
Abstract
Objectives
Neck–shoulder pain (NSP) is a common work-related musculoskeletal disorder with unclear mechanisms. Changes in physical activity and autonomic nervous system regulation may be involved in the pathogenesis of chronic NSP. The aim of the current study was to investigate autonomic regulation in relation to physical activity and perceived symptoms during work and leisure time among workers with chronic NSP (n = 29) as compared to a healthy control group (CON, n = 27).
Methods
Physical activity was objectively monitored for 7 days using accelerometry. Beat-to-beat heart rate was collected continuously for 72 h, with simultaneous momentary ratings of pain, stress, and fatigue. Duration of sitting/lying, standing and walking, number of steps, and energy expenditure were used as measures of physical activity. Heart rate variability (HRV) indices were extracted in time and frequency domains as reflecting autonomic regulation. Data were divided into work hours, leisure time, and sleep.
Results
The NSP group rated higher levels of stress and fatigue at work and leisure, and reduced sleep quality as compared to CON. Elevated heart rate and reduced HRV were found in NSP compared with CON, especially during sleep. The NSP group demonstrated a different pattern of physical activity than CON, with a lower activity level in leisure time. Higher physical activity was associated with increased HRV in both groups.
Conclusion
Changes in HRV reflected an autonomic imbalance in workers with chronic musculoskeletal pain. This can be explained by reduced physical activity in leisure time. Intervention studies aimed at increasing physical activity may shed further light on the association between autonomic regulation and physical activity in work-related NSP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic neck–shoulder pain (NSP) is a common musculoskeletal disorder (MSD) in working populations (Côté et al. 2009). It is associated with high costs due to sick leave (Hansson and Hansson 2005) and loss in productivity (Hagberg et al. 2007) and impacts on quality of life (Rezai et al. 2009). Thus, NSP constitutes a significant occupational health problem.
Repetitive physical loads, sedentary work, and psychosocial stressors are risk factors for the development of NSP (Larsson et al. 2007), potentially because they induce sustained physiological responses such as increases in heart rate and blood pressure, elevated muscle activity, and reduced muscle circulation (Lundberg 2006; Sjøgaard et al. 2000). However, the underlying mechanisms are still not clear. Therefore, strategies for the prevention and treatment for work-related NSP require further understanding about the core mechanisms.
The autonomic nervous system (ANS) is a key stress system in the body, composing a bridge between the brain and the periphery that is closely involved in pain perception and adaptation to various physical and mental stressors (Ulrich-Lai and Herman 2009; Benarroch 2006; Martinez-Lavin 2012). Research suggests that the ANS is involved in both the development and maintenance of chronic musculoskeletal pain (Passatore and Roatta 2006; Visser and van Dieën 2006; Martinez-Lavin 2012). Autonomic imbalance with a predominant sympathetic nervous activation is associated with poor adaptation and increased sensitivity to pain, while chronic pain in turn may affect the regulation of the ANS. Laboratory studies have demonstrated autonomic imbalance, as characterized by increased sympathetic and reduced parasympathetic activity at rest and with altered autonomic reactivity to stressors, in persons with chronic NSP (Gockel et al. 1995; Hallman et al. 2011), fibromyalgia (Martinez-Lavin 2007), and low back pain (Kalezic et al. 2007), although contrasting results have also been reported (Sjörs et al. 2009; Nilsen et al. 2007). Since most studies have been conducted in a laboratory setting, ecologically valid assessment methods are needed to provide information about autonomic regulation in real-life situations, such as work, leisure time, and sleep.
Heart rate variability (HRV) is a noninvasive tool for the assessment of sympathetic and parasympathetic modulation of the heart. Generally, a larger HRV reflects a healthier and more adaptable ANS, while diminished HRV indicates autonomic imbalance (Malik 1996). Results from 24-h HRV analyses have indicated the need to address the circadian pattern of autonomic regulation in conditions of chronic musculoskeletal pain (Martínez-Lavín et al. 1998; Mork et al. 2013). In accordance, we recently found a diminished parasympathetic activation during sleep in subjects with chronic NSP compared with healthy controls (Hallman and Lyskov 2012). However, this needs to be confirmed in a larger, more homogenous group of workers with NSP, using the latest standards for long-term monitoring of HRV and physical activity while simultaneously assessing perceived symptoms using electronic diaries.
Importantly, pain-associated factors such as physical inactivity, perceived stress, and poor sleep need to be accounted for since they influence HRV (Clays et al. 2011; Trinder et al. 2012; Rennie et al. 2003). Particularly, physical activity and exercise are known for enhancing musculoskeletal health and cardiovascular function (Warburton et al. 2006). High-intensity activities induce acute increases in sympathetic activity and diminished parasympathetic activity (Hautala et al. 2010), while the opposite effect of increasing physical activity occurs in the long run. Epidemiological studies indicate a positive association between increasing leisure-time physical activity and improved parasympathetic cardiac activity at rest (Rennie et al. 2003; Melanson 2000).
