
Abstract
Purpose
To develop a sensitive and reproducible method for urinary beryllium and to use this method to establish levels in workers at an aluminium smelter and in unexposed persons.
Methods
A method was developed for urinary beryllium using a Thermo ICP-MS Series 1, which was used to determine beryllium concentrations in urine from 62 people with no known occupational exposure to beryllium and 167 workers with potential exposure to beryllium at an aluminium smelter, where beryllium exists as an impurity in the bauxite ore.
Results
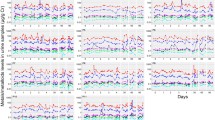
The analytical method has a detection limit (based on three times the background equivalent concentration of the blank) for beryllium in urine of 6 ng/L. The mean and 90th percentiles of urinary beryllium for workers were 19.5 and 42.0 ng/L and compared with 11.6 and 20.0 ng/L in people not occupationally exposed to beryllium. Statistical analysis using mixed effects models showed that workers had 47% (in 135 paired samples) higher levels of urinary beryllium at the end of the working week compared to the start of week and that the workers who smoked also had significantly higher levels of urinary beryllium compared to those that did not smoke. There was also a statistically significant difference between workers and controls in urinary beryllium concentrations not corrected for creatinine.
Conclusions
A sensitive and reliable analytical method was developed for urinary beryllium by ICP-MS. The workers in this study were exposed to beryllium at very low levels.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Beryllium and beryllium compounds are classified by International Agency for Research on Cancer as carcinogenic (class 1) to humans (IARC 1997). The most noticeable adverse health effects from beryllium exposure are those affecting the respiratory system. Acute exposures to high levels of beryllium can cause inflammation of the entire respiratory tract and at lower levels exposure to airborne beryllium particulate can cause an immune system response known as beryllium sensitisation. Sensitised individuals can go on to develop chronic beryllium disease, a debilitating and potentially fatal lung disease characterised by lesions in the lungs known as granulomas (Brisson 2009; Maier et al. 2006). High levels of beryllium exposure are also considered a potential lung cancer risk (Hollins et al. 2009). Effects on the lymph nodes, skin and other target organs have also been reported with the majority of these presenting as contact dermatitis and skin lesions (Maier et al. 2006; Goyer and Clarkson 2001).
Beryllium is a metal with a few specific industrial uses and is found at low concentrations in the Earth’s crust. Since the early twentieth century, it has been produced and used in a variety of applications both as the metal, in alloys, and as its oxide. Beryllium can also be released into the environment from coal combustion. Beryllium is an important industrial metal because it is lighter than aluminium and six times stronger than steel. Major uses of beryllium are as alloys and are used as a structural material for high performance aircraft, aircraft engines, communication satellites, turbine rotor blades, ball bearings, tubing for oil and gas drilling, tools and dies, jewellery, bicycle frames, dental appliances and in night vision systems. Beryllium metal is used in nuclear reactions, aircraft brake parts, spacecraft structures, navigation systems and X-ray windows and other special applications related to space optics, missile fuel and space vehicles (Maier et al. 2006; Rana 2008). Beryllium oxide is used in a variety of ceramic applications such as medical laser bores, integrated circuits, electronic heat sinks and insulators, gyroscopes and thermocouple tubing (Brisson 2009).
Occupational exposure to beryllium can occur during its extraction and uses. Beryllium is most often used as an alloy with copper, aluminium, magnesium or nickel, and the beryllium content of these alloys and its hazards may not always be obvious to workers generating dust and fumes. Recycling of electronics, computers, and scrap alloy to recover copper can also result in beryllium exposure for an unknown number of workers, many of whom may be unaware of the risks (Infante and Newman 2004). In 1990–3, it was estimated that there were 67,000 workers in the European Union exposed to beryllium and its compounds (Kauppinen et al. 2000).
