
Abstract
The purpose of this study was to examine a course of force potentiation and/or inhibition during maximal voluntary eccentric action. Maximal voluntary force (MVC) of elbow flexion of ten healthy male volunteers was measured during isometric and isokinetic eccentric action starting from 80° or 110° and ending at 140° elbow angle. Surface EMG was recorded from biceps brachii (BB) and brachioradialis (BR) muscles. Maximal voluntary eccentric force during the first 10° of the movement was higher (P<0.001) than the maximal voluntary isometric preactivation force both in 80° and in 110° starting position at all three velocities (1, 2, and 4 rad s−1). The relative force potentiation was velocity dependent being smallest at the lowest stretching speed (P<0.01). Average EMG (aEMG) of BB and BR decreased as the joint angle increased both in eccentric and in isometric actions but the decrease in aEMG towards extension was somewhat higher in eccentric actions as compared to isometric. It was concluded that the force measured during the first 10° of eccentric contraction always exceeded the maximal voluntary isometric preactivation force regardless of the joint angle or of the movement velocity. When maximal voluntary preactivation preceded the stretch, the relative force potentiation seemed to be greater at higher stretching velocities (velocity dependent) while at lower preactivation levels, the velocity dependence was not observed. Decreased muscle activation and lower maximal voluntary force towards the end of the movement suggested inhibition during maximal voluntary eccentric actions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Experiments with single muscle fibers have shown that when the fiber is stretched after isometric preactivation the force immediately after the stretch exceeds the force at the prestretched level (e.g. Edman et al. 1978). Similar phenomenon has been observed also in human forearm flexors and knee extensors (Komi et al. 2000; Linnamo et al. 2002). After the onset of muscle lengthening, the muscle force may increase due to muscular (e.g. Rack and Westbury 1974; Harridge and White 1993) and neural mechanisms (e.g. Stein and Kearney 1995; Nicol and Komi 1999). When maximal voluntary eccentric force is compared with separately measured maximal voluntary isometric force at the corresponding joint angle, the isometric force is usually lower than the eccentric one (e.g. Asmussen et al. 1965; Doss and Karpovich 1965; Komi 1973; Griffin 1987), although in some situations it may also be the opposite (Komi et al. 2000; Singh and Karpovich 1966; Spurway et al. 2000; Seger and Thorstenson 2000; Westing et al. 1988). The later could be due to neural inhibition that has been suggested to occur during maximal voluntary eccentric action (Seger and Thorstenson 2000; Westing et al. 1990) and therefore subjects have difficulties to maintain high eccentric force level throughout the motion. Lower activation level measured by twitch interpolation technique (Babault et al. 2001; Beltman et al. 2004) and lower maximal EMG amplitude (Madelaine et al. 2001; Komi et al. 2000; Westing et al. 1991) in eccentric versus isometric supports the concept of inhibition in maximal voluntary eccentric condition. According to Grabiner and Owings (2002) the average EMG (aEMG) can actually be lower already at the isometric preactivation phase before maximal eccentric compared with concentric action.
An increase in the EMG amplitude reflecting the stretch reflex response may be seen after the onset of eccentric movement (e.g. Gottlieb and Agarwal 1979; Lee and Tatton 1978). The reflex can be influenced by the joint angle during the stretch (Fellows and Thilmann 1989; Stein and Kearney 1995), amplitude (Allum and Mauritz 1984; Stein and Kearney 1995), velocity (Allum and Mauritz 1984), direction (Stein and Kearney 1995), duration of the stretch (Stein and Kearney 1995), and by the background activity (Ogiso et al. 2002). When the movement is started with maximal isometric preactivation the EMG may decrease towards the end of the eccentric motion and this decrease appears to be greater with slow movement velocities than with faster ones (Komi et al. 2000). On the other hand, when the eccentric movement was started without isometric preactivation, although the EMG values were lower in eccentric than in concentric, the movement velocity in eccentric condition had no apparent effect on the maximal EMG values (Aagaard et al. 2000; Andersen et al. 2005). With preactivation the maximal eccentric force can, however, be higher and be reached earlier than if the movement is started without preactivation (Linnamo et al. 2003).
