
Abstract
Purpose
Fast muscular oxygen uptake (\({\dot{V}}{\text{O}_\text{2musc}}\)) kinetics are limiting factors for high exercise capacities. It is hypothesized that \({\dot{V}}{\text{O}_\text{2musc}}\) and heart rate (HR) kinetics would be faster in individuals, performing long-distance endurance training (CONT) compared with athletes performing predominantly interval-based sports (INT).
Methods
17 subjects (INT: n = 7, 24 ± 5 years, 183 ± 7 cm, 85 ± 10 kg, 6 ± 3 h of training per week, CONT: n = 10, 37 ± 7 years, 175 ± 9 cm, 69 ± 10 kg, 6 ± 3 h of training per week) completed a treadmill work rate (WR) protocol with pseudo-randomized WR changes with velocities of 6.5 and 9.5 km h−1. \({\dot{V}}\)O2musc and the respective kinetics were estimated from the measured pulmonary oxygen uptake and HR combined with a circulatory model. Kinetics information were calculated using time series analysis. Higher maxima of the cross-correlation function (CCF) of WR and the respective parameter (\({\dot{V}}{\text{O}_\text{2musc}}\), HR) indicate faster kinetics responses.
Results
The kinetics of HR (INT: 0.23 ± 0.04 vs. CONT: 0.42 ± 0.18; P = 0.001), \({\dot{V}}\)O2pulm (0.30 ± 0.05 vs. 0.53 ± 0.20; P = 0.005) and \({\dot{V}}\)O2musc (0.31 ± 0.06 vs. 0.53 ± 0.16; P = 0.005) were significantly slower in INT compared with the CONT athletes.
Conclusions
It seems that at least in the long-term CONT exercise, training without the need of changing intensities is favorable for fast \({\dot{V}}\)O2 and HR kinetics compared with INT exercise including frequently changing intensities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Muscular oxygen uptake (\({\dot{V}}\)O2musc) kinetics are determined by the complex interplay of oxygen delivery and oxygen extraction inside the working muscle in response to changing metabolic demands. An adequate functional interaction between oxygen delivery and oxygen extraction is a prerequisite for fast \({\dot{V}}\)O2musc kinetics (Hughson 2009; Murias et al. 2014; Poole and Jones 2012). Faster oxygen uptake kinetics determined from phase 2 (metabolic component) of pulmonary measurements (\({\dot{V}}\)O2pulm) were reported to be associated with higher maximal oxygen uptake (\({\dot{V}}\)O2max) values (Powers et al. 1985; Regensteiner et al. 1998; Chilibeck et al. 1996) and were documented as more sensitive to training interventions, compared with \({\dot{V}}\)O2max (e.g., Fukuoka et al. 2002; Murias et al. 2014).
Different groups of athletes were compared regarding their \({\dot{V}}\)O2pulm kinetics. Long-distance runners show faster \({\dot{V}}\)O2pulm kinetics compared with middle-distance runners (Berger et al. 2006; Kilding et al. 2006, 2007) and sub-elite sprint-trained athletes (Berger and Jones 2007). In contrast, Do Nascimento Salvador et al. (2016) report no differences in \({\dot{V}}\)O2pulm kinetics during maximal and supramaximal work rate (WR) intensities between sprint-trained and middle-distance runners. However, the comparability with kinetics responses during moderate-intensity exercise is not per se possible, since the characteristics of \({\dot{V}}\)O2 kinetics in these high-intensity exercise domains are still discussed and conclusions on differences between various groups of subjects are difficult. Analyzing muscle biopsies from the m. vastus lateralis, it has been observed that muscles of long-distance runners contain less fast twitch (FT) and more slow twitch (ST) fibers compared with sprint-trained athletes. Further, the percentage of FT fibers decreased with the length of the running events that the individuals participated in (Inbar et al. 1981). From the studies of Crow and Kushmerick (1982), it can be concluded that ST fibers show faster \({\dot{V}}\)O2 kinetics than FT fibers.
\({\dot{V}}\)O2pulm kinetics of endurance athletes and typical team sport athletes with similar lengths of competitive events but different changes of metabolic demands during those events were not compared, yet.