In spite of the substantial health-enhancing effects of leisure-time physical activity (Blair and Morris 2009), contrasting results have been shown for physical activity during work. For instance, high occupational physical activity was found to increase the risk of long-term sickness absence (Holtermann et al. 2012b) and all-cause mortality (Holtermann et al. 2012a). Also, high occupational physical activity was associated with a higher ambulatory blood pressure in workers, whereas the opposite relationship was found for physical activity in leisure time (Clays et al. 2012). Thus, it is important to investigate characteristics of physical activity and autonomic regulation by discriminating between work and leisure time.
In accordance with the fear-avoidance model (Leeuw et al. 2007) and the avoidance–endurance model (Hasenbring et al. 1994), decreased activity levels can be expected with chronic pain. However, objective assessment methods have found rather small differences, if any, in total activity level between those with and without chronic MSDs (van Weering et al. 2007). Instead, a different time pattern in physical activity was observed among patients with low back pain (van Weering et al. 2009) and in persons with chronic NSP (Hallman and Lyskov 2012) as compared with healthy persons, mainly with lower activity levels in the evening. Therefore, long-term ambulatory recordings of HRV in combination with objective methods for accurate assessment of daily physical activity are needed in order to test these ideas in workers with chronic NSP.
Aim
The aim of this study was to investigate daily physical activity, autonomic regulation, and perceived symptoms (i.e., pain, stress, and fatigue) during work and leisure time among workers afflicted with chronic NSP and their healthy counterparts.
We hypothesize that the NSP group will be characterized by a reduced level of physical activity in leisure time and reduced parasympathetic activity during sleep, as compared with controls. We further hypothesize that daily physical activity will be positively associated with parasympathetic activity during sleep.
Methods
Participants
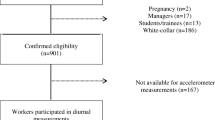
Twenty-nine workers between 25 and 59 years of age reporting chronic pain in the neck–shoulder region (NSP) and 27 healthy controls (CON) without a recent history of pain participated in the study. See Table 1 for group characteristics. The groups were matched for age and gender, and nearly matched for type of work, i.e., office work (NSP, n = 19; CON, n = 20) or production (NSP, n = 10; CON, n = 7). Subjects in both groups were recruited through advertisement at a global manufacturing company within the industrial sector at a site in the middle part of Sweden, in cooperation with ergonomists and health care specialists working at the company. The type of work was assessed using self-reports and company data, which were evaluated by an ergonomist. Office work was characterized by low physical exposure (e.g., sedentary work) while production included more varying exposures, ranging from light industrial work tasks to physically heavy tasks.
Inclusion and exclusion criteria were first evaluated using interviews and questionnaires. Inclusion in the NSP group required non-traumatic chronic pain (>6 months) localized to the neck–shoulder region (i.e., primarily the neck and/or the trapezius muscles). Controls should report that they were healthy and asymptomatic, without pain over the previous 6 months. Subjects had to be between 20 and 59 years of age and employed, and work at least 75 % of full-time. Both males and females were free to take part in the study. Exclusion criteria were the regular use of medications that could affect the ANS or pain perception, including antidepressants, benzodiazepines, beta-blockers, and anti-inflammatory drugs. Further, individuals reporting comorbidity of other disorders known to affect autonomic regulation or pain processing were also excluded, for example diagnoses of rheumatism, diabetes, depression, chronic neurological or endocrinological syndromes, or drug abuse, as well as pain of traumatic origin. In order to avoid possible effects of sick leave on physical activity, workers reporting sick leave (>2 weeks over the past 3 months) were excluded.
Eligible subjects were further examined by a specialized physiotherapist and performed a sub-maximal fitness test using a cycle ergometer (Åstrand and Rhyming 1954). Subjects were classified into chronic NSP (e.g., trapezius myalgia or tension neck syndrome), corresponding to the International Classification of Diseases (ICD) code M 79.1, as they reported chronic pain from the neck–shoulder region, muscle stiffness, and tenderness at palpation, without restricted range of movement of the neck during the examination (Larsson et al. 2007). All volunteers provided written informed consent and were given information about the study prior to participation. The study was approved by the local ethics committee (2010/433) and was conducted according to the Declaration of Helsinki.
Procedure
The ambulatory recordings were carried out at the workplace, which included daytime work, leisure time, and sleep. A typical measurement started at the beginning of a regular week and continued for 7 days (Fig. 1).

