mesh group, OR 2.74, 95% CI (0.91, 8.19), p = 0.07). A low level of heterogeneity was observed between included studies (I2 0%, p = 0.58).
Complications of Clavien-Dindo grade ≥ 3
The number of patients who developed complications graded as Clavien-Dindo grade 3 or higher was reported in two studies with 314 patients in total (Fig. 3). The rate of the described complications was comparable between the two groups (38.1% in mesh group vs. 30.4% in non-mesh group, OR 2.39, 95% CI (0.49, 11.74), p = 0.28). The level of heterogeneity was high among included studies (I2 = 56%, p = 0.13).
Length of hospital stay
The length of hospital stay (LOS) was compared in four studies including 562 patients (Fig. 3). The LOS was comparable between the two groups (16.3 ± 5.54 days in mesh group vs. 15.4 ± 4.96 days in non-mesh group, MD 0.26, 95% CI (− 2.24, 2.76), p = 0.84). A low level of heterogeneity was observed between studies (I2 = 0%, p = 0.61).
Sensitivity analysis
The direction of the pooled effect size remained unchanged when RR or RD was calculated for dichotomous variables. Furthermore, leave one out analysis has not demonstrated important discrepancies with the original analysis.
Discussion
An estimated 24,823 patients underwent emergency laparotomy over a 12-month period in England and Wales [40]. These procedures were performed for various conditions including acute intestinal obstruction, perforated viscus, bowel ischaemia, and abdominal trauma [40]. Although lifesaving, emergency laparotomies have a disproportionately high morbidity and mortality rate and prolonged hospital stay in comparison to elective cases [41]. Mortality is estimated to be almost ten times that of major elective gastrointestinal surgery [42]. Additionally, numerous immediate and delayed complications can occur following an emergency laparotomy. Post-operative cardio-respiratory and infectious complications may be managed conservatively but some often necessitate further surgical intervention including AWD, anastomotic leak, enterocutaneous fistulae, and IH.
The European hernia society defines IH as ‘any abdominal wall gap with or without a bulge in the area of postoperative scar perceptible or palpable by clinical examination or imaging’. Despite advancements in techniques for abdominal wall closure, the incidence of IH formation following an emergency laparotomy remains over 20% [43]. Although the exact aetiology remains unknown, the development of these hernias is thought to be multifactorial. Patient-related factors (obesity, smoking, malnutrition, immuno-suppressants), disease (site of incision, underlying pathology, timing, and urgency of procedure), and technical factors (poor surgical technique, suture material) are all thought to play a role [44,45,46].
IH can have an adverse impact on a patient’s quality of life causing abdominal discomfort and pain. Untreated, some patients may develop serious and potentially life-threating complications like intestinal obstruction, incarceration, or strangulation. Consequently, it is imperative to reduce this risk. This includes adopting general peri-operative measures such as the administration of antibiotics, pain control, optimising respiratory function, reducing operative time, and early mobilisation. Technical factors are also an important consideration. Currently, there is no standardised intervention or procedure to prevent the occurrence of IH following an emergency laparotomy. Although the advent of laparoscopic surgery has greatly reduced the incidence of this occurring [47], a significant number of emergency procedures are still performed through an open abdominal incision.
The use of slowly absorbable/non-absorbable monofilament suture and increasing the ratio of suture length to wound length > 4 helps to reduce the incidence of IH formation. In randomised trials, the use of small-bite closure has also been shown to be superior to mass closure [18]. Depending on the safety profile, prophylactic mesh augmentation (synthetic/biological) may be another strategy as it has shown promising results in elective midline laparotomies [21, 48]. In patients undergoing vascular or bariatric procedures, the use of prophylactic mesh has been shown to reduce IH [49,50,51]. Prophylactic mesh reinforcement during the closure of a temporary stoma also reduces the subsequent risk of stoma site IH and surgical intervention [25].
Our systematic review and meta-analysis primarily assessed the role of prophylactic mesh in reducing the incidence of AWD and IH formation following an emergency laparotomy. Mesh use was associated with a significantly reduced incidence of IH. However, there was no demonstrable difference in AWD rates between the two groups. Furthermore, there was no significant difference between the groups for the measured secondary outcomes (operative time, SSI rate, haematoma/seroma formation, LOS, and grades III–IV Clavien-Dindo complications). There was a variable degree of heterogeneity observed between the included studies.