Further, there is evidence that the analysis of \({\dot{V}}\)O2musc kinetics using the time constant of phase 2 of mono-exponential fitting of the \({\dot{V}}\)O2pulm response to an increased metabolic demand might be distorted by an increasing cardiac output (\({\dot{Q}}\), Hoffmann et al. 2013). It is frequently assumed that the distortions of the pulmonary measured \({\dot{V}}\)O2 response due to an increasing \({\dot{Q}}\) is limited to the cardiodynamic phase (phase I), which is commonly either determined to be constantly 20 s or detected individually and then excluded from the analysis. A lower HR could lead to a faster adjustment of HR (Coote 2010) and, therefore, \({\dot{Q}}\) during changes of metabolic demands. This possibly influences the phase 2 \({\dot{V}}\)O2pulm kinetics, depending on the method, used to determine the cardiodynamic phase of the \({\dot{V}}\)O2pulm response to increased metabolic demands (Mezzani et al. 2010). In the listed references, the kinetics of heart rate (HR) as an indicator of \({\dot{Q}}\) responses (DeLorey et al. 2004) are not mentioned (Berger and Jones 2007; Kilding et al. 2006, 2007; Do Nascimento Salvador et al. 2016). Absolute values of HR were reported as lower during rest and moderate exercise at steady state in long-distance runners compared with middle-distance runners (Kilding et al. 2006). Drescher et al. (2018) compared mono-exponential fitting with time series analyses to determine the kinetics of \({\dot{V}}\)O2musc. The authors suggested to determine the cardiodynamic phase as accurately as possible (Drescher et al. 2018). Hence, the approach of Hoffmann et al. (2013) determines \({\dot{V}}\)O2musc kinetics using time series analysis in combination with a circulatory model. Kinetics responses are not analyzed in two phases, but \({\dot{V}}\)O2musc kinetics are determined from \({\dot{V}}\)O2pulm and HR measurements considering the dynamic adjustment of \({\dot{Q}}\) during changing metabolic demands.
The aim of this study was to compare \({\dot{V}}\)O2 kinetics between endurance-trained athletes with predominantly continuous endurance exercise training characteristics (CONT) and individuals who perform sports with mostly intermittent exercise training characteristics, such as tennis, basketball or handball (INT). Considering the cardiodynamic phase by the use of a circulatory model (Hoffmann et al. 2013) INT and CONT with equal \({\dot{V}}\)O2peak values, but very different training regimes are compared. It was hypothesized that \({\dot{V}}\)O2musc, \({\dot{V}}\)O2pulm and HR kinetics would be faster in CONT than in INT athletes.
Methods
Participants
Overall, 24 subjects participated in the study. Prior to the test procedures, the experimental protocol was approved by the institutional review board of the German Sport University Cologne considering the declaration of Helsinki including the amendments until 2013. A positive vote was available before the beginning of the study. Informed consent was obtained from all individual participants included in the study prior to the tests. The subjects were recruited through social media and with the help of signboards. Subjects were eligible to participate in the experiment if they were between 18 and 45 years of age, reported a minimum of 3 years of experience in their sports activity, had 2–4 training sessions per week, and were experienced with running on a treadmill. Seven subjects had to be excluded from analyses: five subjects due to noisy data and two subjects due to an exercise intensity during the WR protocol that was above their individual gas exchange threshold (GET). Finally, data from 17 subjects [INT n = 7 (6 males, 1 female), CONT n = 10 (5 males, 5 females)] were included in statistical analyses. Anthropometrical data for the included subjects are presented in Table 1.
Subjects were either INT trained (tennis, roller hockey, basketball or handball) or they were CONT trained (long-distance running and cycling) and ran about 19 ± 9 km per week (excluding the km they cycled) without using interval-based exercise training. The INT group trained about 4 ± 1 times per week for 6 ± 3 h for 15 ± 11 years. The CONT group trained about 4 ± 1 times per week for 6 ± 3 h for 8 ± 5 years.
Experimental setup
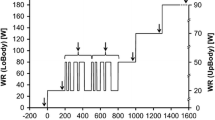
The test protocol, which both groups completed, was performed on a h\p\cosmos pulsar treadmill (h\p\cosmos sports and medical GmbH, Nussdorf-Traunstein, Germany). The work rate (WR) protocol started with a 3 min resting measurement in the standing position, followed by 300 s at 6.5 km h−1 (low step), two 300-s-long sequences of pseudo-randomized WR changes with velocities of either 6.5 or 9.5 km h−1 (PRBS1 and PRBS2) and 300 s at 9.5 km h−1 (high step). The inclination was set to 1% during this part of the WR protocol, the shortest sequence during the PRBS was 20 s and the longest 80 s. The acceleration mode of the treadmill was set to 4, which corresponds to 1.38 m s−2. The subjects were instructed to run and not to walk during the entire protocol, which was monitored at all times by the test supervisor.
The moderate PRBS exercise protocol was followed by an incremental ramp protocol to evaluate peak oxygen uptake (\({\dot{V}}\)O2peak). Every minute the speed was increased by 1 km h−1 until the maximum of 14 km h−1 was reached. The intensity was then further increased by raising the inclination of the treadmill by 1% every 30 s (Fig. 1). An active recovery phase of 5 min at 4 km h−1 was started immediately after completing the ramp protocol. The ramp protocol was terminated when the subject was not able to keep up with the speed of the treadmill anymore.