Assessment protocol with baseline questionnaires and ambulatory measurements. KSQ Karolinska Sleep Questionnaire, SEQ Stress-Energy Questionnaire, IPAQ International Physical Activity Questionnaire, SF36 Short Form health survey
A heart rate monitor and an electronic diary were worn by the subjects for a duration of approximately 72 h, typically representing three full workdays of daytime work. Physical activity was assessed over 7 days, including both workdays and non-workdays. The devices were attached to the subject and were only taken off for a shower or bath. Subjects were instructed to rate their perceived pain intensity, stress, and fatigue when indicated by an auditory alarm. They were instructed to go about their regular activities and were advised to contact the examiner if they had any problem with the equipment.
Ambulatory measurements
Physical activity was measured using the ActivPAL™3 monitor (PAL Technologies Ltd., Glasgow, UK) attached to the thigh using self-adhesive tape. Physical activity and posture (sitting/lying and standing) were measured using a single triaxial accelerometer that produces a continuous signal (20 Hz sampling frequency) related to the movement and inclination of the thigh. The device has shown good validity and reliability (Ryan et al. 2006).
Heart rate was collected using a heart rate monitor, Firstbeat Bodyguard (Firstbeat Technologies Ltd., Jyväskylä, Finland), with a two-lead configuration attached using pre-glued Ag/AgC1 electrodes (Biopac Systems Inc., USA) on cleansed skin.
A specially designed electronic diary, installed on a Windows mobile phone (HTC HD2), was used for momentary ratings during the ambulatory assessment. The intensity of current pain, stress, and general fatigue was assessed in random order using the Borg CR10 scale (Borg 1998) every second hour from 09:00 to 17:00, and at 20:00, as well as 30 min after awakening and prior to going to bed. A reminder alarm was repeated three times at 10-min intervals in cases of missed responses. An instruction manual was also provided. In addition, a paper diary was used to collect written reports of times of working, going to bed, sleeping, and waking up.
Questionnaires
A battery of questionnaires was used to characterize the subjects with regard to symptoms, general health, and sleep quality.
Perceived pain intensity was measured using the Borg CR10 scale at the region of pain, based on “six months,” “last week,” and “currently” (Borg 1998). The response scale ranges from 0 (“nothing at all”) to 10 (“extremely strong”), and subjects were allowed to rate any number, including decimals, in between. Pain localization was assessed using a modified pain drawing (Margolis et al. 1988).
Stress and energy were measured using the Stress-Energy Questionnaire (Kjellberg and Wadman 2002). The stress scale consists of three positively evaluated low activation adjectives (“rested,” “relaxed,” and “calm”) and three negatively evaluated high activation adjectives (“tense,” “stressed,” and “pressured”). The energy scale consists of three negatively evaluated low activation adjectives (“dull,” inefficient,” and “passive”) and three positively evaluated high activation adjectives (“active,” “energetic,” and focused”). The six-point response scale (0–5) ranges from “not at all” to “extremely.” Subjects were asked to recall their perceived stress and energy over the previous 6 months, both “during work” and “after work.”
The Short Form health survey (SF-36) was used to assess health-related functions and quality of life (Ware and Gandek 1998). The survey covers four health domains related to physical health (general health perceptions, physical functioning, bodily pain, and physical role limitations) and four domains related to mental health (general mental health perceptions, emotional role limitations, vitality (energy), and social functioning). The two summary scales physical health and mental health were used, whereby the normative mean is equal to 50 (SD = 10) and higher values reflect better health.
The Karolinska Sleep Questionnaire (KSQ) (Kecklund and Åkerstedt 1992) was used to assess sleep quality based on four items: difficulty falling asleep, repeated awakenings, premature awakening, and disturbed sleep. Subjects responded to the questions based on their perceptions over the past 6 months using a response scale ranging from 1 (always) to 6 (never). These four items were summed up in order to create a sleep quality index ranging from 0 to 24, whereby higher values indicated enhanced sleep.
Data processing
Time spent walking, standing and lying/sitting, number of steps, and cadence (steps/min) was calculated off-line using the proprietary software. Based on the duration and intensity of these activities, the metabolic equivalent (MET) was estimated for each hour and was used as a measure of energy expenditure (i.e., lying/sitting = 1.25 MET; standing = 1.4 MET; stepping 120 steps/min = 4 MET; cadence other than 120 steps per minute was scaled linearly from standing). Due to technical problems, data from two subjects with NSP were not retrieved.
HRV was analyzed using Firstbeat HEALTH (version 3.1.1.0, Firstbeat Technologies Ltd., Jyväskylä, Finland). Time series of beat-to-beat (RR) intervals were visually inspected for electrical artifacts and abnormal heartbeats. Procedures for automatic data editing and short-term Fourier transform filtering have previously been described by Saalasti (2003). Only periods free from artifacts, e.g., due to noise, ectopic beats, or non-wear time, were analyzed. On average, a 1-h segment included 97.4 % (SD 3.7 %) acceptable data. Two NSP and two CON subjects were excluded from the final analysis due to a large proportion of artifacts.
