
Abstract
Purpose
Due to increasing usage of chemicals in various industries, occupational exposure of women with these materials is unavoidable. Nowadays, some studies indicate adverse effects of exposure to these chemicals, especially organic solvents on the reproductive system of females. This study aimed to assess the relationship between spontaneous abortion and occupational exposure to organic solvents mixture in pharmaceutical industry.
Methods
This study was carried out in a pharmaceutical factory located in the suburb of Tehran in 2010. During the study, married women who were working in the factory laboratory units and had exposure to mixed organic solvents were compared with married women who were working in the packing units of the factory without occupational exposure to organic solvents in terms of spontaneous abortion frequency and duration of pregnancy using statistical methods.
Results
In this study, the frequency of spontaneous abortion in employees with and without exposure to organic solvents mixture was 10.7 and 2.9% respectively. This study showed that even after adjustment for confounding factors, there was a significant correlation between spontaneous abortion and occupational exposure to organic solvents mixture and this correlation increased with increasing levels of exposure to organic solvents. Also, a significant correlation was observed between occupational exposure to mixed organic solvents and waiting time to become pregnant (TTP). Furthermore, this study showed that even after adjustment for confounding variables, shift workers were significantly more affected by spontaneous abortion compared to daytime workers (P < 0.001). Also, in our study, synergistic effect between shift working and occupational exposure to organic solvents mixture on spontaneous abortion was seen.
Conclusions
According to the results of this study, since there is probability of spontaneous abortion resulting from occupational exposure to various chemicals including organic solvents, recommendation to review the status of occupational exposure of workers can be helpful in improving fertility consultations and reproductive health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Infertility is one of the important problems of human life that can lead in many cases to the abandonment of couples and problems in social life (Khayata et al. 2003). Female reproductive system is vulnerable in persistent exposure to chemicals (Kumar 2004). Considering the global spread of chemicals in industry, occupational exposure of females to these chemicals is a major risk for their fertility ability. In the recent decade, evidence regarding destructive effects of chronic occupational exposure to chemicals on female reproductive system and pregnancy outcomes has revealed (Kumar 2004).
According to some studies in industrialized countries, infertility problem has increased between 8 and 15% in comparison to two decades ago that in part is attributable to the exposure of female workers to chemicals (Runnebaum et al. 1997). On the other hand, the number of female work force is growing throughout the world and large percentages of them are in childbearing age (Thulstrup and Bonde 2006). The number of female employees in the US reached from 30 million in 1970 to 50 million in 1990 and the number of working women 20–44 years was estimated 35 million in this country (Windham and Osorio 2007).
More than half of women during their employment period are involved in reproductive issues (Zenz 1994). Therefore, attention to reproductive disorders caused by occupational exposure is very important (Thulstrup and Bonde 2006). Several studies about the harmful effects of exposure to chemicals on pregnancy outcome have been done (Nilsson et al. 2005; Virginia et al. 2003). One of the reasons for spontaneous abortion is occupational exposure of female workers to organic solvents (Kumar 2004). Regarding the lipid solubility of organic solvents, they can pass through the placenta and can reach the fetus and induce harmful effect (Kumar 2004). Large numbers of female workers who are in reproductive age have occupational contact with organic solvents (Khattak et al. 1999).
According to the estimates of National Institute of Occupational Safety and Health (NIOSH), 9.8 million workers in the US had exposure to organic solvents in the first half of the 1970s. In the 1980s, about 400,000 workers in Denmark (15% of this country workforce) had daily exposure to solvents (Lundberg et al. 2005).
The effect of occupational exposure to organic solvents on spontaneous abortion has been studied in previous articles but the results are controversial. In a study which was done in 1995 in shoe making industry, it was reported that the frequency of spontaneous abortion was higher in solvent-exposed workers that non-exposed group (Sallmen et al. 1995). Also, the results of Agnesi et al. (2003) study showed that occupational exposure to high concentrations of organic solvents increases the frequency of spontaneous abortion. In another study by Bukowski (2001), the effects of occupational exposure to toluene on the reproductive system were studied. The results of this study showed that the frequency of spontaneous abortion in solvent-exposed workers was higher than non-exposed group.