The current UK Workplace Exposure Limit (WEL) and US Occupational Health and Safety Administration (OSHA) airborne limit for workplace beryllium is 2 μg/m3 (8 h time-weighted-average). This level was first recommended in 1949 by the U.S. Atomic Energy Commission and was adopted in 1956 (Madl et al. 2007). A number of studies have since established that an occupational exposure limit of 2 μg/m3 is not adequately protective because controlling beryllium inhalation exposure to comply with regulatory levels (2 μg/m3) does not appear to prevent cases of beryllium sensitisation and chronic beryllium disease (Madl et al. 2007; Day et al. 2007). In 2009, the American Conference of Governmental Industrial Hygienists (ACGIH) reduced the Threshold Limit Value (TLV) by a factor of 40–0.05 μg/m3 for beryllium over an 8-h shift, (ACGIH website http://www.acgih.org/store/ProductDetail.cfm?id=758). The majority of European airborne beryllium limits are currently set at 2 μg/m3 as in the United Kingdom.
Health surveillance/assessment for beryllium workers commonly involves tests to establish whether sensitisation has occurred, e.g. using beryllium lymphocyte proliferation tests in blood or bronchoalveolar lavage (Santo Tomas 2009; Thomas et al. 2009; Taiwo et al. 2008; Wegner et al. 2000). However, a measurement of exposure could aid improvements in workplace controls and prevent sensitisation occurring. While airborne beryllium levels via personal mounted samplers can be determined as part of routine occupational hygiene methods (Madl et al. 2007), routine biological monitoring to assess exposure has not been widely used. Air monitoring alone will not assess overall systemic beryllium exposures in workers as a result of other possible routes of exposure to be accounted for such as dermal and ingestion routes. The use of biological monitoring can assess the efficacy of respiratory and personal protective equipment and can also help identify individual work practices or habits. The biological monitoring methods published have mostly involved urine samples. It was found in a study in 1977 that more than 90% of inhaled or percutaneously incorporated beryllium is eliminated via urine (Zorn and Stiefel 1977; Stiefel et al. 1980). However, overall there are few publications measuring beryllium in urine because the concentrations are very low and until recently methods did not have sufficient specificity or sensitivity (Apostoli and Schaller 2001).
The UK’s Atomic Weapons Establishment in Cardiff fabricated beryllium until 1997 (Johnson et al. 2001); however, now there are no beryllium manufacturing plants in the United Kingdom. All beryllium currently used in the United Kingdom is imported either as the metal, the oxide or as an alloy. The work reported here describes the development and validation of a sensitive and specific method for beryllium in urine and its application in an aluminium smelter with potential exposure to beryllium as an impurity in bauxite ore. While bauxite is not a beryllium source for production purposes, aluminium smelter workers can be exposed to beryllium in pot emissions (Taiwo et al. 2008). Urine samples were taken from 167 aluminium smelter workers and 62 unexposed persons and the urinary beryllium determined using inductively coupled plasma mass spectrometry (ICP-MS) with optimised conditions.
Methods
Sample collection
All participating individuals provided informed consent, in accordance with HS(G) 167 (HSE 1997). Urine samples (n = 306) were collected from 167 workers at an aluminium production/recycling site. One hundred and thirty-five of these 167 workers provided both start of the week samples (pre) and end of the week samples (post). Workers provided information on male/female, non-smoker or smoker. Control samples were collected from 62 volunteers. Samples were analysed for creatinine on arrival and then frozen until analysed for beryllium.
Creatinine
Creatinine was determined in all urine samples using an automated alkaline picrate method (Jaffe 1886; Bonsnes 1945).
Analytical procedure
Aqueous beryllium standards (ICP-MS standard, BDH, Poole, UK) were made freshly each day; calibration range was 2–200 ng/L for six standards as shown in Table 1. The urine samples were defrosted at room temperature and then mixed on sample rollers for a minimum of 20 min. Urine samples were diluted 1 in 10 with a diluent made up of 1% v/v nitric acid (Romil) with internal standards yttrium and germanium (ICP-MS standards, BDH, Poole, UK) added at a concentration of 100 ng/L. All urine samples were analysed in duplicate.
