
Abstract
Purpose
Previous research has indicated greater muscle activation is needed for children (CH) to match relative intensity submaximal contractions in comparison with adults (AD). However, no study has compared motor unit (MU) firing and recruitment patterns between children and adults. Therefore, MU action potential amplitudes (MUAPAMP) and firing rates were examined during two repetitive submaximal contractions of the first dorsal interosseous in children and adults.
Methods
Twenty-two children (age 9.0 ± 0.8 years) and 13 adults (age 22.9 ± 4.8 years) completed three maximum voluntary contractions (MVC) and two repetitive isometric contractions at 30% MVC for 40 s. Surface electromyography (EMG) was recorded and decomposed into action potential trains. MUAPAMPS, recruitment thresholds (RTs), and mean firing rates (MFRs) were calculated, and EMG amplitude was normalized (N-EMG) to MVC. For each subject and repetition, linear MFR vs. RT and exponential MUAPAMP vs. RT and MFR vs. MUAPAMP relationships were calculated.
Results
N-EMG (P = 0.001, CH = 56.5 ± 31.7%, AD = 30.3 ± 9.1%), MFRs regardless of RT, according to greater y-intercepts of the MFR vs. RT relationships [P = 0.013, CH = 31.1 ± 5.1 pulses per second (pps), AD = 25.9 ± 4.3 pps] and MFRs of MUs with smaller action potential amplitudes (P = 0.017, CH = 29.4 ± 6.8 pps, AD = 23.5 ± 3.5 pps), were greater for children. MUAPAMPS in relation with RT were similar between groups except the highest threshold MUs (RT = 28% MVC) were greater for the adults (1.02 ± 0.43 mV) than children (0.67 ± 0.24 mV) (P = 0.010).
Conclusions
Muscle activation and MU firing rates were greater for children, which likely indicated a greater operating point of MU control in comparison with adults during an isometric contraction performed at a relative submaximal intensity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Our previous work (Miller et al. 2018) indicated children may have differing motor unit control strategies in comparison with adults for the first dorsal interosseous (FDI). Normalized electromyographic (EMG) amplitude was greater for children, aged 8–10 years, than what we have previously reported for younger (23 ± 3 years) and older (62 ± 5 years) adults (Miller et al. 2017). Similar isometric muscle actions of the FDI were performed at 50% of maximum voluntary contraction (MVC), where Miller et al. (2018) observed relatively higher normalized EMG amplitude (~ 86%) in children than Miller et al. (2017) reported in the younger (~ 60%) and older (~ 70%) adults. Normalized EMG amplitude serves as a crude indicator of excitatory drive necessary to achieve a relative percentage of MVC (Adam and De Luca 2005; Farina et al. 2010; Keenan et al. 2005; Miller et al. 2017), and it increases with the recruitment of larger motor units, and to a lesser extent, increases in firing rates (Keenan et al. 2005; Martinez Valdes et al. 2018). Investigation of the sizes and firing rates of motor units may provide insight into the greater normalized EMG amplitude observed in children at the same relative %MVCs performed by adults.
Numerous studies have reported greater firing rates for the earlier recruited (lower threshold) than later recruited (higher threshold) MUs (De Luca et al. 1982; Kamen et al. 1995; Masakado et al. 1995; Monster and Chan 1977; Person and Kudina 1972; Tanji and Kato 1973). Specifically, on a subject-by-subject and/or contraction-by-contraction basis the firing rates of the smaller lower threshold motor units achieve greater firing rates than the larger higher threshold motor units regardless of force and time (Adam and De Luca 2005; De Luca et al. 1996; Farina et al. 2009; McGill et al. 2005; Watanabe et al. 2016). Therefore, strong relationships exist between motor unit firing rates and recruitment thresholds during voluntary contractions in young and older adults (Contessa et al. 2016; De Luca and Contessa 2011; Hu et al. 2013b; Miller et al. 2018; Sterczala et al. 2017; Stock et al. 2012). Miller et al. (2018) reported this same general motor unit scheme in young children.
Farina et al. (2009) and Contessa et al. (2016) have provided evidence that changes in motor unit recruitment occur during repetitive voluntary contractions, such as, changes in motor unit recruitment patterns were dependent upon previous activity. For example, Farina et al. (2009) reported slight increases and decreases in the recruitment thresholds of lower and higher threshold motor units during relatively non-fatiguing 10% MVCs of the abductor pollicis brevis. Contessa et al. (2016) observed continued recruitment of larger motor units of the vastus lateralis during repetitive fatiguing 30% MVCs. To date, no study has directly compared motor unit firing and recruitment patterns between children and adults or potential changes in these parameters during repetitive contractions. It is plausible that greater muscle activation requirements to achieve the targeted force for the children may result in differing motor unit control strategies to achieve the targeted force during a subsequent contraction in comparison with adults.
Motor unit action potential amplitude has been correlated with the diameter of the motor unit’s muscle fibers (Hakansson 1956). Therefore, the size principle (Henneman 1957) is evident when motor unit action potential amplitude is regressed against recruitment threshold (Conwit et al. 1999; Goldberg and Derfler 1977; Hu et al. 2013b; Martinez Valdes et al. 2018; Masakado et al. 1994; Miller et al. 2018; Milner-Brown and Stein 1975; Pope et al. 2016; Sterczala et al. 2017). Previously, the motor unit action potential amplitude vs. recruitment threshold relationship has been sensitive to changes in MU specific hypertrophy (Pope et al. 2016) and atrophy (Sterczala et al. 2017). Pope et al. (2016) reported increases in the rate of rise (slopes) of motor unit action potential amplitudes in relation with recruitment thresholds were strongly correlated with increases in the cross-sectional area of the vastus lateralis (muscle fiber hypertrophy) following 8 weeks of lower body resistance training. Whereas, Sterczala et al. (2017) reported the inverse for older adults in comparison with younger adults and suggested muscle fiber atrophy occurred for fibers comprising higher threshold motor units of the FDI for older adults. Trevino et al. (2018) reported cross-sectional area of the vastus lateralis was strongly correlated with the slopes from the motor unit action potential amplitude vs. recruitment threshold relationships of the vastus lateralis, which indicated the rate of rise in motor unit action potential amplitudes in relation with recruitment threshold was much greater for individuals with large muscle cross-sectional areas. Therefore, larger muscle cross-sectional areas of the FDI for adults could correspond with greater rate of rise of motor unit action potential amplitudes in relation with recruitment threshold in comparison with the children.
