
Abstract
Resistance exercise has recently been shown to improve whole-body insulin sensitivity in healthy males. Whether this is accompanied by an exercise-induced decline in skeletal muscle glycogen and/or lipid content remains to be established. In the present study, we determined fibre-type-specific changes in skeletal muscle substrate content following a single resistance exercise session. After an overnight fast, eight untrained healthy lean males participated in a ~45 min resistance exercise session. Muscle biopsies were collected before, following cessation of exercise, and after 30 and 120 min of post-exercise recovery. Subjects remained fasted throughout the test. Conventional light and (immuno)fluorescence microscopy were applied to assess fibre-type-specific changes in intramyocellular triacylglycerol (IMTG) and glycogen content. A significant 27±7% net decline in IMTG content was observed in the type I muscle fibres (P<0.05), with no net changes in the type IIa and IIx fibres. Muscle glycogen content decreased with 23±6, 40±7 and 44±7% in the type I, IIa and IIx muscle fibres, respectively (P<0.05). Fibre-type-specific changes in intramyocellular lipid and/or glycogen content correlated well with muscle fibre-type oxidative capacity. During post-exercise recovery, type I muscle fibre lipid content returned to pre-exercise levels within 120 min. No changes in muscle glycogen content were observed during recovery. We conclude that intramyocellular lipid and glycogen stores are readily used during resistance exercise and this is likely associated with the reported increase in whole-body insulin sensitivity following resistance exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fat and carbohydrate are the principal substrates that fuel ATP resynthesis in skeletal muscle tissue. Endogenous carbohydrates are mainly stored as muscle and liver glycogen, and represent less than 5% of total energy storage. The vast majority of our energy reserves is stored as fat, mainly deposited as triacylglycerol (TG) in subcutaneous and deep visceral adipose tissue. Smaller quantities of TG are present as lipid droplets inside the muscle fibres, intramyocellular triacylglycerol (IMTG; Hoppeler et al. 1985).
There has been much controversy on the actual contribution of the IMTG pool as a substrate source during exercise (Watt et al. 2002). The apparent discrepancy in the literature likely stems from the methodological difficulties that have been associated with the biochemical triacylglycerol extraction method that has been used to determine IMTG content in muscle biopsies collected before and after exercise (Watt et al. 2002). In accordance, more recent studies using stable isotope methodology, 1H-magnetic resonance spectroscopy, electron and/or immunofluorescence microscopy all support the contention that the IMTG pool can function as an important substrate source during submaximal exercise (van Loon et al. 2003a). Besides the intramyocellular lipid deposits, muscle glycogen stores represent another important substrate source. In accordance, substantial net reductions in both type I and II muscle fibre glycogen content have been reported following prolonged endurance exercise tasks (Tsintzas et al. 2000). These intramyocellular lipid and glycogen stores play a major regulatory role in skeletal muscle metabolism. Muscle glycogen use and subsequent post-exercise glycogen synthesis rates have been shown to be functionally coupled to the exercise-induced increase in skeletal muscle insulin sensitivity in humans and rodents (Bogardus et al. 1983; Derave et al. 2000; Garcia-Roves et al. 2003; Perseghin et al. 1996; Wojtaszewski et al. 2000, 1997). Furthermore, interventions known to improve insulin sensitivity, like weight loss in humans (Goodpaster et al. 1999; Houmard et al. 2002), dietary lipid withdrawal (Oakes et al. 1997a), the use of thiazolidinediones in rodents (Oakes et al. 1997b) as well as an acute bout of endurance exercise in rodents and humans (Oakes et al. 1997a; van Loon et al. 2003a) have all been associated with a reduction in skeletal muscle lipid content. Because of its capacity to reduce both intramyocellular lipid and glycogen content, endurance exercise is generally considered an effective interventional strategy to improve skeletal muscle insulin sensitivity.
However, resistance exercise should also be regarded as an essential component of effective intervention programs designed to improve health. Resistance training increases skeletal muscle mass (Kadi and Thornell 2000) and, as such, can augment whole-body glucose disposal capacity (Craig et al. 1989; Fenicchia et al. 2004; Miller et al. 1984). In addition, resistance training also improves muscle strength, power and functional capacity, which facilitates the adaptation towards a more active lifestyle (Evans 1995; Macaluso and De Vito 2004). Although there is some discrepancy in the existing literature, we (Koopman et al. 2005) as well as others (Fenicchia et al. 2004; Fluckey et al. 1994) have recently shown that even a single resistance exercise session can improve whole-body insulin sensitivity for up to 24 h after cessation of exercise. In line with the acute stimulating effects of endurance exercise on post-exercise insulin sensitivity (Bogardus et al. 1983), it has been speculated that the acute effects of resistance exercise on whole-body insulin sensitivity are also attributed to the reduction of the intramyocellular glycogen and/or lipid stores (Koopman et al. 2005). However, studies on the metabolic demands of resistance exercise are scarce, which is likely due to the methodological difficulties associated with the non-steady state conditions of this type of exercise. Therefore, in the present study, we determined fibre-type-specific changes in intramyocellular glycogen and lipid content during and immediately after a single resistance exercise session.