Another study which was done by Xu et al. (1998), in a petrochemical complex in China, its results indicate an increased risk of spontaneous abortion in female workers who had occupational exposure to benzene, gasoline and hydrogen sulfide. The results of Lindbohm et al. (1990), study in Finland showed that female workers with occupational exposure to organic solvents (aliphatic and aromatic hydrocarbons) experienced spontaneous abortion 2.2 times more than non-exposed group (P < 0.05). In Taskinen et al. (1999), study increased frequency of spontaneous abortion in the laboratory workers with occupational exposure to formaldehyde, xylene and toluene was reported comparing those who did not have exposure (P < 0.05). However, in some studies these results were not confirmed. A study performed in the Netherlands showed that there was no statistically significant difference regarding spontaneous abortion between the painters who had occupational exposure to organic solvents compared to those who did not have (P > 0.05; Hooiveld et al. 2006). Also in the study of Zhu et al. (2006), 1,025 laboratory workers were compared with 8,037 female teachers regarding spontaneous abortion. The results showed that the frequency of spontaneous abortion did not differ significantly with that of teachers (P > 0.05).
Pharmaceutical industry is one of the important industries whose personnel commonly have occupational exposure to organic solvents mixture. Frequent numbers of personnel are employed in pharmaceutical factories. In 2004, there were around 65 pharmaceutical companies in Iran with 20 of them considered as large ones (Cheraghali 2006). In Taskinen et al. (1986) study in Finland about pharmaceutical industry, a significant increase was observed with respect to spontaneous abortion in personnel who had exposure to chemicals than control group (P < 0.05). In another study which was done on the laboratory staff in the pharmaceutical industry in Sweden, an increased risk of spontaneous abortion in this occupational group was observed in comparison to other occupational groups (P < 0.05; Hansson et al. 1980).
The aim of this study was to evaluate the correlation between spontaneous abortion and occupational exposure to organic solvents mixture in pharmaceutical industry.
Methods
Study design and subjects
This study was performed in a pharmaceutical factory located in the suburb of Tehran in 2010. Exposure group consisted of married women employed in laboratory units of the factory who had occupational exposure to organic solvents mixture. Non-exposure group included married women who were working at packing units of this factory who did not have exposure to organic solvents. All female workers who were married and were in reproductive age (20–40 years) and were employed in five laboratory units (with exposure to organic solvents) and two packing units of the factory (no exposure to organic solvents) who had at least 1 year work experience and had history of the first pregnancy during employment in this pharmaceutical company were included in the study, In other words, Our study population included women who achieved pregnancy for the first time while employed at the Pharmaceutical Company.
For all studied individuals, the required information such as demographic data, medical and occupational records were extracted using direct interviews and were documented in a questionnaire that was designed for this study. Information in the questionnaire included age, educational level, weight, height, nutritional status, smoking habit, medication usage, work shifts, age at the time of pregnancy, waiting time to become pregnant (TTP), status and history of pregnancy (its number and time and outcome), duration of exposure to organic solvents in the current job and the study exclusion criteria. Also, some information about medical status of the subjects during their pregnancy period was gathered using medical records at the time of pregnancy.
The exclusion criteria were history of spontaneous abortion before the being employed at the current job, age of spontaneous abortion being less than 20 or more than 35 years, uterine diseases (Leiomyoma, Asherman’s syndrome, premature cervical dilatation,…), history of endocrine system diseases (progesterone deficit, polycystic ovarian syndrome, thyroid disorders, diabetes mellitus,…), history of genetic diseases in the family, history of major trauma to the abdomen during pregnancy, chronic systemic disease (hypertension, immunologic and hematologic diseases,…), occupational exposure to organic solvents in the husband, history of prior exposure to organic solvents in former job or in a second one, history of any recreational exposure to organic solvents, occupational exposure to pesticides and metal fumes.
