
Abstract
To evaluate differences in total haemoglobin mass (tHb mass) and in red blood cell profile between elite endurance-trained (END) and non-endurance-trained (nEND) male and female adolescent athletes, tHb mass (CO rebreathing) and specific variables of red blood cell profile (haemoglobin concentration, haematocrit, erythrocyte indices) were determined in 59 elite junior athletes (29 END, 30 nEND). We hypothesized that at the age of 15–17 years, regular endurance training might induce a significant increase in tHb mass and changes in red blood cell profile. Therefore, all parameters were again determined after 6, 12 and 18 months in a subset of 27 subjects (17 END, 10 nEND). In END, tHb mass related to body weight was ~15% greater than in nEND (11.2 ± 1.6 vs. 9.7 ± 1.3 g kg−1, P < 0.001), whereas no significant differences were observed for the red blood cell profile. In both groups, tHb mass related to body weight and the variables of red blood cell profile had not changed significantly after 6, 12 and 18 months of regular training. In conclusion, in elite junior athletes, differences in tHb mass between END and nEND were similar, however, smaller compared with previously in adult athletes reported values. At the age of 15–17 years, 18 months of regular training did not induce significant changes in tHb mass beyond alterations explained by physical growth and also variables of red blood cell profile did not change significantly.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total haemoglobin mass (tHb mass) is a key determinant for aerobic capacity with strong positive correlations between tHb mass and VO2max in adults (Brotherhood et al. 1975; Gore et al. 1997; Heinicke et al. 2001; Martino et al. 2002; Schmidt and Prommer 2008). Significantly greater tHb mass has been observed in endurance-trained versus non-endurance-trained athletes and versus untrained subjects, respectively (Heinicke et al. 2001; Kjellberg et al. 1949; Schmidt and Prommer 2008). In endurance-trained adult athletes with high aerobic performance capacity, physiological variations in tHb mass during regular training are small (Garvican et al. 2010; Gore et al. 1997; Prommer et al. 2008; Schmidt and Prommer 2008). Increases in tHb mass, however, were reported as a physiological response to the onset of regular endurance training in untrained subjects (Schmidt and Prommer 2008) as well as to altitude training (reviewed by Schmidt and Prommer 2008) or as the result of blood doping (Lundby et al. 2007; Mørkeberg et al. 2009; Parisotto et al. 2000; Pottgiesser et al. 2007). tHb mass in adolescent athletes has only scarcely been investigated. Koch and Röcker (1977) reported higher plasma volume and estimated higher tHb masses in 14–15 years old well-trained boys when compared with reference values from untrained boys. To our knowledge, there is only one study which investigated longitudinal changes in tHb mass in young athletes. Eastwood et al. (2009) reported a significant increase in tHb mass in twelve 11 to 15-year-old male and female cyclists after 1 year of regular training, however, related to body weight, this change was not significant. With regard to the close relationship between aerobic capacity and tHb mass, the development of tHb mass in adolescent athletes is of great interest. It is well known that aerobic capacity in young trained subjects is higher when compared with untrained subjects at all ages, whilst the greatest difference is found during adolescence (Armstrong and Welsman 2001). The greatest effects of regular endurance training on aerobic capacity, beyond the effects explained by growth and maturation, have so far been observed in male adolescents during the late pubertal stage (Armstrong and Welsman 2001; Eisenmann et al. 2001), however, not much is known about the development of tHb mass and red blood cell profile at this age.
The development of tHb mass as well as of erythropoietic markers in adolescent athletes is also important concerning anti-doping regulations. Markers of red blood cell profile have already been part of anti-doping controls in junior athletes (Mayr et al. 2006). In the year 2010, the World Anti-Doping Agency (WADA 2010) released operational guidelines for implementing the athlete biological passport for anti-doping screenings and several markers of the red blood cell profile were selected for the haematological module. tHb mass has also been discussed as a marker (Gore et al. 2006; Pottgiesser et al. 2007; Prommer et al. 2008), but it has not been included in the biological passport so far. It was recommended to start with the blood pass several years before the athletes will participate in international competitions (e.g. during adolescence) (Berglund et al. 2007). Therefore, it is essential to know if and to what extent markers of the red blood cell system change during adolescence in elite junior athletes.
