
Abstract
To investigate thermal responses of children during cold exposure, children and their mothers were exposed to identical environmental conditions in climatic chambers. Subjects comprised 14 mothers (age, 29–40 years) and 15 children (age, 15 months–3 years; 9 boys, 6 girls). Each mother and child wore a t-shirt and short pants over underwear. Subjects were initially seated in a chamber at 25°C for 60 min, then moved to a chamber at 15°C where they were seated for 30 min. During the recovery period, they were returned to the 25°C chamber and kept there for an additional 30 min. During exposure to 15°C, declines in skin temperature (T s) of the hand and foot were significantly greater in children than in mothers. Rectal temperatures (T re) of children increased during cold exposure, whereas T re of mothers decreased. This variation in T re in children might be linked to homodynamic alterations accompanied by greater decreases in T s of the extremities due to a greater degree of vasoconstriction in distal regions during cold exposure. Increases in T re during cold exposure for children correlated with body surface area to mass (Ab/mass), mass and decreases in T s of the abdomen, thigh and leg. During the rewarming period, children exhibited a greater increase in T s of the arm, hand and foot than mothers, and this was attributed to greater relaxation of vasoconstriction in distal regions of children during exposure to the thermoneutral environment. T re in children and mothers decreased during the rewarming period. A gender difference was found only with regard to T re and heart rate (HR) responses in children during cold exposure, and neither physical characteristics nor any T s differed between genders. Furthermore, no significant differences were observed in resting HR of mothers and girls, whereas boys showed significantly lower heart rates at 15°C than at 25°C.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Numerous studies have investigated the thermoregulatory responses of children during exercise in the heat, but few studies have examined the effects of cold exposure in children (Falk 1998). Eight-year-old swimmers were found to remain for a shorter period in water at 20.3°C and showed a greater drop in oral temperature when compared with older subjects (Sloan and Keatinge 1973). Cooling rate is related to an index of body surface area to mass (Ab/mass) and the inverse of subcutaneous adiposity. This data indicates the importance of body size in the thermoregulatory response to cold stimulus for children. Wagner et al. (1974) observed that during cold exposure (16–17°C), heat losses in 9 prepubertal boys (age, 10–13 years) were identical to those observed in men, but the prepubertal boys maintained a higher core temperature, higher metabolic rates and greater cutaneous vasoconstriction when compared with the men. This finding indicates that prepubertal boys are able to compensate for greater Ab/mass ratios by increased cutaneous vasoconstriction. Conversely, with declining ambient temperature from 28 to 15°C over 60 min, decreases in skin temperature (T s) and rectal temperature (T re) were significantly greater for 8-year-old boys than for men, as increase in metabolic rates were significantly lower in the boys than in the men (Inoue et al. 1996). Subjects in these previous studies have predominantly comprised prepubertal boys (age 8–13 years), and comparisons were made to young men. No other age groups have been investigated to assess thermoregulatory responses to cold stimulus in children, with the exception of babies in hospital (Bruck 1961). Moreover, women have been found to be at a severe disadvantage due to a far greater heat loss-to-production (surface-to-mass) ratio compared to their male counterparts in extreme cold and a greater percentage of body fat further reduces relative size of the active (heat-producing) body mass (Burse 1979). Men may be more metabolically sensitive than women to cold air stress and also respond to cold air with bradycardia and increased stroke volume, while women show no such changes in these parameters (Stevens et al. 1987; Graham and Lougheed 1985). Furthermore, Bollinger and Schlumph (1976) found that women display reduced arterial inflow compared to men in response to direct air cooling to the finger, thus indicating even greater susceptibility to cold injury (Burse 1979). Preschool children are mainly cared for at home by their mothers (Tsuzuki et al. 2001). Indeed, since behavioral thermoregulatory strategies such as clothing and alterations in thermal environment are lacking, children are dependent on their mothers to maintain thermal equilibrium. According to a Japanese legend, children can tolerate a cold environment, without perishing under its effect. There are few evidences or studies that explain thermoregulation and perception of cold in young children. The following experiment was conducted to investigate thermoregulatory responses of young children with that of their mothers during cold exposure. In addition, very little has been reported regarding girls in body temperature and heart rate responses to cold. A comparison was performed to investigate gender differences in thermoregulatory responses within young children.