External quality control samples ClinChek levels 1 and 2 (RECIPE Chemicals and Instruments, Munich, Germany) were used to determine accuracy of the method. External quality assurance samples from G-EQUAS (Friedrich-Alexander-University Erlangen-Nuremberg, Germany) were also used to validate the method. Internal quality control was prepared in urine sample from a single donor spiked at a concentration of 50 ng/L. The internal quality control urine sample was frozen in 20 mL aliquots in sterile 50-mL conical tubes with lids (Sarstedt, Leicester, UK) and treated in the same way as urine samples. QC samples were analysed at the start, end and after every ten samples for the duration of the analysis. The remaining blank and spiked samples were frozen at −20°C and analysed at a later date to allow the stability of beryllium in urine to be monitored. A 40 ng/L standard was run at the same intervals as the blank and spiked urine throughout each analysis.
Beryllium analyses
Analyses were carried out using an inductively coupled plasma mass spectrometer (ICP-MS) X series 1 (Thermo Fisher, Hemel Hempstead, UK). The instrument was used with direct nebulisation in normal mode using optimised conditions consisting of an HPi skimmer cone with a Xi sampler cone and a silver screen on the torch to improve the sensitivity for beryllium. The extraction voltage was typically −650 V, the Rf Power 1,350 W, focus voltage was 11 V, the nebuliser gas flow rate (using a Burgener Miramist nebuliser) was 0.87 L/min. Dwell times were 200 ms for 9Be and 20 ms for the internal standards 72Ge and 89Y, 100 sweeps were required per replicate and 3 replicates per sample. Instrument oxide levels were generally between 6 and 10% as measured by the140 Ce16O+/140Ce+ ratio.
Statistical analysis
In addition to calculating simple summary statistics, urinary beryllium levels in workers were analysed using linear mixed-effects models on the log-transformed scale. Fixed effects were used to model the effects of smoking and timing of samples and the correlation with urinary creatinine levels. The random worker effects are used to model other systematic differences between individuals, which are apparent with repeated measurements per individual. The model can be represented in the following form:
where Y i,j is the ith urinary beryllium concentration for the jth worker in sector, ③ is the overall mean (on a log scale), and β 1, β 2 and β 3 are fixed effects for log-transformed creatinine concentration, smoking and time of week, respectively. The random effects (δ j ) and within-worker errors (ε i, j ) were assumed normally distributed with mean zero and standard deviations ⑨bw and ⑨ww, respectively. As the proportion of urinary beryllium concentrations less than the limit of detection (LOD) was relatively modest (9.2% for workers and 3.2% for controls), a value of half LOD was substituted in their place. Thirteen results were excluded from the mixed effects analysis because the timing of the samples relative to the working week was unknown.
Results
Analytical method optimisation
The concentration of beryllium in urine is very low, and to maximise the beryllium sensitivity different cone assemblies in the ICP-MS were evaluated. It was found that using the Thermo Fisher standard sampler ‘Xi’ cone (now a Xt cone) with a Thermo Fisher ‘Hpi’ (now an Xs cone) skimmer cone maximised sensitivity. The ‘Hpi’ cone has more open geometry (a much shallower gradient) and so operates with a much higher extraction voltage (optimised at −650 V), which leads to increased sensitivity across the mass range (as more of the ion beam is collected at higher extraction voltages). The sensitivity was not increased further using an ‘Hpi’ sampler cone in addition to the ‘Hpi’ skimmer cone and so the standard ‘Xi’ sampler cone was used. Table 1 shows the increase in cones with the ‘Xi’ sampler/’Hpi’ skimmer formation compared to the normal set-up of Xi sampler and skimmer. At concentrations of 2 ng/L, a 25-fold increase in counts is observed and at concentrations of 40 ng/L the increase in counts is 28-fold. The counts in Table 1 also show that the background counts have increased but are still very low, at 10 counts per second (cps) for the blank. The overall increase in sensitivity gave better day-to-day stability for urinary beryllium analysis and allowed for the urine samples to be diluted by 1 in 10 and not 1 in 5, which also improved the long-term stability of the ICP-MS.
Quality of the analytical method
The beryllium measurement blank or background equivalent concentration (BEC) varied slightly on a daily basis and was between 0.1 and 0.6 ng/L. Therefore, the analytical method limit of detection was 2 ng/L based on three times the maximum BEC. The limit of quantification (based on ten times the maximum BEC) for the diluted urine beryllium analysis was 6 ng/L (0.7 nmol/L and approximately 0.08 μmol/mol creatinine.