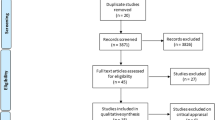
Three-hundred-one and 315 women were working in this factory at laboratory units and the packing units, respectively. Of this, 205 workers in laboratory units and 201 workers in packing units met the inclusion criteria. In exposed group 105 workers were excluded for the following reasons: age less than 20 years (n = 3), age more than 40 years (n = 55), history of spontaneous abortion in previous jobs (n = 3), uterine diseases (n = 1), history of endocrine diseases (n = 28), chronic systemic disease (n = 12) and occupational exposure to organic solvents in the husband (n = 3). Also in non-exposed group 114 workers were excluded for the following reasons: age less than 20 years (n = 5), age more than 40 years (n = 49), history of spontaneous abortion in previous jobs (n = 3), uterine diseases (n = 3), history of endocrine diseases (n = 34), chronic systemic disease (n = 18) and occupational exposure to organic solvents in the husband (n = 2). These two groups were compared in terms of the frequency of spontaneous abortion and waiting time to become pregnant (TTP) during their job period. All workers participated voluntarily in this study and signed informed consent form. This study was approved by the Ethics Committee of Tehran University of Medical Sciences.
Outcome measures
We used time to pregnancy (TTP) as a measure of fertility (Sallmen et al. 2008). Time to pregnancy was defined as the period of unprotected intercourse leading to a clinically detected pregnancy (Hooiveld et al. 2006). TTP refers to the months that the women required to become pregnant. For detection of time to pregnancy, the subjects were asked: “did you become pregnant during the first menstrual cycle when not using contraception? During the second?” If the pregnancy started later, the understudy women were asked to report how many months did it take to get pregnant? The cut point for prolonged TTP was 12 months (Taskinen et al. 1999). A spontaneous abortion was defined as a pregnancy that ended before 20 weeks of gestation (Hooiveld et al. 2006). For detection of spontaneous abortion, the subjects were asked: “Did you get pregnant during employment period in recent job?” If yes: “what was the pregnancy outcome?” A normal birth or miscarriage? If miscarriage was occurred: “in which weeks of the pregnancy period it was occurred?” also all founded cases of spontaneous abortion was confirmed by medical records.
Day time work was defined as fixed daytime. Shift work was defined as all types of shift working except fixed daytime working including fixed evening, fixed night, rotating shift (Zhu et al. 2004b)
Environmental monitoring
In this study, measurement of all solvents present in the work environment was performed by the occupational hygienist team of the factory. The details are as follows: Environmental measurement of organic solvents present in the workplace was performed at the breathing zone. Air samples were collected on charcoal tubes with constant flow (100 ml/min) pumps (SKC 226-01) for laboratory units and packing units. Air monitoring was performed continuously during all working hours. Subsequently, gas chromatography was used to analyze the samples and the average concentration of each solvent was identified.
The results of environmental monitoring showed that the solvents present in all five laboratory units of the factory were formaldehyde, phenol, N-hexane, and chloroform. Mean concentration of the organic solvents in laboratory units for formaldehyde, phenol, N-hexane, and chloroform were 0.01, 0.5, 20.7, 3.2 ppm (part per million), respectively.
The occupational exposure of the women to organic solvents was evaluated according to the American Conference of Industrial Hygienists (ACGIH) equation (American Conference of Governmental Industrial Hygienists 2008). The following equation was used to assess the permitted limit of the mixture of organic solvents.
where Em is the equivalent exposure for the mixture of organic solvents, C is the mean concentration of organic solvents in the air of the environment, and L is the exposure limit for the organic solvents. After measuring the mean concentration of each solvent and replacing it in the equation above, values of Em larger than 1 indicate that the concentration of the mixture of organic solvents in the work environment is higher than the threshold limit values. In laboratory units, the Em ranged from 0.549 to 0.932 with a median value of 0.867, indicating that the concentration of the mixture of organic solvents in the laboratory units was in the permitted range. Also we divided the exposed women into two groups: a low exposure group, defined as an Em of 0.549–0.867, and a high exposure group, defined as an Em > 0.867.
In addition, the organic solvents were measured in packing units, yielding zero or negligible concentrations.
Statistical analysis
Mean, standard deviation (SD) and range of quantitative variables were calculated. The t-test was used for comparing these variables among the groups. The Chi-square test was used for comparing the qualitative variables. Moreover, for the purpose of modifying the confounder factors and evaluating the relationship between exposure to organic solvents and spontaneous abortion more precisely, the logistic regression method was used. Biological interaction between two variables was calculated using the synergic index (SI) score based on the ratio of the combined effects to the sum of the separate effects of two variables according to Rothman and Greenland (1998). An SI score = 1 indicates a departure from an additive effect between two variables. A significant SI score above 1 indicates that synergy exists between two variables. We analyzed how exposure to organic solvents and shift work alone or in combination were associated with spontaneous abortion. P values less than 0.05 were considered as statistically significant. The results of statistical analysis are expressed as odds ratio (OR) with 95% confidence intervals (95% CI). All the mentioned calculations were performed using SPSS 15 software.
