
Abstract
Early effects of a resistance training program include neural adaptations at multiple levels of the neuraxis, but direct evidence of central changes is lacking. Plasticity exhibited by multiple supraspinal centers following training may alter slow negative electroencephalographic activity, referred to as movement-related cortical potentials (MRCP). The purpose of this study was to determine whether MRCPs are altered in response to resistance training. Eleven healthy participants (24.6 ± 3.5 years) performed 3 weeks of explosive unilateral leg extensor resistance training. MRCP were assessed during 60 self-paced leg extensions against a constant nominal load before and after training. Resistance training was effective (P < 0.001) in increasing leg extensor peak force (+22%), rate of force production (+32%) as well as muscle activity (iEMG; +47%, P < 0.05). These changes were accompanied by several MRCP effects. Following training, MRCP amplitude was attenuated at several scalp sites overlying motor-related cortical areas (P < 0.05), and the onset of MRCP at the vertex was 28% (561 ms) earlier. In conclusion, the 3-week training protocol in the present study elicited significant strength gains which were accompanied by neural adaptations at the level of the cortex. We interpret our findings of attenuated cortical demand for submaximal voluntary movement as evidence for enhanced neural economy as a result of resistance training.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Plasticity and adaptation of the human motor system in response to resistance exercise has been well documented (for reviews: Aagaard 2003; Folland and Williams 2007; Gabriel et al. 2006; Griffin and Cafarelli 2005). The loci of these adaptations are not restricted; rather they appear diffuse throughout all levels of the neuraxis (Duchateau and Enoka 2002). At the level of the motor unit, resistance training has been shown to enhance recruitment, firing rate, synchrony, and the incidence of doublets (Van Cutsem et al. 1998). These observations may be a function of augmented volitional drive along the corticospinal pathway (Aagaard et al. 2002; Del Balso and Cafarelli 2007; Duclay et al. 2008) which, in turn, may be preceded by increased cortical excitability (Griffin and Cafarelli 2007). Several attempts have been made to link training-induced plasticity in corticospinal pathways to increased force output (cf. Fig. 8, Del Balso and Cafarelli 2007; Fig. 1, Duchateau and Enoka 2002; Fig. 4, Bawa 2002), yet the supporting evidence comes largely from data obtained via peripheral measures (e.g. surface electromyography) which may not adequately reflect changes in supraspinal centers. Consistent with the limited character of existing evidence, the significance and presence of supraspinal adaptation has been questioned, particularly in the early stages of a program of resistance training (Carroll et al. 2002; Jensen et al. 2005).
Neural adaptations in response to resistance training may be reflected in coordination and learning which act to facilitate recruitment and activation of muscles engaged in a strength task (Folland and Williams 2007). Individuals may ‘learn’ to increase maximal force output as a form of motor learning (Griffin and Cafarelli 2007), and therefore exhibit plasticity in motor cortical areas. Indirect support for supraspinal adaptation comes from studies reporting increased strength gain as a result of imagined contractions (Ranganathan et al. 2004; Sidaway and Trzaska 2005; Yue and Cole 1992), cross-education or contralateral strength training effect (Adamson et al. 2008; Farthing et al. 2007; Lagerquist et al. 2006; Munn et al. 2005) as well as specificity of training (Duchateau and Enoka 2002). Although direct evidence of modified central motor activity influencing these phenomena is lacking, supporting evidence can be adduced from investigations that have utilized evoked reflex (H-reflex) and motor evoked potential (MEP) paradigms demonstrating such an effect.
Presumably, the H-reflex, the electrical analog to the stretch reflex, provides a means to assess net synaptic input (i.e. afferent and descending) as well as excitability of the α-motor neuron pool in vivo (Misiaszek 2003). Additionally, the electrophysiological variant of the H-reflex (V-wave), obtained through supramaximal stimulation of a mixed nerve, has been used to assess the magnitude of efferent neural drive in descending corticospinal pathways (Aagaard et al. 2002). When combined, the H-reflex and V-wave may provide estimates of spinal and supraspinal adaptations, respectively. Facilitation of the H-reflex has been observed following short-term (e.g. 3–8 weeks) plantar flexor resistance training in some (Holtermann et al. 2007; Lagerquist et al. 2006), but not all experiments (Del Balso and Cafarelli 2007; Duclay et al. 2008; Fimland et al. 2009; Gondin et al. 2006). In those studies unable to elicit changes in H-reflex amplitude (i.e. spinal excitability), increases in evoked V-wave responses were reported, suggesting an augmented volitional drive via supraspinal adaptation (Del Balso and Cafarelli 2007; Duclay et al. 2008; Fimland et al. 2009; Gondin et al. 2006). Following a moderate length resistance training program (e.g. 14 weeks), Aagaard and colleagues (2002) observed increases in both H-reflex (~20%) and V-wave (~50%) amplitudes. Lack of consistency amongst these studies may reflect limitations of the H-reflex measure, which has been shown to be highly modifiable and influenced by a variety of factors (Misiaszek 2003).
Motor evoked potentials elicited via transcranial magnetic stimulation (TMS) have been used to examine the neural adaptive effects of resistance training in three separate investigations with equivocal results. Following 4 weeks of isometric tibialis anterior training MEP amplitude increased by 32% (Griffin and Cafarelli 2007), but a depression in cortical excitability was noted for training of the biceps brachii (Jensen et al. 2005) and first dorsal interosseous (Carroll et al. 2002). Griffin and Cafarelli (2007) suggested that these differences may lie in the differing responses of certain muscle groups to TMS and/or dissimilar training protocols. Moreover, changes in the excitability of cortical, subcortical, or spinal neurons likely influence the TMS-induced MEP as the rise time is long enough to include multiple pathways (Taube et al. 2008). For example, alterations at the spinal level (e.g. recruitment, rate coding, synchronization) could potentially influence the evoked force induced by TMS (del Olmo et al. 2006).