For quality control, the in-house control urine blank and spiked urine samples were used on a day-to-day basis to be able to monitor the beryllium levels at lower concentrations between each analysis. The average blank urine (from the same donor) concentration (n = 125) was 7.2 ng/L (±5.7), and the average (n = 125) measured spiked concentration for the internal quality control sample was 54.9 (±8.4) ng/L for a 50 ng/L spike. An average recovery of 95.3% was observed for the spiked urine sample that was used in every analysis, based on 125 blank and 125 urine samples freshly spiked over 29 different analyses. The recovery of the spiked sample frozen was determined on the day of analysis and then reanalysed at a later date showed that after 7 weeks at −20°C there was a 90–95% recovery against the original spiked level of 50 ng/L and after 13 weeks at –20°C there was a 77–78% recovery against the original spiked level of 50 ng/L. Based on the 50 ng/L spiked internal quality control urine sample, the method had a within- and between-day variation coefficients of 15% and less than 10%, respectively.
The external certified reference material used throughout the study was Clinchek (RECIPE Chemicals and Instruments, Munich, Germany). The results based on ten replicates of the certified range and measured values were as follows: Level 1 certified range 35–87 ng/L mean measured value 70.6 ± 3.0 ng/L and Level 2 certified range 150–290 ng/L mean measured value 234.3 ± 10.6 ng/L.
A stability check consisting of a 40 ng/L standard was also run at the same frequency as the spiked urine samples and if drift was more than 20% throughout the analysis the run was not accepted. This method was also assessed externally by successful participation in the German External Quality Assessment Scheme (G-EQUAS) (Friedrich-Alexander-University Erlangen-Nuremberg, Germany). Since this method has been established the tested levels of urinary beryllium have varied from 19 to 999 ng/L in the G-EQUAS scheme.
The difference in the matrices between the aqueous standards and the 1 in 10 diluted urine samples was observed in the suppression of the internal standard counts in the urine samples. For yttrium there was on average a 40% suppression of counts, and for germanium there was on average a 20% suppression in the urine matrix. Each analysis was only accepted if the internal standard counts in aqueous samples at the start and end of the analyses had similar counts (permitted drift for both germanium and yttrium counts was less than 15%).
Urinary beryllium levels in workers and controls
The results from the all the samples analysed for urinary beryllium are presented in Table 2 both in measured units of ng/L (uncorrected) and in creatinine corrected units of μmol/mol creatinine. The results show that in the uncorrected units that the workers have significantly higher urinary beryllium levels with the mean concentrations for workers being 19.5 ng/L compared to 11.6 ng/L for controls (unpaired t test showed p < 0.01 for a difference in uncorrected values). However, the creatinine corrected values do not exhibit a similar difference (Table 2). The results in Table 2 have not discarded any of the results based on low (typically less than 3 mmol/L) or high (typically higher than 30 mmol/L) creatinine levels. Where data were below the LOD this has been substituted by 3 ng/L (half LOD), in total 28 workers samples and 2 controls samples were below the limit of detection of 6 ng/L.
Comparing the geometric standard deviations between the creatinine corrected and uncorrected values shows that there was greater variability in creatinine corrected results compared to uncorrected values. The fact that the workers’ urine beryllium results are significantly higher than the controls in the uncorrected data and that there is little difference in the corrected results suggests that the creatinine levels were higher in the workers than in the controls since the creatinine correction is simply the beryllium concentration in nmol/l divided by the creatinine result in mmol/l to give μmol Be/mol creatinine. This in fact was the case, the 62 control urine samples had an average creatinine concentration of 9.4 mmol/L, and the workers had an average creatinine concentration of 15.7 mmol/L (a median creatinine level from HSL data is 12 mmol/L (HSL 2009).