In a cross-sectional analysis, we evaluated differences in tHb mass and variables of red blood cell profile between endurance-trained and non-endurance-trained male and female elite junior athletes. A subset of these athletes was followed over an 18-month training period to test the hypothesis that elite adolescent athletes show an enhancement of tHb mass at the age of 15–17 years as a response to ongoing endurance training. We also monitored selected blood profile markers to test for alterations reflecting developmental changes during the 18-month observation period.
Materials and methods
Study design
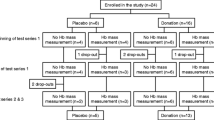
The study consists of a cross-sectional analysis of tHb mass and markers of red blood cell profile in 59 elite adolescent athletes and of a longitudinal analysis of these variables in a subset of 27 athletes. In the longitudinal analysis, tHb mass, red blood cell profile, and performance at the 4 mmol l−1 lactate threshold (4 LT) were determined in 6-month intervals at four time points (T1–T4) resulting in a monitoring phase of 18 months.
Subjects
Fifty-nine adolescent elite athletes volunteered to participate in the present study (anthropometric data in Table 1). Written parental consent was obtained before any testing. The study was approved by the Ethics Committee of the Medical Faculty of the University of Heidelberg, Germany, and conformed to the standards set by the Declaration of Helsinki. All subjects were competing at top national levels in their age class and were members of German youth elite teams, including basketball (17 females), canoeing (8 males and 4 females), tennis (1 male and 1 female), weight lifting (10 males and 1 female), swimming (5 males and 4 females), and distance running (5 males and 3 females). Athletes from canoeing, swimming and distance running were considered as one group (endurance-trained, END), because endurance-type training is the major part of their training regime (>60–70% of all training all year round), in contrast to athletes from basketball, tennis and weight lifting (non-endurance-trained, nEND), where <10–20% of all-year training is designed as endurance-type training. As anthropometric characteristics, body height, body weight, and fat free mass (FFM) were determined. FFM was calculated from estimation of body fat by skinfold measurements performed at three sites [triceps, subscapular, and abdomen (thigh in female athletes)] with a skinfold caliper (Holtain, Crymych, UK) as described by Lohman (1981) and Wagner (1996). Overall, 14 athletes (10 females and 4 males, 6 END and 10 nEND) were iron depleted and in 2 nEND female athletes, mild iron-deficient anaemia occurred (serum ferritin 14 μg l−1, [Hb]: 11.8 g dl−1 and serum ferritin: 4 μg l−1, [Hb]: 11.1 g dl−1, respectively).
Longitudinal observation
Longitudinal monitoring could be done in a subset of 27 out of the 59 athletes (14 males and 13 females, 17 END, 10 nEND, anthropometric data in Table 2). All the 27 athletes trained regularly and answered questions concerning their training programme at all time points (T1–T4) when they reported to our laboratory for the scheduled tests (Table 3). None of the subjects participated in altitude or hypoxia training during the observation phase. Generally, we knew all the subjects and their coaches very well as they regularly trained at the local Olympic Training Centre and we can exclude the possibility of blood manipulations. The subjects were non-smokers, except for one weight lifter. To avoid acute interference with percent carboxyhaemoglobin (%HbCO) measurements within carbon monoxide rebreathing (COR), this weight lifter was asked not to smoke before the investigations at the testing day.
Nine subjects (7 females and 2 males, 6 END and 3 nEND) from the longitudinal monitoring were iron depleted (serum ferritin <20 μg l−1) at T1. These athletes received oral iron supplementation (100 mg of ferrous sulphate daily). No iron-deficient anaemia ([Hb] <12 g dl−1) was detected in any of these athletes. As changes in tHb mass in the iron-depleted, iron-treated athletes were not significantly different from the tHb mass changes observed in the athletes without iron deficiency [similar to our observation in a previous study (Friedmann et al. 2001)] the respective athletes were included into further analysis.