The purpose of this study is to examine differences in motor unit control strategies (recruitment patterns and firing rates) during two 40 s moderate intensity repetitive contractions (30% MVC) of the FDI between children and adults. Motor unit control strategies will be analyzed via firing rates in relation with recruitment threshold and motor unit action potential amplitude as well as motor unit action potential amplitudes in relation with recruitment threshold along with normalized EMG amplitude at steady force. It is hypothesized that greater normalized EMG amplitude in children could be the result of increased motor unit recruitment and firing rates to achieve the targeted force. Motor unit action potential amplitudes will be smaller in children due to smaller muscle cross-sectional areas. In addition, greater muscle activation requirements to achieve the targeted force level during the 1st contraction could lead to differential responses in motor unit control strategies to sustain the 2nd contraction for children in comparison with adults.
Methods
Compliance with ethical standards
This study was approved by the University Institutional Review Boards for Human Subjects and was conducted according to the Declaration of Helsinki. Child participants provided verbal assent and guardians completed a written informed consent form on their child’s behalf. Adult participants provided written informed consent. All subjects completed a Pre-exercise Testing Health & Exercise Status Questionnaire.
Subjects
Twenty-two healthy children (CH) between the ages of 8 and 10 (12 males age 9.0 ± 0.7 years, stature 140 ± 8 cm, mass 34.7 ± 7.1 kg; and 10 females age 8.9 ± 0.9 years, stature 140 ± 8 cm, mass 33.0 ± 4.0 kg) and 13 adults (AD) (6 males age 21.0 ± 2.5 years, stature 180 ± 6 cm, mass 72.2 ± 5.1 kg; and 7 females age 24.6 ± 5.9 years, stature 165 ± 2 cm, mass 63.3 ± 6.6 kg) participated in this study. Participants reported no current or ongoing neuromuscular diseases or musculoskeletal injuries specific to the hand or wrist.
Research design
The participants visited the laboratory two times separated by at least 24 h. The first visit was a familiarization trial followed by an experimental trial. During the first visit the participants practiced the isometric MVC and submaximal isometric contractions several times. Ultrasonography scans of the FDI were completed during the familiarization trial to determine the muscle cross-sectional area (CSA) and subcutaneous fat.
For the isometric muscle actions, the subject’s right forearm was pronated and positioned on a table with the hand open. The forearm, wrist, and third to fifth fingers were immobilized with a Velcro strap. The thumb was restrained with a strap that held a 90° angle between the index finger and thumb during the isometric contractions. The muscle action of the FDI was isolated and measured by instructing the participants to abduct the index finger against a small flat piece of metal connected to the force transducer (MB-100; Interface, Inc., Scottsdale, AZ). Care was taken to instruct and to ensure the muscle action of the FDI was isolated during all contractions to minimize coactivation. Subjects performed three MVCs with 2 min of rest between each contraction. Strong verbal encouragement was given during the MVCs. The peak force from the three MVCs was used to determine the target force amplitude for two repeated submaximal muscle actions at 30% MVC. For each submaximal isometric muscle action, force was increased at a rate of 10% MVC/s to the target force which was maintained for 40 s and decreased at a rate of 10% MVC/s back to baseline (Fig. 1). Each participant was given only 10 s of rest between the two contractions. During the isometric contractions participants maintained their force output as close as possible to the force template displayed digitally on a computer monitor.

Illustration of the first (a) and second (b) repetitions of the 30% maximal voluntary contractions (MVC). Thick black lines represent the subject’s force tracing. Thin grey lines represent motor unit (MU) mean firing rate [MFR (pulses per second)] curves and dashed grey lines are MUs which were not active for the entire steady force period. The dashed black lines are MFR curves of representative lower recruitment threshold (RT) and higher RT MUs which are further illustrated in the subsequent plots. The subject’s MFR vs. RT (c), MU action potential amplitude (MUAPAMP) vs. RT (d), and MFR vs. MUAPAMP (e) relationships plotted with lines of best fit. Action potential templates of the representative MUs from channels 1 (f) and 2 (g) of the four channels recorded
EMG recording
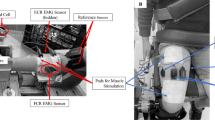
During the muscle actions, surface EMG signals were recorded from the FDI using a 5-pin surface array sensor (Delsys, Inc., Natick, Massachusetts). The diameter of each pin is 0.5 mm that are placed at the corners of a 5 × 5-mm square, with the fifth pin in the center of the square. Before sensor placement, the surface of the skin was prepared by shaving, removing superficial dead skin with adhesive tape, and sterilizing with an alcohol swab. To remove the dead layers of skin, hypoallergenic tape (3M, St. Paul, Minnesota) was applied to the site, then peeled back to remove contaminants (Delsys, Inc., dEMG User Guide). The sensor was placed over the belly of the FDI muscle and secured by adhesive tape. The reference electrode was placed over the elbow of the right arm.
EMG decomposition
Action potentials were extracted into firing events of single MUs from the four separate EMG signals, sampled at 20 kHz, via the precision decomposition III algorithm (version 1.1.0) as described by De Luca et al. (2006). The precision decomposition III algorithm provides four unique action potential waveforms for each EMG channel. Initially, the accuracy of the decomposed firing instances was tested with the reconstruct-and-test procedure (Nawab et al. 2010). Only MUs decomposed with > 90% accuracies were included for analyses. In addition, a secondary spike trigger average (STA) procedure was included to validate the firing times and action potential waveforms generated via the precision decomposition III algorithm. The derived firing times from the precision decomposition III algorithm were used to STA the four raw EMG signals (Hu et al. 2013a, b, c; McManus et al. 2015). A MU was included for further analyses if there were high correlations (r > 0.70) across the four channels between the precision decomposition III algorithm (version 1.1.0) and STA derived action potential waveforms and the coefficient of variation of the STA derived peak-to-peak amplitudes across time was < 0.30 (Hu et al. 2013b). For each MU, recruitment threshold (RT), MU action potential amplitude (MUAPAMP), MU action potential duration (MUAPDUR), and the mean firing rate (MFR) during the steady force plateau were reported. A 2000 ms hanning window was applied to the MU firing instances to create the MFR curves. MUAPAMPS and MUAPDURS were calculated for each MU according to previous methods (Hu et al. 2013b; Miller et al. 2018; Pope et al. 2016; Sterczala et al. 2017), as the average peak-to-peak amplitude values and time elapsed from peak-to-peak, respectively, from each of the four unique action potential waveform templates using a custom-written software program (LabVIEW 2015, National Instruments, Austin, TX, USA). For the 30% MVCs, a linear model was fitted to the MFR (Herda et al. 2015; Miller et al. 2017) and MUAPDUR (Hu et al. 2013b; Milner-Brown and Stein 1975) vs. RT relationships for each subject with the y-intercepts and slopes used for statistical analysis. The following exponential models (Miller et al. 2018; Sterczala et al. 2018) were applied to the MUAPAMP vs. RT and MFR vs. MUAPAMP relationships, respectively:
where A is the theoretical MUAPAMP for a MU recruited at 0% MVC, e is the natural constant, B represents the growth coefficient of MUAPAMP with increments in RT:
where A is the theoretical MFR of a MUAPAMP of 0 mV, and B is the decay coefficient of MFR with increments in MUAPAMP. Pearson product moment correlations were performed to test for significance. Any relationships without an observed recruitment range of MUs > 12% MVC range were excluded from further analysis. MUs that were activated during the steady force were not included in MUAPAMP analysis as the RTs of MUs recruited during the steady force yields the same RT (i.e., 30% MVC). In addition, MUs that were not active during the entire steady force were not included in MFR analysis. These MUs not included for statistical analysis are briefly described in the results and are illustrated in Fig. 1.