An alternative to evoked responses which does not introduce artificial input to the central nervous system or involve the recording of responses distant from the cortex (i.e. surface EMG) (Schillings et al. 2006), may be better-suited for detecting supraspinal adaptations secondary to resistance training. Surface negative potentials, detected at the scalp via electroencephalography (EEG) around the time of voluntary movement, are referred to as movement-related cortical potentials (MRCP). MRCP reflect the summed excitatory post-synaptic potentials of apical dendrites and are related to the preparation and execution of self-initiated movement (for review: Shibasaki and Hallett 2006). It is generally agreed that the temporal course of the MRCP waveform shows an onset 1–2 s prior to movement onset bilaterally in the supplementary motor area (SMA), followed by activity in contralateral premotor and motor cortices with a scalp representation that is somatotypically appropriate (Shibasaki and Hallett 2006). As a result, MRCP may be delineated into three consecutive pre-movement periods (Kristeva et al. 1990; Slobounov and Ray 1998), referred to as (1) the Bereitschaftspotential (i.e. preparation), (2) motor execution and (3) movement-monitoring potentials. The amplitude of each component is a function of the number of active neurons, their synchrony and rate of discharge (Siemionow et al. 2000). The later MRCP components have been correlated with force, rate of force development, and associated EMG amplitude for both elbow-flexion (Siemionow et al. 2000), and plantar-flexion movements (do Nascimento et al. 2005) suggesting that MRCP may index the level of muscle activation.
The present study investigated the possible involvement of supraspinal adaptations in resistance training, using MRCPs as a measure of brain activity. We have noted above several attractive aspects of the MRCP method in this context, including their spatiotemporal resolution and known origins in the underlying cortices. Specifically, we hypothesized that strength training would allow the motor tasks to be performed with less relative effort resulting in adaptive changes in MRCP related to enhanced neural efficiency. The present experiment is, to our knowledge, the first to utilize EEG (i.e. MRCP) as a tool for examining plasticity of the central nervous system in a resistance training paradigm.
Materials and methods
Subjects and design
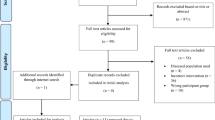
Eleven healthy volunteers (9 female; 2 male), with a mean age of 24.6 ± 3.5 year and body mass of 63.8 ± 9.2 kg, participated in this investigation. All participants were right hand and foot dominant, as assessed through self-report, and had not participated in any resistance training for at least the past year. Participants had no known history of musculoskeletal injury or neurological events, and were deemed eligible to participate in resistance exercise by the Physical Activity Readiness Questionnaire (PAR-Q; Thomas et al. 1992). Following a detailed verbal explanation of study procedures, participants provided their written informed consent and were then familiarized with the training and testing equipment. The Washington University School of Medicine Human Research Protection Office approved the experimental procedures, which were in accordance with the Declaration of Helsinki.
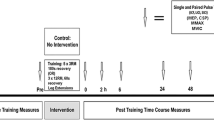
To control inter-individual variance in the MRCP response, this study employed a quasi-experimental (i.e. pre/post) design where participants served as their own controls. Each participant participated in two experimental sessions separated by a 3-week resistance training period. During each experimental session, participants performed maximal and submaximal leg extensions of the dominant leg. Maximal voluntary isometric contractions were performed first, followed by 60 submaximal repetitions. EEG data were recorded only during the submaximal repetitions, whereas force and EMG data were recorded during maximal and submaximal performance. Prior to the training intervention, a subset of subjects (N = 7) also completed a second pre-test session within 3–7 days of their first in order to confirm test–retest reliability of the MRCP measures. All participants completed their post test between 1 and 3 days following their final training session.
Apparatus
Participants performed unilateral maximal and submaximal leg extensions on a modified leg press device (Champion Barbell; Dallas, TX, USA) instrumented with four load cells (Transcell Technology Inc.; Buffalo Grove, IL, USA) which were encased within the foot plate (Fig. 1). A custom-built mechanism was attached to the device that allowed 2 cm individual adjustments. These adjustments were made, and were reproduced for post-testing, such that each participant was positioned in a recumbent seated position in 110° of hip flexion. Locking of this mechanism enabled maximal isometric testing, but could be released for the submaximal MRCP protocol. When released, the leg press device became freely moveable and although no external weight was added, the device itself produced a constant load of approximately 18 kg.

Illustration of experimental setup
Electrophysiological recordings
Participants were fitted with either an appropriately sized 61-channel elastic nylon Quick-cap (Compumedics; Charlotte, NC, USA), and EEG data were acquired using the 70-channel Synamps2 amplifier system and recorded in the Acquire module of Scan 4.3 (Compumedics; Charlotte, NC, USA). This system has a common mode rejection ration of 100 dB, 24-bit A/D resolution, and input impedance of 10 MΩ. Data were recorded with a bandwidth of DC-100 Hz and sampled at 1 kHz. Impedances were kept below 5 kΩ for all electrodes.