Although the separately measured maximal voluntary isometric force may sometimes exceed maximal voluntary eccentric one at the corresponding joint angle it seems that eccentric force after the onset of the movement is always higher than the maximal voluntary isometric preactivation force. Furthermore, if the inhibition in maximal eccentric action is related to movement velocity and working time, with shorter range of motion the reduction in EMG and force should be smaller. Thus, the purpose of the present study was to (1) to examine the role of preactivation force level and movement velocity to the force potentiation and/or inhibition during maximal voluntary eccentric action and (2) examine the effects of the movement range on the maximal voluntary eccentric force production in comparison to the maximal voluntary isometric forces at corresponding angles.
Methods
Ten male subjects aged 20–32 years volunteered to participate in the study. The mean height, body mass, and body fat were 182.4 (SD 4.5) cm, 76.1 (SD 5.2) kg, and 12.6 (SD 2.2)%, respectively. The subjects were physically fit students. Full advice about possible risks and discomfort was given to the subjects and they all gave their written informed consent to participate. The study was conducted according to the declaration of Helsinki and was approved by the ethics committee of the University of Jyväskylä.
The subjects sat in a chair with their right forearm supinated and fixed to a custom-built isokinetic machine driven by a strong electromotor (Komi et al. 2000). Trunk and upper arm were fixed to the chair with a special upper arm support with belts to prevent any movements of the upper body. The elbow axis was aligned with the axis of rotation of the lever arm of the machine. The lever arm was equipped with the strain gauge transducer to measure the force applied on the wrist during elbow flexion/extension. Maximal voluntary isometric force during maximal voluntary elbow flexion was measured in random order at 80°, 95°, 110°, 125°, and 140° of elbow angle. Subjects had to achieve isometric MVC in 1.5 s and maintain it for further 2 s. The highest force was used for analysis. During eccentric action, the range of motion of the elbow joint ranged from 80° to 140° or from 110° to 140° (full extension=180°). The subjects were instructed to maximally resist the elbow extension controlled by the machine at constant velocities of 1, 2, and 4 rad s−1. All eccentric actions were performed with maximal voluntary effort throughout the movement range starting from preactivation levels of 50%, and 100% of separately measured isometric MVC at the corresponding starting joint angle. The eccentric movement started a few hundred milliseconds after stable isometric force in 100% condition and almost immediately after 50% preactivation level was reached, as shown in Fig. 1 at 2 rad s−1 condition. Maximal voluntary force was calculated both in the absolute and in the relative scale. For relative scale the isometric preactivation force just prior to the stretch was chosen to present a level to which the relative increase in force was then compared. In addition, the movement of the lever arm was performed at all the movement velocities with the subject sitting passively without resisting the movement. This was done in order to estimate the effect of the moment of inertia on the measured force. The force measured in the relaxed condition was then subtracted from the forces measured during active resistance. Trials were performed in a random order with a resting period of 2 min between the trials.

Absolute eccentric force curves at 2 rad s−1 from 80° to 140° elbow angle starting from 50 and 100% preactivation (mean of ten subjects)
The range of motion during eccentric action was divided into six 10° sections (80°–140°) and into three 10° sections (110°–140°) for further analyses of force and aEMG. Maximal force and aEMG were obtained from each 10° section in eccentric actions while in isometric action the measurements were taken at the specific elbow angles of 80°, 95°, 110°, 125°, and 140°. EMG signal was recorded from the biceps brachii (BB) and brachioradialis (BR). Bipolar surface EMG recording (Beckman miniature-sized skin electrodes, USA) with inter-electrode distance of 20 mm was employed. The electrodes were placed longitudinally on the muscle approximately halfway from the motor point area to the distal part of the muscle. EMG signals were recorded telemetrically (Glonner Biomes 2000, Germany) with a sampling frequency of 2,096 Hz. All EMG signals were filtered with a high-pass filter (cut-off frequency 20 Hz) to remove a base line shift. For aEMG the signal was fully rectified and average amplitude for each section was calculated.
Means and standard deviations (SD) were calculated. The data was then analyzed with analysis of variance (ANOVA). When ANOVA showed statistically significant differences among conditions, comparisons of means for pairs of conditions were performed by Student’s paired t test. The level of significance was chosen to be P<0.05 (two-tailed).