Ultrasound experimental protocol
Ultrasound images were taken of the right FDI according to previous methods (Miller et al. 2017; Sterczala et al. 2017) using a LOGIQe ultrasound-imaging device (GE Healthcare UK, Ltd., Chalfont, Buckinghamshire, UK). Subjects were examined while sitting at a table with the right hand lying open and pronated on top of foam pads which form an L-shape. The foam pads were used to elevate the hand from the table as well as provide a guide angle at 70° to standardize the thumb in a relatively neutral position. For each scan ultrasound brightness mode (B-mode), the musculoskeletal preset, and a GE 12L-RS Linear Ultrasound Transducer (5–13 MHz), with a 42 × 7 mm footprint was used. The scan depth was set to 2 cm, gain was 38 dB and transducer frequency was 12 MHz. The origin and insertion of the FDI were located by longitudinally scanning the muscle. The origin and insertion were marked and used to determine the site of the CSA image. The midway point between the origin and insertion was measured and considered the site for the mid CSA. Once the mid CSA site was determined, a cross section of the muscle belly was scanned with the probe oriented perpendicular to the second metacarpal. The second metacarpal was used as a reference for the orientation of the probe as the FDI runs along its lateral side. Generous amounts of ultrasound gel were applied for each scan to ensure minimal pressure on the skin. Images were saved for each subject and exported as a jpg format image to a personal computer for subsequent analysis. Muscle CSA (cm2), and subcutaneous fat (mm) were determined using the image analysis program ImageJ (National Institutes of Health, Bethesda, Maryland). The scale of each image was calibrated using the centimeter marks inlaid in the image. Subcutaneous fat was measured from the bottom of the cutaneous layer to the top of the superficial fascia of the muscle, using the mid-point of the cross section of the muscle as a reference point. The periphery of the muscle was carefully outlined using the polygonal tool and the area was measured as CSA.
Signal processing
Channel 1 of the four bipolar EMG channels from the 5-pin surface array sensor was selected for amplitude analyses. The force (N) and the EMG (mV) signals from channel 1 were recorded with a NI cDAQ (National Instruments, Austin, TX USA) during each isometric muscle action. Data was stored on a personal computer (Dell Optiplex 9010; Dell, Inc., Round Rock, TX) for subsequent analysis. EMG amplitude was expressed as root mean square amplitude values calculated by custom-written software (LabVIEW v 15.0; National Instruments, Austin, TX). The sampling frequency for force and EMG signals was 2000 Hz for the MVCs and 20,000 Hz for the submaximal contractions. The EMG signals were bandpass filtered (zero-phase fourth-order Butterworth filter) at 10–500 Hz, while the force signal was low-pass filtered with a 10-Hz cutoff (zero-phase fourth-order Butterworth filter). All EMG calculations were performed on the filtered signals. MVC force and peak EMG (P-EMG) amplitude were recorded during the highest 0.25 s average of force (N) that occurred during the three MVCs. The EMG amplitude values from the 30% MVC were also normalized (N-EMG) as a percentage of the P-EMG for further analysis. For the 30% MVCs, MFR and N-EMG were analyzed over a 10 s epoch in the middle of the steady force segment for both repetitions 1 and 2.
Statistical analysis
Independent samples t tests were used to analyze possible differences between children and adults for MVC force, P-EMG, CSA, subcutaneous fat, and specific force (MVC/CSA). Independent samples t tests were also performed between groups for repetition 1 for the slopes and y-intercepts from the MFR and MUAPDUR vs. RT relationships, the A and B terms from the MFR vs. MUAPAMP and MUAPAMP vs. RT relationships, and N-EMG to examine differences in MU recruitment and firing rate patterns. Nine separate two-way mixed factorial ANOVAs [group (CH vs. AD) × repetition (1 vs. 2)] were used to analyze the absolute changes in slopes and y-intercepts from the MFR and MUAPDUR vs. RT relationships, the A and B terms from the MFR vs. MUAPAMP and MUAPAMP vs. RT relationships, and N-EMG relative to repetition 1. To further test the hypothesis that MUAPAMPS might be changing as a function of RTs from the first to second repetition (Contessa et al. 2016), predicted MUAPAMPS during the second repetition were normalized to the predicted MUAPAMPS for a given RT during the 1st repetition. Therefore, a two-way mixed factorial ANOVA [group (CH vs. AD) × RT (6% MVC vs. 9% MVC vs. 12% MVC…)] was performed on the absolute change scores from repetition 1 to repetition 2 for the predicted MUAPAMPS in the average range of observed recruitment (6–27% MVC). In addition, paired samples and independent samples t tests were performed as a follow-up to significant interactions where necessary. An α of 0.05 and Benjamini-Hochberg false discovery rate corrections (Benjamini and Hochberg 1995) were used to determine statistical significance. Measures of effect size were calculated using Cohen’s d for t tests, and partial eta squared (η2p) for ANOVAs. Statistical analyses were performed using IBM SPSS Statistics v. 24 (SPSS Inc., Chicago, Illinois, USA).
Results
Eight muscle actions did not meet the RT range inclusionary criteria, leaving 18 children and 10 adults for MU analysis. All MFR vs. RT (r = − 0.762 to − 0.983) relationships were significant. For both, the MUAPAMP vs. RT and MFR vs. MUAPAMP, 57 of 58 relationships were significant (r = 0.580 to 0.965 and − 0.702 to − 0.954, respectively), while the contractions that yielded non-significant relationships were excluded from further analysis (r = − 0.386 to − 0.439).
