
Abstract
Objectives
To assess the influence of working conditions and individual factors on the incidence of neck and upper limb symptoms among professional computer users.
Methods
The study is a prospective cohort study with an observation period of 10 months. A baseline questionnaire about symptoms in the neck, shoulder and arm/hand during previous month, individual factors, work content, physical and psychosocial work-related exposures was answered by 1,283 computer operators (response rate 84%). Incidence data were collected by ten monthly questionnaires regarding the occurrence of symptoms categorized into three gross body regions: neck, shoulders and arms/hands. A case, in the specific gross body region, was defined as a subject who was classified as non-symptomatic in that region at baseline or during minimum one follow-up period and later reported symptoms (≥3 days). Univariable and multivariable incidence rate ratios with 95% confidence intervals for first occurrence of neck, shoulder and arm/hand cases, respectively, were calculated with Cox regression analysis.
Results
The incidence rate was 67, 41 and 47 cases per 100 person years for neck, shoulder and arm/hand symptoms, respectively. In the multivariable analyses, comfort of the computer work environment and gender were related to the incidence of symptoms in all body regions (RR = 1.5–1.9 for low comfort and 1.8–2.1 for females, respectively). Duration of mouse use predicted arm/hand symptoms (RR = 1.7 for ≥3 h/day) and job strain (high demands and low decision latitude) predicted neck symptoms (RR = 1.6 and 2.2 for medium and high strain, respectively). Additionally, age was related to neck and shoulder symptoms.
Conclusion
Preventive strategies to reduce neck and upper limb symptoms among computer users should include measures to reduce mouse use, to increase the comfort of the work environment and to reduce job strain. Although the effect estimates were relatively weak to moderate, preventive measures may have a marked impact on the incidence of neck and upper limb symptoms in the general population because of the widespread use of computers in working life as well as at home.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Seventy percent of the Swedish working population use computers at work and 15% report using a computer almost all the time (Work Environment Authority and Statistics Sweden 2008). Neck and upper limb symptoms are common among computer users (Ekman et al. 2000). In computer intensive work sectors as, e.g., office and customer service work, where 38% of the employees report using a computer almost all the time, 40% experience weekly pain in the upper back or neck and 37% experience pain in the shoulders or arms compared with 34 and 32%, respectively, in the general working population (Work Environment Authority and Statistics Sweden 2008).
These symptoms have multifactorial origin and individual and both work and non-work-related physical and psychosocial factors may contribute to the development and impairment (Bongers et al. 2006). Several cross-sectional studies have shown a relationship between exposures related to computer work and subjective complaints in the neck and upper limbs (Karlqvist et al. 1996; Blatter and Bongers 2002; Fogelman and Lewis 2002; Jensen et al. 2002a, b). Additionally, recent longitudinal studies support a cause–effect relationship between intensive computer use or other computer work-related exposures and complaints in the neck and upper limbs (Gerr et al. 2002; Marcus et al. 2002; Jensen 2003; Andersen et al. 2003; Korhonen et al. 2003; Kryger et al. 2003; Brandt et al. 2004; Juul-Kristensen et al. 2004; Lassen et al. 2004; Juul-Kristensen and Jensen 2005; Rempel et al. 2006; IJmker et al. 2007; Andersen et al. 2008).
The aim of this study was to assess the influence of working conditions and individual factors on the incidence of neck and upper limb symptoms among professional computer users.
Methods
Study design
This study is a prospective cohort study with an observation period of 10 months. A self-administered questionnaire at baseline was used to assess individual and life-style factors, work content, physical and psychosocial exposures during work, and information about symptoms in the neck and upper limbs. Incidence data were collected during the observation period, identifying cases by a monthly short questionnaire regarding the occurrence of symptoms in the neck and upper limbs.