Mixed effects analysis for workers
Table 3 presents the results from the mixed effects analysis of uncorrected urinary beryllium concentrations in workers. Statistically significant effects were seen for smoking (smokers 37% higher from the antilog of the estimate in Table 3), time of the week (end of week samples 47% higher) and (log) creatinine, although the estimate for the latter (0.37) indicates a strongly sub-linear relationship between the untransformed urinary concentrations of beryllium and creatinine. As all workers were male, gender effects could not be investigated. The intercept term represents the mean (on a log scale) concentration for non-smokers at the start of the working week. The mixed effects model also gives estimates of inter- and intra-individual variability; both were modest at 0.48 and 0.70, respectively, equating to approximately two-fold and two-and-a-half-fold inter-quartile ranges.
Discussion
The urinary beryllium results from the aluminium smelter workers in this study show only a very low level of exposure with a mean of 19.5 ng/L (0.3 μmol/mol creatinine). There are very few studies reporting urinary beryllium levels at the low levels determined in this study. Some recent publications using a variety of methods—electrothermal atomic absorption spectrometry (Wegner et al. 2000) (quoting a limit of measurement as 60 ng/L) and ICP-MS with LODs up to 130 ng/L (Caldwell et al. 2005; Minoia et al. 1990; Paschal et al. 1998)—all quoted limits of detection not low enough for the measurement of urinary beryllium. Caldwell et al. reported the data for the US NHANES study when urinary beryllium was analysed in 2,465 urine samples. However, the results show that because of the higher LOD of 130 ng/L most of the measurements were not detected (Caldwell et al. 2005). In the results reported here only 8% of all samples below the LOQ in this study (as shown in Table 2).
In fact only five publications have quoted low LODs that would allow the measurement of urinary beryllium at levels found in this study (Apostoli and Schaller 2001; Heitland and Köster 2004, 2006; Horng et al. 2002; Xia et al. 2004). Two of these studies reported data for workers and controls (Apostoli and Schaller 2001; Horng et al. 2002) and two studies reported reference ranges for unexposed persons (Heitland and Köster 2004, 2006). The last study only reported the methods and results from certified reference materials using low temperature electrothermal vaporisation inductively coupled plasma mass spectrometry (Xia et al. 2004); however, the study quoted an impressive LOD of 0.12 pg/mL (ng/L).
Apostoli and Schaller compared the urinary beryllium of 65 metallurgical workers in electrical steel plants and copper alloy foundries with air measurements (Apostoli and Schaller 2001). The instrumental LOD was 30 ng/L, and a correlation between air measurements and urinary beryllium levels was reported. Unexposed controls were reported to have urinary levels of less than 30 ng/L, and workers were shown to have higher urinary beryllium levels up to 540 ng/L depending on the job (Apostoli and Schaller 2001). The levels of urinary beryllium in unexposed persons in Apostoli’s study compared well with those reported here. Apostoli and Schaller also found that beryllium air levels in the then TLV-TWA range of 0.2 μg/m3 (recommended in 2001 by the industry) for inhalable dust corresponded to beryllium levels in urine between 120 and 150 ng/L. Horng et al. published a study looking at differences in beryllium exposure by measuring urinary beryllium in controls and steel workers in China in 2002. This work reported an LOD of 20 ng/L using an ET-AAS; however, the urinary beryllium levels for the unexposed controls were high at a range of 830 ± 460 ng/L with the steel workers having levels as high as 1,580 ± 460 ng/L. This is likely to reflect differences in environmental exposures. Levels of beryllium in 63 urine samples from the general population (all non-smokers) were reported in 2004 by Heitland and Köster. These samples were analysed along with 22 other elements using collision cell gas mode. The urine samples underwent a 5-fold dilution and analysed in cell mode, the LOD was 4 ng/L and the LOQ was reported as 14 ng/L. The concentrations of the urine samples were reported with a mean of 9 ng/L, which is less than the LOQ, the geometric mean was 7 ng/L and the range was <LOQ to 28 ng/L with a 95th percentile of 20 ng/L. The 90th percentile of our data showed a urinary beryllium value of 20 ng/L and this compares with 95th percentile of 20 ng/L as found in Heitland’s study. In the 2006 paper from Heitland looking at 30 elements, all the beryllium results for two children and 87 adults are all lower than the LOQ of 9 ng/L (Heitland and Köster 2006).