Methods
Subjects
Eight healthy untrained male volunteers with no history of participating in any regular exercise program were recruited for the present study. Subjects’ characteristics are shown in Table 1. All subjects were informed on the nature and possible risks of the experimental procedures before their written informed consent was obtained, the latter after approval by the Medical Ethical Committee of the Academic Hospital Maastricht.
Pre-testing
Body composition was assessed using the hydrostatic weighing method in the morning following an overnight fast. Residual lung volume was measured by the helium-dilution technique using a spirometer (Volugraph 2000, Mijnhart, Bunnik, The Netherlands). Body mass was measured with a digital balance with an accuracy of 0.001 kg (E1200, August Sauter GmbH, Albstadt, Germany). Body fat percentage was calculated using Siri’s equation (Siri 1956). Fat free mass (FFM) was calculated by subtracting fat mass from total body mass.
To familiarize subjects with the resistance exercise protocol and the equipment, a familiarization trial was performed. Proper lifting technique was demonstrated and practiced for each of the two lower-limb exercises (leg press and leg extension) and for the three upper-body exercises (chest press, shoulder press and lat-pulldown). Thereafter, maximum strength was estimated using the multiple repetitions testing procedure (Mayhew et al. 1995).
In an additional exercise session, at least 1 week before the first experimental trial, the subjects’ 1 repetition maximum (1RM) was determined (Kraemer and Fry 1995). After warming up, the load was set at 90–95% of the estimated 1RM, and increased after each successful lift until failure. A 5 min resting period between subsequent attempts was allowed. A repetition was valid if the subject was able to complete the entire lift in a controlled manner without assistance.
Standardised diet and activity prior to testing
All subjects received a strict standardised diet for 2 days prior to the resistance exercise test trial, which was performed in the morning after an overnight fast. Subjects were provided with a measured amount of food products, beverages and instant meals, and were allowed to drink water ad libitum. Subjects were instructed to take all main meals (breakfast, lunch and dinner) and between-meal snacks at pre-determined time intervals during each day. The standardised diet provided 0.15 MJ kg−1 day−1 containing 15 Energy% (En%) of protein, 30 En% of fat and 55 En% of carbohydrate. All volunteers were instructed to refrain from any sort of heavy physical exercise during the 2 days prior to the test trial.
Experimental trial
The day of the test, subjects arrived at the laboratory by car or public transportation at 8.00 a.m., following an overnight fast. A Teflon catheter was inserted into an antecubital vein for blood sampling. After 30 min of supine rest, a basal blood sample was collected and a muscle biopsy was taken from the m. vastus lateralis. Thereafter, subjects performed a 5 min low-intensity warm-up on a Stairmaster, followed by three sets of ten repetitions on three resistance exercise machine targeting upper-body muscle groups (chest press, shoulder press and lat-pulldown; Jimsa Benelux BV, Rotterdam, The Netherlands). The latter were included to provide a whole-body warm-up to reduce the risk of injury. Thereafter, subjects performed eight sets of ten repetitions on the horizontal leg press machine (Technogym BV, Rotterdam, The Netherlands) and eight sets of ten repetitions on the leg extension machine (Technogym). Both exercises were performed at 75% of the individual 1RM with 2 min rest intervals between sets and required ~45 min to complete it. All subjects were verbally encouraged during the exercise session to complete the entire protocol. Immediately after cessation of exercise, a second muscle biopsy sample was taken, after which subjects rested supine for 2 h. After 30 min and 2 h of post-exercise recovery, additional muscle biopsies were taken. Blood samples were collected before, after 30 min of exercise, immediately after cessation of exercise and following 30, 60, 90 and 120 min of post-exercise recovery. Subjects remained fasted throughout the test.
Muscle biopsy samples were collected from both legs. The first two biopsies were taken from the same incision in one leg; the last two were taken from the same incision in the contralateral leg. When biopsy samples were taken from the same incision, the first sample was taken from a different region (distal of the incision, with the needle pointing inwards) than the second (proximal with the needle pointing outwards). Muscle biopsies were obtained from the middle region of the m. vastus lateralis (15 cm above the patella) and approximately 3 cm below entry through the fascia using the percutaneous needle biopsy technique (Bergstrom 1975). Muscle samples were dissected carefully, freed from any visible non-muscle material, embedded in Tissue-Tek (Sakura Finetek, Zoeterwoude, The Netherlands) and rapidly frozen in liquid nitrogen-cooled isopentane.
Plasma sample analysis
Blood samples (6 ml) were collected in EDTA-containing tubes and centrifuged at 1,000 g at +4°C for 10 min. Aliquots of plasma were frozen immediately in liquid nitrogen and stored at −80°C. Plasma glucose (Uni Kit III, Roche, Basel, Switzerland), lactate (Gutmann and Wahlefeld 1974) and FFA (Wako NEFA-C test kit, Wako Chemicals, Neuss, Germany) concentrations were analysed with a COBAS FARA semi-automatic analyser (Roche).