WR protocol with the PRBS to evaluate cardiorespiratory kinetics followed by the incremental ramp protocol. WR work rate, PRBS pseudo-random-binary sequence
Pulmonary gas exchange was measured breath-by-breath (Metalyzer 3B, Cortex Biophysik GmbH, Leipzig, Germany). HR, stroke volume (SV), and \({\dot{Q}}\) were measured beat to beat via a Physioflow Enduro device (Manatech Biomedical, Poissy, France). All devices were calibrated according to the manufacturers’ guidelines before each testing. The volume transducer of the gas analyzer was calibrated with a 3L calibration syringe and the analyzers were calibrated with gases of known concentration.
To obtain homogenous samplings, the data were interpolated at 1 s intervals and synchronized through trigger signals at the start of the measurement (Lamarra et al. 1987). Aberrant breaths, caused by, e.g., coughing were identified and deleted if the deviation was greater than four standard deviations of the six surrounding values.
Kinetic analysis
The kinetic analyses followed the description of Hoffmann et al. (2013). The PRBS WR protocol was auto-correlated (ACF) which resulted in a triangular shape and can be interpreted as an approximation of a WR impulse (Bennett et al. 1981). HR, \({\dot{V}}\)O2pulm, and \({\dot{V}}\)O2musc were cross-correlated with the WR protocol (CCF(x)). This resulted in a wave-like form and was interpreted as the response of each parameter to the WR impulse (Fig. 3). A higher maximum of the CCF (CCFmax(x)) describes a faster response of the respective parameter to the change in WR. Therefore, a greater value for CCFmax(\({\dot{V}}\)O2musc) represents a faster kinetics response of the estimated muscular \({\dot{V}}\)O2 response to an increased metabolic demand. A greater time lag of the parameters’ response was indicated by a greater time lag between the maximum of the ACF and the CCF (CCFlag(x)) (Fig. 2). In addition, the entire CCF time courses were analyzed and compared between the groups from lag − 50 s to 150 s in 10 s intervals.

Exemplary response of the parameters to the WR protocol as absolute values (a) and after time series analysis (b). HR heart rate, \({\dot{V}}\text{O}_{2\text{pulm}}\) pulmonary oxygen uptake, \({\dot{V}}\text{O}_{2\text{musc}}\) muscular oxygen uptake, WR work rate, ACF(WR) auto-correlation function of the work rate protocol, CCF cross-correlation function, CCFmax maximum of the cross-correlation function of each respective parameter on the y-axis, CCFlag time lag between the maximum of the ACF and the CCF
\({\dot{V}}\)O2musc kinetics were estimated from \({\dot{V}}\)O2pulm and HR, using a circulatory model, which considers a venous volume as well as \({\dot{V}}\)O2 and perfusion of the non-working part of the body. Applying this method, it is possible to analyze the \({\dot{V}}\)O2pulm (including circulatory distortions) and \({\dot{V}}\)O2musc kinetics separately without excluding certain data from the analyses (Hoffmann et al. 2013).
Peak oxygen uptake
\({\dot{V}}\)O2peak was assumed, in case the subject showed a respiratory exchange ratio of at least 1.05 and HR was above the age-adjusted maximum. The mean \({\dot{V}}\)O2pulm over the last 30 s of the incremental part of the WR protocol was determined as \({\dot{V}}\)O2peak. GET was detected applying the criteria described by Beaver et al. (1986).
Statistical analysis
Differences between the two groups regarding the kinetics parameters, peak values and hours of training were calculated using Mann–Whitney U tests (two-tailed), due to the small sample size. Differences between the groups regarding the different lags of the CCFs were analyzed applying a repeated measures ANOVA with the factors ‘group’ (INT, CONT) and ‘lag’ (− 50 s to 150 s). Mean values of the cardiorespiratory parameters during the PRBS WR protocol were compared between the two groups and the different steps using repeated measures ANOVA with the factors ‘group’ (INT, CONT) and ‘step’ (rest, low, PRBS1, PRBS2, high). In addition, potential differences between \({\dot{V}}\)O2musc and \({\dot{V}}\)O2pulm kinetics (CCFmax and CCFlag) were calculated using repeated measures ANOVA with the factors ‘group’ (INT, CONT) and ‘parameter’ (\({\dot{V}}\)O2musc, \({\dot{V}}\)O2pulm). In case the Mauchly test of sphericity showed significant differences (α ≤ 10%) the Greenhouse–Geisser correction was used. Post hoc effects were calculated using the Bonferroni test. Correlation analyses for HR and HR kinetics were performed using the Spearman rank order correlation coefficient (two-tailed). The level of statistical significance was set to α ≤ 5%.