A 2019 meta-analysis also assessed the safety and efficacy of prophylactic mesh placement in emergency laparotomy [52]. They included two observational studies only that were biased due to many confounding factors [27, 28]. Due to the limited dataset, the authors were unable to draw any meaningful conclusions on the role of prophylactic mesh in such settings. Our analysis attempted to address this through the inclusion of two recent RCTs and another two retrospective studies [26, 29,30,31].
Both observational studies [27, 28] in the aforementioned meta-analysis [52] favoured mesh placement in reducing the risk of subsequent IH compared to standard closure of a laparotomy wound in emergency surgery. Both were similar in the number of patients included (133 vs. 150) and compared mesh with continuous loop PDS (mass) closure. However, the type of mesh used (non-absorbable composite synthetic vs. partially absorbable lightweight large-pore synthetic), mesh position (intra-peritoneal vs. on-lay), and mesh fixation technique (suture, staples, or combination vs. suture and staples) were different. The follow-up period for both studies was similar (17 and 16 months respectively). This could arguably be regarded as an insufficient timeframe to determine the development of complications such as IH. Moreover, a recent prospective study [31] concluded the overall benefit of fixing a retro-rectus polypropylene mesh in preventing AWD. Their 30-day follow-up period did not raise any major safety concern about the mesh implanted. Also, the recently published retrospective study [26] demonstrated the benefit of using a synthetic lightweight mesh in preventing IH over a minimum of 2-year follow-up period of 187 patients. The comparison between using a mesh, which is fixed by staples + / − stitches and positioned on-lay, and conventional closure with a continuous PDS loop suture supported the safety and efficacy of mesh closure.
The addition of two further randomised studies in our meta-analysis was still insufficient to provide a conclusive answer to the use of mesh in preventing/reducing the incidence of IH after emergency surgery. A prospective RCT in patients undergoing emergency abdominal surgery comparing outcomes after prophylactic intraperitoneal implantation of a biological mesh with standard abdominal wall closure was prematurely terminated. Their aim was to study hernia-free survival following mesh implantation, but the trial was ended early due to serious safety concerns and significantly more mesh-associated abdominal wall complications requiring re-operation [30]. These included AWD, septic complications, and necrosis of the abdominal wall. The second RCT had a primary end-point of the incidence of AWD at 30 days post-operation [29]. Although the authors did not consider IH occurrence in their study, their results supported the use of mesh to reduce AWD following emergency laparotomy. The contradiction in results of both RCTs is thought to correlate to the type and potentially position of the mesh used, particularly with the remaining variables being relatively comparable. The biologic mesh was introduced for its potential superiority to combat septic complications in contaminated operative field [53, 54]; however, this has been debated by the lack of SSI reduction reported in some studies [30, 55]. This point is worth investigating, especially with the high cost of biologic meshes; meanwhile, macroporous polypropylene meshes represent a cheaper and maybe more convenient alternative in contaminated abdomen using a specific technique and mesh position [56]. In agreement with this, the authors of this RCT attributed the failure of their mesh technique to lessen AWD to the properties of the acellular porcine mesh as its low foreign body reaction and incomplete biodegradability [30]. It remains uncertain whether this can be generalised to all other biologic meshes.
Five out of six [26,27,28, 30, 31] of the included studies in this review applied the 1 cm rule for closure of the sheath, i.e. both the distance from the stitches to the fascial border and the gap between any two stiches are 1 cm. Moreover, the small bites technique (0.5 cm between stiches and 0.5 cm from the fascial border) was used by Lime et al. [29] A multicentre randomised trial which compared small bites (0.5 cm) versus large bites (1 cm), concluded that small bites technique is superior in preventing incisional hernia [57]. Added to that, results from several reports in the literature support small bites technique over the traditional closure techniques [58, 59].