Methods
Subjects
The subjects comprised 14 mothers (aged 29–40 years) and 15 children (aged 15 months–3 years; 9 boys and 6 girls). The physical characteristics of the subjects are described in Table 1.
Environments
Two adjoining chambers were used; the chambers were equipped with their own set of environmental controls. One of the chambers was kept at an ambient temperature (T a) of 25°C; the relative humidity (rh) was 50%; and the air velocity (v) was less than 0.2 m/s. In the other chamber, the corresponding values of T a, rh, and v were 15°C, 50%, and less than 0.3 m/s, respectively.
Clothing
T-shirts and short pants of the same design and fabric as those commonly worn during the summer season were obtained in different sizes for the experiment. Mothers wore them over their bra and underpants, while the children wore them over their underpants or a disposable diaper. They did not wear socks or shoes.
Procedure
The purpose and procedures of this experiment were verbally explained and also provided in writing to individual mothers. Prior informed consent was obtained from each mother and that for children were obtained from their parents to ensure their voluntary participation in this study. This study was approved by the Human Ethics Committee of the Human-Environment System Department at the National Institute of Bioscience and Human-Technology (formerly AIST).
First, the subjects were weighed with their T-shirts and short pants and were instructed to remain seated for at least 60 min while the necessary transducers were affixed to their bodies. Subsequently, the subjects were instructed to enter the adjacent cold room and sit quietly for 30 min. After the cold exposure, they returned to the 25°C chamber where they remained for an additional 30 min. With exception of the time required to switch chambers, the subjects remained seated and watched the same videotapes during the experiment. A child and his/her mother were made to sit separately and watch a video in order to maintain a resting state. The mother did not hold her child in the experiment. The exposure time to the cold environment was 30 min that was determined based on the results of a preliminary experiment wherein the child was unable to tolerate the cold and maintain a resting position when the total experiment time was more than 2 h. We did not consider 30 min as sufficient exposure time to the cold environment, however, Wagner et al. (1974) had conducted an experiment with 30-min exposure to cold (17°C) for 10- to 13-year-old boys. In our experiment, we selected 15°C and 30 min exposure as the conditions of the cold environment; the subjects were provided with a T-shirt and a pair of shorts but no socks. All experiments were carried out in winter (cold) season (from January to February). The experiments started at 1000 hours in the morning.
Measurements
The body surface area (Ab, m2) of all the subjects were estimated from their height (h, cm) and body mass (mass, kg) data according to the following equations of Fujimoto et al. (1967):
Skinfold thickness was measured using a skinfold caliper in the triceps, subscapular, and abdominal regions.
Temperature data were continuously recorded by using a thermistor probe and data logger (LT8A, Gram Corporation) at 30-s time intervals. Rectal temperature (T re) was used as a measure of the core body temperature and recorded using a thermistor probe (401J, Nikkiko-YSI, Japan) that was inserted 12 and 10 cm beyond the anal sphincters of the mothers and the children, respectively. Skin temperatures (T s) were measured by using thermistors that were affixed to the skin surfaces of the forehead, abdomen, arm, hand, thigh, leg, and foot by means of adhesive surgical tapes. Except abdomen other skin area for T s measured were exposed to the ambient air and not covered by the clothing. Mean skin temperature (T sk) was calculated according to the following equation of Hardy and DuBois (1937):
The heart rate (HR) values were recorded at 30-s intervals by using memory type heart rate monitors (VHM1-016, VINE Co. Limited, Japan) and given by beats min−1.