Results
\({\dot{V}}\)O2peak was significantly higher in the INT group. Relative \({\dot{V}}\)O2peak was not significantly different between the groups. In the INT group, HR at the GET was significantly higher and tended to be higher at peak exercise during the incremental part of the treadmill test. Hours spent for training over the past year were not significantly different between the groups (Table 1).
Comparing the metabolic and cardiac data during the PRBS steps of the treadmill test, differences between the groups were only observed for \({\dot{V}}\)O2pulm and \({\dot{Q}}\), but not for HR or SV. Main effects and post hoc results are shown in Table 2.
Calculating the \({\dot{V}}\)O2pulm as mean value during the two PRBS relative to the \({\dot{V}}\)O2 achieved at GET in percent (%\({\dot{V}}\)O2 GET), there was no statistical difference between INT (73.1 ± 7.3%) and CONT (76.1 ± 7.4%; P = 0.417).
The kinetics parameters, CCFmax(HR), CCFmax(\({\dot{V}}\)O2musc) and CCFmax(\({\dot{V}}\)O2pulm) were significantly greater for CONT compared with INT with no within group differences between CCFmax(\({\dot{V}}\)O2pulm) and CCFmax(\({\dot{V}}\)O2musc) (parameter: P = 0.949; parameter × group: P = 0.864) (Table 3). In addition, CCFlag(\({\dot{V}}\)O2pulm) was significantly greater than CCFlag(\({\dot{V}}\)O2musc) (parameter: P < 0.001; parameter × group: P = 0.117), but there were no differences between the groups (P = 0.118) (Table 3).
The CCF courses for HR, \({\dot{V}}\)O2musc and \({\dot{V}}\)O2pulm in comparison between the two groups are shown in Fig. 3. For the CCF course of \({\dot{V}}\)O2pulm, significant differences were found for the factors lag (P < 0.001), group × lag (P = 0.002) and the factor group (P = 0.032). Similarly, regarding the CCF course of \({\dot{V}}\)O2musc, significant effects for lag (P < 0.001), lag × group (P = 0.001) but not for group (P = 0.574) were calculated. For the CCF course of HR, significant effects for lag (P < 0.001), lag × group (P = 0.020), but not for group (P = 0.350) were calculated. Post hoc, statistical differences between the groups were found at several lags (marked with asterisks in Fig. 3).

Means (± SE) of each 10 s interval of the cross-correlation function between work rate and a pulmonary oxygen uptake (CCF(\({\dot{V}}\)O2pulm)), b heart rate (CCF(HR)) and c muscular oxygen uptake (CCF(\({\dot{V}}\)O2musc)). Sig. significant difference between the groups at the respective lag
A significant correlation was shown between the mean HR during the PRBS and CCFmax(HR) (rSP = − 0.574, P = 0.016).
Discussion
Despite no significant differences in relative \({\dot{V}}\)O2peak, and relative exercise intensities during the kinetics test (%\({\dot{V}}\)O2 GET), \({\dot{V}}\)O2musc, HR as well as \({\dot{V}}\)O2pulm kinetics were significantly faster as assessed by greater CCFmax values, in the CONT compared with the INT training group, which is in line with the hypothesis.
Peak HR, peak respiratory exchange ratio, \({\dot{V}}\)O2 and velocity at GET, %\({\dot{V}}\)O2 GET, hours of training per year (Table 2) as well as HR and SV during the PRBS protocol were not statistically different between the groups (Table 2). Therefore, these factors can be excluded as influencing factors for the significantly different kinetics. However, peak HR (by trend) and HR at GET as well as \({\dot{Q}}\) and \({\dot{V}}\)O2pulm during several steps of the PRBS WR protocol were significantly higher in the INT group (Table 2). The higher HRs at higher exercise intensities may be explained with the younger age of the INT group. The greater \({\dot{Q}}\) and \({\dot{V}}\)O2pulm during several WR steps might be due to the significantly greater body mass and potentially also muscle mass of the INT group.
The comparable relative \({\dot{V}}\)O2peak of the INT and CONT group is in contrast to the results of Berger and Jones (2007) and Do Nascimento Salvador et al. (2016), but in line with those of Kilding et al. (2006, 2007). According to the results, it is considered, that the different training regimes of INT and CONT influence \({\dot{V}}\)O2peak and \({\dot{V}}\)O2 kinetics differently.