MUs that were recruited but did not remain active during the entire steady force were observed for 10 of 19 children and 4 of 10 adults. MUs were observed to be derecruited before the steady force was ended (CH = 122 MUs, AD = 24 MUs) with fewer MUs that were both recruited and derecruited during the steady force (CH = 7 MUs, AD = 5 MUs). The MFRs of these MUs were lower than the earlier recruited MUs and, thus, aligned with the onion-skin scheme (De Luca and Erim 1994) (Fig. 1).
The STA procedure resulted in the removal of 85 MUs, and therefore, a total of 1423 MUs were analyzed. For the children, 23.6 ± 7.0 MUs were observed per contraction for a total of 887 MUs. For the adults, 26.6 ± 4.4 MUs were observed per contraction for a total of 536 MUs. RT ranges were similar between groups as the recorded MUs, on average, had RTs from 6.6 ± 4.5 to 27.6 ± 2.9% MVC for the children and from 6.2 ± 2.9 to 28.5 ± 2.1% MVC for the adults.
MUAPAMP vs. RT relationships
The independent samples t test indicated no differences in the A terms for repetition 1 between groups (P = 0.689, d = 0.168). For the changes in A terms relative to repetition 1, there were no significant interactions or main effects (P = 0.192‒0.241, η2p = 0.055‒0.067). For the B terms, the independent samples t test indicated there were no differences between groups for repetition 1 (P = 0.190, d = 0.545). For the change in B terms relative to repetition 1, there were no significant interactions or main effects (P = 0.072‒0.214, η2p = 0.061‒0.124) (Table 1).
For the absolute differences in MUAPAMPS from repetition 1 to repetition 2 for RTs from 6 to 27% MVC, there was a significant two-way interaction (group × RT, P < 0.001). Independent samples t tests indicated the change in MUAPAMP from repetition 1 to repetition 2 at 27% MVC was not significantly different between groups after false discovery rate correction, although the effect size was large (P = 0.034, d = 0.855, CH = − 0.11 ± 0.28 mV, AD = 0.19 ± 0.41 mV), which tentatively suggested a decrease in predicted MUAPAMPS at 27% for children and an increase for adults (Fig. 2).

Average predicted motor unit action potential amplitude [MUAPAMP (mV)] vs. recruitment threshold [RT (%MVC)] relationships for children (CH) and adults (AD) for repetition (REP) 1 and REP 2. The inlaid column scatter plot illustrates the changes (mean ± SD represented by black bars) in MUAPAMPS from REP 1 to REP 2 at RTs of 6 and 27% MVC. Asterisk indicates a significant difference between CH and AD
After further examination of Fig. 2, it appeared MUAPAMPS of the highest threshold MUs (RT = 28% MVC) were greater for the adults (1.02 ± 0.43 mV) than children (0.67 ± 0.24 mV). An additional independent samples t test on the average estimated MUAPAMPS with RTs of 28% MVC (averaged across repetition 1 and 2) confirmed these differences were significant (P = 0.01, d = 1.01).
MUAPDUR vs. RT relationships
Fifty-three of 58 relationships were not significant (r = 0.012‒0.407), but 4 relationships were positively correlated (r = 0.423‒0.569) with 1 relationship being negatively correlated (r = − 0.390). Despite few significant relationships, statistical tests were still performed on the y-intercepts and slopes. Independent samples t tests indicated there were no differences between groups for repetition 1 for the slopes (P = 0.890, d = 0.059) or y-intercepts (P = 0.736, d = 0.147). There were no significant interactions or main effects for the change in slopes (P = 0.401‒0.927, η2p = 0.001‒0.027) or change in y-intercepts (P = 0.335‒0.694, η2p = 0.006‒0.036). The MUAPDURS were similar between children and adults and were not changing between repetition 1 and 2. The MUs were recorded from similar MU depths regardless of RT and did not change from repetition 1 to repetition 2, and therefore, the depth of MUs did not arbitrarily change the recorded MUAPAMPS.
MFR vs. RT relationships
For the slopes, an independent samples t test indicated there were no differences between group for repetition 1 (P = 0.075, d = 0.772). For the change in slope relative to repetition 1, there were no significant interactions or main effects for group or repetition (P = 0.106‒0.111, η2p = 0.095‒0.097) and, thus, the slopes did not change between repetitions for either group. For the y-intercepts, an independent samples t test indicated children were greater than adults for repetition 1 (P = 0.013, d = 1.08). For the change in y-intercepts relative to repetition 1, there were no significant interactions or main effects for group or repetition (P = 0.121‒0.169, η2p = 0.072‒0.090), which indicated the y-intercepts did not change for either group between repetitions (Table 1; Fig. 3).

Average predicted mean firing rate [MFR (pulses per second)] vs. recruitment threshold [RT (%MVC)] relationships for children (CH) and adults (AD) for repetition (REP) 1 and REP 2. The inlaid column scatter plot illustrates the changes (mean ± SD represented by black bars) in MFRs from REP 1 to REP 2 at RTs of 6 and 27% MVC
MFR vs. MUAPAMP relationships
An independent samples t test indicated the A terms were significantly greater for children than adults for repetition 1 (P = 0.017, d = 1.10). For the change in A terms relative to repetition 1, there were no significant interactions or main effects for group or repetition (P = 0.372‒0.375, η2p = 0.032‒0.032), which indicated A terms did not change between repetitions for either group. For the B terms, an independent samples t test indicated no significant difference between groups for repetition 1 (P = 0.131, d = 0.672). For the change in B terms relative to repetition 1 there were no significant interactions or main effects for group or repetition (P = 0.129‒0.774, η2p = 0.003‒0.090), which indicated B terms did not change between repetitions for either group (Table 1; Fig. 4).

Average predicted mean firing rate [MFR (pulses per second)] vs. motor unit action potential amplitude [MUAPAMP (mV)] relationships for children (CH) and adults (AD) for repetition (REP) 1 and REP 2. The inlaid column scatter plot illustrates the changes (mean ± SD represented by black bars) in MFRs from REP 1 to REP 2 for MUs with action potential amplitudes of 0.175, 0.70, and 1.05 mV
Normalized EMG amplitude
An independent samples t test indicated that N-EMG for repetition 1 was significantly greater (P = 0.001, d = 1.12) for children than adults. For the change in N-EMG relative to repetition 1, there were no significant interactions or main effects (P = 0.358‒0.689, η2p = 0.005‒0.026) and, thus, N-EMG did not change for either group between repetitions (Table 1).