Vertical and horizontal electrooculograms (EOG) were recorded using Ag/AgCl electrodes placed above and below the right eye and the left and right outer canthi, respectively. Electromyographic activity (EMG) of the vastus lateralis was recorded from bipolar electrodes with an inter-electrode distance of approximately 20 mm. Electrodes were arranged according to SENIAM (Hermens et al. 2000) recommendations. Prior to electrode application, the skin was cleaned and vigorously abraded. EOG, EMG, EEG and force signals were all continuously and synchronously recorded through the Synamps2 amplifier and Scan 4.3 software.
Resistance training
Supervised unilateral training of the leg extensors was conducted three times per week on non-consecutive days for 3 weeks (i.e., nine total sessions). A relatively brief, 3-week training regimen was selected on the basis of evidence that neural plasticity governs early adaptive effects (Holtermann et al. 2007). In addition, leg extensions were performed explosively in order to maximize neural adaptations (Behm and Sale 1993; Hakkinen et al. 1985; Van Cutsem et al. 1998). Participants were encouraged to maximally accelerate the load in the concentric phase and slowly (e.g. 2 s tempo) return the load in the eccentric phase. All training was progressive in nature as volume and intensity increased after the third and sixth sessions. Initial training loads were based upon one-repetition maximum (RM) strength, which was determined prior to the first training session. Sessions 1–3 consisted of three sets of 10–12 repetitions at 70–75% RM; Sessions 4–6 consisted of four sets of 8–10 repetitions at 75–80% RM; Sessions 7–9 consisted of five sets of 6–8 repetitions at 80–85% RM.
Strength and muscle activity assessment
Maximal voluntary isometric contraction (MVIC) of the dominant leg extensors was determined from three separate maximal attempts in which subjects were instructed to contract as hard and as fast as possible and to maintain the contraction until they were instructed to release (~3 s). MVICs were preceded by several submaximal preconditioning contractions and a rest period. Force signals and concomitant EMG of the vastus lateralis were synchronously sampled at 1 kHz and digitally converted as described earlier.
Offline, the summed force signals were digitally smoothed using a fourth order, zero-lag Butterworth filter (15 Hz cutoff). Force–time histories were analyzed for MVIC and the rate of force development (RFD). Maximal RFD was computed as the highest values of the slope coefficients of the tangent computed during a sliding 5 ms window (Viitasalo et al. 1980). Onset of contraction was detected using a threshold criteria of 5 Newtons and was confirmed with visual inspection. The average of three MVIC attempts was used for statistical analysis.
Raw EMG signals were digitally high-pass filtered using a fourth order, zero-lag Butterworth filter (5 Hz cutoff), and followed by a moving root-mean-square filter with a 50 ms time constant (Aagaard et al. 2002). Onset of EMG was set to precede the onset of contraction by 70 ms to account for the presence of electromechanical delay (Aagaard et al. 2002). Variables of interest included peak EMG during contraction (EMGpk), and the average integrated EMG in the 200 ms time interval prior to peak force (EMG200) as described elsewhere (Kvorning et al. 2006). Force and EMG signal processing was performed using Datapac 2K2 software (v3.16; Mission Viejo, CA, USA).
MRCP acquisition and analysis
Following MVIC testing and a 5 min rest period, each participant performed three sets of 20 self-paced leg extensions of the dominant leg. Interspersed rest periods of approximately 5 min were given to minimize possible physical and mental fatigue. Participants started from an initial position of 110° hip flexion and 80° knee flexion (see Fig. 1). Upon completion of the movement, they reached a position of 70° hip flexion and 0° knee flexion. Participants were instructed to briskly extend their leg during the concentric phase and slowly lower the arm of the leg press to the starting position (i.e. eccentric phase). Prior to commencing subsequent repetitions, participants were instructed to relax and wait calmly for at least 5 s. To minimize the influence of eye movements on the EEG signal, participants were instructed to maintain an open-eye, fixed-gaze on a target located approximately 3 m in front of them. They were also told to refrain from tensing muscles other than the involved leg extensors and to avoid eye blinks in the period before and during the leg extension to avoid generating artifacts. Their arms gently rested on handles attached to the seat of the leg press device. Between trials (i.e. repetitions), eye blinks were allowed as these periods were not included in the triggered averaging.
All offline analysis was performed utilizing custom MATLAB programs (v7.3.0; Math Works, Inc.; Natick, MA, USA). Raw EEG data were inspected visually to identify and remove signal artifacts. Trials containing blink artifacts occurring during epochs of interest were excluded. Data were high-pass filtered at 0.01 Hz (90 db) to eliminate the baseline shift generated by DC recording and were referenced to a common average. For each trial (i.e. repetition), the onset of force was used to synchronize a 4 s epoch, 3 s before the onset and 1 s after. Force onset was defined as the point when the signal exceeded a threshold of two standard deviations above the activity level at the beginning of the epoch and subsequently remained above that level for at least 500 ms. Non-contaminated epochs were averaged together forming an average MRCP for each participant.
MRCPs were decomposed into three distinct components (Kristeva et al. 1990; Slobounov et al. 2004): (1) mean amplitude between −600 and −500 ms prior to movement onset, or Bereitschaftspotential (BP−600 to −500), (2) mean amplitude between −100 ms and movement onset, or motor potential (MP−100 to 0), and (3) mean amplitude from onset to +100 ms, or movement-monitoring potential (MMP0 to 100). Amplitudes were computed with reference to a baseline of −3,500 to −3,000 ms prior to movement onset. Latencies were also determined by computing the time interval from onset of MRCP negativity to force onset. Onset of negativity (i.e. MRCP onset) was identified as the point when the baseline signal deviated from a 95% confidence interval and subsequently remained above that level for at least 500 ms (Wheaton et al. 2007) from the period of −2,500 to −2,000 ms preceding movement. Analysis focused primarily on three central electrode sites: Cz, C1, and C2. These sites were chosen because leg movements are associated with high activity over the SMA and demonstrate bilateral motor cortex activation (Luft et al. 2002).