The statistical analysis presented in this paper utilises the widespread practice of substituting a value of half LOD in place of non-detected results. This practice is increasingly being recognised as potentially inadequate for anything other than rudimentary nonparametric statistical treatments of the data and can lead to substantial bias in results (Flynn 2010; Helsel 2010). In this study, a more sophisticated treatment of these values as left—censored observations was implemented in this study within a Bayesian framework (Morton et al. 2010). However, these results, which are not presented here, are almost identical to those obtained using the simpler methodology. This reflects the relatively modest number of results less than LOD found in this study (~10%).
Comparing the geometric standard deviations between the creatinine corrected and uncorrected values shows that there was greater variability in creatinine corrected results compared to uncorrected values. This is contrary to the underlying rational of creatinine correction, namely that it should be used to adjust urinary biomarker levels for varying levels of hydrations (if the mechanism of excretion makes hydration relevant), a process that ought to lead to a reduction in variability. Additionally, the linear mixed effects modelling determined a coefficient for log (creatinine) of 0.37 providing further evidence that in this instance conventional creatinine correction would be detrimental. An estimate closer to one would tend to indicate that creatinine correction was a useful entity in the reporting of beryllium.
While there is a statistically significant difference in uncorrected urinary beryllium concentrations between controls and workers, this difference becomes non-significant when considering creatinine corrected values. This reflects the higher creatinine concentrations found in workers (mean 15.7 mmol/L) than unexposed controls (mean 9.4 mmol/L) most likely due to dehydration due to hot working conditions. However, calculations based upon the effect for creatinine from the mixed effects analysis suggest that this difference in creatinine levels should only account for about a 20% difference in uncorrected urinary beryllium concentrations, whereas uncorrected levels in workers are approximately twice those in controls. Although the relationship between urinary beryllium and creatinine demands further investigation, ideally through a cohort of more highly exposed workers with more normal levels of hydration, this study suggests that creatinine adjustment probably should not be used for reporting beryllium results.
The German DFG Deutsche Forschungsgemeinschaft has recently set a Biological Substance Reference Value (BAR) of 50 ng/L (0.05 μg/L) for the 95th percentile of urinary beryllium in the general population (DFG 2009). The 95th percentile for the unexposed control samples (background range) in this study is 30.6 ng/L. This is somewhat lower than that reported by the DFG. In fact, the 95th percentile of workers in this study is only just above the 50 ng/L BAR at 53.8 ng/L, with a mean of 19.6 ng/L. Interestingly, the DFG did not use creatinine corrected values for the BAR that they have set and nor did any of the four publications discussed previously (Apostoli and Schaller 2001; Heitland and Köster 2004, 2006; Horng et al. 2002). The low levels of urinary beryllium observed in both workers and controls in this study are within the DFG background range and show that workers at the UK aluminium smelter are either not exposed or only exposed to very low levels of beryllium.
Workers were seen to have on average 47% higher urinary beryllium levels towards the end of the working week, with a rise in mean levels from 4.1 ng/L to 6.1 ng/L. Smokers were also observed to have a 37% higher urinary beryllium result than non-smokers. This could be as a result of hand-to-mouth transfer of beryllium or the fact that cigarettes are thought to contain beryllium. Historically, it has been believed that cigarettes contain beryllium. It has been estimated that the beryllium concentration of a filterless cigarette to be 120 ng per cigarette and other cigarettes to be as much as 0.74 μg/cigarette (Toxicological Profile for Beryllium, US Agency for Toxic substances and Disease Registry, Atlanta, GA, 2002). Smith et al. (1997) reviewed evidence for beryllium in cigarettes and concluded that it remains unclear as to whether current commercially available domestic cigarettes contain beryllium reporting a concentration range of 0–0005 μg/cigarette reported in the literature (Smith et al. 1997).
Conclusion
A routine ICP-MS method for urinary beryllium determinations has been developed. The method is reliable and reproducible but strict protocols and attention to detail must be in place to detect the low counts being measured. With an LOD of 6 ng/L, the method is sensitive enough to detect levels in non-occupationally exposed persons.