Exercise testing
The elite junior athletes are regularly subjected to performance tests in their different sports, i.e. basketball: 5–6 × 1,200 m field test on a 400-m track, canoeing: 4 × 1,000 m canoeing on a lake, weight lifting: stepwise increasing test on a cycle ergometer (increments: 50 W, step duration 3 min), swimming: stepwise increasing swimming test in a pool (5–8 × 100–400 m), distance running and tennis: stepwise increasing treadmill test (increments: 2 km h−1, step duration 3 min). In all these tests, lactate is determined in capillary blood drawn from the earlobe at the end of each exercise step and performance at 4 mmol l−1 lactate concentration (4 LT) is determined as a critical intensity. Although we are well aware of the limitations of this method, many coaches still rely on 4 LT to monitor submaximal performance and for training recommendations. In the present study, it was not possible to measure VO2max in all the athletes from the different sports, but the above-mentioned tests were performed at T1–T4 and 4 LT was determined (lactate measurement with an automated device, Biosen S-line, EKF Diagnostic, Barleben Germany). To monitor and compare the performance development at 4 LT, performance at 4 LT at the first test (T1) was set as 100% and performance at 4 LT at T2, T3, and T4 was related to the performance at 4 LT at T1.
tHb mass assessment
tHb mass was assessed using CO rebreathing (COR) as described in detail by Schmidt and Prommer (2005) and modified by Prommer and Schmidt (2007). In brief, after 15-min resting in a semi-upright position, the athletes were connected to a specially designed closed spirometric system allowing a CO-bolus application followed by 2 min rebreathing of a small amount of oxygen. The administered amount of CO in mL was individually calculated [mL CO = 0.8 × body weight (kg, males) and mL CO = 0.7 × body weight (kg, females), respectively]. During CO rebreathing, the whole apparatus was checked for CO leakage with a portable CO-gas analyser (Fluke, CO-220, Everett, WA, USA). This analyser was also used to calculate the amount of CO which had not been taken up by the body from the remaining CO in the spirometer and the residual volume of the lung as well as from the CO exhaled after disconnecting the athlete from the spirometer. Blood samples were drawn from an antecubital vein via a cannula (20GA, Beckton Dickinson Venflon™ Pro Safety) immediately before, 6 and 8 min after the start of the rebreathing period. For %HbCO measurement, a 2 mL Blood Gas Monovette (Sarstedt, Nümbrecht, Germany) was taken. The tubes were filled within approximately 3 s at the standard time points. Immediately before the blood samples were drawn, some blood drops were discarded to avoid measuring cannula’s dead space. After the blood drawing, the tubes were vented, closed and then stored in a blood rocker between each of the measurements. Every sample was measured in triplicate with the help of a blood gas analyser (RapidLab 1245, Siemens Healthcare Diagnostics, Sudbury, UK). The average of the replicates was used for further calculations. The RapidLab was at least daily calibrated (automatic calibration) to standard and the quality of measurement was checked by means of three different quality control solutions.
The tHb mass was calculated using the software SpiCo (2005, by Schmidt and Prommer) based on the formula:
where Kbaro is ambient barometric pressure (mmHg) × 760−1 (mmHg) × [1 + (0.003661 × ambient temperature °K)] and VCO the volume of CO (mL) bound to haemoglobin (Hb) at min 7 [CO volume (mL) applied to the system minus the CO volume (mL) not bound to haemoglobin (=sum of CO volume remaining in the spirometer and the volume that was exhaled from minute 2–8)]. ∆%HbCO is the difference between the initial %HbCO (mean %HbCO of 2 initial blood samples) and maximal %HbCO (average %HbCO of blood samples at minute 6 and 8 after starting the rebreathing). 1.39 (mL g−1) is Hüfners number as 1.39 mL CO bind to 1 g Hb. The software program SpiCo corrects for the loss of CO from haemoglobin to myoglobin according to the findings of Schmidt and Prommer (2005) and by Prommer and Schmidt (2007) by 0.3% of administered CO per minute. The reliability of tHb mass measurement had been tested in a pilot study with duplicate tests (n = 20) and was 2.6% (95% confidence interval 1.9–3.8%), expressed as a typical percentage error (%TE, Hopkins 2000).
Red blood cell profile
Before the venous blood sampling within COR, venous blood samples were drawn in a sitting position from an antecubital vein into an EDTA tube (2.7 mL, Sarstedt Monovette, Nümbrecht, Germany) via the cannula and were analysed for haemoglobin concentration [Hb], haematocrit (Hct), mean corpuscular volume (MCV), mean corpuscular haemoglobin concentration (MCHC) and mean corpuscular haemoglobin (MCH) using ADVIA 2120 (Siemens Healthcare, Eschborn, Germany). To monitor for iron deficiency, ferritin was determined in venous blood drawn from an antecubital vein by immunoturbidimetry (ADVIA® 2400, Siemens Healthcare, Eschborn, Germany).