Results
In this study, the researchers examined 406 women in reproductive age, working in pharmaceutical industry. 205 subjects (50.5%) were in exposure group (laboratory staff) and 201 patients (49.5%) were in non-exposure group (packing unit staff). In all studies subjects, mean age was 31.7 years (range = 22–40 years). Mean work experience was 8.9 years (range = 1–24 years). Mean body mass index (BMI) was 23.8 kg/m2 (range = 17.21–38.05). In each group only one person was cigarette smoker. Also, 73.6% of the workers were daytime workers and 26.4% of them were shift workers. In general, 28 cases (6.9%) had experienced spontaneous abortion during pregnancy.
Table 1 presents the comparison of exposed vs. non-exposed group regarding the quantitative variables. As shown, the two groups were similar regarding age, pregnancy age, work experience and BMI (P > 0.05). Also, the comparison of qualitative variables between the two groups is presented in Table 2. This table depicts that there was no significant difference between groups in terms of educational level, shift working, and ergonomic factors (including “standing duration” and “heavy lifting” during the work; P > 0.05).
Spontaneous abortion
The frequency of spontaneous abortion in the exposed group (laboratory workers) was significantly higher than the non-exposed group (workers in packing units); (OR = 3.9, 95% CI: 1.54–9.85 and P < 0.05; Table 3) in a way that the risk of spontaneous abortion in expose group was 3.9 times higher than non-exposed group.
We divided all spontaneous abortion cases based on etiology to 3 categories of less than 6 weeks, between the 6th and 12th weeks and between the 12th and 20th weeks. In exposed group the numbers of Spontaneous Abortion cases were 7, 13 and 2 cases respectively and these numbers for non-exposed group were 3, 2 and 1 case respectively.
Also, the frequency of spontaneous abortion in shift workers (12.1%) was higher than daytime workers (5.01%; OR 2.68, 95% CI: 1.20–5.71; P < 0.024).
Logistic regression analysis was used for more exact evaluation of relationship between exposure to organic solvents and the frequency of spontaneous abortion (Table 4). It was observed that even after adjustments for age at pregnancy, work experience and shift working, there was a significant relationship between the exposure to organic solvents and the occurrence of spontaneous abortion (P < 0.05). With increasing concentration of organic solvent exposure, the likelihood of spontaneous abortion increased. In other words a dose–response relationship was observed for spontaneous abortion with odds ratios increasing from 5.21 in the low exposed group to 7.70 in the high exposed groups. Also, there was a significant relationship between age at pregnancy, work experience and shift working with spontaneous abortion (P < 0.05).
The estimated synergic index (SI) was significantly greater than 1. A significant SI was found between shift work and exposure to organic solvents (SI = 2.85). When analyzed alone or in combination, shift work and exposure to organic solvents were positively associated with spontaneous abortion (P < 0.05). Odds ratios for isolated and combined factors of shift work and exposure to organic solvents on spontaneous abortion are shown in Table 5. It was observed that for combined factors, the estimated effect on spontaneous abortion was higher than the sum of the effects from each isolated variable.
Time to pregnancy
The average waiting time to get pregnant (TTP), in exposure group was significantly higher than non-exposure group (P < 0.001; Table 1). The number of women whose mean waiting time for becoming pregnant (TTP) was 12 months or more was significantly higher in exposed group than non-exposed group (OR = 2.2, 95% CI: 1.26–4.30 and P < 0.05; Table 3).
Also logistic regression analysis was done to evaluate the relationship between exposure to organic solvents and time to pregnancy period increasing (Table 6). For this purpose Time to pregnancy period was divided into 2 categories of TTP ≥ 12 month and TTP < 12 month. With increasing concentration of organic solvent exposure, the likelihood of prolonged TTP increased. In other words, after adjustment for confounding factors, the risk of prolonged TTP increased with exposure level from 2.76 in the low exposure group to 4.48 in the high exposure group.