Mixed effect modelling of the data has shown significant differences were observed between the urinary beryllium levels in controls and workers; workers at the end of the week compared with the start of the week; and smokers compared to non-smokers.
There is some debate as to whether the results should be creatinine corrected or not. Both uncorrected results (in ng/L) and corrected results (μmol/mol creatinine) have been reported in this study. While creatinine correction seems to increase the variability of the results within the workers, there is an obvious difference in creatinine levels between the worker and the control samples in this study and so there is a possible case for creatinine correction to compensate differences in the urine matrices. However, the statistical analysis of workers suggests conventional creatinine adjustment may over compensate for differences in hydration.
The level of exposure in the workers in this study was low, with a mean urine beryllium concentration of 19.5 ng/L. Further work is needed from more workplaces before guidance values could be set. Biological monitoring can offer an early overall assessment of exposure to beryllium in the workplace. This information could be used to identify areas and workers that require the use of better controls and thus subsequently help protect workers from exposure and potential sensitisation.
References
Apostoli P, Schaller KH (2001) Urinary beryllium- a suitable tool for assessing occupational and environmental exposure? Int Arch Occup Environ Health 74:162–166
Bonsnes RW (1945) On the determination of creatinine by the Jaffé reaction. J Biol Chem 158:581
Brisson MJ (2009) Overview of Beryllium Sampling and Analysis, Chapter 1 In: Brisson MJ, Ekechukwu AA (ed) Beryllium- environmental analysis and monitoring. RSC Publishing, Cambridge, UK
Caldwell KL, Hartel J, Jarrett J, Jones RL (2005) Inductively coupled plasma mass spectrometry to measure multiple toxic elements in urine in NHANES 1999–2000. At Spectrosc 26:1–7
Day GA, Dufresne A, Stefaniak AB, Schuller CR, Stanton ML, Miller WE, Kent MS, Deubner DC, Kreiss K, Hoover MD (2007) Exposure pathway assessment at a copper-beryllium alloy facility. Ann Occup Hyg 51:67–80
Flynn M (2010) Analysis of censored data by constrained maximization of the Shapiro-Wilk W statistic. Ann Occup Hyg 54:263–271
DFG German DFG Deutsche Forschungsgemeinschaft (2009) List of MAK and BAT values 2009. Wiley-VCH, Germany
Goyer RA, Clarkson TW (2001) Toxic effects of metals, Chap. 23. In: Curtis D. Klassen (eds) Casarett & Doull’s toxicology-the basic science of poisons, 6th edn. McGraw-Hill, US
Heitland P, Köster HD (2004) Fast, simple and reliable routine determination of 23 elements in urine by ICP-MS. J Anal At Spectrosc 19:1552–1558
Heitland P, Köster HD (2006) Biomonitoring of 30 trace elements in urine of children and adults by ICP-MS. Clinica Chemica Acta 365:310–318
Helsel D (2010) Much ado about nothing: incorporating nondetects in science. Ann Occp Hyg 54:257–262
Hollins DM, McKinley MA, Williams C, Wiman A, Fillos D, Chapman PS, Madl AK (2009) Beryllium and lung cancer: a weight of evidence evaluation of the toxicological and epidemiological literature. Crit Rev Toxicol 39(S1):1–32
Horng CJ, Horng PH, Lin SC, Tsai JL, Lin SR, Tzeng CC (2002) Determination of urinary beryllium, arsenic and selenium in steel production workers. Biol Trace Elem Res 88:235–246
HSE (1997) HSG 167 Biological monitoring in the workplace. http://www.hse.gov.uk/pubns/books/hsg167.htm
HSL (2009) Guidance on laboratory techniques in occupational medicine HSE. 11th Edn
IARC (1997) Monographs on the evaluation of carcinogenic risks to humans. Beryllium, cadmium, mercury, and exposures in the glass manufacturing industry, vol 58. http://monographs.iarc.fr/ENG/Monographs/vol58/volume58.pdf