Indices of HRV were extracted for each hour in both time and frequency domains. The time domain measures were RR intervals, SDNN (the standard deviation of RR intervals), and RMSSD (the square root of the mean squared successive differences of successive RR intervals). The frequency domain measures were VLF (very low frequency 0–0.03 Hz), LF (low frequency 0.04–0.15 Hz), and HF (high frequency 0.15–0.4 Hz) spectral power (ms2). Respiratory frequency was calculated based on the frequency distribution of the HF power spectra (Saalasti 2003).
RMSSD and HF were used as measures of parasympathetic (vagal) activity, whereas SDNN and LF are influenced by both the sympathetic and parasympathetic nervous systems. LF/HF was used as a measure of sympathetic-to-parasympathetic balance (Malik 1996). As the exact contribution of the ANS to VLF is largely unknown, it was considered an explorative variable.
All data were obtained from the long-term recording, including the objective measures (RR intervals, HRV, physical activity scores, and METs), and momentary ratings were imported to the Spike2 software (version, 7.03, Cambridge Electronic Design) for visual data inspection. Data were processed and extracted on an hour-to-hour basis, and mean values for each hour were pooled for work, leisure time, and sleep.
Statistical analyses
Group differences (NSP–CON) in subject characteristics were analyzed using t tests. Repeated measures analysis of variance (ANOVA) with group (NSP–CON) as a between-subjects factor and time (work–leisure) as a within-subjects factor was carried out in order to analyze the main effects and the interaction effects for physical activity (MET, walk, stand, sedentary, and steps), and perceived, stress, and fatigue. Differences in physical activity variables between workdays and work-free days were analyzed using ANOVA (group × time (workdays–work-free days)). For HRV indices, ANOVAs were carried out with group (NSP–CON) as a between-subjects factor and time (work–leisure–sleep) as a within subject factor. In addition, ANCOVAs (group × time) were used for HRV to investigate possible associations with physical activity (total MET or MET in leisure time), momentary stress ratings, and sleep quality. All statistical analyses were conducted using SPSS version 20, and p values < 0.05 were considered significant. A priori power analysis indicated that 25 subjects in each group (NSP–CON) would be sufficient for detecting group differences in objective physical activity, HRV, and self-ratings with adequate statistical power (ß = 0.8 and α = 0.05).
Results
Background data
There were no differences between NSP and CON groups regarding age, gender (NSP: women, n = 13; CON women, n = 12), BMI, or physical fitness (VO2max). The NSP group reported higher levels of perceived pain and stress, impaired physical health, and worse quality of sleep than CON. Also, the NSP group reported longer workdays than CON (Table 1).
Differences in physical activity
The main effects of time (work–leisure) indicated an increased level of physical activity from work to leisure time for mean MET, duration walking and steps/h (p < 0.05). No time effect was observed for sedentary (lie/sit) or standing time. Mean activity levels were lower during workdays than on work-free days, as reflected in MET (p = 0.002), walking time (p < 0.001), and steps/h (p = 0.002). Sedentary time was reduced from workdays to work-free days (p = 0.008).
The group effect (NSP–CON) indicated more time spent in standing posture for NSP than CON (p = 0.037). Group-by-time interactions were found for MET (p = 0.039) and steps (p = 0.042), with NSP showing a smaller increase in physical activity from work to leisure time as compared to CON (Table 2). Similar trends were observed when only workdays were included in the analysis, although with smaller p values for the interaction effects (group × time): MET (p = 0.009), walking time (p = 0.026), steps (p = 0.009), and sitting/lying (p = 0.069).
Differences in heart rate variability
NSP showed shorter RR intervals and attenuated HRV in RMSSD, SDNN, and VLF power compared to CON, as indicated by the main effects of group (Table 3). ANOVAs (group × time) revealed significant time effects (work–leisure–sleep), which indicated that RR intervals, RMSSD, VLF, LF, and HF were increased during nighttime sleep while LF/HF was attenuated compared to work and leisure time (all p < 0.05). SDNN was increased and LF was reduced during leisure time as compared to sleep and work (all p < 0.05).
Interaction effects (group × time) were found for RR intervals, RMSSD, LF, and VLF, in terms of NSP showing diminished HRV during work and sleep, but not in leisure time. There was no effect of group on respiration rate.
ANCOVAs adjusted for total METs, perceived stress, and sleep quality indicated that HRV was positively associated with physical activity, although the group differences in HRV remained significant (Table 3). Including MET in leisure time in the ANCOVA models resulted in nonsignificant main effects of group, while the interactions (group × time) still indicated a significantly different pattern of HRV in the NSP group. Perceived stress or sleep quality was not associated with HRV.