Results
Eccentric versus isometric preactivation
Maximal voluntary eccentric force during the first 10° of the movement was significantly higher (P<0.001) than the maximal isometric preactivation force both in 80° and in 110° starting position at all three velocities. The relative force potentiation after 100% preactivation level was significantly lower throughout the motion (P<0.01) during 1 rad s−1 as compared with 2 and 4 rad s−1 starting either from the 110° (P<0.01) or, as shown in Figs. 2 and 3, from 80° (P<0.05) elbow angle. Regardless of the movement velocity no significant differences were observed in aEMG of BB or BR between the isometric preactivation phase and the first 10° of movement. In the absolute scale, regardless of the starting angle and movement velocity, maximal force throughout the motion was lower (P<0.001) starting the eccentric action from 50% preactivation level as compared to 100% preactivation level. At 1 rad s−1 from 80° elbow angle the difference was no longer that clear but even then still significant (P<0.05). Figure 1 shows an example of force curves starting from different preactivation levels from 80° elbow angle at 2 rad s−1. Tables 1 and 2 summarize the relative force increases throughout the whole range of motion from both starting positions and from both starting levels.

Relative eccentric force curves at 1, 2, and 4 rad s−1 from 80° to 140° elbow angle starting from maximal preactivation (mean of ten subjects)

Relative average force potentiation at 1, 2, and 4 rad s−1 from 80° to 140° elbow angle starting from maximal preactivation (mean of ten subjects)
Eccentric versus separately measured isometric
Separately measured isometric force was higher (P<0.05) than the corresponding eccentric force at 80° and 95° (all velocities) and at 110° (1 rad s−1) joint angle when the movement started from 80° (Fig. 4). However, only half of the subjects were able to start the eccentric movement from a similar force level (within ±5%) as their separately measured maximal isometric force. For those subjects the eccentric force exceeded the isometric force at all the joint angles. Average EMG of BB was higher at smaller joint angles (P<0.05) and at larger joint angles (P<0.001) in separately measured isometric than in eccentric actions with maximal preactivation, while similar differences in BR occurred only at larger joint angles (P<0.05).

Maximal isometric and eccentric force from 80° to 140° elbow angle (mean of ten subjects)
Effect of joint angle and range of motion
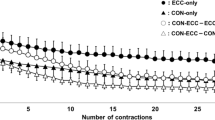
Maximal eccentric force during the last 10° of motion (100% preactivation) at 1 rad s−1 was lower (P<0.05) when the movement was started from 80° as compared to the 110° starting position, while at the other two velocities no significant differences were observed. aEMG decreased as the joint angles increased in BB (NS) and in BR (P<0.05) both in isometric and in eccentric actions but the changes were similar between the three movement velocities (Fig. 5a, b). No significant differences were observed in aEMG between different joint angles during the whole range of motion with the 50% preactivation level.

aEMG of BB (a) and BR (b) muscles from 80° to 140° elbow angle (mean of ten subjects)
Discussion
The results of the present study clearly indicate that when maximal voluntary eccentric force is compared to maximal voluntary isometric force it is of crucial importance whether the eccentric force is compared with the isometric preactivation force or with the separately measured isometric force. In the present study when the eccentric force was measured immediately after the stretch the eccentric force will always exceed the preactivated isometric force. On the other hand, the present results also showed that in certain conditions the separately measured isometric force may be higher than eccentric force at the corresponding joint angle.
Eccentric versus isometric preactivation
If the eccentric force is measured immediately after the stretch, as shown with isolated muscle fibers or sarcomeres (Edman et al. 1978), the eccentric force will exceed the preactivated isometric force. This phenomenon was well supported by the results of the present study since, regardless of the starting angle, movement velocity or preactivation level, the isometric preactivation force was always exceeded by the following eccentric force. The increase in muscle force after the stretch can be due to both muscular (e.g. Rack and Westbury 1974; Harridge and White 1993) and neural mechanisms (e.g. Stein and Kearney 1995; Nicol and Komi 1999). In the present study aEMG during the first 10° of motion did not increase above the preisometric level. Thus, the effect of the stretch reflex response could not be clearly demonstrated in the elbow flexors as has been previously shown with angle plantar flexor muscles (e.g. Nicol and Komi 1999). Despite the lack of the clear reflex response the increase in force was related to the stretching velocity. When the movement started with maximal preactivation and the increase in force was calculated on the relative scale the results clearly indicated that the greatest force potentiation was caused by the highest stretching velocities. These results are in line with those of Komi (1973) who used full isometric preactivation before the eccentric mode similar to that used in the isolated preparation (Edman et al. 1978). As seen in Tables 1a and 2a, the clearest differences in the relative force potentiation between the three movement velocities were observed in the latter part of the movement. This indicates that not only is the force potentiation higher at higher stretching velocities but it is also maintained better throughout the movement which would support the concept of possible inhibition at lower velocities.