Statistics
Data were analysed with PASW Statistics 17.0.2 for Windows (SPSS, Chicago, IL). Statistical significance was set at P < 0.05. Values are presented as mean ± standard deviation. Kolmogorov–Smirnov tests were performed to test for normality distribution. A general linear model (GLM) two-way ANOVA (2 × 2 design) was used to evaluate effects of gender and group (END, nEND) and interaction effects (group × gender) on tHb mass and blood profile parameters in the cross-sectional analysis. Changes in performance at 4 LT, body height, body weight, and FFM over time were analysed with an one-way ANOVA with repeated measures for each group (END, nEND). To identify effects for gender, group (END, nEND) and time (time points 1–4) on tHb mass and blood profile variables, a GLM three-way ANOVA with repeated measures (2 × 2 × 4 design) was conducted. Owing to the small sample size, only main effects and two-way interactions (group × time and gender × time) were studied. To exclude an effect of iron-treated iron deficiency on changes in tHb mass and blood profile variables, a GLM two-way ANOVA with repeated measures (2 × 4 design) was performed additionally. Between-group differences were determined involving the Bonferroni’s post hoc test. In ANOVAs, homogeneity of variances was checked with Levene’s test and for repeated measurements, sphericity was checked via Mauchly’s test. If necessary, a Greenhouse–Geisser adjustment was made to the degrees of freedom.
Results
Cross-sectional analysis
tHb mass (Fig. 1)
Related to body weight, tHb mass was significantly (P < 0.001) greater in END compared with nEND (11.2 ± 1.6 vs. 9.7 ± 1.3 g kg−1), in male (P < 0.01) as well as in female (P < 0.05) athletes. Related to FFM, tHb mass was significantly (P < 0.01) greater in END as compared to nEND (12.8 ± 1.3 vs. 11.6 ± 1.0 g kg−1), however, there was no significant difference between female END and nEND. A significant group × gender effect was observed for absolute tHb mass (P < 0.05) with slightly (non-significantly) higher values in male END when compared with male nEND and non-significantly lower values in female END when compared with female nEND. There was a gender difference with significantly (P < 0.001) greater absolute tHb mass, tHb mass related to body weight, and tHb mass related to FFM in male when compared with female athletes, in END as well as in nEND.

Cross-sectional analysis: total haemoglobin mass (tHb mass) in absolute values, related to body weight, and related to fat free mass (FFM) in male and female endurance-trained (END, male n = 18, female n = 11) and non-endurance-trained (nEND, male n = 11, female n = 19) athletes [mean (SD)]. #,##Significantly (# P < 0.05, ## P < 0.01) different between male and female athletes; *;**significantly (*P < 0.05, **P < 0.01) different between END and nEND
Red blood cell profile (Table 4)
There was a significant group × gender effect on [Hb] (P < 0.05) as well as on Hct (P < 0.05), indicating slightly, but not significantly, higher values in male nEND compared with male END and lower values in female nEND when compared with female END. Average [Hb] and Hct values were significantly (P < 0.001) higher in male (14.6 ± 0.8 g dl−1 and 41.9 ± 2.9%) compared with female athletes (13.0 ± 0.7 g dl−1 and 36.8 ± 2.1%). No significant differences between END and nEND were detected for any variable of the red blood cell count.
Longitudinal observation
Anthropometric data (Table 2)
In END, body height (P < 0.05), body weight (P < 0.001), and FFM (P < 0.01) increased significantly during 18 months (T1–T4) from 176 ± 5 to 177 ± 5 cm, 64.0 ± 6.8 to 69.5 ± 6.5 kg and from 58.5 ± 7.6 to 59.1 ± 8.1 kg, respectively. In nEND, only body weight (P < 0.01) increased significantly (70.0 ± 10.0 to 72.5 ± 8.0 kg).
tHb mass (Fig. 2)
No significant time × group and time × gender interactions were observed. Only in END, significant increases in tHb mass occurred from time point 2 to time point 3 (P < 0.05) and 4 (P < 0.05), whereas tHb mass in nEND remained unchanged. Related to body weight, no significant changes in relative tHb mass over time were found. Only for tHb mass related to body weight, significantly (P < 0.01) greater tHb mass was observed in END when compared with nEND at all time points. For tHb mass related to FFM, the differences between END and nEND reached the level of significance only at T1. At all time points, tHb mass was significantly greater in male compared with female athletes in absolute as well as in relative terms.