Momentary ratings
Momentary CR10 ratings are shown in Fig. 2. Significant group effects indicated that perceived pain (p < 0.0001), stress (p < 0.001), and fatigue (p = 0.006) were higher in the pain group at both work and leisure time. Time effects revealed that perceived stress level was reduced from working hours to leisure time (p < 0.001), whereas perceived fatigue increased from work to leisure time (p < 0.001). No interaction effects (group × time) were found.

Momentary ratings of pain, stress, and fatigue averaged for work and leisure time in a neck–shoulder pain (NSP) and b control (CON) groups. Error bars represent standard deviation
Discussion
Based on a long-term monitoring of physical activity, HRV, and perceived symptoms, the present study found reduced leisure-time physical activity, diminished HRV, and higher stress and fatigue levels among workers afflicted with chronic NSP, as compared to a group of healthy workers. Several parameters of HRV in both time and frequency domain were positively associated with physical activity.
Changes in physical activity
Evidence regarding the health benefits of physical activity extends to different occupational groups (Warburton et al. 2006). The present study confirmed the hypothesis of reduced physical activity in leisure time among workers with chronic NSP. The reference group showed enhanced energy expenditure (METs) during leisure time compared to work, which corresponded to an increased duration of walking and more steps per hour. In comparison, the NSP group showed only a marginal increase in physical activity from work to leisure time, in terms of both intensity and duration. In accordance, altered activity patterns have been observed in persons with chronic muscle pain in the neck–shoulder or lower back (Hallman and Lyskov 2012; van Weering et al. 2009). In contrast, apart from an increased standing time in NSP compared with CON, overall physical activity levels were not markedly different between groups. Increased standing was an unexpected finding among persons with NSP and may not be fully explained by fear-avoidance behavior (Leeuw et al. 2007), which is a model based on low back pain. Thus, it may be specifically addressed in the future studies.
The placement of the activity monitor on the thigh is widely used for the assessment of a wide range of daily activities, including sedentary time, standing, and walking (Ryan et al. 2006), although it may be less accurate in detecting high-intensity activities. This is a potential limitation of the study.
Analyses of sedentary time are useful for investigating physical inactivity, which is uniquely associated with poor health outcomes (Hamilton et al. 2008). We did not observe any marked group difference in sedentary time, although when the analyses were restricted to workdays CON showed a trend toward reduced duration of lying/sitting from work to leisure, compared to NSP. Discriminating between seated and lying posture may, thus, have provided further information about inactivity in NSP. Still, the lack of increase in physical activity during leisure time may suggest that workers with pain spend more of their resources while accomplishing their work tasks. Unexpectedly, the NSP group reported longer workdays than CON. Apart from poor sleep quality and the presence of chronic pain (Fishbain et al. 2004), this might explain why perceived fatigue was higher in the NSP group. As a result, higher fatigue in NSP may have contributed to lower activity levels in leisure time. Altogether, these results indicate that physical activity patterns might be equally, or even more, important than total activity levels for musculoskeletal health outcomes among workers. Considering that low physical activity in leisure time is associated with an increased risk for cardiovascular mortality among the working population (Holtermann et al. 2013), we suggest that future intervention studies should aim at increasing physical activity in leisure time among workers with chronic NSP.
As regards the whole sample, work hours showed a predominance of sedentary time (> 50 %), which may be explained by a relatively large proportion of office workers in the current sample. The influence of occupational type (office–production) was not included in the statistical models, as the study focused on differences between NSP and CON groups. However, in the whole study group, physical activity levels were higher during work-free days compared with workdays, which suggests that work exposure impacts on inactivity.
Perceived stress at work is a possible mediator for reduced physical activity in chronic muscle pain, acting as a further barrier (Ryan et al. 2010; Wemme and Rosvall 2005). Persons with chronic back pain and high levels of stress were found to have lower activity levels than their non-stressed counter parts (Ryan et al. 2010). However, these results may have been confounded by fewer employed subjects in the high-stress group. We found a higher stress level in the NSP group compared with CON, although this did not affect physical activity in the current study. Importantly, workers on sick leave were not included in our study, and all subjects were employed and worked during the measurement.
Changes in autonomic regulation
In the present study, HRV analyses, including work, leisure time, and sleep, revealed a reduced parasympathetic component (i.e., diminished HRV) in the NSP group during work and sleep, as compared to CON. This was in line with the study hypothesis. Models of chronic MSDs have pointed out the involvement of the ANS in the maintenance of regional and widespread pain (Passatore and Roatta 2006; Martinez-Lavin 2007). Aberrant ANS regulation may contribute to pain sensitization at both central and peripheral levels. Laboratory studies have found signs of increased sympathetic and reduced parasympathetic activity at rest in subjects with NSP (Hallman et al. 2011; Gockel et al. 1995). In accordance, studies indicate that chronic pain is associated with an altered autonomic balance during sleep, resulting in excessive sympathetic activation (Chouchou et al. 2011; Martínez-Lavín et al. 1998; Hallman and Lyskov 2012). Although worse sleep quality was reported in NSP than CON, ANCOVAs did not reveal any effect of this factor on HRV.
