
Abstract
Background
We report the surgical treatment of a consecutive series of scan negative patients with the intention of unilateral parathyroid exploration with the aid of intraoperative quick PTH (qPTH).
Materials and methods
The study included 35 consecutive sestamibi scan negative patients (27 women, eight men) with sporadic pHPT subjected to first time surgery. Median age was 70 years and median preoperative calcium level 2.8 mmol/L.
Results
Thirty-three patients had a histological diagnosis of a parathyroid adenoma (median weight 0.48 g [range 0.12 g–2.5 g]). Nineteen patients were explored bilaterally and 16 patients (46%) were operated unilaterally. The median operation time was 40 min in the unilateral group and 95 min in the bilateral group (p < 0.001). Three patients were treated for postoperative hypocalcemia after bilateral exploration versus none in the unilateral group (p = 0.23). With a minimum of 12 months of follow-up, 33 patients (94.3%) were cured. One case of recurrent HPT presented after bilateral exploration with visualization of four glands. One case of persistent HPT was observed after unilateral exploration. qPTH was predictive of operative failure in both patients.
Conclusion
Forty-six percent of the patients in our study could be operated unilaterally with a total cure rate of 94%. Patients in the unilateral group had a significant shorter operation time and a lower incidence of postoperative hypocalcemia. In conclusion our investigation shows that limited parathyroid exploration can safely be performed on patients with negative sestamibi scintigraphy by the aid of qPTH.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Primary hyperparathyroidism (pHPT) is a common disease that affects 1% of the adult population [1] and some 3% in postmenopausal women.
Classic signs of pHPT include renal lithiasis, cholecystolithiasis, gastrointestinal ulcerations, depression, and osteoporosis.
Despite lack of classical signs, a higher incidence of glucose intolerance, hypertension, hyperlipidemia, and increased morbidity and mortality from cardiovascular disease as well as an increased fracture risk is seen in patients with pHPT [2, 3].
Bilateral neck exploration with visualization of all four parathyroid glands has been regarded as the gold standard in treatment of pHPT. Recently minimal invasive and/or focused approach after preoperative localization studies with the aid of intraoperative measurement of PTH (ioPTH), have challenged bilateral neck exploration [4–6]. It has been shown that limited exploration has advantages such as shorter hospital stay, less postoperative pain, and fewer complications, e.g., severe postoperative hypocalcemia [4, 7].
Quick PTH has been proved earlier to be a reliable marker for successful removal of parathyroid tissue [8].
The aim of the present study was to evaluate if it is feasible to perform focused unilateral surgery of pHPT patients with preoperatively negative sestamibi scintigraphy with the aid of ioPTH.
Materials and methods
Patients
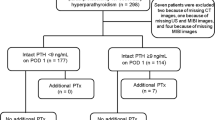
Thirty-five consecutive sestamibi scan negative patients (27 women and eight men) with sporadic pHPT, subjected to first time surgery at Lund University Hospital between October 2003 and May 2006 were included in our study. The median age was 70 years (range 37–83 years). The median preoperative serum calcium level was 2.8 mmol/L (range 2.6–3.2 mmol/L). Median preoperative PTH level was 9.7 pmol/L (range 5.3–31 pmol/L).
Exclusion criteria were family history of pHPT, familial hypocalciuric hypercalcemia (FHH), and other planned operations during the surgical procedure including thyroid surgery. The biochemical diagnosis of pHPT was based on a serum calcium level of more than 2.60 mmol/L and a serum PTH level of more than 5 pmol/L with a serum creatinine level of less than 200 µmol/L. Postoperative hypocalcemia was defined as serum calcium <2.2 mmol/L with typical symptoms of hypocalcemia.
Planned intervention
The patients were subjected to surgery with the intent of limited parathyroid exploration. Surgery commenced with operation of the left side with a minimal transverse incision, 15–20 mm long. If no adenoma was found, the patient was explored bilaterally; this operation was performed by a second lateral incision of 15 to 20 mm with the possibility of conversion to standard open technique (Kocher incision) if needed. Due to the infrequent use of neck ultrasound between 2003 and 2006, we decided to start exploration on the left side of the neck. This approach was once introduced by Sten Tibblin for patients with negative, preoperative localization results, and has a long tradition at the Lund University Hospital.
Sestamibi scintigraphy
Sestamibi subtraction scintigraphy was performed with 30 MBq 99 m Tc and 500 MBq 99 mTc sestamibi [9].