Discussion
Occupational exposure to various chemicals can have adverse effects on pregnancy outcome (Petrelli et al. 2003). In pharmaceutical industry, laboratory employees are exposed to a variety of chemicals and these substances can have adverse effects on the reproductive system (Zhu et al. 2006).
Spontaneous abortion
Our results showed that occupational exposure to a mixture of organic solvents significantly increases frequency of spontaneous abortion. In this study, we considered many confounding factors including age at the time of pregnancy, BMI, work experience, and ergonomic factors. In some studies, high physical demands of the job, different types of inappropriate working postures (prolonged sitting and standing) and heavy lifting considered as probable causes of increased rate of spontaneous abortion (Taskinen et al. 1986). However, results of some studies have not confirmed these findings (Marbury et al. 1984).
The results of a study that was conducted in Canada shows that workers with lifting more than 10 kg of weight, had an increased frequency of spontaneous abortion (23.6%) was seen in comparison to other workers (17.7%; McDonald et al. 1983). In a study on women who worked in laboratory and had history of heavy lifting, a slight increase in spontaneous abortion was seen, though not significant (RR = 1.36, CI = 0.91–2.02; Axelsson et al. 1984). In the current study, exposed group did not differ from non-exposed group in terms of ergonomic factors (P > 0.05). Also in our study the frequency of spontaneous abortion in exposed group was 10.7% which is compatible with the results of Elliott et al. (1999).
In previous studies, the detrimental effects of occupational exposure to organic solvents on the reproductive system have been described (Chen et al. 2002; Smith et al. 1997). Previous studies have shown the relationship between occupational exposure to different concentration levels of organic solvents and spontaneous abortion (McMartin et al. 1998; Wennborg et al. 2002). In our study, even after adjustment for confounding factors, a significant association was seen between spontaneous abortion rate and occupational exposure to organic solvents mixture at high and low concentrations (P < 0.05). Also, the ORs for spontaneous abortion were higher among women workers with high levels of exposure to organic solvents. The findings agree with the findings of Agnesi et al. (1997).
Since workers in work environment may have exposure to a mixture of organic solvents, it is difficult to attribute spontaneous abortion to a specific solvent. In our study, formaldehyde, phenol and chloroform were the major component of the organic solvent mixture. In some studies, the association between occupational exposure to chloroform and spontaneous abortion has been reported (Lindbohm et al. 1992).
In Axelsson et al. (1984), study, an increased probability of spontaneous abortion was seen amongst laboratory workers who had occupational exposure to chloroform. However, in a study in Sweden by Wennborg et al. (2000) on 856 laboratory workers who had occupational exposure to chloroform, no significant difference was observed regarding spontaneous abortion between exposed group vs. non-exposed group (P > 0.05). In previous studies, the relationship between occupational exposure to formaldehyde and spontaneous abortion has been reported (Taskinen et al. 1999). The mechanism of spontaneous abortion due to occupational exposure to formaldehyde is not clear. Formaldehyde like most forms of organic solvents passes through the placenta and causes adverse effect on the fetus. Accompany between exposure to organic solvent and salpingo-ovaritis has been reported in previous studies (Taskinen et al. 1999). Smith et al. (1997), found an association between exposure to organic solvents, and tubal infertility. Infection is a common cause for tubal infertility, and hypothetically, external agents might modify the effects of the infectious agents in the inner genitalia (Taskinen et al. 1999).
In our study, even after adjustment for confounding variables, female shift workers had significantly more spontaneous abortions than daytime workers (P < 0.001). Also, a synergistic effect on spontaneous abortion was seen between shift working and occupational exposure to organic solvent mixtures (SI = 2.85). Information on shift work, in developing countries, is very limited. According to ILO statistics, about 15–30% of working population in developing countries are shift workers (Dumont 1985).
The results of previous studies indicate adverse effects of shift working on pregnancy outcomes (Axelsson et al. 1996; Zhu et al. 2004a). However, some studies have not confirmed the aforementioned findings (Eskenazi et al. 1994; Fenster et al. 1997). In Li et al. (2002), study, a significant correlation between nighttime working and spontaneous abortion was found. Whelan et al. (2007), study results showed that nighttime working and increased working hours causes increased likelihood of spontaneous abortion. The Mechanism of adverse effects of shift working on pregnancy outcomes, including spontaneous abortion is not clear. Hormonal disturbance, sleep rhythm disorders and abnormal circadian rhythm that cause alterations and disturbance in cellular immunity balance which is necessary in maintaining pregnancy is a possibility (Akerstedt 1990). Also, shift working by causing physiologic dysfunction and impairment in circadian rhythm decreases the production of melatonin (Whelan et al. 2007). Hansen (2001) study showed that nighttime working causes extensive changes in the amount and time of melatonin production. Reduced production of melatonin causes changes in the concentration level of other hormones such as estrogen and progesterone which are essential for pregnancy (Whelan et al. 2007).