The present results may reflect a pain-induced alteration in ANS regulation with a shift toward sympathetic predominance. It is also possible that the pain-afflicted workers had reduced HRV prior to the development of pain. Due to the cross-sectional study design, however, inferences about causal relationships are limited. Furthermore, shorter RR intervals (i.e., increased heart rate) were observed in the pain group. This is in accordance with previous studies on chronic neck pain (Gockel et al. 1995; Sjörs et al. 2009; Hallman et al. 2011) and in contrast to the results reported by other authors (Nilsen et al. 2007). As there was no group difference in VO2max, as assessed using a sub-maximal test, a potential confounding effect of physical fitness could be ruled out.
Physical activity, perceived stress, and poor sleep are possible confounders for diminished HRV; yet few studies have investigated these factors simultaneously with markers of autonomic function in individuals with musculoskeletal pain. A strength of the current study is that we addressed this issue by performing long-term ambulatory monitoring of HRV, physical activity and perceived pain, stress, and fatigue in workers with chronic NSP. Thus, between-subjects variance in physical activity and stress perception were taken into account.
Total physical activity (MET/day) was positively associated with HRV (i.e., enhanced parasympathetic activation with increasing physical activity), but did not account substantially for the observed differences in HRV between groups. As expected, HRV was also positively associated with leisure-time physical activity. Thus, when MET in leisure time was included in the ANCOVAb model (Table 3), only the pattern of HRV (interaction: work–leisure–sleep) remained significant. This suggests that the activity pattern, i.e., reduced physical activity in leisure time, contributed to the attenuation of parasympathetic activity observed in the pain group during work and sleep. This is an important finding, which is in line with our theory that low physical activity in leisure time may contribute to worsening of NSP symptoms due to changes in ANS regulation.
Furthermore, the NSP group rated higher perceived stress at work and leisure time than CON, both momentarily using CR10 ratings and retrospectively using the Stress-Energy Questionnaire. A negative association between work stress and HRV has previously been reported (Clays et al. 2011). Contrary to the hypothesis, perceived stress did not influence HRV in the current study. However, as the observed stress levels were relatively low, a direct effect of stress on the physiological systems would not be expected.
In conclusion, the observed aberrations in HRV during sleep reflected an imbalanced autonomic regulation among workers with chronic neck–shoulder pain. Diminished parasympathetic activity can be explained by reduced physical activity in leisure time and may further reflect an insufficient adaptability to physical and/or psychological workloads among workers with chronic neck–shoulder pain. Follow-up and intervention studies are needed to evaluate the effects of physical activity changes on pain and autonomic regulation.
References
Åstrand PO, Rhyming I (1954) A nomogram for calculation of aerobic capacity from pulse rate during submaximal work. J Appl Physiol 7:215–221
Benarroch E (2006) Pain-autonomic interactions. Neurol Sci 27:s130–s133
Blair SN, Morris JN (2009) Healthy hearts—and the universal benefits of being physically active: physical activity and health. Ann Epidemiol 19(4):253–256. doi:10.1016/j.annepidem.2009.01.019
Borg G (1998) Borg’s perceived exertion and pain scales. Human Kinetics, Champaign
Chouchou F, Pichot V, Perchet C, Legrain V, Garcia-Larrea L, Roche F, Bastuji H (2011) Autonomic pain responses during sleep: a study of heart rate variability. Eur J Pain 15(6):554–560. doi:10.1016/j.ejpain.2010.11.011
Clays E, De Bacquer D, Crasset V, Kittel F, de Smet P, Kornitzer M, Karasek R, De Backer G (2011) The perception of work stressors is related to reduced parasympathetic activity. Int Arch Occup Environ Health 84(2):185–191. doi:10.1007/s00420-010-0537-z
Clays E, De Bacquer D, Van Herck K, De Backer G, Kittel F, Holtermann A (2012) Occupational and leisure time physical activity in contrasting relation to ambulatory blood pressure. BMC Public Health 12(1):1002
Côté P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, Carragee EJ, Haldeman S, Nordin M, Hurwitz EL, Guzman J, Peloso PM (2009) The burden and determinants of neck pain in workers: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manip Physiol Ther 32(2, Supplement 1):S70–S86