Ultrasonography and maximum voluntary contractions
Independent samples t tests indicated the adults possessed significantly greater MVC force (P = 0.002, d = 2.99, CH = 15.6 ± 3.5 N, AD = 23.1 ± 6.6 N), P-EMG (P < 0.001, d = 3.51, CH = 262 ± 134 mV, AD = 595 ± 260 mV), and CSA (Fig. 5) (P < 0.001, d = 9.06, CH = 1.12 ± 0.15 cm2, AD = 2.05 ± 0.39 cm2) than children, whereas the children had greater subcutaneous fat (P = 0.007, d = 1.10, CH = 2.54 ± 0.94 mm, AD = 1.73 ± 0.46 mm) and specific force (P = 0.002, d = 1.09, CH = 14.0 ± 3.1 N/cm2, AD = 11.2 ± 1.8 N/cm2) than adults.

Ultrasound images of the first dorsal interosseous from a child (top), and an adult (bottom). The white outline indicates the cross-sectional area (CSA) of the muscle
Discussion
For MU recruitment and firing rates in children and adults, there were four main findings: (1) greater muscle activation, as measured with N-EMG (Farina et al. 2010), was needed to maintain the target 30% MVC for children than adults; (2) the MFRs in relation with RTs for the children were greater than the adults; (3) the MFRs in relation with MUAPAMPS indicated that the firing rates of only the smaller MUs were greater for the children; and (4) the MUAPAMPS in relation with RT were similar between children and adults; however, the adults did have significantly larger action potential amplitudes of the last recruited MUs within the observed RT range (RTs of 28% MVC). Together, the greater N-EMG and MFRs with similar MUAPAMPS vs. RT relationships suggests children had greater neural drive and a greater percentage of the MU pool activated to sustain the 30% MVC (Contessa and De Luca 2013; Farina et al. 2010).
Presented in Table 1, N-EMG regardless of repetition was greater for children (56.0 ± 29.7%) than adults (31.3 ± 10.3%) which is consistent with previous findings (Grosset et al. 2008; Lambertz et al. 2003). In addition, Farina et al. (2010) suggests firing rates can be considered a measure of neural drive, thus, in the present study the children would have had greater neural drive as indicated by greater N-EMG and higher MFRs regardless of RT. The operating point of the motoneuron pool indicates that an increase in excitation will increase firing rates simultaneously with the recruitment of larger higher threshold MUs (Contessa and De Luca 2013; Contessa et al. 2016). Therefore, children may have performed the contractions at an operating point that was closer to maximal excitation of the motoneuron pool [rightward shift (see Fig. 2 from Contessa and De Luca 2013)] in comparison with the adults, which may provide an explanation for the greater MFRs in children and similar MUAPAMPS between groups.
Previously, Pope et al. (2016) reported that changes in MUAPAMPS were correlated with changes in vastus lateralis CSA pre- to post-resistance training, whereas Sterczala et al. (2017) reported smaller contractile tissue and MUAPAMPS for older than younger individuals of the FDI. More recently, Trevino et al. (2018) reported the slopes from the MUAPAMPS vs. RT relationships accounted for sex-related differences in CSA and percentage of type II myosin heavy chain isoform expression for the vastus lateralis. Together these studies suggest the rate of increase in MUAPAMPS is sensitive to differences in muscle CSA. The similar rate of rise of the MUAPAMPS in relation with RT between children and adults seem to contradict previous findings as the adults had significantly larger CSAs. However, considering the lower firing rates and N-EMG, the adults likely performed the 30% MVCs at a much lower operating point than children. Therefore, the similar MUAPAMP vs. RT relationships are a function of the adults not recruiting relatively larger MUs to achieve the targeted force in comparison with the children. Ultimately, it cannot be concluded that MUAPAMPS are similar between children and adults, it is instead an indication that the level of MU recruitment needed to perform the submaximal contractions for the adults was less than for the children.
There are a few possible explanations for the greater excitation or neural drive needed for the children to sustain the 30% MVC. First, the validity of the MVC may justify the higher N-EMG values. Previous research has questioned children’s ability to reach a true maximal level of contraction (Dotan et al. 2012; Murphy et al. 2014; Ratel et al. 2006). However, this would lead to an arbitrary slight decrease in N-EMG for children due to the non-linear relationship between N-EMG and excitation (Keenan et al. 2005) which contradicts the greater N-EMG observed in children. In addition, specific force was greater for the children than adults providing further support that voluntary effort was high for children. Specific force has been reported to be greater for boys (~ 11 years old) than men in the lateral gastrocnemius (Morse et al. 2008), but similar between children (~ 9 years old) and adults for the quadriceps (O’Brien et al. 2010). Although a mechanism is unclear, it is likely that muscle and methodological differences account for the discrepancies among studies. Greater specific force for the children in the present study could be the result of greater synergist coactivation during the MVC. Contessa et al. (2018) observed increased synergist coactivation as a strategy to maintain force during fatigue caused by repetitive 50% MVCs of the FDI. Great care was taken to minimize synergist coactivation during the isometric muscle actions of the FDI; however, it was not measured in the present study. Nonetheless, N-EMG and specific force provide evidence that the MVC was likely not arbitrarily lower for children. Therefore, children failing to produce a true MVC is not a cofounding factor.
A potential explanation for the higher operating point for children is differential coactivation of antagonist muscles between children and adults. For the FDI, the antagonist muscle (second palmar interosseous) has been reported to be activated in abduction of the index finger (Burnett et al. 2000; Contessa et al. 2018; De Luca et al. 1996). Burnett et al. (2000) reported minimal second palmer interosseous coactivation in young adults, but significantly greater coactivation in older subjects. For children, Grosset et al. (2008) observed greater activation of the triceps surae and coactivation of the antagonist, tibialis anterior, in children than adults during a 25% MVC of the plantar flexors. This increased antagonist coactivation was observed alongside decreased neuromuscular efficiency, which was the ratio of torque to agonist EMG amplitude, during both maximal and submaximal contractions in children. Therefore, it could be speculated that the greater operating point for the FDI in children could at least be partially due to greater antagonist coactivation during submaximal contractions causing decreased neuromuscular efficiency (Grosset et al. 2008; Lambertz et al. 2003). Unfortunately, activation of the second palmer interosseous could not be feasibly measured in the children as invasive intramuscular electrodes are required for EMG analysis of muscles that are not superficial.
Future studies should examine the effects of coactivation during plantar flexion contractions on the operating point of motor unit control in children vs. adults. Use of the plantar flexors is advantageous in that coactivation of the primary antagonist, the tibialis anterior, has been shown to be increased for children and can be measured noninvasively (Grosset et al. 2008; Lambertz et al. 2003). The effects of motor learning through repeated practice of the muscle action or through resistance training should be examined as potential modalities for counteracting the increased coactivation in children. In addition, potential differences between children and adults in motor cortex and/or motor neuron excitability, which are known to affect MU activity (McNeil et al. 2013), warrant further investigation.