In keeping with the findings from the previous study, we found no significant difference in SSI rates between the mesh vs. non-mesh groups. This is important especially at a time of heightened public concern surrounding the use of meshes in surgery. Moreover, the additional step of mesh fixation did not significantly increase total operative time (MD 21 min) and there was no significant difference in haematoma/seroma formation between the groups.
None of the included studies assessed cosmesis and post-operative pain, apart from the latest published study [26] that reported absence of chronic pain in both groups. Mesh implantation particularly after emergency abdominal surgery and in the presence of contamination may be associated with chronic infection and enterocutaneous fistulas. These may require mesh extraction; however, the reported 2 cases of chronic mesh infection in one of the studies were treated without mesh removal [26]. Only 2 comparative studies reported on enterocutaneous fistula formation noting a comparable rate between the mesh group and conventional abdominal wall closure in patients with peritonitis [27, 31].
In this meta-analysis, we attempted to address the safety and efficacy of mesh placement during abdominal wall closure in emergency laparotomies through the addition of four recent studies, including two RCTs [26, 29,30,31]. In particular, we were interested in prevention of short-term and long-term wound failure. Despite these new studies, the current literature remains insufficient to reliably answer this question.
There are many limitations in this analysis, and some have been mentioned previously. The dataset remains small and not all studies reported on our primary outcome. Four out of six of the included studies are retrospective studies which leads to high risk of selection bias and significant heterogeneity between the included studies. Important differences in the degree of peritoneal contamination/soiling in each study could have an impact on outcomes. Other important and relevant endpoints like wound healing, chronic pain, cosmesis, and long-term follow-up are needed to make definitive conclusions on the value of mesh placement at the time of abdominal wall closure in an emergency setting. Moreover, there was significant variation between the studies in terms of mesh type, mesh positioning (intra-peritoneal, sub-lay, on-lay), and fixation method. Therefore, our conclusion of reduced IH rates with the use of mesh in emergency surgery remains weak as it draws on three observational studies. Our sub-group analysis showed no significant difference in the incidence of AWD between the mesh and non-mesh groups. Future research should include well-designed RCTs addressing these criticised points to establish powerful evidence.
Conclusion
Wound failure (AWD and IH) is a common complication following a midline laparotomy especially in the emergency setting. The existing evidence for the use of prophylactic mesh in emergency laparotomy remains heterogenous and inconclusive. Although the data suggests a reduction in the incidence of IH, further high-quality RCTs are required to reliably assess the safety and efficacy of meshes in preventing wound failure following emergency laparotomies. These should involve a standardised cohort of patients including comparable underlying pathologies, degree of peritoneal contamination/soiling, type and location of mesh used, and fixation method(s) to draw meaningful conclusions.
References
Tolstrup M-B, Watt SK, Gögenur I (2017) Morbidity and mortality rates after emergency abdominal surgery: an analysis of 4346 patients scheduled for emergency laparotomy or laparoscopy. Langenbecks Arch Surg 402(4):615–623
Murtaza B, Saeed S, Sharif MA (2010) Postoperative complications in emergency versus elective laparotomies at a peripheral hospital. J Ayub Med Coll Abbottabad 22(3):42–47