Fishbain DA, Cutler RB, Cole B, Lewis J, Smets E, Rosomoff HL, Steele Rosomoff R (2004) Are patients with chronic low back pain or chronic neck pain fatigued? Pain Med 5(2):187–195
Gockel M, Lindholm H, Alaranta H, Viljanen A, Lindquist A, Lindholm T (1995) Cardiovascular functional disorder and stress among patients having neck–shoulder symptoms. Ann Rheum Dis 54(6):494–497. doi:10.1136/ard.54.6.494
Hagberg M, Vilhemsson R, Tornqvist EW, Toomingas A (2007) Incidence of self-reported reduced productivity owing to musculoskeletal symptoms: association with workplace and individual factors among computer users. Ergonomics 50(11):1820–1834. doi:10.1080/00140130701674539
Hallman DM, Lyskov E (2012) Autonomic regulation, physical activity and perceived stress in subjects with musculoskeletal pain: 24-hour ambulatory monitoring. Int J Psychophysiol 86:276–282. doi:10.1016/j.ijpsycho.2012.09.017
Hallman DM, Lindberg L-G, Arnetz BB, Lyskov E (2011) Effects of static contraction and cold stimulation on cardiovascular autonomic indices, trapezius blood flow and muscle activity in chronic neck–shoulder pain. Eur J Appl Physiol 111(8):1725–1735. doi:10.1007/s00421-010-1813-z
Hamilton M, Healy G, Dunstan D, Zderic T, Owen N (2008) Too little exercise and too much sitting: inactivity physiology and the need for new recommendations on sedentary behavior. Current Cardiovasc Risk Rep 2(4):292–298. doi:10.1007/s12170-008-0054-8
Hansson EK, Hansson TH (2005) The costs for persons sick-listed more than one month because of low back or neck problems. A two-year prospective study of Swedish patients. Eur Spine J 14(4):337–345. doi:10.1007/s00586-004-0731-3
Hasenbring M, Marienfeld G, Kuhlendahl D, Soyka D (1994) Risk factors of chronicity in lumbar disc patients: a prospective investigation of biologic, psychologic, and social predictors of therapy outcome. Spine 19(24):2759–2765
Hautala AJ, Karjalainen J, Kiviniemi AM, Kinnunen H, Mäkikallio TH, Huikuri HV, Tulppo MP (2010) Physical activity and heart rate variability measured simultaneously during waking hours. Am J Physiol Heart Circul Physiol 298(3):H874–H880. doi:10.1152/ajpheart.0 0856.2009
Holtermann A, Burr H, Hansen J, Krause N, Søgaard K, Mortensen O (2012a) Occupational physical activity and mortality among Danish workers. Int Arch Occup Environ Health 85(3):305–310. doi:10.1007/s00420-011-0668-x
Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G (2012b) The health paradox of occupational and leisure-time physical activity. Br J Sports Med 46(4):291–295. doi:10.1136/bjsm.2010.079582
Holtermann A, Marott JL, Gyntelberg F, Søgaard K, Suadicani P, Mortensen OS, Prescott E, Schnohr P (2013) Does the benefit on survival from leisure time physical activity depend on physical activity at work? A prospective cohort study. PLoS ONE 8(1):e54548. doi:10.1371/journal.pone.0054548
Kalezic N, Åsell M, Kerschbaumer H, Lyskov E (2007) Physiological reactivity to functional tests in patients with chronic low back pain. J Musculoskelet Pain 15(1):29–40
Kecklund G, Åkerstedt T (1992) The psychometric properties of the Karolinska Sleep Questionnaire. J Sleep Res 1(1):113
Kjellberg A, Wadman C (2002) Subjektiv stress och dess samband med psykosociala arbetsförshållanden och besvär. En prövning av Stress-Energi-modellen. Arbete och hälsa, vol 12. National Institute of Working life, Stockholm
Larsson B, Søgaard K, Rosendal L (2007) Work related neck–shoulder pain: a review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Practice Res Clin Rheumatol 21(3):447–463
Leeuw M, Goossens M, Linton S, Crombez G, Boersma K, Vlaeyen J (2007) The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med 30(1):77–94
Lundberg U (2006) Stress, subjective and objective health. Int J Soc Welf 15:S41–S48. doi:10.1111/j.1468-2397.2006.00443.x
Malik M (1996) Task force of the European Society of Cardiology and The North American Society of pacing and electrophysiology. Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Eur Heart J 93(5):1043–1065
Margolis RB, Chibnall JT, Tait RC (1988) Test–retest reliability of the pain drawing instrument. Pain 33(1):49–51. doi:10.1016/0304-3959(88)90202-3
Martinez-Lavin M (2007) Biology and therapy of fibromyalgia. Stress, the stress response system, and fibromyalgia. Arthritis Res Ther 9(4):216
Martinez-Lavin M (2012) Fibromyalgia: when distress becomes (un)sympathetic pain. Pain Res Treat. doi:10.1155/2012/981565