Different MU recruitment strategies were used to complete the repetitive contractions between children and adults as indicated by the MUAPAMP analyses. For children, an unexpected finding was that the recruited higher threshold MUs were slightly smaller for repetition 2 in comparison with repetition 1. Although not significant, a large effect size (d = 0.855) indicated action potential amplitudes of MUs recruited at 27% MVC may have been larger during repetition 1 than 2. This suggests some of the largest highest threshold MUs active during repetition 1 were recruited at later forces or not recruited at all during repetition 2. In contrast, the adults relied on recruitment of larger MUs to complete repetition 2 (Figs. 2, 6).

Illustration of the changes in recruitment threshold [RT (%MVC)] from repetition 1 to repetition 2 for motor units (MU) with similar action potential amplitudes [MUAPAMP (mV)]. Black lines are force tracings from the ramp-up phase for a child for repetition 1 (a) and repetition 2 (b) and for an adult for repetition 1 (c) and repetition 2 (d). Grey circles represent the moment during the ramp-up when a MU was recruited. Mean firing rates [MFR (pulses per second)] are also presented for each MU
Recruitment of larger MUs to complete subsequent contractions has been previously observed in the vastus lateralis of adults during repetitive 30% MVCs to exhaustion (Contessa et al. 2016). In the current study, the increase in MU recruitment for repetition 2 for the adults was observed in the absence of significant increases in MFRs from repetition 1 to 2. The first repetitive contraction was held for 40 s and likely resulted in decreased twitch forces of the active MUs. Therefore, additional recruitment of larger higher threshold MUs was necessary to reach and sustain the targeted force during repetition 2 for the adults. Although these contractions were not performed until task failure (fatigue), the MU recruitment patterns for adults in response to repetitive contractions align with the results and conclusions provided by Contessa et al. (2016).
For the children, an alternate explanation is needed for the smaller MUs observed at higher recruitment thresholds for repetition 2 than 1. It is reported children potentiate to the same extent as adults (Paasuke et al. 2000). Potentiation is the increase in twitch force of a MU as a result of recent or previous activity (Hodgson et al. 2005). In theory, potentiation of twitch forces would decrease the number of required MUs to complete repetition 2. However, this phenomenon did not occur for the adults and, therefore, probably did not occur for the children. In addition, the lack of changes in N-EMG and firing rates between repetitions would contrast what would be expected if potentiation occurred based on previous research (Adam and De Luca 2005; Contessa et al. 2016; De Luca et al. 1996; Dorfman et al. 1990).
Another possible explanation is that the amount of coactivation of the antagonist and synergist muscles may have changed from repetition 1 to 2 for the children. If a decrease in coactivation of the antagonist and/or increase in coactivation of the synergist muscles occurred the operating point of the FDI would shift to the left during repetition 2 and result in a decrease in the recruitment of large MUs and the firing rates of the active MUs. There were significantly smaller MUAPAMPS of the higher threshold MUs at the same relative RTs (> 25% MVC) during repetition 2 suggesting that the operating point did shift slightly to the left. This potential effect, however, was not large as indicated by similar N-EMG and firing rates during repetition 1 and 2. Further research is necessary to confirm, and to understand mechanisms responsible for, decreased MU recruitment in children during a subsequent contraction.
While not statistically significant, the changes in the slopes and y-intercepts of the MFR vs. RT relationships for the children might be interpreted as slight decreases in firing rates of the lower threshold with increases in firing rates for the higher threshold MUs from repetition 1 to 2. However, these minor changes are a result of altered recruitment patterns rather than changes in the firing rates of the recorded MUs. The examination of MFRs as a function of MUAPAMP (i.e., serves as a constant) is method to account for the well documented decreases in recruitment thresholds that occur with fatigue (Adam and De Luca 2005; Contessa et al. 2016; de Ruiter et al. 2005; McManus et al. 2015) providing a clearer understanding of firing rate changes between repetitions. However, motor unit action potential shapes have been shown to change with fatigue, such as decreasing MUAPAMP and increasing MUAPDUR when MUs are tracked across multiple fatiguing contractions (Klein et al. 2006; Sandercock et al. 1985). For the current study there was no change in MUAPDUR between repetitions 1 and 2, thus it is unlikely the shape of action potentials changed significantly between repetitions, indicating the action potential amplitudes of single MUs were constant between repetitions. The MFR vs. MUAPAMP relationships were unaltered which indicates firing rates did not change from repetitions 1 to 2 (Fig. 4). Contessa et al. (2016) speculated that increases in firing rates for a MU would occur simultaneously with increased MU recruitment during repetitive submaximal contractions performed to fatigue. The current protocol was not performed until fatigue which is a likely explanation for no significant increases in firing rates for a given MU. Nevertheless, changes in recruitment patterns were observed from repetition 1 to 2 without any significant changes in firing rates.
Conclusions
Children performed the 30% MVCs at a higher operating point in comparison with adults as supported by the greater N-EMG and MFRs. Consequently, since children had greater overall recruitment, the MUAPAMPS were more similar than expected between children and adults; however, adults did have larger MUs recruited at 28% MVC. Although antagonist coactivation was not measured in the current study, previous research suggests it could be a factor that explains the greater operating point of motor control of the FDI for the children. In addition, adults recruited larger MUs, but children relied on smaller MUs to complete the second repetition which suggests differences in MU recruitment patterns from repetition 1 to repetition 2 between adults and children. Future research is needed to confirm the role of antagonist coactivation for the higher operating point observed in children and the role of modulating synergist and antagonist activation during repetitive contractions that may have caused the differential recruitment response to the second repetition in children.