The eccentric action with the lowest velocity including the isometric preactivation phase lasted less than 2,500 ms. Thus, it seems unlikely that the fatigue would play a role in the force decrease but the inhibition seems to be a more likely explanation. The relative scale was chosen because some, although not significant, variations were observed in the absolute maximal isometric preactivation force between the movement velocities. At 50% preactivation level the velocity dependence was no longer observed. In fact at 50% starting level the highest relative force increases, taken from the first 10° of the motion, were observed after the slowest velocity. This could simply be due to longer time available to activate additional motor units in the course of the lever arm displacement. The absolute maximal force and the average force throughout the whole range of motion, however, were lower when the movement started from 50% as compared to 100% preactivation level. These lower forces with low preactivation level appear to be particularly clear with high movement velocities and small range of motion when the subjects simply may not even have enough time to reach the maximal force.
Eccentric versus separately measured isometric force
In the situation where the isometric force is measured separately from eccentric force the isometric force can sometimes exceed the maximal eccentric force of the corresponding joint angle (Komi et al. 2000; Singh and Karpovich 1966; Spurway et al. 2000; Westing et al. 1988). Due to possible neural inhibition it may be difficult to maintain the full activation of the muscles during maximal eccentric action (Babault et al. 2001; Seger and Thorstenson 2000; Westing et al. 1990). This may be relevant especially with slow movement velocity and when the maximal eccentric force is maintained throughout rather large range of motion (110°) (Komi et al. 2000). Similar phenomenon, but with smaller range of motion (60°), was observed also in the present study. During the slowest velocity (1 rad s−1) in the present study the maximal eccentric force in the middle part of the motion was somewhat, although not significantly, lower (P=0.093) as compared to the two faster velocities, whereas with even smaller range of motion (30°) the absolute forces were almost similar. In addition, only at the lowest velocity was the maximal force in the final part of motion significantly lower when the movement started from 80° in comparison to the movement starting from 110°.
As the results of the separately measured isometric forces in the present study suggest, it is relevant how much time is used to build up the maximal force and which part of the isometric force curve is chosen for the analysis. The peak force may occur around 2–3 s which is much longer than the time usually given for maximal preactivation before the stretch. This could be due to increased activation of some other muscles trying to assist in increasing the force. In the present study the aEMG of BB muscle indicated that it was fully activated already during the 500 ms whereas the activity of BR increased significantly towards the end of the isometric maximum (2–3 s). Although the subjects were secured firmly with seatbelts in order to fix the body position, it is possible that some other upper body muscles have contributed to the force as well. If the separately measured maximal isometric force was similar to the maximal preactivation force, which was the case for half of the subjects, it was always exceeded by the maximal eccentric force.
In dynamic condition the movement range was divided into 10° sections. This allowed the comparison at the same joint angles between the larger (60°) and shorter (30°) range of motion. The separately measured isometric joint angles were chosen to match the joint angles 80° and 110° used in the isometric preactivation phases prior to the movements. In addition, the isometric force was measured within 15° intervals to represent the force–length relationship of the whole range of motion. As in the eccentric condition the analysis was done within 10° intervals, the comparisons between dynamic and isometric actions were not made using exactly the same joint angles. Therefore, some inaccuracy may have taken place in the comparison between the conditions.