Martínez-Lavín M, Hermosillo AG, Rosas M, Soto ME (1998) Circadian studies of autonomic nervous balance in patients with fibromyalgia: a heart rate variability analysis. Arthritis Rheum 41(11):1966–1971
Melanson EL (2000) Resting heart rate variability in men varying in habitual physical activity. Med Sci Sports Exerc 32(11):1894–1901
Mork PJ, Nilsson J, Lorås HW, Riva R, Lundberg U, Westgaard RH (2013) Heart rate variability in fibromyalgia patients and healthy controls during non-REM and REM sleep: a case–control study. Scand J Rheumatol 1–4. doi:10.3109/03009742.2012.755564
Nilsen KB, Sand T, Westgaard RH, Stovner LJ, White LR, Bang Leistad R, Helde G, Rø M (2007) Autonomic activation and pain in response to low-grade mental stress in fibromyalgia and shoulder/neck pain patients. Eur J Pain 11(7):743–755
Passatore M, Roatta S (2006) Influence of sympathetic nervous system on sensorimotor function: whiplash associated disorders (WAD) as a model. Eur J Appl Physiol 98(5):423–449
Rennie KL, Hemingway H, Kumari M, Brunner E, Malik M, Marmot M (2003) Effects of moderate and vigorous physical activity on heart rate variability in a British study of civil servants. Am J Epidemiol 158(2):135–143. doi:10.1093/aje/kwg120
Rezai M, Côté P, Cassidy J, Carroll L (2009) The association between prevalent neck pain and health-related quality of life: a cross-sectional analysis. Eur Spine J 18(3):371–381. doi:10.1007/s00586-008-0823-6
Ryan CG, Grant PM, Tigbe WW, Granat MH (2006) The validity and reliability of a novel activity monitor as a measure of walking. Br J Sports Med 40(9):779–784. doi:10.1136/bjsm.2006.027276
Ryan CG, Gray HG, Newton M, Granat MH (2010) The relationship between psychological distress and free-living physical activity in individuals with chronic low back pain. Man Ther 15(2):185–189
Saalasti S (2003) Neural networks for heart rate time series analysis. University of Jyväskylä, Jyväskylä
Sjøgaard G, Lundberg U, Kadefors R (2000) The role of muscle activity and mental load in the development of pain and degenerative processes at the muscle cell level during computer work. Eur J Appl Physiol 83(2):99–105. doi:10.1007/s004210000285
Sjörs A, Larsson B, Dahlman J, Falkmer T, Gerdle B (2009) Physiological responses to low-force work and psychosocial stress in women with chronic trapezius myalgia. BMC Musculoskelet Disord 10(1):63
Trinder J, Waloszek J, Woods M, Jordan A (2012) Sleep and cardiovascular regulation. Pflügers Archiv Eur J Physiol 463(1):161–168. doi:10.1007/s00424-011-1041-3
Ulrich-Lai YM, Herman JP (2009) Neural regulation of endocrine and autonomic stress responses. Nat Rev Neurosci 10 (6):397–409. http://www.nature.com/nrn/journal/v10/n6/suppinfo/nrn2647_S1.html
van Weering M, Vollenbroek-Hutten MMR, Kotte EM, Hermens HJ (2007) Daily physical activities of patients with chronic pain or fatigue versus asymptomatic controls. A systematic review. Clin Rehabil 21(11):1007–1023. doi:10.1177/0269215507078331
van Weering MGH, Vollenbroek-Hutten MMR, Tönis TM, Hermens HJ (2009) Daily physical activities in chronic lower back pain patients assessed with accelerometry. Eur J Pain 13(6):649–654
Visser B, van Dieën JH (2006) Pathophysiology of upper extremity muscle disorders. J Electromyogr Kinesiol 16(1):1–16
Warburton DER, Nicol CW, Bredin SSD (2006) Health benefits of physical activity: the evidence. CMAJ 174(6):801–809. doi:10.1503/cmaj.051351
Ware JE, Gandek B (1998) Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J Clin Epidemiol 51(11):903–912. doi:10.1016/s0895-4356(98)00081-x
Wemme KM, Rosvall M (2005) Work related and non-work related stress in relation to low leisure time physical activity in a Swedish population. J Epidemiol Commun Health 59(5):377–379
Acknowledgments
We would like to thank Eva Bergsten for assistance in the data collection. Göran Sandström is acknowledged for excellent engineering and data processing, and Tomas Ersson is acknowledged for performing the physical examinations. Judith Gold is acknowledged for providing valuable comments on the manuscript.
Conflict of interest
The authors declare that they have no conflict of interest, in accordance with IAOEH guidelines.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hallman, D.M., Ekman, A.H. & Lyskov, E. Changes in physical activity and heart rate variability in chronic neck–shoulder pain: monitoring during work and leisure time. Int Arch Occup Environ Health 87, 735–744 (2014). https://doi.org/10.1007/s00420-013-0917-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-013-0917-2