Webster C, Neumayer L, Smout R, Horn S, Daley J, Henderson W et al (2003) Prognostic models of abdominal wound dehiscence after laparotomy. J Surg Res 109(2):130–137
Halasz NA (1968) Dehiscence of laparotomy wounds. Am J Surg 116(2):210–214
Díaz CJG, Cladera PR, Soto SN, Rosas JMH, Aufroy AL, Vioque SM et al (2014) Validation of abdominal wound dehiscence’s risk model. Cirugía Española (English Edition) 92(2):114–119
Meena K, Ali S, Chawla AS, Aggarwal L, Suhani S, Kumar S et al (2013) A prospective study of factors influencing wound dehiscence after midline laparotomy. Surg Sci 4(8):354–358
van Ramshorst GH, Nieuwenhuizen J, Hop WC, Arends P, Boom J, Jeekel J et al (2010) Abdominal wound dehiscence in adults: development and validation of a risk model. World J Surg 34(1):20–27
Fleischer G, Rennert A, Rühmer M (2000) Infected abdominal wall and burst abdomen. Der Chirurg; Zeitschrift fur Alle Gebiete der Operativen Medizen 71(7):754–62
Carlson MA (1997) Acute wound failure. Surg Clin North Am 77(3):607–636
Fischer JP, Basta MN, Mirzabeigi MN, Bauder AR, Fox JP, Drebin JA et al (2016) A risk model and cost analysis of incisional hernia after elective, abdominal surgery based upon 12,373 cases: the case for targeted prophylactic intervention. Ann Surg 263(5):1010–1017
van Ramshorst GH, Eker HH, Hop WC, Jeekel J, Lange JF (2012) Impact of incisional hernia on health-related quality of life and body image: a prospective cohort study. Am J Surg 204(2):144–150
Sørensen LT, Hemmingsen U, Kallehave F, Wille-Jørgensen P, Kjærgaard J, Møller LN et al (2005) Risk factors for tissue and wound complications in gastrointestinal surgery. Ann Surg 241(4):654
Sanders DL, Kingsnorth AN (2012) The modern management of incisional hernias. BMJ 344:e2843
Moussavian MR, Schuld J, Dauer D, Justinger C, Kollmar O, Schilling MK et al (2010) Long term follow up for incisional hernia after severe secondary peritonitis—incidence and risk factors. Am J Surg 200(2):229–234
Mingoli A, Puggioni A, Sgarzini G, Luciani G, Corzani F, Ciccarone F et al (1999) Incidence of incisional hernia following emergency abdominal surgery. Ital J Gastroenterol Hepatol 31(6):449–453
Itatsu K, Yokoyama Y, Sugawara G, Kubota H, Tojima Y, Kurumiya Y et al (2014) Incidence of and risk factors for incisional hernia after abdominal surgery. Br J Surg 101(11):1439–1447
Aksamija G, Mulabdic A, Rasic I, Aksamija L (2016) Evaluation of risk factors of surgical wound dehiscence in adults after laparotomy. Med Arch 70(5):369
Deerenberg EB, Harlaar JJ, Steyerberg EW, Lont HE, van Doorn HC, Heisterkamp J et al (2015) Small bites versus large bites for closure of abdominal midline incisions (STITCH): a double-blind, multicentre, randomised controlled trial. Lancet 386(10000):1254–1260
Rink AD, Goldschmidt D, Dietrich J, Nagelschmidt M, Vestweber K-H (2000) Negative side-effects of retention sutures for abdominal wound closure. A prospective randomised study. Eur J Surg 166(12):932–7
Khorgami Z, Shoar S, Laghaie B, Aminian A, Araghi NH, Soroush A (2013) Prophylactic retention sutures in midline laparotomy in high-risk patients for wound dehiscence: a randomized controlled trial. J Surg Res 180(2):238–243
Borab ZM, Shakir S, Lanni MA, Tecce MG, MacDonald J, Hope WW et al (2017) Does prophylactic mesh placement in elective, midline laparotomy reduce the incidence of incisional hernia? A systematic review and meta-analysis. Surgery 161(4):1149–1163
Bhangu A, Fitzgerald J, Singh P, Battersby N, Marriott P, Pinkney T (2013) Systematic review and meta-analysis of prophylactic mesh placement for prevention of incisional hernia following midline laparotomy. Hernia 17(4):445–455
Bhangu A, Nepogodiev D, Ives N, Magill L, Glasbey J, Forde C et al (2020) Prophylactic biological mesh reinforcement versus standard closure of stoma site (ROCSS): a multicentre, randomised controlled trial. Lancet 395(10222):417–426
Rios-Diaz AJ, Fischer JP (2020) Stoma closure reinforcement with biological mesh and incisional hernia. The Lancet 395(10222):393–395