Statistical analysis
For the purpose of statistical analysis, the T s and T re values were averaged during 5 min for each subject. To investigate the effect of age on thermal responses, we compared the children group with the mother group; similarly, to investigate the effect of gender, we compared the boys and girls within the children group. Student t test was performed to assess the differences in the physical characteristics. A one-way ANOVA with repeated measures was used to compare the T s, T sk, T re, and HR values at the end of control, cold exposure and recovery period between the children and mothers and between the boys and girls. Fisher’s PLSD was used for the post-hoc pair wise comparison. The level of significance was considered to be P < 0.05. Student t test was performed to assess the rates of change in the T s, T sk, and T re values during exposure to cold and rewarm periods between the children and mothers and between the boys and girls. Especially for children group, the rate of change in the T re was calculated by subtracting the control value obtained at the end of control period from the maximum T re value during exposure to cold. The exposure time was also calculated from the point of cold exposure when the maximum T re value was obtained. Correlational analyses were used to examine relationships among physical characteristics, including height, mass, body surface area to mass ratio, skinfold thickness, age, and rates of change in the T re, T sk and T s at seven sites during cold period. To incorporate any influence of gender into the correlational analysis, a point-biserial correlation using categorical data for gender was employed (boys = 1, girls = 2). After a significant gender difference was detected, correlational analyses were performed separately to examine these relationships for the boys and girls. Direct correlational inquiries were conducted using Pearson product-moment correlations. The significance of correlations was established at 5% probability level.
Results
There were significant differences with regard to the physical characteristics of the subjects between the children and mothers. The children had a greater Ab/mass ratio, lower height and body mass, and lower skinfold thickness when compared with the corresponding values in the mothers (Table 1). The physical characteristics of the children were in the range of 22–55% of the corresponding values in the mothers except with regard to the Ab/mass ratio. The Ab/mass ratio in children was 163% of the corresponding value in the mothers. In children, these physical characteristics were examined for any gender-related differences, and it was proven that there was no significant influence of gender on the physical characteristics of children.
Figure 1 shows the time courses of changes in the T re, T sk, and local T s values at seven sites for both the groups. At the end of the 25°C control period, the children had significantly higher T s values in the abdomen [mean (SD) 35.6 (0.7) and 34.7°C (1.5) for the children and mothers, respectively] and lower T s values in the hand [33.2 (0.8) and 33.8°C (0.7) for the children and mothers] and arm [31.6 (0.5) and 32.1°C (0.7) for the children and mothers] when compared with the corresponding values in the mothers. However, there were no significant differences in the T re [37.4 (0.2) and 37.4°C (0.2) for the children and mothers], T sk, and T s values in the head, thigh, leg, and foot regions at the end of the control period prior to the cold exposure.

Comparison of time course of rectal temperature (T re), mean skin temperature (T sk), local skin temperature (T s) for head, abdomen, arm, hand, thigh, leg and foot during the experiment. *P < 0.05 and **P < 0.01 shows the difference between the young children and mothers at the 25°C control period, the end of cold exposure and the end of 25°C recovery period. #P < 0.05, ##P < 0.01 and ###P < 0.001 shows the difference between the children and mothers during the cold exposure and the thermo-neutral exposure of recovery period
The T s values of all subjects decreased when they moved to the cold chamber. At the end of the cold exposure, the T s values of the arm [25.7 (1.2) and 27.1°C (2) for the children and mothers, respectively] and hand [24.7 (2.2) and 28.1°C (1.1) for the children and mothers] were significantly lower in the children than in the mothers; however, there were no significant differences in the T s values at other sites. The T re values of the children gradually increased [37.5°C (0.3) for the children] when the subjects moved to the cold chamber, on the other hand, the T re values of the mothers decreased slightly during the cold exposure [37.3°C (0.2) for the mothers]. The T re values of the children were significantly higher than that of the mothers at the end of cold exposure. During the recovery period, the T re values of the children decreased after a slight delay and the T re values of the mothers continued to decrease further during the recovery period following the cold exposure. The T re values of the children [37.3°C (0.2)] tended to be higher than that of the mothers [37.1°C (0.4)] at the end of rewarming period (P = 0.06). The T s values of all subjects increased when they moved to the warm chamber from the cold chamber. During the recovery period, there were no significant differences in the T s values at all sites between the children and mothers. However, the T s values at arm, hand, leg and foot were significantly lower at rewarming period than those at the end of control period.