Longitudinal analysis: total haemoglobin mass (tHb mass) in absolute values, related to body weight, and related to fat free mass (FFM). The left panels show tHb mass over four time points (T1–T4) separated by 6-month intervals in endurance-trained (END, n = 17) and non-endurance-trained (nEND, n = 10) athletes [mean (SD)], #;##significantly (P < 0.05; P < 0.01) different between END and nEND at the respective time points, *significant (P < 0.05) difference between the respective time points in END. The right panels show the parameters in male (male, n = 14) and female athletes (female, n = 13) [mean (SD)]. ## P < 0.01 significantly different male and female athletes at the respective time points
Red blood cell profile (Table 5)
No significant differences between END and nEND were found for [Hb] and [Hct] and these variables did not change significantly over time. [Hb] and Hct were significantly (P < 0.001) higher in male when compared with female athletes at all time points ([Hb]: P < 0.01; Hct: T1–T3, P < 0.01; T4, P < 0.05). There was a significant time × gender interaction effect for MCV (P < 0.01) with slightly reduced MCV values in male athletes over time when compared with stable values in female athletes; no other significant time × gender interactions were located on MCH and MCHC. No significant gender or group differences were observed for MCV and MCH; MCHC was slightly, but significantly higher in male when compared with female athletes at T4 (P < 0.05).
Performance at 4 LT (Table 2)
In END, performance at 4 LT did not change significantly during the 18 months of regular training (T1 100%, T2 100 ± 4%, T3 101 ± 5%, T4 98 ± 7%). In nEND, performance at 4 LT decreased significantly (P < 0.05) from T1 to T4 (100 vs. 93 ± 5% P < 0.05) and T2 to T4 (103 ± 3 vs. 93 ± 5%; P < 0.05), respectively.
Discussion
To our knowledge, this is the first study that evaluated differences in tHb mass and markers of red blood cell profile in elite endurance-trained and non-endurance-trained male and female adolescent athletes. Beyond the cross-sectional analysis, tHb mass development and changes in red blood cell profile were investigated in a subset of the elite junior athletes during 18 months of regular training in the late pubertal phase. tHb mass related to body weight was found to be significantly greater in END when compared with nEND and in male when compared with female adolescent athletes. There were no significant differences between END and nEND for [Hb] and [Hct] whilst the well-known gender differences with significantly higher values for male compared with female athletes were evident. No significant changes in tHb mass beyond the alterations explained by growth and maturation were found during ongoing regular training at the age of 15–17 years. In line with the findings for tHb mass, markers of red blood cell profile also did not change significantly during the observation period.
Cross-sectional analysis
In the endurance-trained group of adolescent athletes, tHb mass related to body weight was significantly, about 15%, greater than in the non-endurance-trained group. This difference is smaller than the differences observed in adult athletes. About 35–40% higher relative tHb mass values in endurance-trained compared with non-endurance-trained athletes (~15 vs. 11 g kg−1) were found by Heinicke et al. (2001). Prommer and Schmidt (2009) reported a difference of up to ~50% (15 and 12 g kg−1 for adult male and female elite endurance athletes versus 10 and 9 g kg−1 for male and female untrained individuals). The male (12.0 ± 1.3 g kg−1) and female (9.9 ± 0.9 g kg−1) adolescent endurance athletes of the present study had lower tHb masses than the above-mentioned elite adult endurance athletes, however, their tHb masses were similar to the values reported for adolescent endurance athletes in other studies (Eastwood et al. 2009; Koch and Röcker 1977). Koch and Röcker (1977) estimated tHb mass from the measurement of plasma volume and reported tHb mass of 12.6 ± 1.9 g kg−1 in eight 14–15-year-old trained boys as compared to 14.4 ± 2.0 g kg−1 in six endurance-trained men. Although the difference between the trained boys and men did not reach the level of significance, this result supports the findings of the present study. We can only speculate about the reasons for the lower tHb masses in our elite endurance-trained adolescent athletes as compared to the values reported for elite adult endurance athletes. First of all, the main increase in tHb mass due to regular endurance stimuli might occur during the late adolescent phase at the age of 17–20 years. To our knowledge, this phase has not been investigated so far. When considering the lack of performance increase at 4 LT, intensity and extent of endurance training might have been too low for further development of endurance performance, however, all the included athletes competed successfully in the monitored 18-month period and stayed in the German elite youth teams. Furthermore, we wonder if it should be taken into consideration that the high tHb masses reported for some of the world class adult endurance athletes might have been flawed by blood doping.