Together with the employers and the Occupational Health Care Centers, 46 different worksites or departments from both the private and the public sector were selected to achieve contrasts regarding computer work duration and type of computer work tasks. The number of employees at these sites varied between 7 and 260 persons. All employees with seniority of at least 1 month in the present job and without any additional employment exceeding 25% of a full-time employment were included in the study population. The questionnaires were distributed and recollected by ergonomists at the Occupational Health Care Centers. The study was approved by the local ethics committee at the Karolinska Institute and the regional ethics committee at the University of Gothenburg. All participants gave their informed consent prior to their inclusion in the study.
Study population
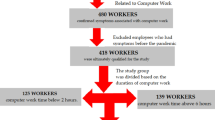
The study population included 1,529 employees from a variety of occupations. The baseline questionnaire was answered by 1,283 subjects, 498 men and 785 women with a mean age of 44 years (range 20–65) (Fig. 1). The response rate was thus 84%, and the main reason for not participating was refusal. The average follow-up time from baseline was 320 days (range 0–540).

Flow chart of the enrolled study population, participants at baseline and follow-up and incidence rates for neck, shoulder and arm/hand symptoms, respectively
The participants included the following occupations; administrators (n = 115), call-centre operators (n = 57), computer support personnel (n = 23), engineers (n = 186), graphics industry operators (n = 121), handling officers/investigators (n = 138), insurance officers (n = 169), librarians (n = 83) managers/marketing officers (n = 92), medical secretaries (n = 72), messengers (n = 53), occupational health personnel (39), receptionists (14), university teachers/researchers (n = 121). The participants had the same or similar work tasks since in average 12 years (SD 10) and had used computers since 11 years (SD 7). They worked in average 38 h/week (SD 5) and computer work represented in average 48% (SD 23) of their working hours. Information about computer work tasks, physical and psychosocial working conditions is presented elsewhere (Karlqvist et al. 2002).
Out of those 1,283 subjects who answered the baseline questionnaire, 1,247 answered at least one follow-up questionnaire whereof 1,216 subjects responded to the first and 951 to the last follow-up questionnaire (Fig. 1). The average follow-up time from baseline among those who answered at least one follow-up questionnaire was 329 days (range 28–540). There were some differences between dropouts and subjects remaining until the 10th follow-up. The prevalence of neck symptoms at baseline was significantly higher (55 and 45%, Chi-square P = 0.002) and the mean age slightly lower (43 and 44 years, Chi-square P = 0.02) among dropouts compared with subjects remaining. No significant differences were, however, observed regarding the prevalence of shoulder and arm/hand symptoms or daily duration of computer work.
Questionnaire
The occurrence of symptoms in the neck and upper limbs, work-related exposures during the preceding month and individual and life-style factors were assessed at baseline by a self-administered questionnaire containing 88 items (http://www.amm.se/eng). The questions about symptoms referred to the duration (days) of pain or ache during the preceding month in the following regions: the neck, right and left scapular area, shoulder joint/upper arm, elbow/forearm, wrist and hand/fingers (including numbness in the hand/fingers), respectively. Information about symptoms prior to the preceding month was not asked for.
The present paper includes exposures related to work content; daily duration of computer work, duration of data/text entry, duration and frequency of continuous computer work without breaks, duration of mouse (or other non-keyboard input device) use, variation of work tasks; physical exposures; mouse placement, comfort of the computer work environment, psychosocial exposures; job demands in relation to competence, job strain, social support and individual factors; sex, age and educational level. Additionally, potential effects of body mass index (BMI), number of children at home, nicotine use and physical training were investigated.
Description of work-related exposures and related questionnaire items
Duration of computer work
Computer work was one item in a question regarding the percentage of working time spent on nine specified work tasks; computer work, typewriting, telephoning, non-computer desk work (e.g., reading and writing, calculating, drawing by hand), copying and bringing material, teaching, meetings (formal), discussions with co-workers (informal), rest-breaks, and one unspecified “other” work task. The sum of the percentage given for each task comprised 100% of the working time and the duration, hours/day, of computer work was calculated from the percentage of time spent on this task and the number of working hours.