The data analysis by Abdelkrim et al. (2010) revealed that basketball players spend 19.3 ± 3.5% of total time of a game in the maximal intensity HR zone, 56.0 ± 6.3% in the high-intensity zone, 17.3 ± 5.5% in the moderate and 7.4 ± 6.1% of total time in the low-intensity zone. Activities during a game vary from sprinting over striding, running, jogging and walking. Smekal et al. (2001) documented frequently changing HRs between 100 min−1 and ~ 160 min−1 during a 70-min tennis game, which is very different to CONT athletes who run mostly at a constant HR during competitive events. Exercise intensities of INT athletes vary between 20.4 and 86.8% of \({\dot{V}}\)O2max (Smekal et al. 2001; compare also Abdelkrim et al. 2010). Therefore, INT athletes train for repetitive, short but high metabolic demands over the duration of the respective game. CONT athletes train for long, rather stable metabolic demands during their competitions. \({\dot{V}}\)O2pulm and \({\dot{V}}\)O2musc kinetics both are faster in CONT compared with INT athletes. Faster \({\dot{V}}\)O2musc kinetics in the CONT group may be explained with different muscle fiber type distributions, which can be assumed in the respective athlete groups. Oxygen extraction depends on enzymatic activity of the corresponding working muscle fibers. ST fibers contain more mitochondria and have a higher oxidative capacity, FT fibers are known to depend more on glycolytic processes. ST fibers are assumed to show faster \({\dot{V}}\)O2 kinetics compared with FT fibers (Crow and Kushmerick 1982). Pringle et al. (2003) found a correlation between phase 2 \({\dot{V}}\)O2 kinetics and the percentage of ST muscle fibers during heavy and severe, but not moderate exercise. It has been observed that muscles of long-distance runners have less FT fibers compared with sprint-trained athletes (Saltin and Gollnick 1983) and that the percentage of FT fibers decreases with the length of the running events, that the individuals participate in (Inbar et al. 1981). In line with this, it is assumed that training with high volume, low velocity and low intensity is favorable for the development of ST fibers and training with low volume but high velocity and high intensity is in favor of FT fiber formation (Kohn et al. 2007; Wilson et al. 2012). In former studies with long-distance runners, distributions of about 63% ST fibers and 37% FT fibers were observed whereas about a distribution of 48% ST and 52% FT fibers were reported for Field Hockey Players (Saltin and Gollnick 1983). Ostojic et al. (2006) estimated a mean of 64.1 ± 9.4% FT fiber content in professional basketball players using assumptions from vertical jumps. Although no muscle biopsy samples were taken and the respective games were not analyzed as in the experiments of Smekal et al. (2001) and Abdelkrim et al. (2010), a higher percentage of FT fibers in INT athletes would be in line with their slower \({\dot{V}}\)O2musc kinetics.
The time lag (CCFlag) was significantly greater for \({\dot{V}}\)O2pulm, which is due to the delayed appearance of the oxygen signal traveling through the venous volume between muscle and mouth. However, no significant differences were found between \({\dot{V}}\)O2pulm and \({\dot{V}}\)O2musc kinetics considering the CCFmax for this treadmill exercise test protocol.
Similar to \({\dot{V}}\)O2musc and \({\dot{V}}\)O2pulm kinetics, the HR kinetics were slower in the INT compared with the CONT group. The slower HR kinetics were most likely caused by the higher absolute mean HR values by trend during the PRBS (Table 2), since the mean HR during the two PRBS correlated negatively with HR kinetics. A higher HR indicates a greater sympathetic nerve activity during exercise, which has been reported to be slower compared with the adjustment of HR by a predominantly decreasing parasympathetic nerve activity (Coote 2010). In the CCF courses of HR (Fig. 3b, lag 80–110 s), a slower return to baseline is visible in the INT group. This might be beneficial during repetitively changing and eventually higher metabolic demands. HR kinetics represent the kinetics of \({\dot{Q}}\) (DeLorey et al. 2004). Therefore, it is speculated that perfusion may be maintained in the formerly working muscle after the end of the metabolic demand. This might be beneficial for the elimination of lactic acid and other metabolites in the muscle and, therefore, a better muscle metabolic baseline for the next increase in work rate intensity. This would be in line with the characteristics of a competitive event for INT athletes.
The results of this experiment are not comparable to those of short-term training interventions. Training interventions with interval or continuous exercise were either shown as similarly effective (Berger et al. 2006; Da Boit et al. 2014; McKay et al. 2009; Murias et al. 2010; Overend et al. 1992) or interval training was even superior to continuous endurance exercise training in accelerating \({\dot{V}}\)O2 kinetics (Daussin et al. 2008; Drescher et al. 2018 [by trend]), although \({\dot{V}}\)O2max changed after both interventions. Over several years, continuous aerobic exercise training seems favorable to speed \({\dot{V}}\)O2 kinetics, compared with interval training as performed by the INT athletes. This might be explained with the formation of a greater percentage of ST fibers in endurance athletes.