With regard to gender differences, we observed ~20% higher values for tHb mass related to body weight for male when compared with female athletes in END as well as in nEND. Related to FFM, this gender difference was diminished to ~10%, but it still was significant. Studies focussing on gender differences in tHb mass in athletes are rare. Prommer and Schmidt (2009) reported ~25% higher tHb mass related to body weight in elite male when compared with elite female endurance athletes. In untrained adolescents of the same age group as in the present study, Åstrand (1952) found ~24 to 32% higher tHb mass in male when compared with female sedentary subjects. The gender difference in tHb mass, emerging during adolescence, is most likely due to the rapid increase in testosterone levels observed during puberty. Besides the well-known effects on FFM, testosterone has a strong stimulating effect on erythropoiesis that has previously been reported (Hero et al. 2005). Accordingly, we found significant gender differences in [Hb] and Hct in the cross-sectional analysis, with higher values in male adolescent athletes. Higher values of [Hb] and Hct in boys compared with girls from puberty onwards through adolescence have been well documented (e.g. Flegar-Mestric et al. 2000).
Longitudinal observation
During the 18-month observation period, a significant increase in tHb mass occurred in END only; however, related to body weight, the change was not significant. As also only END showed a significant increase in body height and FFM the augmentation of tHb mass most likely is explained by physical growth. This observation is in line with the results of two investigations performed with younger athletes than in the present study. Eastwood et al. (2009) also found a significant increase in tHb mass in 11–15-year-old cyclists after 12 months of regular endurance training, but unchanged values when tHb mass was related to body weight. In a study with previously untrained 11–13-year-old boys, an increase in tHb mass was observed after these boys had been subjected to 34 training sessions (3×/week) designed to improve aerobic capacity and this increase in tHb mass was also explained by growth processes taking place in the observation period (von Döbeln and Eriksson 1972). However, a significant difference in tHb mass between END and nEND was observed in the cross-sectional analysis. This difference in adolescent athletes indicates a strong role of heredity for determining tHb mass as already suggested by other investigators (Eastwood et al. 2009; Martino et al. 2002).
[Hb] and Hct were also found to be stable in the adolescent athletes of the present study. However, there was a significant time × gender interaction for MCV with a decrease in male athletes from 86 ± 5 to 84 ± 3 fl, whereas in female athletes MCV no such development was observed (85 ± 2 to 85 ± 2 fl). Because MCH values were stable, a significant gender difference in MCHC at time point 4 is a logic consequence. To our knowledge, there are no longitudinal studies on the development of MCV, MCH and MCHC in young athletes and we do not know if this phenomenon is of importance. In previously untrained adults, however, a significant increase in MCV along with a significant decrease in MCHC was observed after several weeks of training (reviewed by El-Sayed et al. 2005). In contrast, Rietjens et al. (2002) did not find significant alterations in elite Olympic distance triathletes in [Hb], Hct, MCV, MCH and MCHC over a period of 3 years. Haemodilution with a decrease in [Hb] and Hct is a well-known phenomenon occurring with regular endurance training in adults (El-Sayed et al. 2005). In accordance with the results reported by Koch and Röcker (1977), plasma volumes in END have to be significantly larger than in nEND with regard to the significantly increased tHb mass in END. However, in contrast to the findings in adult athletes, [Hb] and Hct did not differ significantly between END and nEND in the cross-sectional analysis indicating that, unlike in adult endurance athletes, the increase in plasma volume did not exceed the increase in tHb mass. To our knowledge, there are only two studies which compared parameters of red blood cell profile in adolescent athletes with age-matched controls and the results were inconsistent. Whilst Mayr et al. (2006) did not observe significant differences in [Hb] and Hct between 14 and 18-year-old elite speed skaters and age-matched non-athletes [Hb] and Hct were shown to be significantly lower in ~14-year-old highly trained athletes when compared with untrained individuals in a study of Boyadjiev and Taralov (2000).