On the rates of change in T s during cold exposure, the decreases in the T s values of the hand [−8.5 (2.2) and −5.7°C (0.8) for the children and mothers, respectively] (P < 0.001) and foot [−7.3 (1.4) and −6°C (1) for the children and mothers] (P < 0.05) during cold exposure were significantly greater in the children than in the mothers although there were no significant differences in the variation of T s values at other sites between the two groups. There was significant difference in the variation in the T re values between the children and the mothers [0.1 (0.1) and −0.1°C (0.1) for the children and mothers, respectively] during the cold exposure (P < 0.001). During rewarming phase the increases in T s values for the arm [4.6 (1.2) and 3.7°C (1.2) for the children and mothers, respectively] (P < 0.05), hand [6.4 (2.1) and 3.2°C (1.3) for the children and mothers] (P < 0.001), and foot [3.5 (1.5) and 2.5°C (1.1) for the children and mothers] (P < 0.05) were significantly greater in the children than in the mothers. There was no significant difference in the variation in the T re values between the children and mothers during the recovery period.
Table 2 shows average heart rate (HR) of the children and mother groups during control, cold exposure and rewarming phase. There was a significant difference in the average HR between the children and the mothers (P < 0.0001), although no significant difference was found among the conditions. The average HR of the children was significantly higher than that of the mothers in the control, cold, and rewarming periods. The average HR of the mothers was not significantly different among the three conditions (P = 0.8). However, the average HR of the children was significantly lower during cold exposure than that during control and rewarming periods (P < 0.01) while there was no significant difference in the HR between control and rewaming period.
Boys-girls comparison
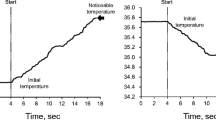
There was no significant difference between the rectal temperature (T re) of boys [37.4 (0.2)°C] and girls [37.4 (0.3)°C] in the control period. The rate of change due to the cold exposure and the subsequent rewarming is shown in Fig. 2. This graph shows that the T re of boys increased during the first half of the cold exposure and then decreased gradually in the latter half of the cold exposure and the subsequent rewarming period. Contrastingly, the T re of girls continued to increase during the entire period of the cold exposure and then decreased, with a slight delay, when the girls were moved to a warm room for rewarming. During the rewarming period, the T re of the girls appeared to decrease more steeply than that of the boys. Significant effect of interaction of gender and condition was found on T re in the control, cold, and rewarming periods although post-hoc comparison did not show significant difference in the T re between the boys and girls. Due to the cold exposure, the maximum increase in the T re was 0.1 (0.1) and 0.3 (0.1)°C, and the duration of increase was 19 (9) and 30 (6) min for the boys and girls, respectively. The rate of increase in the T re was 0.008 (0.004) and 0.009 (0.004)°C min−1 for the boys and girls, respectively. The increase in the T re due to the cold exposure was significantly greater (P < 0.07) and the duration of increase was longer (P < 0.02) for the girls than for the boys; however, no significant difference was observed in the rate of increase in the T re between the boys and girls. Due to the rewarming, the maximum decrease in the T re was 0.2 (0.1) and 0.4 (0.2)°C, and the duration of decrease was 21 (10) and 28 (2) min for the boys and girls, respectively. The rate of decrease in the T re was 0.01 (0.005) and 0.01 (0.006)°C min−1 for the boys and girls, respectively. The decrease in the T re due to rewarming was greater (P < 0.06) and the duration of decrease was longer (P < 0.06) for the girls than for the boys; however, no significant difference was observed in the rate of decrease in the T re between the boys and girls.

Comparison of time course of rectal temperature (Tre) of boys and girls during the experiment
Age and gender showed no significant correlations with physical characteristics such as skinfold thickness, mass, height, and Ab/mass ratio, as indicated by the correlation matrix presented in Table 3. The matrix also reveals a co-linearity between the Ab/mass ratio and mass; the latter exhibited a significant correlation with skinfold thickness. In addition, a significant correlation between height and mass was also found in the correlation matrix. There were significant correlations between the rate of change in the T re during cold exposure and mass, Ab/mass ratio, and gender. Nevertheless, the rate of change in the T re during the rewarming period correlated negatively with the rate of change in the T re during cold exposure and the Ab/mass ratio. The correlational analysis revealed significant differences between boys and girls. In boys, age significantly correlated with mass, height, and the Ab/mass ratio. On the other hand, in girls, the rate of change in the T re during cold exposure significantly correlated with mass and the Ab/mass ratio.
Although the average HR of the boys tended to be higher than that of the girls, there was no significant difference between their average HRs (P = 0.08) in Table 2. For the boys, the average HR was significantly lower in the cold than that in the control (P < 0.05) and rewarming (P < 0.001) environments; however, there was no significant difference between the average HR in the control and rewarming (P = 0.19) environments. There was no effect of the cold exposure on the average HR of the girls (P = 0.17).