Muscle sample analysis
Multiple serial sections (5 μm) from biopsy samples collected before, immediately after, and 30 and 120 min after exercise were thaw-mounted together on uncoated, pre-cleaned glass slides for each subject. To permit the determination of muscle fibre IMTG content stained by oil red O together with immunolabelled cellular constituents we used the protocol as previously described (Koopman et al. 2001; van Loon et al. 2004, 2003a, b). The proportion of type I, IIa and IIx muscle fibres was determined by ATPase staining (Mabuchi and Sreter 1980). To assess intramyocellular glycogen content we used the modified PAS stain as recently described (Schaart et al. 2004), allowing direct, fibre-type-specific determination of muscle glycogen content. Muscle fibre-type-specific oxidative capacity was estimated by determining succinate dehydrogenase activity (SDH) in the muscle cross-sections using histochemical analyses (Gosker et al. 2002). Histological techniques, like oil red O, PAS and SDH staining combined with either immunofluorescence or conventional light microscopy are semi-quantitative. As a consequence, the present study does not provide absolute measures of skeletal muscle lipid and/or glycogen concentrations. After 24 h, glass slides were examined using a Nikon E800 fluorescence microscope (Uvikon, Bunnik, The Netherlands) coupled to a Basler A113 C progressive scan colour CCD camera, with a Bayer colour filter. Epifluorescence signal was recorded using a Texas red excitation filter (540–580 nm) for oil red O, a fluorescein isothiocyanate (FITC) excitation filter (465–495 nm) for muscle fibre type, and a 4′,6-diamidino-2-phenylindole (DAPI) UV excitation filter (340–380 nm) for laminin.
Digitally captured images (240× magnification) with a minimum of six fields-of-view per muscle cross-section (12±1 fibres per field-of-view), were processed and analysed using Lucia 4.8 software (Nikon, Düsseldorf, Germany). The signal derived from the antibody against laminin was used to select single muscle fibres and with the antibody against human myosin heavy chain I, we were able to differentiate between type I and II muscle fibres. To differentiate between type IIa and IIx fibres we used matching serial cross-section stained using routine ATPase staining. The oil red O epifluorescence signal was recorded for each muscle fibre, resulting in a total of 70±5 muscle fibres analysed for each muscle cross-section (35±2 type I, 25±4 type IIa and 10±1 type IIx muscle fibres). An intensity threshold representing minimal intensity values corresponding to lipid droplets was set manually and uniformly used for all images. Total area measured and the area as well as the number of objects emitting oil red O epifluorescence signal were recorded. Fibre-type-specific IMTG content was expressed as the percentage of the measured area that was stained with oil red O. In a previous study, two different muscle samples from two different subjects were analysed; showing a coefficient of variance of 10.5 and 38.6% for the type I and II muscle fibres (van Loon et al. 2003a). Mixed muscle fibre lipid content, as determined by oil red O staining, has been shown to correlate significantly with measures of intramyocellular lipid content as assessed by 1H-magnetic resonance spectroscopy (van Loon et al. 2003b). Average lipid droplet size was calculated by dividing the total area lipid stained by total number of lipid droplets. Lipid droplet density was calculated by dividing the total number of lipid droplets by the total area measured.
PAS and SDH stained sections were captured in full colour using bright field light microscopy. Digitally captured images (120× magnification) with a minimum of four fields-of-view per muscle cross-section (37±2 fibres per field-of-view) were processed and analysed using the Lucia 4.8 software package. The PAS and SDH signals were recorded for each muscle fibre, resulting in a total of 142±8 muscle fibres analysed for each muscle cross-section (64±4 type I, 57±5 type IIa and 21±2 type IIx muscle fibres). The bright-field images of the PAS and SDH stains were converted post hoc to 8 bit greyscale values. The mean optical density of the PAS or SDH-raised signal per individual fibre was determined by averaging the optical density measured in every pixel in the cell, corrected for the mean optical density of the background stain measured in a field-of-view containing no muscle fibres. Mixed muscle glycogen content, as determined by PAS staining, correlates significantly with muscle glycogen content as measured using biochemical analyses (Schaart et al. 2004).
Statistics
All data are expressed as means ± SEM. Analyses of variance (ANOVA) for repeated measures were applied to determine differences in muscle lipid and glycogen content over time in type I, IIa and IIx fibres with time and muscle fibre type as factors. In case of a significant F-ratio, a Scheffe post hoc test was applied to locate the differences. Statistical significance was set at P<0.05. Simple regression analysis was performed on mean muscle fibre-type oxidative capacity and glycogen/lipid content.