Limitations of the study
Unfortunately, VO2max could not be determined in the different tests. However, having in mind the results reported by Eastwood et al. (2009) with a significant increase in relative VO2max without corresponding augmentation of tHb mass after 1 year of endurance training in young cyclists, the lacking VO2max measurement might not be a major drawback. As performance at 4 LT was the only method of performance measurement, we could apply in the adolescent athletes from different sports and as performance at 4 LT did not increase during 18 months of endurance training, we cannot judge whether endurance training was successful or not. As another limitation, some of the non-significant findings might be due to small sample size.
Conclusions
In elite adolescent athletes, the same differences in relative tHb mass between endurance-trained and non-endurance-trained male and female athletes can be observed as in adult elite athletes, however, to a smaller extent. Apparently, ongoing regular endurance training at the age of 15–17 years does not induce a significant increase in tHb mass in already endurance-trained young athletes beyond the changes due to growth and maturation and relative tHb mass remains unchanged as well as markers of red blood cell profile. The critical age and determining factors for the development of the reported large differences between adult elite endurance-trained and non-endurance-trained male and female athletes remain unknown.
References
Armstrong N, Welsman JR (2001) Peak oxygen uptake in relation to growth and maturation in 11- to 17-year-old humans. Eur J Appl Physiol 85:546–551
Åstrand P-O (1952) Experimental studies of physical capacity in relation to sex and age. Munksgaard, Copenhagen
Berglund B, Ekblom B, Ekblom E, Berglund L, Kallner A, Reinebo P, Lindeberg S (2007) The Swedish blood pass project. Scand J Med Sci Sports 17:292–297
Boyadjiev N, Taralov Z (2000) Red blood cell variables in highly trained pubescent athletes: a comparative analysis. Br J Sports Med 34:200–204
Brotherhood J, Brozovic B, Pugh LG (1975) Haematological status of middle- and long-distance runners. Clin Sci Mol Med 48:139–145
Eastwood A, Bourdon PC, Withers RT, Gore CJ (2009) Longitudinal changes in haemoglobin mass and VO2max in adolescents. Eur J Appl Physiol 105:715–721
Eisenmann JC, Pivarnik JM, Malina RM (2001) Scaling peak VO2 to body mass in young male and female distance runners. J Appl Physiol 90:2172–2180
El-Sayed MS, Ali N, El-Sayed AZ (2005) Haemorheology in exercise and training. Sports Med 35:649–670
Flegar-Mestric Z, Nazor A, Jagarinec N (2000) Haematological profile in healthy urban population (8 to 70 years of age). Coll Antropol 24:185–196
Friedmann B, Weller E, Mairbaurl H, Bärtsch P (2001) Effects of iron repletion on blood volume and performance capacity in young athletes. Med Sci Sports Exerc 33:741–746
Garvican LA, Martin DT, McDonald W, Gore CJ (2010) Seasonal variation of haemoglobin mass in internationally competitive female road cyclists. Eur J Appl Physiol 109:221–231
Gore CJ, Hahn AG, Burge CM, Telford RD (1997) VO2max and haemoglobin mass of trained athletes during high intensity training. Int J Sports Med 18:477–482
Gore CJ, Bourdon PC, Woolford SM, Ostler LM, Eastwood A, Scroop GC (2006) Time and sample site dependency of the optimized co-rebreathing method. Med Sci Sports Exerc 38:1187–1193
Heinicke K, Wolfarth B, Winchenbach P, Biermann B, Schmid A, Huber G, Friedmann B, Schmidt W (2001) Blood volume and hemoglobin mass in elite athletes of different disciplines. Int J Sports Med 22:504–512
Hero M, Wickman S, Hanhijarvi R, Siimes MA, Dunkel L (2005) Pubertal upregulation of erythropoiesis in boys is determined primarily by androgen. J Pediatr 146:245–252
Hopkins WG (2000) Measures of reliability in sports medicine and science. Sports Med 30:1–15