Discussion
The main findings in the present study were that T s of the arm and hand were significantly lower and the rates of decrease in T s for the hand and foot were significantly greater during cold exposure in children than in mothers, although no significant difference in T sk and other T s values was found between mothers and children. Moreover, a transient rise in T re during cold exposure was observed only in children, not in mothers. A significantly greater decrease in distal T s was supported by previous studies that observed naked 8- to 12-year-old boys at 5, 15 and 17°C (Smolander et al. 1992; Inoue et al. 1996, 2006), and this was interpreted as reflecting greater cutaneous vasoconstriction. This interpretation was based on the findings of Wagner et al. (1974), who reported that boys exhibited a greater decrease in T s of the finger, arm and leg due to a greater decrease in blood flow in the finger and forearm in response to cold (16–17°C) compared to adults. Reduced limb T s in children may well be resulted from a diminution of arterial inflow to the deeper limb structures, as well as from generalized vasoconstriction of the cutaneous circulation as seen in women (Burse 1979). Arterial inflow to the fingers of women is normally only about half that of men, and women reduce arterial finger inflow much more than men in response to both indirect (foot) cooling and direct (finger) cooling (Bollinger and Schlumpf 1976). Clearly, lower limb T s due to the reduced heat inflow makes children much more susceptible to cold injury compared to adult women and especially men. However, other T s values except those of the extremities in children during cold exposure resembled those in mothers. T s responses during moderate cold exposure are modified by physical characteristics, particularly body adiposity and Ab/mass ratio (Buskirk et al. 1963; Bittel et al. 1988; Budd et al. 1991). Similar T s values in children and mothers can be explained by increased cooling stress coming from the combination of greater Ab/mass ratio and greater conductive heat loss due to less subcutaneous fat, which is offset by greater vasoconstriction (Inoue et al. 2006). Such a transient rise in T re has been observed previously in a study in which men were abruptly exposed to cold (Budd and Wrhaft 1966; Wagner et al. 1974; Wagner and Horvath 1985; Bittel et al. 1988), and was considered to be caused by either reduced return of cooled venous blood or compensatory vasodilatation in the intestinal blood vessels as generalized vasoconstriction develops in peripheral vessels (Budd and Wrhaft 1966). In previous studies, metabolic heat was reportedly more increased in boys than in men during cold exposure (Smolander et al. 1992; Wagner et al. 1974) and attributed to shivering (Budd and Warhaft 1966). Although we did not measure heat production, shivering was observed in children in the present study. The greater increase in T re for children might be induced by the redistribution of blood flow as well as increased heat production. Several investigations have revealed significant amounts of brown adipose tissue (BAT) in human prenatal offspring and newborns (Aherne and Hull 1966; Itoh and Kuroshima 1967). Because skeletal muscle function is not fully developed in a newborn, nonshivering thermogenesis is the principal mechanism of heat production in a postnatal infant. The presence of widely distributed BAT in the early years of life would appear to be related to the incomplete development of heat-regulating mechanisms at this time (Merklin 1974). After birth, the newborn increases heat production by nonshivering thermogenesis in the first half year of its life, while shivering thermogenesis is dominant thereafter (Hull and Smales 1978). BAT gradually disappears with advancing age (Heaton 1972). The children in the present study might possess BAT that might have increased nonshivering thermogenesis. However, it was also observed that all children exhibited horripilation, and in particular, most of the boys experienced shivering during the cold exposure. The heat production might have been insufficient, rendering the boys incapable of tolerating the decrease in their T re. Conversely, a decrease of only 0.1°C was observed in the T re in the control group, which comprised the mothers of the children used in the present study. This change in the T re was similar to that in the T re of adult men subjected to an environment at 16−17°C (Wagner et al. 1974). This might be because the mothers did not show a prompt and intense peripheral vasoconstriction since the temperature (15°C) was not too low for them. According to previous studies, women can tolerate a temperature of 10°C by minimizing heat loss from the body surface area without increasing their metabolic rate (Osada et al. 1972); further, women were not considered more metabolically sensitive to cold air than men (Stevens et al. 1987). In our experiment, the mothers exhibited a smaller decrease in the limb T s than the children at 15°C.