Duration of data/text entry
Data/text entry was one item in a question regarding the percentage of time spent on nine specified computer work sub-tasks; data/text entry from source document, authoring own texts, layout and graphics, construction and design, economic and personnel administration, data treatment and statistics, programming, e-mailing, internet search and one unspecified “other” computer task. The sum of the percentage given for each computer task comprised 100% of the duration of computer work and the duration, hours/day, of data/text entry was calculated from the percentage of time spent on this sub-task and the duration of computer work (above).
Duration and frequency of continuous computer work without breaks
Ratings of the longest period of continuous computer work without a break (>10 min), 7-graded scale from <1 to >6 h, in combination with ratings of how often this happened, 4-graded scale from very occasionally to daily or almost daily.
Duration of mouse (or other non-keyboard input device) use
Ratings of the percentage of the computer working time spent using the mouse (or other non-keyboard input devices) and the keyboard, respectively. The sum of the percentage given for each device comprised 100% of the duration of computer work and the duration, hours/day, was calculated from the percentage of time spent with mouse use and the duration of computer work (above).
Variation of work tasks
This exposure was based on the question regarding the percentage of working time spent on nine specified work tasks and the calculated duration, hours/day, of each task (see “Duration of computer work”). Exposure was categorized from the number of tasks that constituted on average of at least 30 min/day.
Mouse placement
The mouse position was marked on a drawing illustrating the work table and the operator’s position. Mouse placement within forearms length and shoulder width was considered as “optimal”, otherwise “non-optimal” exposure (Karlqvist et al. 1996).
Comfort of the computer work environment
Ratings of 11 variables related to the comfort of the computer work environment (general lighting, workstation lighting, dazzling/reflections on the screen, noise level, indoor climate, chair, work posture, work space, screen position, keyboard and mouse position), a 9-graded scale from −4, very, very bad to +4, very, very good. Exposure was categorized from the sum score, range −44 to +44 (Karlqvist et al. 1996).
Job demands in relation to competence
Ratings of demands at work in relation to competence, 6-graded scale from “considerable above my level of competence” to “considerable below my level of competence” and “do not know”.
Job strain
Ratings of job demands (five items) and decision latitude (four items about possibilities to learn and develop and two about authority over decisions) used 4-graded scales from “almost never/never” to “often” (1–4) (Karasek 1979; Theorell et al. 1988; Toomingas et al. 1997). An index score for job demands was calculated by adding scores from the five items (range 5–20; the higher score the higher job demands). A similar index score for decision latitude was calculated by adding scores from the combined six items (range 6–24; the higher score the higher decision latitude). Exposure was categorized from the combinations of the job demand and decision latitude scores.
Social support
Ratings of social support at work, six items, 4-graded scales from “strongly agree” to “strongly disagree” (1–4) (Toomingas et al. 1997). An index score was calculated by adding scores from the six items (range 6–24; the higher score the better social support).
Follow-up
Incidence data were collected by ten monthly questionnaires regarding the occurrence of neck and upper limb symptoms. The questions referred to the time period following the preceding questionnaire, which usually covered approximately 1 month. This period could be longer due to vacations or other reasons for absence. If a follow-up questionnaire was not returned before the next one appeared, the time frame considered for reporting symptoms covered the whole period since the previous questionnaire, i.e., approximately 2 months. If two consecutive questionnaires were missing, the person–time for that subject was terminated at the time when the last questionnaire was completed.
Data treatment and analysis
Symptoms were defined as reports of pain or aches in any of the body regions asked about, or numbness in the hand/fingers, ≥3 days during the preceding month. Symptoms in the specific body regions were compiled into three gross body regions: (a) neck and/or scapular area (here called neck), (b) shoulder joints/upper arms (here called shoulders), (c) elbows/forearms and/or wrists and/or hands/fingers (here called arms/hands). Subjects reporting symptoms ≤2 days in all regions included in the respective compiled region (a–c) were regarded as non-symptomatic for this region.