Time to pregnancy
In our study mean time to achieve pregnancy (TTP) in exposed and non exposed groups were 9.55 and 7.52 months respectively and a significant relationship between occupational exposure to mixed organic solvents and increased waiting time to become pregnant (TTP) was seen which is in agreement with the results of Sallmen et al. (2003), study. On the other hand the mean time to achieve pregnancy (TTP) in exposed and non exposed groups derived from this study are too long in comparison of other similar studies (Sallmen et al. 2008). This difference may be due to inappropriate and inadequate educations about sexual habits and sexual health in Iranian working population. Also based on the results of a similar study, Prolonged TTP indicates reproductive loss at any of several different stages, including gametogenesis, transport of gametes in both male and female reproductive tracts, fertilization, migration of zygote to uterus, implantation, and early survival of the conceptus (Bretveld et al. 2008).
Also a dose–response relationship was observed for increased TTP with odds ratios increasing from 2.76 in the low exposed group to 4.48 in the high exposed groups. Our findings are in agreement with previous studies (Chen et al. 2002; Sallmen et al. 2008; Taskinen et al. 1999).
The study limitations were the difficulty in identifying and recognition of spontaneous abortion especially in early stages. Also in this study, because of some limitations, the study design was retrospective and results of retrospective studies on spontaneous abortion can be influenced by recall bias. Therefore, it is recommended that prospective studies about evaluation of correlation between occupational exposure to mixture of organic solvents and spontaneous abortion should be done in case of the confirmation of our results; spontaneous abortion should be prevented by limited occupational exposure with organic solvents mixture.
Conclusions
This study provides limited support for the hypothesis that exposure to organic solvents is associated with decreased fertility. Also our findings provide further evidence that exposure to organic solvents possibly leading to prolonged time-to-pregnancy.
Since spontaneous abortion due to occupational exposure to organic solvents can be prevented with avoidance of exposure, before any invasive measurement to resolve infertility, occupational exposure of workers should be assessed and unnecessary measures such as surgery and expensive medical treatments should not be initiated.
Generally, since there is probability of spontaneous abortion caused by occupational hazards, it is possible to discriminate occupational cases from idiopathic ones by reviewing occupational exposure of workers to prevent from imposing additional health costs to workers and a step towards improvement in occupational health of workers community.
References
Agnesi R, Valentini F, Mastrangelo G (1997) Risk of spontaneous abortion and maternal exposure to organic solvents in the shoe industry. Int Arch Occup Environ Health 69:311–316
Agnesi R, Valentini F, Meneghetti M, Fedeli U, Fadda E, Tartari M, Mastrangelo G (2003) Changes in risk factors for spontaneous abortion in an area with high concentrations of shoe manufacture after a preventive intervention. G Ital Med Lav Ergon 25:79–80
Akerstedt T (1990) Psychological and psychophysiological effects of shift work. Scand J Work Environ Health 16:67–73
American Conference of Governmental Industrial Hygienists (2008) ACGIH TLVs and BEIs for chemicals substances, physical agents and biological exposure indices. ACGIH, Cincinnati
Axelsson G, Luitz C, Rylander R (1984) Exposure to solvents and outcome of pregnancy in university laboratory employees. Br J Ind Med 41:305–312
Axelsson G, Ahlborg G, Bodin L (1996) Shift work, nitrous oxide exposure, and spontaneous abortion among Swedish midwives. Occup Environ Med 53:374–378