During the rewarming period, a significantly greater increase in T s of the arm, hand and foot of the children was observed when compared with corresponding values in mothers in the present study. However, aside from T s values of the extremities, other T s values were similar to those in mothers. This finding also suggests that children demonstrate a greater degree of relaxation of vasoconstriction during the rewarming phase compared to mothers. Consequently, a greater decline in T re was also observed in both children and mothers during the rewarming period, and was suggested to be due to renewed flow of blood through cold distal tissues as vasoconstriction relaxed (Budd and Wrhaft 1966).
T re, T sk and local T s values at seven sites were compared to investigate gender-related variations, but with the exception of T re, no significant differences were detected between boys and girls. During cold exposure, increases in T re were significantly greater in girls than in boys, although no significant difference was found in physical characteristics between boys and girls and average T s of the extremities tended to be lower in girls than in boys with no significant differences. We did not measure metabolic rate in the present study, and a difference of only a few percent between the metabolic rates of boys and girls has been reported (Davies 1996). This is therefore the first study to investigate relationships between variation in T re and T s, physical characteristics and gender for young children during cold exposure. Age and gender exhibited no significant correlations with physical characteristics such as skinfold thickness, mass, height or Ab/mass ratio in the correlation matrix. We confirmed a significant relationship between rates of change in T re during cold exposure and both mass and Ab/mass ratio, as reported by other studies (Slon and Keating 1973; McArdle et al. 1984; Kollias et al. 1974; White et al. 1992). However, rates of change in T re during cold and rewarming periods differed between gender in the present study, contradicting the result of a previous study in which cooling rates significantly correlated with mass, even though this relationship did not hold true across genders (White et al. 1992). In previous exercise studies, differences between genders with regard to T re response were apparent in exercise under cold conditions, in which premenarcheal girls displayed a significant decrease in T re (Klentrou et al. 2003), while prepubescent boys did not (Smolander et al. 1992) despite the absence of any difference in Ab/mass ratio or heat production. This difference in T re was suggested to be due to inadequate heat storage mechanisms in girls (Klentrou et al. 2003). In the present study T re in both boys and girls increased immediately after exposure to the cold environment. Nevertheless, T re in boys started to decrease earlier than that in girls in the middle of the cold exposure period in the present study. The matrix table showed no correlation between rate of change in T re and physical characteristics in boys, but age of boys was found to correlate with mass, height and Ab/mass ratio. Conversely, rate of change in T re during cold exposure for girls correlated significantly with mass and Ab/mass ratio. Moreover, changes in T re for children correlated with Ab/mass and decreased T s for the abdomen, thigh and leg. This means that the decrease in T s for the abdomen, thigh and leg became greater with smaller Ab/mass (greater mass). Likewise, the increase in T re of children became greater with smaller Ab/mass (greater mass). The increase in T re of children became greater with greater decreases in T s for the abdomen, thigh and leg during cold exposure. Boys in particular showed a correlation with changes in T re and decreases in T s for the abdomen and thigh, although girls did not show any correlation between decreases in T s and T re. The change in T s for the arm correlated with Ab/mass, fatness and age in boys. Although these correlations have been identified, no causal relationship is yet implied. As with all cross-sectional studies, statistical associations can only suggest, not prove, the existence of an underlying causal relationship (Budd et al. 1991). In the present study, neither the physical characteristics nor any T s differed between boys and girls. These results suggest that gender differences exist only with regard to changes in T re, and this might be due to differing metabolic rates or speeds of metabolic response as explained by Klentrou et al. (2003), but further investigation is required.