A case, in the gross body region, was defined as a subject who was classified as non-symptomatic in that region at baseline or during minimum one follow-up period and later reported symptoms. Only first-time cases were considered. The incidence rate was calculated as the frequency of cases divided by the total person–time at risk over the period (Rothman and Greenland 1998). Cases contributed with a person–time corresponding to the period between the dates of the questionnaires when they were non-symptomatic for the first time and when they for the first time during follow-up became a case. Subjects who did not become a case during the follow-up contributed with a person–time corresponding to the period between the dates when they were non-symptomatic for the first time and when they filled in their last follow-up questionnaire.
The subjects were categorized into a low exposed “reference” group and generally into two exposure levels, a “medium” and a “highly” exposed group (see “Results”).
Univariable incidence rate ratios (relative risks, RR) with 95% confidence intervals (95% CI) were calculated for neck, shoulder and arm/hand cases, respectively. Adjusted RRs were subsequently calculated for each body region by multivariable Cox regression analyses for exposures where the 95% CI did not include 1.00 for any of the three outcome categories in the univariable analyses (Cox regression analysis, PHREG procedure, SAS statistical package, version 9.1.3, SAS Institute, Cary, NC, USA). Thus, for the sake of comparability, the multivariable analyses included the same exposures for all three outcomes.
The statistical test for trend was used to estimate if there was a linear trend across the exposure categories, i.e., if an exposure–response relationship was indicated. The test was based on one variable with three values (lowest to highest) in the multivariable analyses.
Results
During the observation period, 441 neck cases, 343 shoulder cases and 381 arm/hand cases were identified. The incidence rate was 67, 41 and 47 cases per 100 person years for neck, shoulder and arm/hand symptoms, respectively (Fig. 1). Several cases reported co-morbidity, 62% of the neck cases and 90 and 77% of the shoulder and arm/hand cases, respectively (Table 1).
Kaplan–Meier survival curves illustrate examples of the difference in non-case frequency during follow-up between low, medium and high exposures (Fig. 2a–c). Similar curves were observed for all exposures that indicated effects in the univariable analyses.

Kaplan–Meier survival curves showing the difference in a neck, b shoulder and c arm/hand non-case frequency, respectively, during follow-up between low, medium and high computer work-related exposures
Univariable results
The work-related exposures duration and frequency of continuous computer work without breaks, comfort of the computer work environment, variation of work tasks and job strain predicted symptoms in all body regions (Table 2). Duration of computer work predicted neck and hand/arm symptoms and duration of mouse use predicted shoulder and arm/hand symptoms. Additionally, duration of data/text entry and demands in relation to competence predicted neck symptoms. Female gender showed an approximately twofold increased RR for all outcomes compared with men. In the intermediary age group, 36–50 years, an increased RR was observed for neck and shoulder symptoms and the oldest age group, >50 years, also showed an increased RR for shoulder symptoms. Low education predicted neck symptoms.
Apart from the exposures presented in Table 2, BMI, number of children at home, nicotine use and physical exercise were investigated. These determinants did not show any effect on the incidence of symptoms except for the medium category of physical exercise (1–7 times, ≥30 min/time, previous month) where a slight increase in incidence of neck and shoulder symptoms was indicated compared with both more and less exercise. However, none of these determinants had any marked effect on the multivariable results and were not included in the multivariable model.
Multivariable results
Comfort of the computer work environment predicted symptoms in all body regions, and exposure–response relationships was observed (Table 3). Additionally, duration of mouse use predicted shoulder and arm/hand symptoms, with an indicated exposure–response relationship for arm/hand symptoms. Job strain predicted symptoms in the neck and an exposure–response relationship was observed. Female gender was a marked risk factor for all outcomes. Intermediary age increased the RR for neck and shoulder symptoms and the oldest age group also showed an increased RR for shoulder symptoms.
Discussion
A high incidence of neck and upper extremity symptoms were observed among professional computer users and the comfort of the computer work environment, duration of mouse use and job strain were the most prominent work-related risk factors.