Results
Resistance exercise
Mean 1RM measured during the pre-test was 198±7 kg on the horizontal leg press and 105±3 kg on the leg extension. Therefore, average weight lifted during the resistance exercise was set at 148±5 and 79±3 kg for the leg press and leg extension, respectively. All subjects completed eight sets with ten repetitions on the leg press. One subject was unable to finish ten repetitions during the sixth set, after which resistance was reduced to 65% of the individual 1RM. All subjects completed eight sets of ten repetitions on the leg extension machine.
Plasma analyses
Plasma glucose, lactate and FFA concentrations are presented in Fig. 1a–c, respectively. Plasma glucose concentrations increased during exercise and peaked immediately post-exercise (P<0.05), after which they returned to baseline values. Plasma lactate concentrations markedly increased during exercise (P<0.0001), and decreased during recovery. Plasma FFA concentrations tended to decrease during exercise (P=0.08), and markedly increased during recovery (P<0.001).

Plasma glucose (a), lactate (b) and free fatty acid (c) concentrations at rest, during resistance exercise and subsequent recovery. Data provided are means ± SEM. *, denotes significantly different from pre-exercise values (P<0.05)
Muscle glycogen content
Representative images of muscle cross-sections obtained before (Fig. 2a) and immediately after (Fig. 2b) exercise following PAS staining for analyses of intramyocellular glycogen content are shown. Muscle fibre glycogen content was similar at rest in all fibre types. Mixed muscle glycogen content declined by 33±7% following the exercise session (P<0.0001). Glycogen content had declined by 23±6% in the type I fibres (P<0.01), 40±7% in the type IIa fibres (P<0.001), and 44±7% in the type IIx fibres (P<0.001) compared to pre-exercise values (Fig. 3). The observed decrease over time in glycogen content was significantly greater in the type IIx fibres compared to the type I muscle fibres (P<0.05). During post-exercise recovery muscle glycogen content remained below pre-exercise levels, with no significant changes over time in the type I, IIa and IIx muscle fibres.

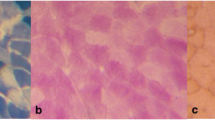
Images (120× magnification) of representative cross-sections of vastus lateralis muscle obtained before (a) and immediately after exercise (b) with sections stained for glycogen content (a/b), and laminin and myosin heavy chains (c/d) (showing the cell membranes in blue and the type I muscle fibres in green). The muscle fibres are labelled as type I, type IIa and type IIx. Differentiation between type IIa and IIx fibres was made based on ATPase staining

The effect of resistance exercise on muscle glycogen content. Fibre-type-specific glycogen content (expressed in arbitrary units) before and immediately after exercise, and following 30 and 120 min of post-exercise recovery as determined by brightfield microscopy on PAS-stained muscle cross-sections. Data provided are means ± SEM. *, denotes significantly lower than pre-exercise values (P<0.05); #, significantly different over time compared to type I muscle fibres (P<0.05)
IMTG content
Representative images of muscle cross-sections obtained before (Fig. 4a) and immediately after (Fig. 4b) exercise stained for intramyocellular lipid content are shown. Muscle tissue analyses for IMTG content applying fluorescence microscopy on oil red O stained muscle cross-sections showed that at rest IMTG content in type I fibres was higher compared with type II fibres (P<0.05). Mixed muscle IMTG content tended to decline with 25±10% following the exercise session (P=0.087). In addition, a substantial 27±7% decline in lipid content in the type I fibres (P<0.05) was found, with IMTG content in the type I muscle fibres being significantly lower both immediately post-exercise as well as following 30 min of post-exercise recovery compared to pre-exercise values (Fig. 5). After 2 h of post-exercise recovery, IMTG content had returned to values similar to pre-exercise values. The observed decrease in IMTG content was accounted for by a significant decrease in lipid droplet size (from 0.69±0.08 to 0.53±0.07 and 0.53±0.07 μm2, P<0.01) without any changes in lipid droplet density (from 0.049±0.003 to 0.045±0.004 and 0.041±0.003 droplets μm−2) as determined before, immediately after, and after 30 min of post-exercise recovery exercise, respectively. Net changes in IMTG content over time in the type 1 fibres were significantly different compared to the type IIa and IIx fibres (P<0.05). No significant changes over time were observed in intramyocellular lipid content in the type IIa or IIx muscle fibres.