The mothers exhibited no HR alterations in the cold at rest, which confirmed the findings of Wagner and Horvath (1985) and Stevens et al. (1987). The average HR of the children was significantly higher than that of the mothers. Although the average HR of the boys tended to be higher than that of the girls, there was no significant difference between their average HRs. This might be because there was no significant difference between the boys and girls with regard to T s responses and body size. However, the boys exhibited significantly lower HR during cold exposure than that in the control and rewarming environments. This result was supported by their exercise HR, which was lower in 12-year-old boys at 10°C as compared to at 25°C and in 11- to 12-year-old boys at 7 and 13°C as compared to at 22°C (cited in Falk 1998). These HR results for the boys agree with the HR responses of adult men exposed to the cold. On the other hand, the girls did not show any significant decrease in their HRs due to the cold environment in the present study. There is limited information available regarding the cardiovascular response of the girls to the cold. These results for the girls correspond to those of the HR responses of the mothers in the present and previous studies (Wagner and Horvath 1985; Stevens et al. 1987). A gender-related difference in the HRs of the children, as indicated above, is similar to that observed for the HRs of adult men and women (Wagner and Horvath 1985; Stevens et al. 1987). HR alterations at rest during cold exposure might be natural for men since childhood. A possible interpretation is that lower HR during cold exposure represented a reflex response to vasoconstriction in the present study, as the children were inactive, watching television, and not exercising. However, the underlying mechanisms are not entirely clear, and further examination of cardiovascular responses of children to cold is required.
A gender difference was observed only with regard to the change in the T re and HRs of the children during the cold exposure. It is unknown whether this gender difference in the HRs is directly or indirectly related to the change in the T re. Previous investigators have reported that men at rest during cold exposure respond by increasing stroke volume and lowering their HRs (Budd and Warhaft 1966; Raven et al. 1970, 1975). The explanation that has been suggested (Raven et al. 1970, 1975) implies that skin vasoconstriction and cooling result in venoconstriction and enhanced venous return, resulting in increased stroke volume. This explanation supports the results obtained for the boys in the present study. However, neither the body size nor the T s differed between the boys and girls in the present study. Meanwhile, the HR of the girls did not reduce, while their T re continued to increase during the cold exposure. This finding might be explained by the different metabolic rates or speeds of metabolic response in the boys and girls. Moreover, the effectiveness of the mechanism underlying increased heat storage (Klentrou et al. 2003) might be due to a single factor that induces gender difference in this regard since birth.
In conclusion, T s for the arm and hand were significantly lower in children than in mothers, although no significant differences in T sk or other T s values were seen. This suggests that the disadvantageous morphological characteristics of children might be compensated for over a short period by stronger vasoconstriction during cold exposure. However, such cooler distal T s from reduced heat inflow might make children much more susceptible to cold injury. Increased T re in children during cold exposure might be a causal effect of greater decreases in T s for the abdomen, thigh and leg. Particularly for children, decreases in T s for the abdomen, arm and thigh significantly and negatively correlated with Ab/mass. Significant differences were observed in resting HRs of boys between 15 and 25°C and boys showed significantly lower HR at 15°C than at 25°C. A gender difference was found only with regard to T re and HR responses in children during cold exposure, and neither body size nor any T s differed between genders.
References
Aherne W, Hull D (1966) Brown adipose tissue and heat production in the newborn infant. J Pathol Bacteriol 91:223–234
Bittel JH, Nonotte-Varly C, Livecchi-Gonnot GH, Savourey GL, Hanniquet AM (1988) Physical fitness and thermoregulatory reactions in a cold environment in men. J Appl Physiol 65(5):1984–1989
Bollinger A, Schlumpf M (1976) Finger blood flow in healthy patients of different age and sex and in patients with primary Raynauds disease. Acta Chir Scand 465:42–47