Incidence of symptoms
The highest incidence was observed for neck symptoms, 67 cases per 100 person years, followed by arm/hand and shoulder symptoms, 47 and 41 cases per 100 person years, respectively. The incidence rates observed are of the same magnitude as observed in a prospective study of computer users, by Gerr et al. (2002). In that study the incidence for neck/shoulder and hand/arm symptoms, respectively, was 58 and 39 cases per 100 person years, although the symptom case definition (symptoms during the preceding week combined with discomfort severity or medication) differed from the definition in our study.
The difference in incidence between the different body regions shows the same pattern as observed for the prevalence of symptoms observed at baseline in the present study, i.e., the highest prevalence was observed for neck symptoms, 48%, followed by arm/hand, 33%, and shoulder symptoms, 26% (Karlqvist et al. 2002).
Work-related risk factors
The general pattern of associations between several computer related duration variables and the incidence of neck, shoulder and arm/hand symptoms, respectively, observed in the univariable analyses was not evident in the multivariable analyses: Here, only the duration of mouse use was quite clearly related to arm/hand symptoms and, although only statistically significant for the medium exposure category, also to shoulder symptoms. These results are in agreement with a recent systematic review of the relationship between the duration of working time spent using the computer and the incidence of arm/hand and neck/shoulder symptoms and disorders (IJmker et al. 2007). The authors conclude that there is moderate evidence, with a dose–response relationship, for a positive association between duration of mouse use and hand/arm symptoms. The risk estimates were generally stronger for the hand/arm region than for the neck/shoulder region, and stronger for mouse use than for keyboard and total computer use (IJmker et al. 2007). A recent prospective study, with continuous objective recordings of computer usage, showed that for each quartile increase in mouse usage the risk for acute neck pain increased by 4% and the risk for acute shoulder pain by 10% (Andersen et al. 2008).
Comfort of the computer work environment predicted symptoms in all three outcome regions with a significant effect in the multivariable analyses and an exposure–response relationship for all outcomes. This determinant is a crude measure of overall comfort and besides comfort regarding different aspects of the computer workstation layout and work postures it also includes lighting, noise and indoor climate conditions. The ratings of comfort regarding different aspects of computer workstation layout have been validated in relation to ergonomic observations and the concordance between ratings and observations were reasonably good to good (Lindegård et al. 2005). In a prospective study of Finnish office employees with VDU work, self-rated poor physical work environment and VDU-related ergonomics predicted incident neck pain (Korhonen et al. 2003). A recent cross-sectional study among call-centre operators showed strong associations between comfort of the work environment and neck/shoulder and arm/hand symptoms, respectively (Norman et al. 2008). Although cause–effect relations cannot be evaluated from the above cross-sectional study our longitudinal results support a possible cause–effect relation.
Job strain was the strongest work-related predictor for neck symptoms with a significant exposure–response relationship. There are increasing evidence that psychosocial work-related factors may increase muscle tension and play an important role in the development of neck and upper limb symptoms and disorders (Theorell 1996; Lundberg 2002; Bongers et al. 2006). A recent review of longitudinal relationships between the demand-control-support dimensions and upper limb symptoms shoved that high work demands or low control at work are often related to these symptoms but the relationship is neither very strong nor very specific (Bongers et al. 2006). The combination of high demands and low control, i.e., high job strain, seemed to have more impact on neck/shoulder symptoms than on arm/wrist symptoms (Bongers et al. 2006). Although the etiologic mechanisms are still insufficiently understood several plausible explanations have been suggested (Theorell 1996; Toomingas et al. 1997; Lundberg 2002; Melin and Wigaeus Tornqvist 2005). Compared with physical exposures, psychosocial exposures are usually more lasting and may contribute to elevated muscle tension also during breaks and after work (Lundberg 2002). Thus, reducing job strain, and other adverse psychosocial conditions, is probably of great importance to prevent neck pain.