Images (240× magnification) of representative cross-sections of vastus lateralis muscle obtained before (a) and immediately after exercise (b) with sections stained for lipid content (a/b), and laminin and myosin heavy chains (c/d; showing the cell membranes in blue and the type I muscle fibres in green). The muscle fibres are labelled as type I, type IIa and type IIx. Differentiation between type IIa and IIx fibres was made, based on standard ATPase staining

The effect of resistance exercise on muscle lipid content. Mean fibre-type-specific intramyocellular lipid content (expressed as percentage of area lipid stained) before exercise, immediately after exercise and following 30 and 120 min of post-exercise recovery as determined by fluorescence microscopy on oil red O stained muscle cross-sections Data provided are means ± SEM. *, significantly lower than pre-exercise values (P<0.05); #, significantly different over time compared to type IIa fibres (P<0.05); ^, significantly different over time compared to type IIx fibres (P<0.05)
Muscle fibre oxidative capacity
A histochemical analysis for SDH activity in muscle cross-sections was performed as a measure of muscle fibre oxidative capacity and results are shown in Table 2. SDH activity was significantly greater in the type I versus the type II fibres (P<0.05). Type IIa muscle fibre SDH activity was substantially greater when compared to the IIx fibres (P<0.05). Positive correlations were observed between muscle fibre-type oxidative capacity and baseline muscle fibre lipid content (r=0.573, P<0.01), and muscle fibre-type oxidative capacity and the net reduction in muscle fibre lipid content observed following exercise (r=0.482, P<0.05). No significant correlation was observed between muscle fibre-type-specific oxidative capacity and resting muscle fibre glycogen content. A significant negative correlation was observed between muscle fibre-type oxidative capacity and the net reduction in muscle fibre glycogen content observed during exercise (r = −0.556, P<0.05).
Discussion
In the present study, we show that resistance exercise can substantially reduce skeletal muscle glycogen and lipid content. A single resistance exercise session reduces both type I and II muscle fibre glycogen content, with most pronounced changes located in the type IIx fibres. Furthermore, resistance exercise also reduces intramyocellular lipid content, which is restricted to the type I muscle fibres. Fibre-type-specific substrate utilisation during resistance exercise seems to be tightly coupled to muscle fibre-type oxidative capacity.
The exercise-induced reduction in skeletal muscle glycogen and/or lipid content has been associated with an increase in insulin sensitivity in humans (Bogardus et al. 1983; Perseghin et al. 1996; Wojtaszewski et al. 2000, 1997). Numerous studies have reported intramuscular substrate availability to play a key regulatory role in skeletal muscle insulin signalling (Hegarty et al. 2003; Wojtaszewski et al. 2003). For example, skeletal muscle glucose uptake and glycogen synthase activity strongly depend on muscle glycogen availability (Nielsen and Richter 2003; Wojtaszewski et al. 2003). The mechanism for this phenomenon is related to increased GLUT4 translocation under reduced muscle glycogen availability, and is likely coupled to an increased activation of AMP-activated protein kinase (AMPK) (Wojtaszewski et al. 2003). Furthermore, a decrease in muscle lipid content following exercise has also been linked to greater insulin sensitivity in rodents (Oakes et al. 1997a). Although a variety of mechanisms have been suggested, recent studies seem to indicate that the relationship between IMTG content and skeletal muscle insulin sensitivity is not functional (van Loon et al. 2004).
Aging, disability and functional incapacity often result in the inability/inefficacy to perform moderate-intensity endurance exercise. Therefore, resistance exercise training is being more frequently advocated as a necessary component of effective exercise intervention programs to augment muscle mass (Kadi and Thornell 2000), strength, power and functional capacity (Evans 1995; Macaluso and De Vito 2004). However, only few studies have investigated the acute effects of resistance exercise on insulin sensitivity (Chapman et al. 2002; Fenicchia et al. 2004; Fluckey et al. 1994). Recently, we showed that a single resistance exercise session improves whole-body insulin sensitivity by ~13% for up to 24 h after exercise (Koopman et al. 2005). The latter seems to be of a similar magnitude as the ~20% increase in whole-body insulin sensitivity has been reported after ~60 min of endurance exercise (Devlin et al. 1987; Devlin and Horton 1985; Mikines et al. 1988; Perseghin et al. 1996). It could be speculated that the increase in insulin sensitivity following resistance exercise is also associated with a net reduction in skeletal muscle glycogen and/or lipid content. However, literature on the metabolic demands of resistance exercise is scarce. Early reports suggest that energy needs during resistance exercise can be provided with only minor activation of glycogenolysis or lipolysis (Keul et al. 1978).