Biochemistry
All blood samples were collected after an overnight fast. Preoperative data were obtained from blood samples collected the day before surgery after an overnight fast. Twenty-four hours urine calcium excretion was routinely evaluated to exclude patients with FHH. Serum ionized calcium concentrations (reference range 2.20–2.60 mmol/L) were analyzed from blood samples normalized to a pH of 7.4 with the ion selective electrode ABL 505 (Radiometer, Copenhagen, Denmark). Serum PTH (reference range 1.0–5.0 pmol/L) was analyzed by using an assay for intact PTH (Incstar, Stillwater, MN, USA) with a sensitivity of 0.13 pmol/L and a reference range of 1.0–5.0 pmol/L. The inter-assay coefficient of variation (CV) is <11% and the intra-assay variation <6%. The method has a CV of 2.2% at a value of 5 pmol/L.
To shorten the time for intraoperative analysis, the method was modified as previously described [10]. The within-assay variation between 0.8 and 10 pmol/L is less than 8% for the rapid method. The correlation between the two methods is 0.99.
A decrease of ioPTH of >50% after 5 min or >60% after 15 min has been proved earlier to be a reliable predictor for successful removal of pathological parathyroid tissue [8, 10–13].
Follow-up
All patients were followed at least 12 months after surgery. Persistent disease was defined as raised levels of serum calcium before 6 months after surgery. Recurrent disease was defined as raised serum calcium levels after 6 months.
Statistics
Results for continuous variables are expressed as median and range if not stated otherwise. For numeric data, differences between groups were analyzed with the Mann–Whitney test. For categorical data, statistic significance was analyzed using the chi-squared test and the Fishers exact test when frequencies were expected to be less than five. A probability level for a random difference of p < 0.05 was considered to be significant. For categorical data, absolute numbers in addition to percentage are given.
Results
Of 35 patients, 16 underwent unilateral surgery and 19 patients were explored bilaterally. One patient had persisting HPT after 12 months follow-up and one patient suffered from recurrent disease. Thus, the overall cure rate was 94.3%. Among all 35 patients, 33 got the histological diagnosis adenoma. The median weight was 0.48 g (range 0.12–2.49 g). Operation time in the unilateral group was significantly (p < 0.001) lower compared to the bilateral group. Adenoma weight did not differ significant (p = 0.45). Three patients in the bilateral group suffered from postoperative hypocalcemia compared to zero patients in the unilateral group (p = 0.23).
None of the 35 patients suffered from laryngeal nerve damage. There was no significant difference in the complication rate (postoperative bleeding, hematoma, and local discomfort) between the two groups. Cosmetic results were estimated by the patients with the visual analog scale (VAS). Median VAS in the unilateral group was 10 compared to 9 in the bilateral group (p = 0.1).
The results of both groups are presented in Table 1.
Unilateral group
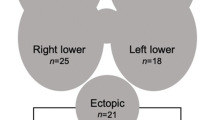
This group is composed of 16 patients; 12 females and four males with a median age of 71.5 years (range 49–83 years). In all 16 patients autopsy showed solitary adenoma with a median weight of 0.48 g (range 0.15–2.5 g). Median operation time was 39.5 min (range 13–64 min). None of the patients suffered from postoperative hypocalcemia and all patients but one were cured 12 months after surgery with one case of persistent HPT 12 months after surgery.
Intraoperative PTH in this patient declined 48%, 5 min after removal of the lower left gland and 54% after 15 min with an additional decline after 20 min. Therefore, the surgeon decided to terminate operation without bilateral exploration. The final histopathological report showed solitary adenoma. The patient should have become subject to bilateral exploration according to ioPTH protocol.
Bilateral group
This group is composed of 19 patients; 15 females, four males with a median age of 67 years (range 37–83 years) were operated bilaterally. Seventeen patients histopathological report showed single gland disease (solitary adenoma) with median weight of 0.4 g (range 0.12–1.6 g). Operation time was median 95 min (range 29–266 min). Three patients suffered from postoperative hypocalcemia. Eighteen out of 19 patients (94.7%) were cured with correct prediction by intraoperative qPTH.
In one case of recurrent HPT observed in this group, four enlarged glands could be identified. After removal of three glands, qPTH declined 13% only. The patient was intraoperatively conceived to have hyperplasia, final histopathological report showed however normal glands. FHH or a fifth, not identified gland was discussed as a possible explanation. This patient did unfortunately not collect 24 h urine for further investigation. At 6 months follow-up, the patient was normocalcemic. Twelve months after surgery, the disease recurred.
In one case of hyperplasia, the patient suffered from a large groin. Two glands on the left side were removed without PTH decline. After negative reexploration we converted to bilateral surgery without identifying any glands on the right side. After bilateral exploration, PTH declined to normal levels and operation was executed. The final histopathological report showed hyperplasia.
Operation time was 266 min and the patient suffered from postoperative hypocalcemia that needed treatment. After both 6 and 12 months the patient was normocalcemic and was considered to be cured.
Intraoperative PTH
Thirteen out of 35 patients declined less than 50% of PTH after 5 min (median 59.2%), seven of these 13 patients declined more than 60% after 15 min. Among the remaining six that declined less than 60%, two suffered from persistent or recurrent pHPT.