Also in each trial, the EMG signal was processed in the same manner as performed in MVIC, but was averaged over a 2,500 ms epoch (i.e. 1,000 ms prior to 1,500 ms after movement onset), and then averaged over all trials. Mean amplitude and onset relative to movement onset (i.e. force onset) were calculated. The criteria for EMG onset were equivalent to MRCP onset described above. Mean force and maximal RFD was obtained by triggered averaging as well.
Two-dimensional (2D) topographical maps were created to reflect spatial features of the MRCP considering the entire 61-electrode montage (Fig. 3). Separate 2D maps were created for each of the three distinct MRCP components for pre- and post-testing, using group mean data. Group mean data rather than single-subject data were used to better demonstrate true cortical activity preceding movement (Fang et al. 2004).
Statistical analysis
Paired t tests were used to compare force, EMG, and MRCP measures between pre- and post-tests. As multiple electrode sites were compared, we additionally performed a Hotelling T 2 test to maintain statistical power, as has been used previously in similar studies (Fang et al. 2004). For MVIC measures one-tailed tests were performed to compare force and EMG as these measures are known to increase with resistance training. Two-tailed tests were used to examine MRCP measures. Pearson correlation coefficients were computed to assess the relationships between MRCP measures and force and EMG during the submaximal protocol. Test–retest reliability was assessed via intraclass correlation coefficients (ICC3,1) (Weir 2005) and ICCs greater than 0.60 were considered acceptable (Chinn 1991). Data are presented as means ± SD and statistical significance was set at α ≤ 0.05.
Results
Reliability
ICCs for each MRCP measure all exceeded the 0.60 criterion for acceptability as follows: BP−600 to −500 = 0.77, MP−100 to 0 = 0.82, MMP0 to 100 = 0.89, onset latency = 0.92. No significant differences were observed between sessions for any of these measures across electrode sites (P > 0.05). For electrode position Cz, 95% confidence intervals were computed for the above measures to demonstrate observed variability for this subgroup; BP−600 to −500 = 0.10–7.5, MP−100 to 0 = 1.5–13.6, MMP0 to 100 = 1.5–15.2.
Maximal strength assessment
After 3 weeks of strength training, MVIC increased significantly by 21.6% from 1,479.6 ± 579.2 to 1,800.0 ± 533.6 N (P < 0.001). RFD also significantly increased by 31.6% from 5.3 ± 2.3 to 7.0 ± 2.6 N/ms (P < 0.001). In regards to EMG, no difference was found for EMGpk (P = 0.23), but a significant 47.2% increase was observed for EMG200 (P = 0.04).
Submaximal leg extension performance
After rejection of contaminated epochs, the average number of trials analyzed per subject was similar for pre- (34.2 ± 10.8) and post-tests (35.5 ± 12.5). Previous research has demonstrated that the MRCP is associated with the rate and magnitude of force production (do Nascimento et al. 2005; Siemionow et al. 2000; Slobounov et al. 2004); therefore, these variables before and after training were analyzed to assess their possible contribution to any MRCP effects. Overall, the findings indicated little if any change in submaximal force production. No differences (P > 0.05) were observed for mean force (pre: 277.4 ± 35 N; post: 282.9 ± 22 N) or RFD (pre: 2.6 ± 1 N/s, post: 2.2 ± 1 N/s). Inter-trial response intervals, defined as the interval between the offset and onset of force production, was also similar between sessions before and after training (pre: 12.2 ± 1.7 s; post: 11.4 ± 2.4 s). Similarly, mean EMG amplitude (pre: 366.6 ± 186.2 μV; post: 378.4 ± 241.4 μV) and the onset of EMG (pre: −184.2 ± 93.9 s; post: −168.91 ± 90.7) were not significantly different (P > 0.05).
MRCP parameters
MRCP amplitude measures for Cz, C1, and C2 are illustrated in Fig. 2, and their resultant waveforms are illustrated in Fig. 4. Irrespective of measure, amplitudes generally were attenuated following resistance training at each of the electrode sites. However, these differences were statistically significant only for MP−100 to 0 and MMP0 to 100, as BP−600 to −500 did not satisfy the Hotelling t 2 test (P = 0.09). Our automatic detection methods were unable to consistently detect MRCP onsets at the C1 or C2 electrode sites, therefore latencies were computed only for Cz. A significant difference (P = 0.02) was observed for onset latency (pre: −1,939.9 ± 658.3; post: −1,378.2 ± 600.5), such that onsets, on average, began approximately 28% later at Cz after training. Visual inspection of the 2D topographical maps (Fig. 3) further confirms the attenuation of cortical activity during each of the three MRCP components. Note statistical analysis was not performed on these maps, which are used for the purposes of illustrating in general form the spatial features.