Individual risk factors
Women were approximately twice as likely as men to develop neck, shoulder as well as arm/hand symptoms. Similar results were observed in other longitudinal studies (Gerr et al. 2002; Jensen 2003; Kryger et al. 2003; Juul-Kristensen et al. 2004; Andersen et al. 2008). The difference between men and women seems to only partly be explained by the gender segregated labor market since differences within the same occupations are also observed (Melin and Wigaeus Tornqvist 2005). Women may be at higher risk than men due to different work tasks within the same job but gender differences have also been observed in jobs where men and women have identical work tasks, e.g., among call-centre operators (Karlqvist et al. 2002; Norman et al. 2004). In addition, women do generally have more household duties and childcare and thus a larger total workload and less possibility to recover after work. Studies have also shown that women may perform the same computer work tasks with more non-optimal postures than men, which may be due to anthropometric differences (Karlqvist et al. 1999; Wahlström et al. 2000). Biological/physiological differences may also contribute to the observed gender differences and both subjective and objective measurement methods have demonstrated greater sensitivity to pain in women than in men (Hellström and Lundberg 2000; Hallin 2003). Additionally, women may have a lower threshold than men to report symptoms. However, a prospective study of computer users showed that women, compared with men, had a 1.7 and 1.6 times higher risk for developing neck/shoulder and arm/hand symptoms, respectively, whereas the risk of developing examination-confirmed neck/shoulder or arm/hand disorders was 1.9 and 2.4, respectively (Gerr et al. 2002). Additionally, in a case–control study of the influence of work-related exposures on seeking care due to neck and shoulder disorders 71% of the women who sought care received a confirmed diagnosis compared with 58% of the men (Wigaeus Tornqvist et al. 2001). These observations do not support that women have a lower threshold to report symptoms than men do.
In the multivariable analyses medium age (36–50 years) was a risk factor for neck symptoms and both high (>50 years) and medium age was a risk factor for shoulder symptoms, whereas age did not predict arm/hand symptoms. These findings are consistent with other prospective studies of computer users showing increased age as a risk factor for neck and shoulder symptoms (Gerr et al. 2002; Andersen et al. 2008), but not for hand/wrist symptoms (Gerr et al. 2002; Lassen et al. 2004).
Co-morbidity
This study showed a high co-morbidity; 62% of the neck cases experienced symptoms also in the shoulder and/or arm/hand and corresponding figures for shoulder and arm/hand cases were 90 and 77%, respectively. This reduces the possibility to identify risk factors specific for different body regions and the general pattern of risk factors observed in the univariable analyses was quite similar for the three outcome regions. However, the multivariable analyses do indicate that duration of mouse use seem to have a greater impact on arm/hand compared with neck symptoms, which is in agreement with the review by IJmker et al. (2007). Additionally, the multivariable analyses do also indicate that job strain have a greater impact on neck symptoms compared with arm/hand symptoms, which is in agreement with the review by Bongers et al. (2006).
Methodological considerations
The major strength of this study is its longitudinal design allowing for identification of cause–effect relationships. One problem in longitudinal studies is dropouts during the follow-up period. In the present study, 76% of those who answered at least one follow-up questionnaire participated at the final 10th follow-up. There was a slight selection bias, dropouts had a higher prevalence of neck symptoms at baseline and was slightly younger compared with subjects who remained until the last follow-up. The higher prevalence of neck symptoms among drop-outs may have entailed a slight reduction of neck cases since previous symptoms predict the development of “new” symptoms (Jensen 2003; Juul-Kristensen et al. 2004). It is, however, unlikely that this selection bias would entail overestimation of effects. Another problem in longitudinal studies is that exposure is usually only determined at one point in time, but may vary during the observation period. In this study, changes of work-related exposures were included in the short monthly questionnaire, but potential effects of these changes were not considered in the present paper. Potential changes in exposures are, however, unlikely to cause overestimation of effects, but would rather cause an underestimation of effects due to non-differential misclassification of exposure.