Abbreviations
- AD:
-
Adults
- CH:
-
Children
- CSA:
-
Cross-sectional area
- EMG:
-
Electromyography
- FDI:
-
First dorsal interosseous
- MFR:
-
Mean firing rate
- MU:
-
Motor unit
- MUAPAMP :
-
Motor unit action potential amplitude
- MUAPDUR :
-
Motor unit action potential duration
- MVC:
-
Maximum voluntary contraction
- N-EMG:
-
Normalized electromyographic amplitude
- P-EMG:
-
Peak electromyographic amplitude
- REP:
-
Repetition
- RT:
-
Recruitment threshold
- STA:
-
Spike trigger average
References
Adam A, De Luca CJ (2005) Firing rates of motor units in human vastus lateralis muscle during fatiguing isometric contractions. J Appl Physiol (1985) 99:268–280. https://doi.org/10.1152/japplphysiol.01344.2004
Benjamini Y, Hochberg Y (1995) Controlling the false discovery rate—a practical and powerful approach to multiple testing. J R Stat Soc B 57:289–300
Burnett RA, Laidlaw DH, Enoka RM (2000) Coactivation of the antagonist muscle does not covary with steadiness in old adults. J Appl Physiol (1985) 89:61–71. https://doi.org/10.1152/jappl.2000.89.1.61
Contessa P, De Luca CJ (2013) Neural control of muscle force: indications from a simulation model. J Neurophysiol 109:1548–1570. https://doi.org/10.1152/jn.00237.2012
Contessa P, De Luca CJ, Kline JC (2016) The compensatory interaction between motor unit firing behavior and muscle force during fatigue. J Neurophysiol 116:1579–1585. https://doi.org/10.1152/jn.00347.2016
Contessa P, Letizi J, De Luca G, Kline JC (2018) Contribution from motor unit firing adaptations and muscle co-activation during fatigue. J Neurophysiol. https://doi.org/10.1152/jn.00766.2017
Conwit RA, Stashuk D, Tracy B, McHugh M, Brown WF, Metter EJ (1999) The relationship of motor unit size, firing rate and force. Clin Neurophysiol 110:1270–1275
De Luca CJ, Contessa P (2011) Hierarchical control of motor units in voluntary contractions. J Neurophysiol 107:178–195. https://doi.org/10.1152/jn.00961.2010
De Luca CJ, Erim Z (1994) Common drive of motor units in regulation of muscle force. Trends Neurosci 17:299–305
De Luca CJ, LeFever RS, McCue MP, Xenakis AP (1982) Behaviour of human motor units in different muscles during linearly varying contractions. J Physiol 329:113–128
De Luca CJ, Foley PJ, Erim Z (1996) Motor unit control properties in constant-force isometric contractions. J Neurophysiol 76:1503–1516
de Ruiter CJ, Elzinga MJ, Verdijk PW, van Mechelen W, de Haan A (2005) Changes in force, surface and motor unit EMG during post-exercise development of low frequency fatigue in vastus lateralis muscle. Eur J Appl Physiol 94:659–669. https://doi.org/10.1007/s00421-005-1356-x
De Luca CJ, Adam A, Wotiz R, Gilmore LD, Nawab SH (2006) Decomposition of surface EMG signals. J Neurophysiol 96:1646–1657. https://doi.org/10.1152/jn.00009.2006
Dorfman LJ, Howard JE, McGill KC (1990) Triphasic behavioral response of motor units to submaximal fatiguing exercise. Muscle Nerve 13:621–628. https://doi.org/10.1002/mus.880130711
Dotan R, Mitchell C, Cohen R, Klentrou P, Gabriel D, Falk B (2012) Child-adult differences in muscle activation—a review. Pediatr Exerc Sci 24:2–21
Farina D, Holobar A, Gazzoni M, Zazula D, Merletti R, Enoka RM (2009) Adjustments differ among low-threshold motor units during intermittent, isometric contractions. J Neurophysiol 101:350–359. https://doi.org/10.1152/jn.90968.2008
Farina D, Holobar A, Merletti R, Enoka RM (2010) Decoding the neural drive to muscles from the surface electromyogram. Clin Neurophysiol 121:1616–1623. https://doi.org/10.1016/j.clinph.2009.10.040
Goldberg LJ, Derfler B (1977) Relationship among recruitment order, spike amplitude, and twitch tension of single motor units in human masseter muscle. J Neurophysiol 40:879–890
Grosset JF, Mora I, Lambertz D, Perot C (2008) Voluntary activation of the triceps surae in prepubertal children. J Electromyogr Kinesiol 18:455–465. https://doi.org/10.1016/j.jelekin.2006.11.002
Hakansson CH (1956) Conduction velocity and amplitude of the action potential as related to circumference in the isolated fibre of frog muscle. Acta Physiol Scand 37:14–34. https://doi.org/10.1111/j.1748-1716.1956.tb01338.x
Henneman E (1957) Relation between size of neurons and their susceptibility to discharge. Science 126:1345–1347
Herda TJ, Siedlik JA, Trevino MA, Cooper MA, Weir JP (2015) Motor unit control strategies of endurance- versus resistance-trained individuals. Muscle Nerve 52:832–843. https://doi.org/10.1002/mus.24597
Hodgson M, Docherty D, Robbins D (2005) Post-activation potentiation: underlying physiology and implications for motor performance. Sports Med 35:585–595
Hu X, Rymer WZ, Suresh NL (2013a) Assessment of validity of a high-yield surface electromyogram decomposition. J Neuroeng Rehabil 10:99. https://doi.org/10.1186/1743-0003-10-99
Hu X, Rymer WZ, Suresh NL (2013b) Motor unit pool organization examined via spike-triggered averaging of the surface electromyogram. J Neurophysiol 110:1205–1220. https://doi.org/10.1152/jn.00301.2012
Hu X, Rymer WZ, Suresh NL (2013c) Reliability of spike triggered averaging of the surface electromyogram for motor unit action potential estimation. Muscle Nerve 48:557–570. https://doi.org/10.1002/mus.23819
Kamen G, Sison SV, Du CC, Patten C (1995) Motor unit discharge behavior in older adults during maximal-effort contractions. J Appl Physiol (1985) 79:1908–1913
Keenan KG, Farina D, Maluf KS, Merletti R, Enoka RM (2005) Influence of amplitude cancellation on the simulated surface electromyogram. J Appl Physiol (1985) 98:120–131. https://doi.org/10.1152/japplphysiol.00894.2004
Klein CS, Hager-Ross CK, Thomas CK (2006) Fatigue properties of human thenar motor units paralysed by chronic spinal cord injury. J Physiol 573:161–171. https://doi.org/10.1113/jphysiol.2005.103044
Lambertz D, Mora I, Grosset JF, Perot C (2003) Evaluation of musculotendinous stiffness in prepubertal children and adults, taking into account muscle activity. J Appl Physiol (1985) 95:64–72. https://doi.org/10.1152/japplphysiol.00885.2002
Martinez Valdes E, Negro F, Falla D, De Nunzio AM, Farina D (2018) Surface EMG amplitude does not identify differences in neural drive to synergistic muscles. J Appl Physiol (1985). https://doi.org/10.1152/japplphysiol.01115.2017