MRCP amplitude measures (μV), Note Amplitudes for each component before (black) and after (gray) training. Error bars are standard deviation. Hotelling t 2: † P < 0.05; Paired t test: **P < 0.01, *P < 0.05

2D topographical maps of component amplitudes, Note Each map is oriented such that the anterior–posterior axis is arranged vertically (i.e. nasion is located at the top)
No significant correlations were observed for the pre-testing session between MRCP measures and mean force or RFD (P > 0.05). However, mean EMG amplitude was significantly associated with MP−100 to 0 (r = 0.68; P = 0.03) and MMP0 to 100 (r = 0.64; P = 0.05), but only at electrode site C2. For post-testing, MMP0 to 100 at Cz was significantly correlated (r = 0.61; P = 0.05) with mean force. No other significant associations were observed for RFD or mean EMG amplitude during the post test.
Discussion
We hypothesized that following a brief program of resistance training, supraspinal adaptive changes would be reflected in the MRCP. As expected, this 3-week program elicited marked increases in MVIC, RFD, and EMG200 during maximal leg extensor contraction. For repetitive submaximal leg extensions, we observed attenuation of MRCP amplitude at several motor electrode sides, supporting our hypothesis that by increasing strength, comparable motor tasks may be performed with a lower level of neural effort.
We are confident that the observed changes were not artifactual in nature for two main reasons. First, we were able to demonstrate that MRCP are repeatable (ICCs = 0.77–0.92) for self-paced submaximal leg extensions, and without intervention, there were no changes in response amplitude measures or onset latencies as seen with our sub-group analysis. Second, we found no differences in the manner in which leg extensions were performed (e.g. force applied, RFD, inter-trial interval) as well the number of trials analyzed before and after training. In concert with the findings of significant differences in the associated MRCPs, these results indicate that MRCP may be a valuable method for evaluating adaptive neural changes in response to resistance training.
Implications for reduced cortical activity
If, secondary to resistance training, individual motor units are capable of producing more force, then fewer motor neurons are required to accomplish a given physical task. Presumably, a reduction in recruitment would be reflected in diminished cortical activation. Carroll et al. (2002) hypothesized that such a reduction would reduce activation of neural elements unrelated to the intended movement, thereby resulting in enhanced performance. As such, enhanced performance is likely to reflect a lower metabolic cost, as has been reported elsewhere. For example, elite rifle shooters consistently demonstrate decreased MRCP amplitude in comparison to novices (Di Russo et al. 2005), suggesting more efficient movement preparation and execution (Hatfield et al. 2004).
Such findings are consistent with results from the present study indicating that the amplitudes of later components, MP−100 to 0 and MMP0 to 100, were considerably reduced (effect sizes: 0.70–0.85) following 3 weeks of resistance training. It has previously been reported that these same time intervals (i.e. MP−100 to 0 and MMP0 to 100) are sensitive to inertial loading, whereby amplitudes are greater at appropriate electrode sites when loading is higher (Kristeva et al. 1990). In other words, when individuals were asked to perform muscle contractions under light- and heavy-loads, larger MP−100 to 0 and MMP0 to 100 responses (i.e. greater negativity) were observed under heavy-loading conditions. We consider these findings directly applicable to the present study in which subjects performed movements at a constant load prior to and following resistance training. At baseline, MP−100 to 0 and MMP0 to 100 amplitudes were 26.1–49.7% higher than after training. Since subjects experienced significant gains in MVIC (+21.6%) and RFD (31.6%), it is reasonable to assume that strength gain altered the level of relative loading in which the constant load became lighter after training and thus easier to perform. This is further confirmed by Slobounov et al. (2004) who reported MRCP amplitudes to proportionally increase as a function of perceived effort on the part of the subject.
In a cross-sectional study, the MRCP preceding wrist extensions was compared in athletes (e.g. kendoists, gymnasts) versus non-athletes (Kita et al. 2001). The authors reported that the early component (i.e. BP) in athletes had a later onset and reduced amplitude in comparison to non-athletes. Similarly, we observed that the onset of negativity at electrode site Cz occurred approximately 561 ms later following training (Fig. 4). However, we did not find a significant decrease in amplitude at BP−600 to −500 in our multi-channel comparison (t 2; P = 0.09), but believe this to be reflective of statistical power as a substantial reduction in amplitude (e.g. 43–67%) was observed after training. Post hoc power analysis using our sample size, α = 0.05, and our observed effect size d = 0.80 yielded an achieved power estimate of 1 − β = 0.66. Thus, although care must be taken in interpreting such results, a non-significant trend towards decreased BP−600 to −500 was observed.

Grand average waveforms of MRCP and multi-channel display. Note Grand average waveforms are presented for Cz, C1, and C2 both before (black) and after (gray) training. Dashed line represents the onset of movement. Multiple electrode sites around those of interest (e.g. Cz, C1, C2) are also displayed
In the study of Kita et al. (2001), the distributions of potentials between athletes and non-athletes were also compared using topographical maps (cf. Fig. 2; Kita et al. 2001). These maps indicated that activity was significantly more localized in athletes. The authors speculated that habitual training involving wrist extensions caused initially diffuse brain activation to become specific. Evidence of increased spatial localization of potentials was also observed in the topographical maps of the present study (Fig. 3). It is important to note that the absence of the lateralized activity normally associated with upper extremity movements is not surprising given the arrangement of the motor homunculi and is consistent with the findings of other studies examining lower extremity recordings (Luft et al. 2002; Wheaton et al. 2007). Finally, it is interesting to observe changes after only nine training sessions in contrast to the years of habitual training examined by the Kita et al. (2001) study.