Bretveld R, Hooiveld M, Zielhuis G, Pellegrino A, van Rooij I, Roeleveld N (2008) Reproductive disorders among male and female greenhouse workers. Reprod Toxicol 25:107–114
Bukowski J (2001) Review of the epidemiological evidence relating toluene to reproductive outcomes. Regul Toxicol Pharmacol 33:147–156
Chen P, Hsieh G, Wang J, Cheng T (2002) Prolonged time to pregnancy in female workers exposed to glycol ethers in semiconductor manufacturing. Epidemiology 13:191–196
Cheraghali A (2006) Iran pharmaceutical market (editorial). Iran J Pharm Res 1:1–7
Dumont C (1985) Shiftwork in Asian developing countries: an overview. In: International Labour Office (ed). Shiftwork related issues in Asian countries. ILO Publications, Geneva, pp 24–42
Elliott R, Jones J, McElvenny D, Pennington M, Northage C, Clegg T, Clarke S, Hodgson J, Osman J (1999) Spontaneous abortion in the British semiconductor industry: An HSE investigation. Am J Ind Med 36:557–572
Eskenazi B, Fenster L, Wight S, English P, Windham G, Swan S (1994) Physical exertion as a risk factor for spontaneous abortion. Epidemiology 5:6–13
Fenster L, Hubbard A, Windham G, Waller K, Swan S (1997) A prospective study of work-related physical exertion and spontaneous abortion. Epidemiology 8:66–74
Hansen J (2001) Increased breast cancer risk among women who work predominantly at night. Epidemiology 12:74–77
Hansson E, Jansa S, Wande H, Kallen B, Ostlund E (1980) Pregnancy outcome for women working in laboratories in some of the pharmaceutical industries in Sweden. Scand J Work Environ Health 6:131–134
Hooiveld M, Haveman W, Roskes K, Bretveld R, Burstyn I, Roeleveld N (2006) Adverse reproductive outcomes among male painters with occupational exposure to organic solvents. Occup Environ Med 63:538–544
Khattak S, K-Moghtader G, McMartin K, Barrera M, Kennedy D, Koren G (1999) Pregnancy outcome following gestational exposure to organic solvents: a prospective controlled study. JAMA 28:1106–1109
Khayata G, Rizk D, Hasan M, Ghazal-Aswad S, Asaad M (2003) Factors influencing the quality of life of infertile women in United Arab Emirates. Int J Gynaecol Obstet 80:183–188
Kumar S (2004) Occupational exposure associated with reproductive dysfunction. J Occup Health 46:1–19
Li P, Fang Z, Pan X, Wang L, Xu X (2002). The impact of night work near the day of ovulation on outcome of pregnancy. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 20:369–371
Lindbohm M, Taskinen H, Sallman M, Hemminki K (1990) Spontaneous abortions among women exposed to organic solvents. Am J Ind Med 17:449–463
Lindbohm M, Taskinen H, Kyyronen P, Sallmen M, Anttila A, Hemminki K (1992) Effects of parental occupational exposure to solvents and lead on spontaneous abortion. Scand J Work Environ Health 18:37–39
Lundberg I, Hogstedt C, Linden C, Nise G (2005) Organic solvents and related compounds. In: Rosenstock L, Cullen A, Brodkin A, Redlich (eds) Textbook of clinical occupational and environmental medicine, 2nd edn. Elsevier, China, p 991
Marbury M, Linn S, Monson R, Wegman D, Schoenbaum S, Stubblefield P (1984) Work and pregnancy. J Occup Med 26:415–421
McDonald A, Cherry N, Commandeur C, Delorme C, Lavoie J, Marquis S (1983) Work and pregnancy in Montreal-preliminary findings. Third Conference on epidemiology in occupational health, Singapore, 28–30 September
McMartin K, Chu M, Kopecky E, Einarson T, Koren G (1998) Pregnancy outcome following maternal organic solvent exposure: a meta-analysis of epidemiologic studies. Am J Ind Med 34:288–292
Nilsson R, Bjordal C, Andersson M, Bjordal J, Nyberg A, Welin B, Willman A (2005) Health risks and occupational exposure to volatile anaesthetics a review with a systematic approach. Clin Nurs 14:173–186
Petrelli G, Figa-Talamanca I, Lauria L, Mantovani A (2003) Spontaneous abortion in spouses of greenhouse workers exposed to pesticides. Environ Health Prev Med 8:77–81