Masakado Y, Noda Y, Nagata MA, Kimura A, Chino N, Akaboshi K (1994) Macro-EMG and motor unit recruitment threshold: differences between the young and the aged. Neurosci Lett 179:1–4
Masakado Y, Akaboshi K, Nagata M, Kimura A, Chino N (1995) Motor unit firing behavior in slow and fast contractions of the first dorsal interosseous muscle of healthy men. Electroencephalogr Clin Neurophysiol 97:290–295
McGill KC, Lateva ZC, Marateb HR (2005) EMGLAB: an interactive EMG decomposition program. J Neurosci Methods 149:121–133. https://doi.org/10.1016/j.jneumeth.2005.05.015
McManus L, Hu X, Rymer WZ, Lowery MM, Suresh NL (2015) Changes in motor unit behavior following isometric fatigue of the first dorsal interosseous muscle. J Neurophysiol 113:3186–3196. https://doi.org/10.1152/jn.00146.2015
McNeil CJ, Butler JE, Taylor JL, Gandevia SC (2013) Testing the excitability of human motoneurons. Front Hum Neurosci 7:152. https://doi.org/10.3389/fnhum.2013.00152
Miller JD, Herda TJ, Trevino MA, Sterczala AJ, Ciccone AB, Nicoll JX (2017) Age-related differences in twitch properties and muscle activation of the first dorsal interosseous. Clin Neurophysiol 128:925–934. https://doi.org/10.1016/j.clinph.2017.03.032
Miller JD, Sterczala AJ, Trevino MA, Herda TJ (2018) Examination of muscle composition and motor unit behavior of the first dorsal interosseous of normal and overweight children. J Neurophysiol 119:1902–1911. https://doi.org/10.1152/jn.00675.2017
Milner-Brown HS, Stein RB (1975) The relation between the surface electromyogram and muscular force. J Physiol 246:549–569
Monster AW, Chan H (1977) Isometric force production by motor units of extensor digitorum communis muscle in man. J Neurophysiol 40:1432–1443. https://doi.org/10.1152/jn.1977.40.6.1432
Morse CI, Tolfrey K, Thom JM, Vassilopoulos V, Maganaris CN, Narici MV (2008) Gastrocnemius muscle specific force in boys and men. J Appl Physiol (1985) 104:469–474. https://doi.org/10.1152/japplphysiol.00697.2007
Murphy JR, Button DC, Chaouachi A, Behm DG (2014) Prepubescent males are less susceptible to neuromuscular fatigue following resistance exercise. Eur J Appl Physiol 114:825–835. https://doi.org/10.1007/s00421-013-2809-2
Nawab SH, Chang SS, De Luca CJ (2010) High-yield decomposition of surface EMG signals. Clin Neurophysiol 121:1602–1615. https://doi.org/10.1016/j.clinph.2009.11.092
O’Brien TD, Reeves ND, Baltzopoulos V, Jones DA, Maganaris CN (2010) In vivo measurements of muscle specific tension in adults and children. Exp Physiol 95:202–210. https://doi.org/10.1113/expphysiol.2009.048967
Paasuke M, Ereline J, Gapeyeva H (2000) Twitch contraction properties of plantar flexor muscles in pre- and post-pubertal boys and men. Eur J Appl Physiol 82:459–464. https://doi.org/10.1007/s004210000236
Person RS, Kudina LP (1972) Discharge frequency and discharge pattern of human motor units during voluntary contraction of muscle. Electroencephalogr Clin Neurophysiol 32:471–483
Pope ZK, Hester GM, Benik FM, DeFreitas JM (2016) Action potential amplitude as a noninvasive indicator of motor unit-specific hypertrophy. J Neurophysiol 115:2608–2614. https://doi.org/10.1152/jn.00039.2016
Ratel S, Duche P, Williams CA (2006) Muscle fatigue during high-intensity exercise in children. Sports Med 36:1031–1065
Sandercock TG, Faulkner JA, Albers JW, Abbrecht PH (1985) Single motor unit and fiber action potentials during fatigue. J Appl Physiol (1985) 58:1073–1079. https://doi.org/10.1152/jappl.1985.58.4.1073
Sterczala AJ, Herda TJ, Miller JD, Ciccone AB, Trevino MA (2017) Age-related differences in the motor unit action potential size in relation to recruitment threshold. Clin Physiol Funct Imaging. https://doi.org/10.1111/cpf.12453
Sterczala AJ, Miller JD, Trevino MA, Dimmick HL, Herda TJ (2018) Differences in the motor unit firing rates and amplitudes in relation to recruitment thresholds during submaximal contractions of the first dorsal interosseous between chronically resistance trained and physically active men. Appl Physiol Nutr Metab. https://doi.org/10.1139/apnm-2017-0646
Stock MS, Beck TW, Defreitas JM (2012) Effects of fatigue on motor unit firing rate versus recruitment threshold relationships. Muscle Nerve 45:100–109. https://doi.org/10.1002/mus.22266
Tanji J, Kato M (1973) Firing rate of individual motor units in voluntary contraction of abductor digiti minimi muscle in man. Exp Neurol 40:771–783
Trevino MA et al (2018) Sex-related differences in muscle size explained by amplitudes of higher-threshold motor unit action potentials and muscle fiber typing. Acta Physiol. https://doi.org/10.1111/apha.13151
Watanabe K, Holobar A, Kouzaki M, Ogawa M, Akima H, Moritani T (2016) Age-related changes in motor unit firing pattern of vastus lateralis muscle during low-moderate contraction. Age 38:1–14
Acknowledgements
We would like to thank the undergraduate students who assisted in the collection of data, as well as each of the subjects for their selfless participation.
Funding
This study was supported financially by the National Strength and Conditioning Association Foundation’s Graduate Research Grant (#0000010446) and by the University of Kansas via the General Research Fund (GRF 2301166-RSC).
Author information
Authors and Affiliations
Contributions
TJH and JDM conceived and designed the study. JDM, AJS, HLD, MEW, and MAT collected and analyzed the data. All authors interpreted the results. JDM prepared the first draft of the manuscript and figures. All authors edited the figures and manuscript. All authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed. All experiments were performed in the University of Kansas Neuromechanics Laboratory.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest, financial or otherwise.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the University Institutional Review Boards for Human Subjects and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Communicated by Toshio Moritani.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Miller, J.D., Sterczala, A.J., Trevino, M.A. et al. Motor unit action potential amplitudes and firing rates during repetitive muscle actions of the first dorsal interosseous in children and adults. Eur J Appl Physiol 119, 1007–1018 (2019). https://doi.org/10.1007/s00421-019-04090-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-019-04090-0