Comparison to evoked responses
Our findings are convergent with prior demonstrations of attenuated cortical activity in response to short-term training. Taube et al. (2007) reported a reduction in corticospinal excitability that was correlated with improved motor performance (e.g. postural stability) following 4 weeks of balance training. Excitability was assessed using a collision technique of sub-threshold TMS and H-reflex as described elsewhere (Nielsen and Petersen 1995). In brief, this technique is able to attenuate the influence of spinal excitability by adjusting the H-reflex to a specific level, therefore if changes are observed they are most likely reflective of cortical excitability (Taube et al. 2007). As a result, conditioning of the H-reflex with TMS is considered more reliable than TMS alone to infer changes in cortical excitability (Misiaszek 2003). Schubert et al. (Schubert et al. 2008) also used the conditioned H-reflex to identify supraspinal changes in response to either 4 weeks of balance or explosive resistance training of the lower limbs. Both balance and resistance training improved RFD concomitant with a diminished facilitation of the conditioned H-reflex after training. In addition, they also observed no adaptation in reflex gain via the unconditioned reflex, suggesting that changes in the firing rate or intrinsic properties of spinal motor neurons were not responsible for the modulation of the conditioned H-reflex (Schubert et al. 2008). Consequently, observed changes were interpreted mainly as changes in cortical excitability.
Schubert and colleagues’ interpretation is in contrast to Carroll et al. (2002) who suggest that resistance training does not elicit substantial modification of motor cortical centers; rather, it exhibits its greatest influence on the functional properties of the spinal cord circuitry. In that study, subjects performed 4 weeks of resistance training of the first dorsal interosseous. After training, MVIC increased by 33%, but no change in TMS-induced MEPs was evident at rest or at contraction intensities below 40% MVIC. Only at higher contraction intensities (i.e. 40–60%) were MEPs reduced. Similarly, Jensen et al. (2005) found no evidence of increased cortical excitability following 4 weeks of biceps brachii resistance training that increased MVIC by 32%. Unlike Carroll and colleagues, they observed a significant depression in maximal MEP amplitude at rest, and only a similar trend during tonic contraction. Decreased corticospinal excitability at rest was not correlated to changes with strength, leading the authors to suggest that the observed strength gain was unrelated to cortical changes.
Jensen et al. (2005) suggested that slight differences between their findings and that of Carroll et al. (2002) may be explained by the variability of recordings during voluntary contractions, supported by the finding that cortical and spinal excitability is better maintained at low intensity stable contractions (Darling et al. 2006). This variability underscores the role of voluntary effort and lack of consistency amongst studies. For example, Griffin and Cafarelli (2007) found no changes in MEP at rest following 4 weeks of plantar-flexion resistance training, but found a 32% increase in MEP during a 10% MVIC contraction. Although Jensen and colleagues studied the upper extremity, they did not find an increase in MEP during a baseline contraction of 5% MVIC. Presumably, techniques such as the conditioned H-reflex (Schubert et al. 2008; Taube et al. 2007) as well as the methods of the present study may circumvent some limitations related to voluntary effort.
Paradigm considerations
Direct comparisons of results of the present study to those utilizing evoked responses are difficult for several reasons. Foremost, interpretations of volitional drive and/or cortical excitability are drawn from peripheral EMG assessment whereas the present study records activity at the level of the cortex. Moreover, in order to resolve the MRCP from spontaneous EEG activity, multiple trials are necessary in order to generate a stable average and improve signal to noise ratio. As such, MRCP data were obtained at submaximal intensity. If data were recorded during repetitive maximal contractions, the MRCP signal would be subject to the effects of fatigue which would significantly influence our results (Schillings et al. 2006). To this end, our design may not reflect the full range of neural adaptation (i.e. low to high intensity force exertion), which may be a design limitation. What the MRCP protocol does provide is a measure during more natural repetitive movement which is distinct from H-reflex or MEP designs that elicit a response at rest or during tonic contraction. While MRCPs may rely more directly on central nervous system activity, evoked response may be more conducive for evaluating the functional state of the corticospinal pathway as they represent excitatory and inhibitory interactions occurring at various levels of the neuraxis (Bonato et al. 2006). Unique features of each technique contribute to the understanding of cortical reactivity and connectivity and its resultant adaptations, as underscored by recent technical advances permitting the combination of TMS-EEG (Miniussi and Thut 2010). Future studies are warranted to compare changes amongst MRCP characteristics with modifications of cortical and spinal excitability.
We acknowledge that the present investigation lacks a detailed assessment of peripheral adaptation (i.e. EMG sites). Due to practical limitations (e.g. available channels for bipolar recording), we were unable to assess the full musculature involved in the leg extension task. This may be a potential shortcoming by limiting our ability to quantify the relative amount of central and peripheral adaptation that occurs in response to resistance training. Future studies should consider a larger EMG recording montage.
The present study is unique in many aspects. This is the first study to report supraspinal adaptations in response to short-term resistance training using the MRCP paradigm. Moreover, recordings of MRCP associated with lower-extremity movements have been infrequently obtained (Wheaton et al. 2007). To the knowledge of these authors, an examination of multi-joint movements as employed here has not been previously performed. The greater MRCP responses in comparison to reports in the existing literature may, in fact, be the result of performing movements requiring action across several joints. This is in agreement with increased responses observed when movements are more complex (Fang et al. 2001, 2004). The multi-joint training protocol is also unique to the literature investigating neural adaptive effects with short-term resistance training which has primarily studied single-joint actions such as index finger flexion (Carroll et al. 2002), ulnar deviation (Farthing et al. 2007), elbow- (Jensen et al. 2005), and plantar-flexion (Del Balso and Cafarelli 2007; Gondin et al. 2006; Holtermann et al. 2007; Lagerquist et al. 2006). We note in passing the importance of these findings in suggesting that the MRCP method may be useful in the study of multi-joint movements relating to key daily activities including gait and the maintenance of posture.