Infante PF, Newman LS (2004) Beryllium exposure and chronic beryllium disease. Lancet 363:1358–1359
Jaffe M (1886) Methods determining creatinine. Physiol Chem 10:39–40
Johnson JS, Foote K, McClean M, Cogbill G (2001) Beryllium exposure control program at the cardiff atomic weapons establishment in the United Kingdom. Appl Occup Environ Hyg 16:619–630
Kauppinen T, Toikkanen J, Pederson D, Young R, Ahrens W, Boffetta P, Hansen J, Kromhout H, Blasco JM, Mirabelli D, de la Orden-Rivera V, Pannett B, Plato N, Savela A, Vincent R, Kogevinas M (2000) Occupational exposure to carcinogens in the European union. Occup Environ Med 57:10–18
Madl AK, Unice K, Brown JL, Kolanz ME, Kent MS (2007) Exposure-response analysis for beryllium sensitisation and chronic beryllium disease among workers in a beryllium metal machining plant. J Occup Environ Hyg 4:448–466
Maier LA, Gunn C, Newman LS (2006) Beryllium disease. In: Rom WN, Markowitz S (eds) Environmental and occupational medicine, 4th edn. Lippincott Williams & Wilkins, Philadelphia, pp 1021–1037
Minoia C, Sabbioni E, Apostoli P, Pietra R, Poxxoil L, Gallorini M, Nicolaou G, Alessio L, Capodaglio E (1990) Trace element reference values in tissues from inhabitants of the European community I. A study of 46 elements in urine, blood and serum of Italian subjects. Sci Total Environ 95:89–105
Morton J, Cotton R, Cocker J, Warren ND (2010) Trends in blood lead levels in UK workers 1995–2007. J Occup Environ Med 67:590–595
Paschal DC, Ting BG, Morrow JC, Pirkel JL, Jackson RJ, Sampson EJ, Miller DT, Caldwell KL (1998) Trace element in urine of US residents: reference range concentrations. Environ Res Sect A 76:53–59
Rana SVS (2008) Metals and apoptosis: recent developments. J Trace Elem Med Biol 22:262–284
Santo Tomas LH (2009) Beryllium hypersensitivity and chronic lung disease. Curr Opin Pulm Med 15:165–169
Smith CJ, Livingston SD, Doolittle DJ (1997) An international literature survey of ‘IARC group 1 carcinogens’ reported in mainstream cigarette smoke. Food Chem Toxicol 35:1107–1130
Stiefel T, Schulze K, Zorn H, Tölg G (1980) Toxicokinetic and thermodynamic studies of beryllium. Arch Toxicol 45:81–92
Taiwo OA, Slade MD, Cantley LF, Fiellin MG, Wesdock JC, Bayer FJ, Cullen MR (2008) Beryllium sensitization in aluminum smelter workers. J Occup Environ Med 50:157–162
Thomas CA, Bailey RL, Kent MS, Duebner DC, Kreiss K, Schuler CR (2009) Efficacy of a program to prevent beryllium sensitisation among new employees at a copper-beryllium alloy processing facility. Public Health Rep 124P:112–124
Wegner R, Henrich-Ramm R, Nowak D, Olma K, Poschadel B, Szadkowski D (2000) Lung function, biological monitoring and biological effect monitoring of gemstone cutters exposed to beryls. Occup Environ Med 57:133–139
Xia L, Hu B, Jiang Z, Wu Y, Liang Y (2004) Single-drop microextraction combined with low-temperature electrothermal vaporization ICP-MS for the determination of trace Be, Co, Pd and Cd in biological samples. Anal Chem 76:2910–2915
Zorn H, Stiefel T (1977) The problem of a threshold limit value of beryllium and its salts. In: Proceeding of the Fourth International Conference on Beryllium. The Metals Society, London
Acknowledgments
The work described here was funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy. The Health and Safety Laboratory’s Investment Research Programme funded the writing of this publication. The authors would also like to thank Dr Simon Nelms from Thermo Fisher Scientific for his expertise and assistance with the ICP-MS method.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morton, J., Leese, E., Cotton, R. et al. Beryllium in urine by ICP-MS: a comparison of low level exposed workers and unexposed persons. Int Arch Occup Environ Health 84, 697–704 (2011). https://doi.org/10.1007/s00420-010-0587-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-010-0587-2