In the present study, we investigated fibre-type-specific changes in skeletal muscle glycogen and lipid content following resistance exercise and subsequent recovery by using semi-quantitative histology techniques. The latter provides an effective strategy to assess fibre-type-specific changes in intramyocellular lipid and/or glycogen content, without the methodological limitations associated with biochemical extraction analyses. In accordance, we recently reported a good correlation between IMTG content as determined by 1H-magnetic resonance spectroscopy (MRS) and fluorescence microscopy (van Loon et al. 2003a). In addition, strong correlations between data on (mixed-muscle) glycogen content obtained by the use of both biochemical and histochemical methods have recently been reported (Schaart et al. 2004). In the present study, mixed muscle glycogen content declined by 33±7% following the resistance exercise session. The latter seems to be in line with previous studies applying biochemical analysis on mixed muscle tissue (Essen-Gustavsson and Tesch 1990; Tesch et al. 1986). We extent their findings by showing that these changes in muscle glycogen are fibre-type-specific, and seem to be tightly coupled to (non-)oxidative capacity (Table 2, Fig. 3). Linear regression revealed a negative correlation between the net reduction in muscle fibre-type glycogen content and fibre-type oxidative capacity (r = −0.556, P<0.05). As such, net changes in muscle fibre glycogen content were more pronounced in type IIx fibres compared to type I muscle fibres, which can be attributed to the greater recruitment of these fibres during high-intensity resistance exercise (Fry 2004). During post-exercise recovery no significant differences in muscle glycogen content were observed over time in the type I, IIa or IIx muscle fibres. Furthermore, we observed a significant 27±7% reduction in type I muscle fibre lipid content (P<0.05). No changes in IMTG content were observed in the type IIa and IIx fibres (Fig. 5). The net reduction in IMTG content was significantly different compared to the type II fibres (P<0.05). On average, type I muscle fibre lipid content was 2.5±0.3 and 8.8±1.4 times greater when compared to the type IIa and IIx fibres, respectively. Due to the many methodological difficulties with the biochemical triacylglycerol extraction analyses on mixed muscle biopsy samples (Howald et al. 2002), we applied (immuno)histochemical IMTG analyses on ORO stained muscle cross-section to enable fibre-type-specific determination of intramyocellular lipid content. The latter might be the reasons why Essen-Gustavsson and Tesch (1990) failed to detect a significant reduction in mixed muscle lipid content following resistance exercise. In accordance, we observed a non-significant 25±10% net decline in calculated mixed muscle lipid content (P=0.087).
The reported net changes in muscle fibre-type-specific lipid content following exercise were positively correlated with muscle fibre-type oxidative capacity (Table 2). Interestingly, within 120 min of post-exercise recovery, muscle fibre lipid content had returned to pre-exercise values. This could be attributed to the substantial increase in circulating plasma FFA concentrations during post-exercise recovery. The latter is in line with reports on IMTG accumulation under conditions of elevated plasma FFA availability, like prolonged fasting (Schrauwen-Hinderling et al. 2003; Stannard et al. 2002), prolonged endurance exercise in regard to inactive muscle tissue (Schrauwen-Hinderling et al. 2003) and/or 48 h of post-exercise recovery on a relatively high-fat diet (van Loon et al. 2003b). The absence of a prolonged net reduction in skeletal muscle lipid content implies that the reported stimulating effects of resistance exercise on whole-body insulin sensitivity is unlikely to be attributed to a reduction in intramuscular lipid content. The latter is in line with the fact that the proposed relationship between IMTG deposition and insulin sensitivity does not appear functional (van Loon and Goodpaster 2005). It has been suggested that the ratio between IMTG content and oxidative capacity likely represents a more appropriate parameter to assess the risk of developing insulin resistance and/or type 2 diabetes (van Loon and Goodpaster 2005). This is especially important when evaluating the benefits of exercise intervention programs, as intervention studies have actually shown IMTG contents to remain stable or even increase despite substantial improvements in muscle oxidative capacity and/or whole-body insulin sensitivity (Bruce et al. 2004; He et al. 2004; Pruchnic et al. 2004).
In conclusion, a single resistance exercise session substantially reduces intramyocellular lipid and glycogen content. These changes are fibre-type-specific and are closely related to fibre-type oxidative capacity. The present data suggest that earlier reports on the acute improvements in whole-body insulin sensitivity following resistance exercise could, at least partly, be attributed to the net reduction in skeletal muscle glycogen content.