Conclusion
In advance of significant muscle architectural and contractile changes in the first few weeks of a program of resistance training, neural adaptive effects are thought to predominantly govern the observed increases in force output (i.e. MVIC). Evidence of adaptation at multiple levels of the neuraxis has been reported previously (Aagaard 2003; Folland and Williams 2007; Gabriel et al. 2006; Griffin and Cafarelli 2005), yet direct evidence of supraspinal adaptation has been lacking. The present data are consistent with the conclusion that supraspinal adaptations reflect enhanced neural economy. These insights into the mechanisms of neuronal plasticity have implications for disciplines such as neurorehabilitation. The MRCP protocol offers an important approach to the study of early phase neural adaptations during a program of resistance training.
References
Aagaard P (2003) Training-induced changes in neural function. Exerc Sport Sci Rev 31:61–67
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P (2002) Neural adaptation to resistance training: changes in evoked V-wave and H-reflex responses. J Appl Physiol 92:2309–2318
Adamson M, Macquaide N, Helgerud J, Hoff J, Kemi OJ (2008) Unilateral arm strength training improves contralateral peak force and rate of force development. Eur J Appl Physiol 103:553–559
Bawa P (2002) Neural control of motor output: can training change it? Exerc Sport Sci Rev 30:59–63
Behm DG, Sale DG (1993) Intended rather than actual movement velocity determines velocity-specific training response. J Appl Physiol 74:359–368
Bonato C, Miniussi C, Rossini PM (2006) Transcranial magnetic stimulation and cortical evoked potentials: a TMS/EEG co-registration study. Clin Neurophysiol 117:1699–1707
Carroll TJ, Riek S, Carson RG (2002) The sites of neural adaptation induced by resistance training in humans. J Physiol 544:641–652
Chinn S (1991) Statistics in respiratory medicine. 2. Repeatability and method comparison. Thorax 46:454–456
Darling W, Wolf S, Butler A (2006) Variability of motor potentials evoked by transcranial magnetic stimulation depends on muscle activation. Exp Brain Res 174:376–385
Del Balso C, Cafarelli E (2007) Adaptations in the activation of human skeletal muscle induced by short-term isometric resistance training. J Appl Physiol 103:402–411
del Olmo MF, Reimunde P, Viana O, Acero R, Cudeiro J (2006) Chronic neural adaptation induced by long-term resistance training in humans. Eur J Appl Physiol 96:722–728
Di Russo F, Pitzalis S, Aprile T, Spinelli D (2005) Effect of practice on brain activity: an investigation in top-level rifle shooters. Med Sci Sports Exerc 37:1586–1593
do Nascimento OF, Nielsen KD, Voigt M (2005) Relationship between plantar-flexor torque generation and the magnitude of the movement-related potentials. Exp Brain Res 160:154–165
Duchateau J, Enoka RM (2002) Neural adaptations with chronic activity patterns in able-bodied humans. Am J Phys Med Rehabil 81:S17–S27
Duclay J, Martin A, Robbe A, Pousson M (2008) Spinal reflex plasticity during maximal dynamic contractions after eccentric training. Med Sci Sports Exerc 40:722–734
Fang Y, Siemionow V, Sahgal V, Xiong F, Yue GH (2001) Greater movement-related cortical potential during human eccentric versus concentric muscle contractions. J Neurophysiol 86:1764–1772
Fang Y, Siemionow V, Sahgal V, Xiong F, Yue GH (2004) Distinct brain activation patterns for human maximal voluntary eccentric and concentric muscle actions. Brain Res 1023:200–212
Farthing JP, Borowsky R, Chilibeck PD, Binsted G, Sarty GE (2007) Neuro-physiological adaptations associated with cross-education of strength. Brain Topogr 20:77–88
Fimland MS, Helgerud J, Gruber M, Leivseth G, Hoff J (2009) Functional maximal strength training induces neural transfer to single-joint tasks. Eur J Appl Physiol 107:21–29
Folland JP, Williams AG (2007) The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Med 37:145–168
Gabriel DA, Kamen G, Frost G (2006) Neural adaptations to resistive exercise: mechanisms and recommendations for training practices. Sports Med 36:133–149
Gondin J, Duclay J, Martin A (2006) Soleus- and gastrocnemii-evoked V-wave responses increase after neuromuscular electrical stimulation training. J Neurophysiol 95:3328–3335
Griffin L, Cafarelli E (2005) Resistance training: cortical, spinal, and motor unit adaptations. Can J Appl Physiol 30:328–340
Griffin L, Cafarelli E (2007) Transcranial magnetic stimulation during resistance training of the tibialis anterior muscle. J Electromyogr Kinesiol 17:446–452
Hakkinen K, Komi PV, Alen M (1985) Effect of explosive type strength training on isometric force- and relaxation-time, electromyographic and muscle fibre characteristics of leg extensor muscles. Acta Physiol Scand 125:587–600
Hatfield BD, Haufler AJ, Hung TM, Spalding TW (2004) Electroencephalographic studies of skilled psychomotor performance. J Clin Neurophysiol 21:144–156
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10:361–374
Holtermann A, Roeleveld K, Engstrom M, Sand T (2007) Enhanced H-reflex with resistance training is related to increased rate of force development. Eur J Appl Physiol 101:301–312