Rothman K, Greenland S (1998) Modern epidemiology. Lippincott-Raven, Philadelphia
Runnebaum B, Rabe T, Sillem M, Eggert-Kruse W (1997) Infertility. In: Runnebaum B, Rabe T (eds) Gynecological endocrinology and reproductive medicine, 1st edn. Springer, New York, pp 107–164
Sallmen M, Lindbohm ML, Kyyronen P, Nykyri E, Anttila A, Taskinen H, Hemminki K (1995) Reduced fertility among women exposed to organic solvents. Am J Ind Med 27:699–713
Sallmen M, Liesivuori J, Taskinen H, Lindbohm M, Anttila A, Aalto L, Hemminki K (2003) Time to pregnancy among the wives of Finnish greenhouse workers. Scand J Work Environ Health 29:85–93
Sallmen M, Neto M, Mayan O (2008) Reduced fertility among shoe manufacturing workers. Occup Environ Med 65:518–524
Smith E, Hammonds-Ehlers M, Clark M, Kirchner H, Fuortes L (1997) Occupational exposures and risk of female infertility. J Occup Environ Med 39:138–147
Taskinen H, Lindbohm M, Hemminki K (1986) Spontaneous abortions among women working in the pharmaceutical industry. Brit J Ind Med 43:199–205
Taskinen H, Kyyronen P, Sallmen M, Virtanen S, Liukkonen T, Huida O, Lindbohm M, Anttila A (1999) Reduced fertility among female wood workers exposed to formaldehyde. Am J Ind Med 36:206–212
Thulstrup A, Bonde J (2006) Maternal occupational exposure and risk of specific birth defects. Occup Med 56:532–543
Virginia T, Gauger T, Voepel L, Rubin P, Kostrzewa A, Tait A (2003) A survey of obstetric complications and pregnancy outcomes in paediatric and nonpaediatric anaesthesiologists. Pediatr Anaesth 13:490–495
Wennborg H, Bodin L, Vainio H, Axelsson G (2000) Pregnancy outcome of personnel in Swedish biomedical research laboratories. J Occup Environ Med 42:438–446
Wennborg H, Bonde JP, Stenbeck M, Olsen J (2002) Adverse reproduction outcomes among employees working in biomedical research laboratories. Scand J Work Environ Health 28:5–11
Whelan E, Lawson C, Grajewski B, Hibert E, Spiegelman D, Rich-Edwards J (2007) Work schedule during pregnancy and spontaneous abortion. Epidemiology 18:350–355
Windham GC, Osorio AM (2007) Female reproductive toxicology. In: LaDou J (ed) Current occupational & environmental medicine, 4th edn. Mc Graw-Hill Companies, USA, p 385
Xu X, Cho S, Sammel M, You L, Cui S, Huang Y, Ma G, Padungtod C, Pothier L, Niu T, Christiani D, Smith T, Ryan L, Wang L (1998) Association of petrochemical exposure with spontaneous abortion. Occup Environ Med 55:31–36
Zenz C (1994) Reproductive toxicology and occupational exposure. In: Zenz C, Dickerson O, Bruce O, Horvath JR, Edward P (eds) Occupational medicine, 3rd edn. Mosby, USA, pp 836–839
Zhu JL, Hjollund NH, Andersen AM, Olsen J (2004a) Shift work, job stress, and late fetal loss: the national birth cohort in Denmark. J Occup Environ Med 46:1144–1149
Zhu J, Hjollund N, Olsen J (2004b) Shift work, duration of pregnancy, and birth weight: the National Birth Cohort in Denmark. Am J Obstet Gynecol 19:285–291
Zhu J, Knudsen L, Andersen A, Hjollund N, Olsen J (2006) Laboratory work and pregnancy outcomes: a study within the National Birth Cohort in Denmark. Occup Environ Med 63:53–58
Acknowledgments
This study was conducted with support from the Deputy for Research at Tehran University of Medical Sciences. The authors wish to express their gratitude to the sincere contributions of the Deputy, particularly the research expert Ms. Azvan. Additionally, we are grateful to the noble workers and personnel of the pharmaceutical factory.
Conflicts of interest
we declare that we do not have any competing interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Attarchi, M.S., Ashouri, M., Labbafinejad, Y. et al. Assessment of time to pregnancy and spontaneous abortion status following occupational exposure to organic solvents mixture. Int Arch Occup Environ Health 85, 295–303 (2012). https://doi.org/10.1007/s00420-011-0666-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-011-0666-z