Intraoperative PTH predicted operative success in 29 of 33 cases (88%). All patients with a surgical failure and persistent or recurrent pHPT were true negative.
The sensitivity was 88% and specificity was 100%.
Discussion
Even in the era of minimal invasive surgery, patients with negative sestamibi scintigraphy are still undergoing open, bilateral exploration as a standard procedure. In this study we compared bilateral, conventional neck exploration with a bilateral procedure by two lateral 15–20-mm incisions on each side in patients with negative sestamibi scintigraphy.
Previous studies have shown that patients with negative sestamibi scintigraphy have smaller adenomas, lower PTH levels, and a lower cure rate than patients with positive scintigraphy results [14, 15].
In our study we could not find any proof for a higher incidence of multiglandular disease in patients with pHPT and negative scintigraphy. Although there were only few patients in this study, we show that unilateral procedure can be performed safely with better cosmetic results, shorter operation time, and less early hypocalcemia with the aid of ioPTH in these patients. Further in 46% of all cases we succeeded with unilateral operation. Patients with negative scintigraphy results have a higher risk of persistent HPT [14, 15]. Cure rate in our study was 94.3%.
In conclusion we showed that limited parathyroid exploration with the aid of intraoperative PTH measurement can be performed in pHPT patients with negative sestamibi scintigraphy with a high cure rate.
References
Jorde R, Bonaa KH, Sundsfjord J (2000) Primary hyperparathyroidism detected in a health screening. The Tromso study. J Clin Epidemiol Volume, 1164–1169
Vestergaard P et al (2003) Cardiovascular events before and after surgery for primary hyperparathyroidism. World J Surg Volume 27(2):216–222
Hagstrom E et al (2006) Metabolic abnormalities in patients with normocalcemic hyperparathyroidism detected at a population-based screening. Eur J Endocrinol 155(1):33–39
Bergenfelz A et al (2002) Unilateral versus bilateral neck exploration for primary hyperparathyroidism: a prospective randomized controlled trial. Ann Surg 236(5):543–551
Russell CF, Dolan SJ, Laird JD (2006) Randomized clinical trial comparing scan-directed unilateral versus bilateral cervical exploration for primary hyperparathyroidism due to solitary adenoma. Br J Surg 93(4):418–421
Gil-Cardenas A et al (204) Is intraoperative parathyroid hormone assay mandatory for the success of targeted parathyroidectomy? J Am Coll Surg 204(2):286–290
Tang T et al (2007) Does the surgical approach affect quality of life outcomes?—a comparison of minimally invasive parathyroidectomy with open parathyroidectomy. Int J Surg 5(1):17–22
Westerdahl J, Lindblom P, Bergenfelz A (2002) Measurement of intraoperative parathyroid hormone predicts long-term operative success. Arch Surg 137:186–190
Bergenfelz A et al (1997) Sestamibi versus thallium subtraction scintigraphy in parathyroid localization: a prospective comparative study in patients with predominantly mild primary hyperparathyroidism. Surgery 121:601–605
Bergenfelz A, Isaksson A, Ahren B (1994) Intraoperative monitoring of intact PTH during surgery for primary hyperparathyroidism. Langenbecks Arch Chir 379:50–53
Inabnet WB (2004) Intraoperative parathyroid hormone monitoring. World J Surg 28:1212–1215
Bergenfelz A et al (1998) Measurement of parathyroid hormone in patients with primary hyperparathyroidism undergoing first and reoperative surgery. Br J Surg 85:1129–1132. doi:10.1046/j.1365-2168.1998.00824.x
Bergenfelz A, Norden NE, Ahren B (1991) Intraoperative fall in plasma levels of intact parathyroid hormone after removal of one enlarged parathyroid gland in hyperparathyroid patients. Eur J Surg 157:109–112
Chiu B, Sturgeon C, Angelos P (2006) What is the link between nonlocalizing sestamibi scans, multigland disease, and persistent hypercalcemia? A study of 401 consecutive patients undergoing parathyroidectomy. Surgery 140:418–422
Mihai R et al (2006) Negative imaging studies for primary hyperparathyroidism are unavoidable: correlation of sestamibi and high-resolution ultrasound scanning with histological analysis in 150 patients. World J Surg 30:697–704
Author information
Authors and Affiliations
Corresponding author
Additional information
Best of Endocrine Surgery in Europe 2009
Rights and permissions
About this article
Cite this article
Thier, M., Nordenström, E., Bergenfelz, A. et al. Surgery for patients with primary hyperparathyroidism and negative sestamibi scintigraphy—a feasibility study. Langenbecks Arch Surg 394, 881–884 (2009). https://doi.org/10.1007/s00423-009-0524-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-009-0524-6