Mohamedahmed AYY, Stonelake S, Zaman S, Hajibandeh S (2020) Closure of stoma site with or without prophylactic mesh reinforcement: a systematic review and meta-analysis. Int J Colorectal Dis: 1–12
Bravo-Salva A, Argudo-Aguirre N, González-Castillo A, Membrilla-Fernandez E, Sancho-Insenser J, Grande-Posa L et al (2021) Long-term follow-up of prophylactic mesh reinforcement after emergency laparotomy. A retrospective controlled study. BMC Surg 21(1):1–8
Kurmann A, Barnetta C, Candinas D, Beldi G (2013) Implantation of prophylactic nonabsorbable intraperitoneal mesh in patients with peritonitis is safe and feasible. World J Surg 37(7):1656–1660
Argudo N, Pereira JA, Sancho JJ, Membrilla E, Pons MJ, Grande L (2014) Prophylactic synthetic mesh can be safely used to close emergency laparotomies, even in peritonitis. Surgery 156(5):1238–1244
Lima HV, Rasslan R, Novo FC, Lima TM, Damous SH, Bernini CO et al (2020) Prevention of fascial dehiscence with onlay prophylactic mesh in emergency laparotomy: a randomized clinical trial. J Am Coll Surg 230(1):76–87
Jakob MO, Haltmeier T, Candinas D, Beldi G (2020) Biologic mesh implantation is associated with serious abdominal wall complications in patients undergoing emergency abdominal surgery: a randomized-controlled clinical trial. J Trauma Acute Care Surg 89(6):1149–1155
Tiwari G, Dadoriya A, Thakur DS, Somashekar U, Kothari R, Agarwal P, Sharma D (2020) Prophylactic mesh placement for emergency midline laparotomy in peptic perforation peritonitis: a prospective observational study of short term results. Asian J Surg 43(2):456–457. https://doi.org/10.1016/j.asjsur.2019.11.017
Choi JJ, Palaniappa NC, Dallas KB, Rudich TB, Colon MJ, Divino CM (2012) Use of mesh during ventral hernia repair in clean-contaminated and contaminated cases: outcomes of 33,832 cases. Ann Surg 255(1):176–180
Haskins IN, Amdur RL, Lin PP, Vaziri K (2016) The use of mesh in emergent ventral hernia repair: effects on early patient morbidity and mortality. J Gastrointest Surg 20(11):1899–1903
Higgins JP, Green S, Collaboration C (2011) Cochrane handbook for systematic reviews of interventions. 2011
Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8(5):336–341
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M et al (2000) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Oxford
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5(1):1–10
Lau J, Ioannidis JP, Schmid CH (1997) Quantitative synthesis in systematic reviews. Ann Intern Med 127(9):820–826
Nela.org.uk. NELAN. National Emergency Laparotomy Audit (NELA). Nela.org.uk.
Bansal A, Mallick MR, Jena S (2019) A study of post-operative complications of all emergency laparotomy in a tertiary care hospital within 90 days. Arch Clin Gastroenterol 5(2):015–018
Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C et al (2012) Mortality after surgery in Europe: a 7 day cohort study. Lancet 380(9847):1059–1065
Peponis T, Bohnen JD, Muse S, Fuentes E, Van Der Wilden GM, Mejaddam A et al (2018) Interrupted versus continuous fascial closure in patients undergoing emergent laparotomy: a randomized controlled trial. J Trauma Acute Care Surg 85(3):459–465
Kaneko T, Funahashi K, Ushigome M, Kagami S, Goto M, Koda T et al (2019) Incidence of and risk factors for incisional hernia after closure of temporary ileostomy for colorectal malignancy. Hernia 23(4):743–748
Basta MN, Kozak GM, Broach RB, Messa CA IV, Rhemtulla I, DeMatteo RP et al (2019) Can we predict incisional hernia?: Development of a surgery-specific decision–support interface. Ann Surg 270(3):544–553
Inamdar MF, Singh AR, Inamdar N (2017) Incisional hernia: risk factors, clinical presentations, and pre-peritoneal polypropylene mesh repair. Int Surg J 4(4):1189–1194
Nho RLH, Mege D, Ouaïssi M, Sielezneff I, Sastre B (2012) Incidence and prevention of ventral incisional hernia. J Visc Surg 149(5):e3–e14