Muscle activation
Additional candidate why the difference between maximal eccentric and maximal isometric force may not be so clear is the previously mentioned inhibition and difficulties in maintaining the maximal activation throughout the motion in maximal eccentric action. In a previous study from our lab with the same protocol but larger range of motion (110°), aEMG in maximal eccentric actions decreased towards extended elbow angles and the decrease was more substantial at lowest velocities (Komi et al. 2000). The EMG results of the present study with smaller range of motion were not that clear failing to show any differences between the movement velocities. However, the difference in aEMG between isometric and eccentric actions was somewhat greater towards the extended position of the elbow joint, thus supporting the difficulties in maintaining the full activation of the muscles throughout maximal eccentric actions. Similarly as with zero preactivation (Aagaard et al. 2000) in the present study with 50% preactivation level no clear changes in aEMG during the movement or between the velocities were observed. Thus, besides longer working time the preactivation may also play a role in possible inhibition. The possible mechanism causing the reduction in muscle activation during maximal eccentric action has been suggested to be originating from free nerve endings in the muscle, joint receptors, pain receptors, and Golgi tendon organs (e.g. Houk and Rymer 1981; Romano and Schieppati 1987).
Surface EMG may also be influenced by cancellation of the negative and positive phases of motor unit action potentials as they sum to form the interference EMG (Day and Hulliger 2001). Changes in action potential shape, e.g. due to motor unit synchronization can affect the amount of cancellation in different conditions (Yao et al. 2000). The synchronization may be greater for eccentric actions compared with concentric and isometric actions (Semmler et al. 2002). Therefore, the amount of cancellation and thus the quantity of EMG activity may be influenced more during eccentric compared with concentric or isometric actions. On the other hand, there is also evidence that the average amplitude of the surface EMG may increase due to synchronization (Yao et al. 2000).
In conclusion, if the force is measured immediately after the stretch it will always exceed the maximal isometric preactivation force regardless of the joint angle or of the movement velocity. The relative force potentiation seems to be velocity dependent being greater at higher stretching velocities but only when maximal preactivation preceded the stretch. At lower preactivation levels the velocity dependence was not observed. Decreased muscle activation and lower maximal force towards the end of the movement suggest that inhibition may take place during maximal eccentric actions.
References
Aagaard P, Simonsen E, Andersen J, Magnusson S, Halkjaer-Kristensen J, Dyhre-Poulsen P (2000) Neural inhibition during maximal eccentric and concentric quadriceps contraction: effects of resistance training. J Appl Physiol 89:2249–2257
Allum J, Mauritz K (1984) Compensation for intrinsic muscle stiffness by short-latency reflexes in human triceps surae muscles. J Neurophysiol 52:797–818
Andersen L, Andersen J, Magnusson S, Aagaard P (2005) Neuromuscular adaptations to detraining following resistance training in previously untrained subjects. Eur J Appl Physiol 93:511–518
Asmussen E, Hansen O, Lammert O (1965) The relation between isometric and dynamic muscle strength in man. Communications from the testing and observation institute of the Danish National Association for Infantile Paralysis, Hellerup, Denmark, No. 20, pp 3–11
Babault N, Pousson M, Ballay Y, Van Hoecke J (2001) Activation of human quadriceps femoris during isometric, concentric, and eccentric contractions. J Appl Physiol 91:2628–2634
Beltman J, Sargeant A, van Mechelen W, de Haan A (2004) Voluntary activation level and muscle fiber recruitment of human quadriceps during lengthening contractions. J Appl Physiol 97:619–626
Day S, Hulliger M (2001) Experimental simulation of cat electromyogram: evidence for algebraic summation of motor unit action-potential trains. J Neurophysiol 86:2144–2158
Doss W, Karpovich P (1965) A comparison of concentric, eccentric and isometric strength of elbow flexors. J Appl Physiol 20(2):351–353
Edman K, Elzinga G, Noble M (1978) Enhancement of mechanical performance by stretch during tetanic contractions of vertebrate skeletal muscle fibres. J Physiol 281:139–155