Jensen JL, Marstrand PCD, Nielsen JB (2005) Motor skill training and strength training are associated with different plastic changes in the central nervous system. J Appl Physiol 99:1558–1568
Kita Y, Mori A, Nara M (2001) Two types of movement-related cortical potentials preceding wrist extension in humans. Neuroreport 12:2221–2225
Kristeva R, Cheyne D, Lang W, Lindinger G, Deecke L (1990) Movement-related potentials accompanying unilateral and bilateral finger movements with different inertial loads. Electroencephalogr Clin Neurophysiol 75:410–418
Kvorning T, Bagger M, Caserotti P, Madsen K (2006) Effects of vibration and resistance training on neuromuscular and hormonal measures. Eur J Appl Physiol 96:615–625
Lagerquist O, Zehr EP, Docherty D (2006) Increased spinal reflex excitability is not associated with neural plasticity underlying the cross-education effect. J Appl Physiol 100:83–90
Luft AR, Smith GV, Forrester L, Whitall J, Macko RF, Hauser TK, Goldberg AP, Hanley DF (2002) Comparing brain activation associated with isolated upper and lower limb movement across corresponding joints. Hum Brain Mapp 17:131–140
Miniussi C, Thut G (2010) Combining TMS and EEG offers new prospects in cognitive neuroscience. Brain Topogr 22:249–256
Misiaszek JE (2003) The H-reflex as a tool in neurophysiology: its limitations and uses in understanding nervous system function. Muscle Nerve 28:144–160
Munn J, Herbert RD, Hancock MJ, Gandevia SC (2005) Training with unilateral resistance exercise increases contralateral strength. J Appl Physiol 99:1880–1884
Nielsen J, Petersen N (1995) Evidence favouring different descending pathways to soleus motoneurones activated by magnetic brain stimulation in man. J Physiol 486(Pt 3):779–788
Ranganathan VK, Siemionow V, Liu JZ, Sahgal V, Yue GH (2004) From mental power to muscle power-gaining strength by using the mind. Neuropsychologia 42:944–956
Schillings ML, Kalkman JS, van der Werf SP, Bleijenberg G, van Engelen BG, Zwarts MJ (2006) Central adaptations during repetitive contractions assessed by the readiness potential. Eur J Appl Physiol 97:521–526
Schubert M, Beck S, Taube W, Amtage F, Faist M, Gruber M (2008) Balance training and ballistic strength training are associated with task-specific corticospinal adaptations. Eur J Neurosci 27:2007–2018
Shibasaki H, Hallett M (2006) What is the Bereitschaftspotential? Clin Neurophysiol 117:2341–2356
Sidaway B, Trzaska AR (2005) Can mental practice increase ankle dorsiflexor torque? Phys Ther 85:1053–1060
Siemionow V, Yue GH, Ranganathan VK, Liu JZ, Sahgal V (2000) Relationship between motor activity-related cortical potential and voluntary muscle activation. Exp Brain Res 133:303–311
Slobounov SM, Ray WJ (1998) Movement-related potentials with reference to isometric force output in discrete and repetitive tasks. Exp Brain Res 123:461–473
Slobounov S, Hallett M, Newell KM (2004) Perceived effort in force production as reflected in motor-related cortical potentials. Clin Neurophysiol 115:2391–2402
Taube W, Gruber M, Beck S, Faist M, Gollhofer A, Schubert M (2007) Cortical and spinal adaptations induced by balance training: correlation between stance stability and corticospinal activation. Acta Physiol (Oxf) 189:347–358
Taube W, Leukel C, Schubert M, Gruber M, Rantalainen T, Gollhofer A (2008) Differential modulation of spinal and corticospinal excitability during drop jumps. J Neurophysiol 99:1243–1252
Thomas S, Reading J, Shephard R (1992) Revision of the physical activity readiness questionnaire (PAR-Q). Can J Sport Sci 17:338–345
Van Cutsem M, Duchateau J, Hainaut K (1998) Changes in single motor unit behaviour contribute to the increase in contraction speed after dynamic training in humans. J Physiol 513(Pt 1):295–305
Viitasalo JT, Saukkonen S, Komi PV (1980) Reproducibility of measurements of selected neuromuscular performance variables in man. Electromyogr Clin Neurophysiol 20:487–501
Weir JP (2005) Quantifying test–retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res 19:231–240
Wheaton LA, Mizelle JC, Forrester LW, Bai O, Shibasaki H, Macko RF (2007) How does the brain respond to unimodal and bimodal sensory demand in movement of the lower extremity? Exp Brain Res 180:345–354
Yue G, Cole KJ (1992) Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. J Neurophysiol 67:1114–1123
Acknowledgments
Authors would like to thank Drs. Andrey Anokhin, Simon Golosheykin, and Sean Kristjansson for their technical expertise and guidance; Paula Stewart and Corey Lohnes for their assistance in data collection; and Joshua Funk for the creation of figures and illustrations. Direct support for this research was provided by National Strength and Conditioning Association (M.J. Falvo), and Missouri Physical Therapy Association (G.M. Earhart). Additional support was provided by NIH grants T32HD007434 (Program in Physical Therapy) and 1K01HD048437 (G.M. Earhart).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Susan Ward.
Rights and permissions
About this article
Cite this article
Falvo, M.J., Sirevaag, E.J., Rohrbaugh, J.W. et al. Resistance training induces supraspinal adaptations: evidence from movement-related cortical potentials. Eur J Appl Physiol 109, 923–933 (2010). https://doi.org/10.1007/s00421-010-1432-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1432-8