Bruck K (1961) Temperature regulation in the newborn infant, Bil. Neonatorum 3:65–119
Budd GM, Warhaft N (1966) Body temperature, shivering, blood pressure and heart rate during a standard cold stress in Australia and Antarctica. J Physiol 186(1):216–232
Budd GM, Brotherhood JR, Hendrie AL, Jeffery SE (1991) Effects of fitness, fatness, and age on men’s responses to whole body cooling in air. J Appl Physiol 71(6):2387–2393
Burse RL (1979) Sex differences in human thermoregulatory response to heat and cold stress. Hum Factors 21:687–699
Buskirk ER, Thompson RH, Whedon GD (1963) Metabolic responses to cold air in men and women in relation to total body fat content. J Appl Physiol 18:603–612
Davies PSW (1996) Total energy expenditure in young children. Am J Hum Biol 8:183–188
Falk B (1998) Effects of thermal stress during rest and exercise in the paediatric population. Sports Med 25(4):221–240
Fujimoto K, Watanabe T, Sakamoto A, Yukawa K, Morimoto K (1967) Studies on the physiological area of Japanese 18. Calculation formula in three stages over all age (in Japanese). Jpn J Hyg 21:443–450
Graham TE, Lougheed MD (1985) Thermal responses to exercise in the cold: influence of sex differences and alcohol. Hum Biol 57(4):687–698
Hardy JD, DuBois E (1937) The technic of measuring radiation and convection. Nutrition 15(5):461–475
Heaton JM (1972) The distribution of brown adipose tissue in the human. J Anat 112(1):35–39
Hull D, Smales ORC (1978) Heat production in the newborn. In: Sinclair JC (ed) Temperature regulation and energy metabolism in the newborn. Grune & Stratton, New York, pp 129–156
Inoue Y, Araki T, Tsujita J (1996) Thermoregulatory responses of prepubertal boys and young men in changing temperature linearly from 28 to 15°C. Eur J Appl Physiol 72:204–208
Inoue Y, Nakamura S, Yonehiro K, Kuwahara T, Ueda H, Araki T (2006) Regional differences in peripheral vasoconstriction of prepubertal boys. Eur J Appl Physiol 96(4):397–403
Itoh S, Kuroshima A (1967) Distribution of brown adipose tissue in Japanese newborn infants. J Physiol Soc Jpn 29:660–661
Klentrou P, Cunliffe M, Slack J, Wilk B, Bar-Or O, De Souza MJ, Plyley M (2003) Temperature regulation during rest and exercise in the cold in premenarcheal and menarcheal girls. J Appl Physiol 96(4):1393–1398
Kollias J, Barlett L, Bergsteinova V, Skinner JS, Buskirk ER, Nicholas WC (1974) Metabolic and thermal responses of women during cooling in water. J Appl Physiol 36:577–580
McArdle WD, Magel JR, Gergley TJ, Spina RJ, Toner MM (1984) Thermal adjustment to cold-water exposure in resting men and women. J Appl Physiol 56(6):1565–1571
Merklin RJ (1974) Growth and distribution of human fetal brown fat. Anat Rec 178:637–646
Osada Y, Yoshida K, Ogawa S, Hirokawa A, Kikuchi K, Ohkubo C (1972) On the difference between men and women in their response to cold. Bull Inst Public Health (Tokyo) 21(2):60–67
Raven PB, Niki I, Dahms TE, Horvath SM (1970) Compensatory cardiovascular responses during an environmental cold stress, 5°C. J Appl Physiol 29:417–421
Raven PB, Wilkerson JE, Horvath SM, Bolduan NW (1975) Thermal, metabolic, and cardiovascular responses to various degrees of cold stress. Can J Physiol Pharmacol 53:293–298
Sloan REG, Keatinge WR (1973) Cooling rates of young people swimming in cold water. J Appl Physiol 35(3):371–375
Smolander J, Bar-or O, Korhonen O, Ilmarinen J (1992) Thermoregulation during rest and exercise in the cold in pre-and early pubescent boys and in young men. J Appl Physiol 72(4):1589–1594
Stevens GH, Graham TE, Wilson BA (1987) Gender differences in cardiovascular and metabolic responses to cold and exercise. Can J Physiol Pharmacol 65(2):165–171
Tsuzuki K, Iizuka S, Mitsutsuji S, Ikeda A, Tomita J, Tohihara Y, Ohnaka T (2001) Typical thermal environment for young children dwelling in and around the Tokyo metropolitan area. J Home Econ 52(5):429–438
Wagner JA, Robinson S, Marino RP (1974) Age and temperature regulation of humans in neutral and cold environments. J Appl Physiol 37(4):562–565
Wagner JA, Horvath SM (1985) Influences of age and gender on human thermoregulatory responses to cold exposures. J Appl Physiol 58(1):180–186
White MD, Ross WD, Mekjavic IB (1992) Relationship between physique and rectal temperature cooling rate. Undersea Biomed Res 19(2):121–130
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tsuzuki, K., Tochihara, Y. & Ohnaka, T. Comparison of thermal responses between young children (1- to 3-year-old) and mothers during cold exposure. Eur J Appl Physiol 103, 697–705 (2008). https://doi.org/10.1007/s00421-008-0730-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-008-0730-x