Fellows S, Thilmann A (1989) The role of joint biomechanics in determining stretch reflex latency at the normal human ankle. Exp Brain Res 77:135–139
Gottlieb GL, Agarwal GC (1979) Response to sudden torques about ankle in man: myotatic reflex. J Neurophysiol 42:91–106
Grabiner M, Owings T (2002) EMG differences between concentric and eccentric maximum voluntary contractions are evident prior to movement onset. Exp Brain Res 145(4):505–511
Griffin JW (1987) Differences in elbow flexion torque measured concentrically, eccentrically, and isometrically. Phys Ther 67(8):1205–1208
Harridge S, White M (1993) Muscle activation and the isokinetic torque–velocity relationship of the human triceps surae. Eur J Appl Physiol 67(3):218–221
Houk J, Rymer W (1981) Neural control of muscle length and tension. In: Brooks VB (ed) Handbook of physiology, section I, part 2. American Physiological Society, Bethesda, pp 257–323
Komi PV (1973) Relationship between muscle tension, EMG and velocity of contraction under concentric and eccentric work. In: Desmedt JE (ed) New developments in electromyography and clinical neurophysiology, vol 1. Karger, Basel, pp 596–606
Komi PV, Linnamo V, Silventoinen P, Sillanpää M (2000) Force and EMG power spectrum during eccentric and concentric actions. Med Sci Sports Exerc 32(10):1757–1762
Lee R, Tatton W (1978) Long loop reflexes in man: clinical applications. In: Desmedt JE (ed) Cerebral motor control in man: long loop mechanisms. Karger, Basel, pp 320–333
Linnamo V, Strojnik V, Komi PV (2002) EMG power spectrum and features of the superimposed maximal M-wave during voluntary eccentric and concentric actions at different activation levels. Eur J Appl Physiol 86:534–540
Linnamo V, Moritani T, Nicol C, Komi PV (2003) Motor unit activation patterns during isometric, concentric and eccentric actions at different force levels. J Electromyogr Kinesiol 13(1):93–101
Madeleine P, Bajaj P, Sogaard K, Arendt-Nielsen L (2001) Mechanomyography and electromyography force relationships during concentric, isometric and eccentric contractions. J Electromyogr Kinesiol 11(2):113–121
Nicol C, Komi PV (1999) Quantification of Achilles tendon force enhancement by passively induced dorsiflexion stretches. J Appl Biomech 15:221–232
Ogiso K, McBride JM, Finni T, Komi PV (2002) Stretch-reflex mechanical response to varying types of previous muscle activities. J Electromyogr Kinesiol 12(1):27–36
Rack P, Westbury D (1974) The short range stiffness of active mammalian muscle and its effect on mechanical properties. J Physiol 240:331–350
Romano C, Schieppati M (1987) Reflex excitability of human soleus motoneurons during voluntary shortening or lengthening contractions. J Physiol 390:271–284
Seger J, Thorstensson A (2000) Electrically evoked eccentric and concentric torque–velocity relationships in human knee extensor muscles. Acta Physiol Scand 169:63–69
Semmler J, Kornatz K, Dinenno D, Zhou S, Enoka R (2002) Motor unit synchronisation is enhanced during slow lengthening contractions of a hand muscle. J Physiol 545:681–695
Singh M, Karpovich P (1966) Isotonic and isometric forces of forearm flexors and extensors. J Appl Physiol 21(4):1435–1437
Spurway N, Watson H, McMillan K, Connolly G (2000) The effect of strength training on the apparent inhibition of eccentric force production in voluntarily activated human quadriceps. Eur J Appl Physiol 82:374–380
Stein R, Kearney R (1995) Nonlinear behavior of muscle reflexes at the human ankle joint. J Neurophysiol 73:65–72
Westing S, Seger J, Karlson E, Ekblom B (1988) Eccentric and concentric torque–velocity characteristics of the quadriceps femoris in man. Eur J Appl Physiol 58:100–104
Westing S, Seger J, Thorstensson A (1990) Effects of electrical stimulation on eccentric and concentric torque–velocity relationships during knee extension in man. Acta Physiol Scand 140:17–22
Westing SH, Cresswell AG, Thorstensson A (1991) Muscle activation during maximal voluntary eccentric and concentric knee extension. Eur J Appl Physiol 62(2):104–108
Yao W, Fuglevand A, Enoka R (2000) Motor-unit synchronization increases EMG amplitude and decrease force steadiness of simulated contractions. J Neurophysiol 83:441–452
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Linnamo, V., Strojnik, V. & Komi, P. Maximal force during eccentric and isometric actions at different elbow angles. Eur J Appl Physiol 96, 672–678 (2006). https://doi.org/10.1007/s00421-005-0129-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-0129-x