References
Bergstrom J (1975) Percutaneous needle biopsy of skeletal muscle in physiological and clinical research. Scand J Clin Lab Invest 35:609–616
Bogardus C, Thuillez P, Ravussin E, Vasquez B, Narimiga M, Azhar S (1983) Effect of muscle glycogen depletion on in vivo insulin action in man. J Clin Invest 72:1605–1610
Bruce CR, Kriketos AD, Cooney GJ, Hawley JA (2004) Disassociation of muscle triglyceride content and insulin sensitivity after exercise training in patients with Type 2 diabetes. Diabetologia 47:23–30
Chapman J, Garvin AW, Ward A, Cartee GD (2002) Unaltered insulin sensitivity after resistance exercise bout by postmenopausal women. Med Sci Sports Exerc 34:936–941
Craig BW, Everhart J, Brown R (1989) The influence of high-resistance training on glucose tolerance in young and elderly subjects. Mech Ageing Dev 49:147–157
Derave W, Hansen BF, Lund S, Kristiansen S, Richter EA (2000) Muscle glycogen content affects insulin-stimulated glucose transport and protein kinase B activity. Am J Physiol Endocrinol Metab 279:E947–E955
Devlin JT, Horton ES (1985) Effects of prior high-intensity exercise on glucose metabolism in normal and insulin-resistant men. Diabetes 34:973–979
Devlin JT, Hirshman M, Horton ED, Horton ES (1987) Enhanced peripheral and splanchnic insulin sensitivity in NIDDM men after single bout of exercise. Diabetes 36:434–439
Essen-Gustavsson B, Tesch PA (1990) Glycogen and triglyceride utilization in relation to muscle metabolic characteristics in men performing heavy-resistance exercise. Eur J Appl Physiol Occup Physiol 61:5–10
Evans WJ (1995) Effects of exercise on body composition and functional capacity of the elderly. J Gerontol A Biol Sci Med Sci 50 Spec No:147–150
Fenicchia LM, Kanaley JA, Azevedo JL Jr, Miller CS, Weinstock RS, Carhart RL, Ploutz-Snyder LL (2004) Influence of resistance exercise training on glucose control in women with type 2 diabetes. Metabolism 53:284–289
Fluckey JD, Hickey MS, Brambrink JK, Hart KK, Alexander K, Craig BW (1994) Effects of resistance exercise on glucose tolerance in normal and glucose-intolerant subjects. J Appl Physiol 77:1087–1092
Fry AC (2004) The role of resistance exercise intensity on muscle fibre adaptations. Sports Med 34:663–679
Garcia-Roves PM, Han DH, Song Z, Jones TE, Hucker KA, Holloszy JO (2003) Prevention of glycogen supercompensation prolongs the increase in muscle GLUT4 after exercise. Am J Physiol Endocrinol Metab 285:E729–E736
Goodpaster BH, Kelley DE, Wing RR, Meier A, Thaete FL (1999) Effects of weight loss on regional fat distribution and insulin sensitivity in obesity. Diabetes 48:839–847
Gosker HR, van Mameren H, van Dijk PJ, Engelen MP, van der Vusse GJ, Wouters EF, Schols AM (2002) Skeletal muscle fibre-type shifting and metabolic profile in patients with chronic obstructive pulmonary disease. Eur Respir J 19:617–625
Gutmann I, Wahlefeld AW (1974) L-(+)-Lactate, determination with lactate dehydrogenase and NAD. In: Bergmeyer HU (ed) Methods in enzymatic analysis, 2nd edn. Academic, New York, pp 1464–1468
He J, Goodpaster BH, Kelley DE (2004) Effects of weight loss and physical activity on muscle lipid content and droplet size. Obes Res 12:761–769
Hegarty BD, Furler SM, Ye J, Cooney GJ, Kraegen EW (2003) The role of intramuscular lipid in insulin resistance. Acta Physiol Scand 178:373–383
Hoppeler H, Howald H, Conley K, Lindstedt SL, Claassen H, Vock P, Weibel ER (1985) Endurance training in humans: aerobic capacity and structure of skeletal muscle. J Appl Physiol 59:320–327
Houmard JA, Tanner CJ, Yu C, Cunningham PG, Pories WJ, MacDonald KG, Shulman GI (2002) Effect of weight loss on insulin sensitivity and intramuscular long-chain fatty acyl-CoAs in morbidly obese subjects. Diabetes 51:2959–2963
Howald H, Boesch C, Kreis R, Matter S, Billeter R, Essen-Gustavsson B, Hoppeler H (2002) Content of intramyocellular lipids derived by electron microscopy, biochemical assays, and (1)H-MR spectroscopy. J Appl Physiol 92:2264–2272
Kadi F, Thornell LE (2000) Concomitant increases in myonuclear and satellite cell content in female trapezius muscle following strength training. Histochem Cell Biol 113:99–103
Keul J, Haralambie G, Bruder M, Gottstein HJ (1978) The effect of weight lifting exercise on heart rate and metabolism in experienced weight lifters. Med Sci Sports 10:13–15
Koopman R, Schaart G, Hesselink MK (2001) Optimisation of oil red O staining permits combination with immunofluorescence and automated quantification of lipids. Histochem Cell Biol 116:63–68
Koopman R, Manders RJ, Zorenc AH, Hul GB, Kuipers H, Keizer HA, van Loon LJ (2005) A single session of resistance exercise enhances insulin sensitivity for atleast 24 h in healthy men. Eur J Appl Physiol 94:180–187
Kraemer WJ, Fry AC (1995) Strength testing: development and evaluation of methodology. In: Maud PJ, Leeds FC (eds) Physiological assessment of human fitness. Human kinetics, UK, pp 115–133