Jairam AP, Timmermans L, Eker HH, Pierik RE, van Klaveren D, Steyerberg EW et al (2017) Prevention of incisional hernia with prophylactic onlay and sublay mesh reinforcement versus primary suture only in midline laparotomies (PRIMA): 2-year follow-up of a multicentre, double-blind, randomised controlled trial. Lancet 390(10094):567–576
Strzelczyk J, Szymański D, Nowicki M, Wilczyński W, Gaszynski T, Czupryniak L (2006) Randomized clinical trial of postoperative hernia prophylaxis in open bariatric surgery. Br J Surg 93(11):1347–1350
Bevis P, Windhaber R, Lear P, Poskitt K, Earnshaw J, Mitchell D (2010) Randomized clinical trial of mesh versus sutured wound closure after open abdominal aortic aneurysm surgery. Br J Surg 97(10):1497–1502
Curro G, Centorrino T, Low V, Sarra G, Navarra G (2012) Long-term outcome with the prophylactic use of polypropylene mesh in morbidly obese patients undergoing biliopancreatic diversion. Obes Surg 22(2):279–282
Burns FA, Heywood E, Challand C, Lee MJ (2020) Is there a role for prophylactic mesh in abdominal wall closure after emergency laparotomy? A systematic review and meta-analysis. Hernia 24(3):441–447
Bondre IL, Holihan JL, Askenasy EP, Greenberg JA, Keith JN, Martindale RG, Roth JS, Liang MK, Ventral Hernia Outcomes Collaborative (2016) Suture, synthetic, or biologic in contaminated ventral hernia repair. J Surg Res. 200(2):488–494
Rosen MJ, Bauer JJ, Harmaty M et al (2017) Multicenter, prospective, longitudinal study of the recurrence, surgical site infection, and quality of life after contaminated ventral hernia repair using biosynthetic absorbable mesh: the COBRA study. Ann Surg 265(1):205–211
Atema JJ, de Vries FE, Boermeester MA (2016) Systematic review and meta-analysis of the repair of potentially contaminated and contaminated abdominal wall defects. Am J Surg 212(5):982-95e1
Kockerling F, Alam NN, Antoniou SA et al (2018) What is the evidence for the use of biologic or biosynthetic meshes in abdominal wall reconstruction? Hernia 22(2):249–269
Deerenberg EB, Harlaar JJ, Steyerberg EW, Lont HE, van Doorn HC et al (2015) Small bites versus large bites for closure of abdominal midline incisions (STITCH): a double-blind, multicentre, randomised controlled trial. Lancet 386(10000):1254–1260. https://doi.org/10.1016/S0140-6736(15)60459-7
Henriksen NA, Deerenberg EB, Venclauskas L, Fortelny RH, Miserez M, Muysoms FE (2018) Meta-analysis on materials and techniques for laparotomy closure: the MATCH review. World J Surg 42(6):1666–1678. https://doi.org/10.1007/s00268-017-4393-9
Lesch C, Kallinowski F, Uhr K, Vollmer M, Gerhard CP, Gutjahr D, Krimmel L, Ludwig Y-M (2021) Reduction of failure rates after incisional hernia repair by adding a prophylactic mesh. Brit J Surg 108(Supplement_8):znab395.050. https://doi.org/10.1093/bjs/znab395.050
Author information
Authors and Affiliations
Contributions
Conception and design: MA, AYYM, SZ. Literature search and study selection: MA, AYYM. Data collection, analysis, and interpretation: MA, AYYM, SZ. Writing the article and critical revision: all authors. Final approval of the article: all authors. Statistical analysis: AYYM, MA.
Corresponding author
Ethics declarations
Ethical approval
Considering the nature of this study, ethical approval was not required.
Human and animal rights
This study is a systematic review with meta-analysis of outcomes which does not include research directly involving human or animal participation.
Informed consent
Considering the nature of this study, informed consent was not required.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Mohamed Albendary and Ali Yasen Y Mohamedahmed had equal contribution in this study proposing joint first authorship.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Albendary, M., Mohamedahmed, A.Y.Y., Alamin, A. et al. Efficacy and safety of mesh closure in preventing wound failure following emergency laparotomy: a systematic review and meta-analysis. Langenbecks Arch Surg 407, 1333–1344 (2022). https://doi.org/10.1007/s00423-021-02421-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-021-02421-4