Limitations
All subjects were tested using the same WR protocol on the treadmill. According to individual exercise capacity and body mass, the relative intensity of the WR protocol was higher in some cases compared with others. Koppo et al. (2004) found slower \({\dot{V}}\)O2 kinetics in untrained subjects with increasing WR intensity, possibly caused by increased motor unit recruitment. However, %\({\dot{V}}\)O2 GET and the velocity at GET were not significantly different between INT and CONT. Therefore, it can be assumed that the relative intensity of the WR protocol did not cause the differences in the kinetics responses. However, the significantly greater BMI, caused by the greater body mass and height in the INT group is in accordance with the results of Santos et al. (2014), showing different anthropometric characteristics of different groups of athletes. The subjects of the CONT group were older, which might have had an influence on maximal HR, which was lower in the CONT group. Further, age per se was reported not to influence cardiorespiratory kinetics. Physical exercise capacity seems to have a greater influence, as outlined by Grey et al. (2015). In addition, one could have assumed that the maximum oxygen uptake of the CONT athletes would have to be higher compared to the INT athletes. The CONT athletes might have been in a lower performance class, compared to INT. This would further underline the results of INT athletes showing slower kinetics although being in a higher performance class. However, it should be pointed out that it is not possible to reconstruct and compare the detailed training regimes (volume, intensity) of both groups over the past years. In future experiments, it is suggested to analyze teams of the same type of sport and specify the activities during a game as done by Smekal et al. (2001) and Abdelkrim et al. (2010) for a more detailed comparison.
Conclusions
Despite no significant differences in relative \({\dot{V}}\)O2peak, the kinetics of \({\dot{V}}\)O2pulm and \({\dot{V}}\)O2musc were slower in INT compared with the CONT athletes. This might be affected by a higher percentage of ST fibers in the CONT athletes, which were documented to show faster kinetics compared with FT fibers. Although this was not measured in the present experimental setup, it can be concluded, that the ratio of ST and FT muscle fibers in the respective athlete is an important influencing factor for \({\dot{V}}\)O2musc kinetics. It was also shown for the first time that HR kinetics are faster in CONT compared with INT athletes. This is associated with a higher HR in the INT athletes during the test and possibly beneficial for a maintained perfusion of the working muscle during repetitive short metabolic demands. It seems that at least in the long term, high-volume exercise training without the need of changing intensities, as performed in the CONT group, is favorable for fast \({\dot{V}}\)O2 and HR kinetics, compared with the typical team sports training with frequently changing intensities.
Abbreviations
- %\({\dot{V}}\)O2 GET:
-
Oxygen uptake at the gas exchange threshold
- ACF:
-
Auto-correlation function
- CCF:
-
Cross-correlation function
- CCFlag(x):
-
Delay between the maxima of ACF and CCF
- CCFmax(x):
-
Maximum of the CCF between work rate and the respective parameter
- CONT:
-
Individuals performing predominantly long-distance endurance training
- FT:
-
Fast twitch fibers
- GET:
-
Gas exchange threshold
- HR:
-
Heart rate
- INT:
-
Individuals performing predominantly interval-based sports
- PRBS:
-
Pseudo-random binary sequences
- \({\dot{Q}}\) :
-
Cardiac output
- ST:
-
Slow twitch fibers
- SV:
-
Stroke volume
- \({\dot{V}}\)O2max :
-
Maximal oxygen uptake
- \({\dot{V}}\)O2peak :
-
Peak oxygen uptake
- \({\dot{V}}\)O2musc :
-
Muscular oxygen uptake
- \({\dot{V}}\)O2pulm :
-
Pulmonary oxygen uptake
- WR:
-
Work rate
References
Abdelkrim BN, Castagna C, Jabri I, Battikh T, El Fazaa S, Ati JE (2010) Activity profile and physiological requirements of junior elite basketball players in relation to aerobic-anaerobic fitness. J Strength Cond Res 24:2330–2342. https://doi.org/10.1519/JSC.0b013e3181e381c1
Beaver WL, Wasserman K, Whipp BJ (1986) A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 60:2020–2027