Mabuchi K, Sreter FA (1980) Actomyosin ATPase. II. Fiber typing by histochemical ATPase reaction. Muscle Nerve 3:233–239
Macaluso A, De Vito G (2004) Muscle strength, power and adaptations to resistance training in older people. Eur J Appl Physiol 91:450–472
Mayhew JL, Prinster JL, Ware JS, Zimmer DL, Arabas JR, Bemben MG (1995) Muscular endurance repetitions to predict bench press strength in men of different training levels. J Sports Med Phys Fitness 35:108–113
Mikines KJ, Sonne B, Farrell PA, Tronier B, Galbo H (1988) Effect of physical exercise on sensitivity and responsiveness to insulin in humans. Am J Physiol 254:E248–E259
Miller WJ, Sherman WM, Ivy JL (1984) Effect of strength training on glucose tolerance and post-glucose insulin response. Med Sci Sports Exerc 16:539–543
Nielsen JN, Richter EA (2003) Regulation of glycogen synthase in skeletal muscle during exercise. Acta Physiol Scand 178:309–319
Oakes ND, Bell KS, Furler SM, Camilleri S, Saha AK, Ruderman NB, Chisholm DJ, Kraegen EW (1997a) Diet-induced muscle insulin resistance in rats is ameliorated by acute dietary lipid withdrawal or a single bout of exercise: parallel relationship between insulin stimulation of glucose uptake and suppression of long-chain fatty acyl-CoA. Diabetes 46:2022–2028
Oakes ND, Camilleri S, Furler SM, Chisholm DJ, Kraegen EW (1997b) The insulin sensitizer, BRL 49653, reduces systemic fatty acid supply and utilization and tissue lipid availability in the rat. Metabolism 46:935–942
Perseghin G, Price TB, Petersen KF, Roden M, Cline GW, Gerow K, Rothman DL, Shulman GI (1996) Increased glucose transport-phosphorylation and muscle glycogen synthesis after exercise training in insulin-resistant subjects. N Engl J Med 335:1357–1362
Pruchnic R, Katsiaras A, He J, Kelley DE, Winters C, Goodpaster BH (2004) Exercise training increases intramyocellular lipid and oxidative capacity in older adults. Am J Physiol Endocrinol Metab 287:E857–E862
Schaart G, Hesselink RP, Keizer HA, Van Kranenburg G, Drost MR, Hesselink MK (2004) A modified PAS stain combined with immunofluorescence for quantitative analyses of glycogen in muscle sections. Histochem Cell Biol 122:161–169
Schrauwen-Hinderling VB, van Loon LJ, Koopman R, Nicolay K, Saris WH, Kooi ME (2003) Intramyocellular lipid content is increased after exercise in nonexercising human skeletal muscle. J Appl Physiol 95:2328–2332
Siri WE (1956) The gross composition of the body. Adv Biol Med Physiol 4:238–280
Stannard SR, Thompson MW, Fairbairn K, Huard B, Sachinwalla T, Thompson CH (2002) Fasting for 72 h increases intramyocellular lipid content in nondiabetic, physically fit men. Am J Physiol Endocrinol Metab 283:E1185–E1191
Tesch PA, Colliander EB, Kaiser P (1986) Muscle metabolism during intense, heavy-resistance exercise. Eur J Appl Physiol Occup Physiol 55:362–366
Tsintzas K, Williams C, Constantin-Teodosiu D, Hultman E, Boobis L, Greenhaff P (2000) Carbohydrate ingestion prior to exercise augments the exercise-induced activation of the pyruvate dehydrogenase complex in human skeletal muscle. Exp Physiol 85:581–586
van Loon LJ, Koopman R, Stegen JH, Wagenmakers AJ, Keizer HA, Saris WH (2003a) Intramyocellular lipids form an important substrate source during moderate intensity exercise in endurance-trained males in a fasted state. J Physiol 553:611–625
van Loon LJ, Schrauwen-Hinderling VB, Koopman R, Wagenmakers AJ, Hesselink MK, Schaart G, Kooi ME, Saris WH (2003b) Influence of prolonged endurance cycling and recovery diet on intramuscular triglyceride content in trained males. Am J Physiol Endocrinol Metab 285:E804–E811
van Loon LJ, Koopman R, Manders R, van der Weegen W, van Kranenburg GP, Keizer HA (2004) Intramyocellular lipid content in type 2 diabetes patients compared with overweight sedentary men and highly trained endurance athletes. Am J Physiol Endocrinol Metab 287:E558–565
van Loon LJ and Goodpaster BH (2005) Increased intramuscular lipid storage in the insulin-resistant and endurance-trained state. Pflugers Arch
Watt MJ, Heigenhauser GJ, Spriet LL (2002) Intramuscular triacylglycerol utilization in human skeletal muscle during exercise: is there a controversy? J Appl Physiol 93:1185–1195
Wojtaszewski JF, Hansen BF, Kiens B, Richter EA (1997) Insulin signaling in human skeletal muscle: time course and effect of exercise. Diabetes 46:1775–1781
Wojtaszewski JF, Hansen BF, Gade, Kiens B, Markuns JF, Goodyear LJ, Richter EA (2000) Insulin signaling and insulin sensitivity after exercise in human skeletal muscle. Diabetes 49:325–331
Wojtaszewski JF, Jorgensen SB, Frosig C, MacDonald C, Birk JB, Richter EA (2003) Insulin signalling: effects of prior exercise. Acta Physiol Scand 178:321–328
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koopman, R., Manders, R.J.F., Jonkers, R.A.M. et al. Intramyocellular lipid and glycogen content are reduced following resistance exercise in untrained healthy males. Eur J Appl Physiol 96, 525–534 (2006). https://doi.org/10.1007/s00421-005-0118-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-0118-0