Kjellberg SR, Rudhe U, Sjöstrand T (1949) Increase of the amount of hemoglobin and blood volume in connection with physical training. Acta Physiol Scand 19:146–151
Koch G, Röcker L (1977) Plasma volume and intravascular protein masses in trained boys and fit young men. J Appl Physiol 43:1085–1088
Lohman TG (1981) Skinfolds and body density and their relation to body fatness: a review. Hum Biol 53:181–225
Lundby C, Thomsen JJ, Boushel R, Koskolou M, Warberg J, Calbet JA, Robach P (2007) Erythropoietin treatment elevates haemoglobin concentration by increasing red cell volume and depressing plasma volume. J Physiol 578:309–314
Martino M, Gledhill N, Jamnik V (2002) High VO2max with no history of training is primarily due to high blood volume. Med Sci Sports Exerc 34:966–971
Mayr A, Kuipers H, Falk M, Santer P, Wierer B (2006) Comparison of hematologic data in world elite junior speed skaters and in non-athletic juniors. Int J Sports Med 27:283–288
Mørkeberg J, Sharpe K, Belhage B, Damsgaard R, Schmidt W, Prommer N, Gore CJ, Ashenden MJ (2009) Detecting autologous blood transfusions: a comparison of three passport approaches and four blood markers. Scand J Med Sci Sports. doi:10.1111/j.1600-0838.2009.01033.x
Parisotto R, Gore CJ, Emslie KR, Ashenden MJ, Brugnara C, Howe C, Martin DT, Trout GJ, Hahn AG (2000) A novel method utilising markers of altered erythropoiesis for the detection of recombinant human erythropoietin abuse in athletes. Haematologica 85:564–572
Pottgiesser T, Umhau M, Ahlgrim C, Ruthardt S, Roecker K, Schumacher YO (2007) Hb mass measurement suitable to screen for illicit autologous blood transfusions. Med Sci Sports Exerc 39:1748–1756
Prommer N, Schmidt W (2007) Loss of CO from the intravascular bed and its impact on the optimised CO-rebreathing method. Eur J Appl Physiol 100:383–391
Prommer N, Schmidt W (2009) Total hemoglobin mass and sports. Dtsch Z Sportmed 60:293–294
Prommer N, Sottas PE, Schoch C, Schumacher YO, Schmidt W (2008) Total hemoglobin mass—a new parameter to detect blood doping? Med Sci Sports Exerc 40:2112–2118
Rietjens GJ, Kuipers H, Hartgens F, Keizer HA (2002) Red blood cell profile of elite Olympic distance triathletes: a three-year follow-up. Int J Sports Med 23:391–396
Schmidt W, Prommer N (2005) The optimised CO-rebreathing method: a new tool to determine total haemoglobin mass routinely. Eur J Appl Physiol 95:486–495
Schmidt W, Prommer N (2008) Effects of various training modalities on blood volume. Scand J Med Sci Sports 18:57–69
von Döbeln W, Eriksson BO (1972) Physical training, maximal oxygen uptake and dimensions of the oxygen transporting and metabolizing organs in boys 11–13 years of age. Acta Paediatr Scand 61:653–660
WADA (2010) Athlete biological passport operating guidelines. Version 2.0. http://www.wada-ama.org/Documents/Science_Medicine/Athlete_Biological_Passport/WADA_AthletePassport_OperatingGuidelines_FINAL_EN.pdf. Accessed 20 August 2010
Wagner DR (1996) Body composition assessment and minimal weight recommendations for high school wrestlers. J Athl Train 31:262–265
Acknowledgments
The authors want to thank Kai Schommer, Rüdiger Schmieder, Susanne Hupfer, Falko Frese, Judith Strunz and Joachim Jost for support within the measurements and for technical assistance. The authors also acknowledge the commitment of the young athletes in completing this lengthy undertaking and thank their coaches and parents for permission and understanding.
Conflict of interest
The authors have no conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Guido Ferretti.
Rights and permissions
About this article
Cite this article
Ulrich, G., Bärtsch, P. & Friedmann-Bette, B. Total haemoglobin mass and red blood cell profile in endurance-trained and non-endurance-trained adolescent athletes. Eur J Appl Physiol 111, 2855–2864 (2011). https://doi.org/10.1007/s00421-011-1920-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-011-1920-5