Bennett FM, Reischl P, Grodins FS, Yamashiro SM, Fordyce WE (1981) Dynamics of ventilatory responses to exercise in humans. J Appl Physiol Respir Environ Exerc Physiol 51:194–203
Berger NJA, Jones AM (2007) Pulmonary O2 uptake on-kinetics in sprint- and endurance-trained athletes. Appl Physiol Nutr Metab 32:383–393. https://doi.org/10.1139/H06-109
Berger NJA, Tolfrey K, Williams AG, Jones AM (2006) Influence of continuous and interval training on oxygen uptake on-kinetics. Med Sci Sports Exerc 38:504–512. https://doi.org/10.1249/01.mss.0000191418.37709.81
Chilibeck PD, Paterson DH, Smith WD, Cunningham DA (1996) Cardiorespiratory kinetics during exercise of different muscle groups and mass in old and young. J Appl Physiol 81:1388–1394
Coote JH (2010) Recovery of heart rate following intense dynamic exercise. Exp Physiol 95:431–440. https://doi.org/10.1113/expphysiol.2009.047548
Crow MT, Kushmerick MJ (1982) Chemical energetics of slow- and fast-twitch muscles of the mouse. J Gen Physiol 79:147–166. https://doi.org/10.1085/jgp.79.1.147
Da Boit M, Bailey SJ, Callow S, Dimenna FJ, Jones AM (2014) Effects of interval and continuous training on O2 uptake kinetics during severe-intensity exercise initiated from an elevated metabolic baseline. J Appl Physiol 116:1068–1077. https://doi.org/10.1152/japplphysiol.01365.2013
Daussin FN, Zoll J, Dufour SP, Ponsot E, Lonsdorfer-Wolf E, Doutreleau S, Mettauer B, Piquard F, Geny B, Richard R (2008) Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions. Relationship to aerobic performance improvements in sedentary subjects. Am J Physiol Regul Integr Comp Physiol 295:R264–R272. https://doi.org/10.1152/ajpregu.00875.2007
DeLorey DS, Kowalchuk JM, Paterson DH (2004) Effects of prior heavy-intensity exercise on pulmonary O2 uptake and muscle deoxygenation kinetics in young and older adult humans. J Appl Physiol 97:998–1005. https://doi.org/10.1152/japplphysiol.01280.2003
Do Nascimento Salvador PC, Dal Pupu J, de Lucas RD, de Aguiar RA, Arins FB, Guglielmo LGA (2016) The V'O2 kinetics of maximal and supramaximal running exercises in sprinters and middle distance runners. J Strength Cond Res 30:2857–2863
Drescher U, Schefter T, Koschate J, Schiffer T, Brixius K, Schneider S, Hoffmann U (2018) Oxygen uptake kinetics following six weeks of interval and continuous endurance exercise training—an explorative pilot study. Respir Physiol Neurobiol 247:156–166. https://doi.org/10.1016/j.resp.2017.09.015
Fukuoka Y, Grassi B, Conti M, Guiducci D, Sutti M, Marconi C et al (2002) Early effects of exercise training on V′O2 on-and off-kinetics in 50-year-old subjects. Pflüg Arch 443:690–697. https://doi.org/10.1007/s00424-001-0748-y
Grey TM, Spencer MD, Belfry GR, Kowalchuk JM, Paterson DH, Murias JM (2015) Effects of age and long-term endurance training on V′O2 kinetics. Med Sci Sports Exerc 47(2):289–298. https://doi.org/10.1249/MSS.0000000000000398
Hoffmann U, Drescher U, Benson AP, Rossiter HB, Essfeld D (2013) Skeletal muscle V′O2 kinetics from cardio-pulmonary measurements: assessing distortions through O2 transport by means of stochastic work-rate signals and circulatory modelling. Eur J Appl Physiol 113:1745–1754. https://doi.org/10.1007/s00421-013-2598-7
Hughson RL (2009) Oxygen uptake kinetics: historical perspective and future directions. Appl Physiol Nutr Metab 34:840–850. https://doi.org/10.1139/H09-088
Inbar O, Kaiser P, Tesch P (1981) Relationships between leg muscle fiber type distribution and leg exercise performance. Int J Sports Med 2:154–159. https://doi.org/10.1055/s-2008-1034603
Kilding A, Winter E, Fysh M (2006) A comparison of pulmonary oxygen uptake kinetics in middle- and long-distance runners. Int J Sports Med 27:419–426. https://doi.org/10.1055/s-2005-865778
Kilding AE, Fysh M, Winter EM (2007) Relationships between pulmonary oxygen uptake kinetics and other measures of aerobic fitness in middle- and long-distance runners. Eur J Appl Physiol 100:105–114. https://doi.org/10.1007/s00421-007-0413-z
Kohn TA, Essen-Gustavsson B, Myburgh KH (2007) Exercise pattern influences skeletal muscle hybrid fibers of runners and nonrunners. Med Sci Sports Exerc 39:1977–1984. https://doi.org/10.1249/mss.0b013e3181453546
Koppo K, Bouckaert J, Jones AM (2004) Effects of training status and exercise intensity on phase II V′O2 kinetics. Med Sci Sports Exerc 36:225–232. https://doi.org/10.1249/01.MSS.0000113473.48220.20
Lamarra N, Whipp BJ, Ward SA, Wasserman K (1987) Effect of interbreath fluctuations on characterizing exercise gas exchange kinetics. J Appl Physiol 62:2003–2012
McKay BR, Paterson DH, Kowalchuk JM (2009) Effect of short-term high-intensity interval training vs. continuous training on O2 uptake kinetics, muscle deoxygenation, and exercise performance. J Appl Physiol 107:128–138. https://doi.org/10.1152/japplphysiol.90828.2008
Mezzani A, Grassi B, Giordano A, Corra U, Colombo S, Giannuzzi P (2010) Age-related prolongation of phase I of V′O2 on-kinetics in healthy humans. AJP Regul Integr Comp Physiol 299(3):R968–R976. https://doi.org/10.1152/ajpregu.00739.2009
Murias JM, Kowalchuk JM, Paterson DH (2010) Speeding of V′O2 kinetics with endurance training in old and young men is associated with improved matching of local O2 delivery to muscle O2 utilization. J Appl Physiol 108:913–922. https://doi.org/10.1152/japplphysiol.01355.2009
Murias JM, Spencer MD, Paterson DH (2014) The critical role of O2 provision in the dynamic adjustment of oxidative phosphorylation. Exerc Sport Sci Rev 42:4–11
Ostojic SM, Mazic S, Dikic N (2006) Profiling in basketball: physical and physiological characteristics of elite players. J Strength Cond Res 20:740–744
Overend TJ, Paterson DH, Cunningham DA (1992) The effect of interval and continuous training on the aerobic parameters. Can J Sport Sci 17:129–134
Poole DC, Jones AM (2012) Oxygen uptake kinetics. Compr Physiol 2:933–996
Powers SK, Dodd S, Beadle RE (1985) Oxygen uptake kinetics in trained athletes differing in V'O2max. Eur J Appl Physiol 54:306–308
Pringle JSM, Doust JH, Carter H, Tolfrey K, Campbell IT, Sakkas GK, Jones AM (2003) Oxygen uptake kinetics during moderate, heavy and severe intensity “submaximal” exercise in humans. The influence of muscle fibre type and capillarisation. Eur J Appl Physiol 89(3–4):289–300. https://doi.org/10.1007/s00421-003-0799-1
Regensteiner JG, Bauer TA, Reusch JEB, Brandenburg SL, Sippel JM, Vogelsong AM, Smith S, Wolfel EE, Eckel RH, Hiatt WR (1998) Abnormal oxygen uptake kinetics responses in women with type II diabetes mellitus. J Appl Physiol 85:310–317
Saltin B, Gollnick PD (1983) Skeletal muscle adaptability significance for metabolism and performance. In: Peachy LD, Adnan R, Geiger SR (eds) Handbook of physiology section 10: skeletal muscle. The Williams & Wilkins Company, Baltimore, pp 555–631
Santos DA, Dawson JA, Matias CN, Rocha PM, Minderico CS, Allison DB, Sardinha LB, Silva AM (2014) Reference values for body composition and anthropometric measurements in athletes. PLoS ONE 9(5):e97846. https://doi.org/10.1371/journal.pone.0097846
Smekal G, von Duvillard SP, Rihacek C, Pokan R, Hofmann P, Baron R, Tschan H, Bachl N (2001) A physiological profile of tennis match play. Med Sci Sports Exerc 33:999–1005. https://doi.org/10.1097/00005768-200106000-00020
Wilson JM, Loenneke JP, Jo E, Wilson GJ, Zourdos MC, Kim J-S (2012) The effects of endurance, strength, and power training on muscle fiber type shifting. J Strength Cond Res 26:1724–1729
Acknowledgements
This research was supported by a research fund of the German Aerospace Center (DLR e.V.; Grant number 50WB1626). We would like to thank Janosch Wacker for his support during the measurements.
Funding
This research was supported by a research fund of the German Aerospace Center (DLR e.V.; Grant number: 50WB1626).
Author information
Authors and Affiliations
Contributions
JK, UH, LG and VW conceived and designed the research. JK, LG and VW conducted the experiments. UD and UH contributed new analytical thoughts. JK, LG, VW, LT, UD and UH analyzed the data and wrote the manuscript. All the authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by Guido Ferretti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Koschate, J., Gerlich, L., Wirtz, V. et al. Cardiorespiratory kinetics: comparisons between athletes with different training habits. Eur J Appl Physiol 119, 1875–1883 (2019). https://doi.org/10.1007/s00421-019-04176-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-019-04176-9