One limitation in the present study is that both exposures and outcomes were self-reported. The validity of self-reported physical exposures has been questioned. Studies have shown that self-reported duration and proportions of computer work is overestimated, and only moderately associated with objective measurements (Faucett and Rempel 1996; Heinrich et al. 2004; Homan and Armstrong 2003; Mikkelsen et al. 2007). Self-reports explained about one-fourth to one-third of objective recordings and the overestimation was large at low levels and less pronounced at higher objectively measured exposures (Mikkelsen et al. 2007). If the misclassification of exposure is independent of the outcome, this non-differential misclassification will entail an underestimation of effects and, as the overestimation of computer time variables were more marked at low exposures the underestimation of effects will be even more prominent. Therefore, in the present study, misclassification may have diluted the effect estimates for the computer-time-related exposures and some risk factors may not have been identified. If, however, the misclassification differs between cases and non-cases this can lead to overestimation of effects. In the above validation study of self-reported computer time variables there was a small bias in self-reported computer time variables related to arm pain (Mikkelsen et al. 2007), while other studies found no symptom-related bias (Faucett and Rempel 1996; Heinrich et al. 2004). Theoretically, differential misclassification should not be a problem in this study because exposure was assessed before the outcome. However, as the these symptoms often are recurrent events it is possible that subjects who experience symptoms now and then may unconsciously overestimate exposures that they relate to feelings of fatigue or pain even if they are symptom-free during the month when they report exposure. As prior symptoms are a risk factor for “new” events (Jensen 2003; Juul-Kristensen et al. 2004), we cannot exclude the possibility of differential misclassification. To avoid such possible bias it is necessary to study the incidence of pure first time cases. An optimal design would be to follow subjects from when exposure starts. However, as computer use starts early in life and young people experience symptoms before they enter into the working life, such design is not easy to accomplish (Palm et al. 2007). Additionally, the debate in media about computer- and mouse-related symptoms may bias self-reported exposure and outcome.
In the present study, we chose self-reported symptoms for 3 days or more during the previous month as the outcome measure. By asking the participants to answer a short questionnaire each month, we anticipated that subjects would remember potential symptoms, and that the risk of unidentified events was minimized. The reason for not including symptoms less than 3 days during the previous month was to exclude muscle soreness after physical training. As the case definition does not include any criteria for pain intensity or disability the outcome may include cases with mild as well as more severe symptom intensity. Between 16 and 18% of the cases did, however, report reduced computer work productivity owing to musculoskeletal symptoms (Hagberg et al. 2007). Several studies have shown that a relatively low proportion of symptomatic computer users can be classified into specific diagnostic categories (Andersen et al. 2003; Brandt et al. 2004; Lassen et al. 2004), although other studies report that a relatively large proportion of symptom cases met the criteria for specific disorders (Gerr et al. 2002). However, the proportion between diagnosed and symptom cases depends on the diagnostic criteria used, the seriousness of the symptoms and the study population. Reasons for a low concordance between complaints and specific diagnoses may be that the complaints are mild and early cases of a specific disease, that the complaints are related to multiple diagnosis or that the pain processes do not fit into (yet) accepted diagnoses (Sluiter et al. 2001). Additionally, beliefs regarding associations between exposure and symptoms may bias symptom reporting. Although several computer work-related exposures have been associated with neck and upper-extremity musculoskeletal complaints, studies where disorders are verified by physical findings as outcomes have not been able to confirm the results based on subjective complaints and a recent review indicate only limited evidence for a causal relationship between computer use and wrist tendonitis and neck pain with physical findings (Veierstedt et al. 2006).
However, regardless of a confirmed diagnosis or physical findings, prevention of neck and upper extremity pain is important as these symptoms may cause individual suffering, increased costs for employers and society due to, e.g., sickness absenteeism, and also “hidden” costs due to reduced productivity (Hagberg et al. 2002, 2007). Although the risk factors for neck and upper limb symptoms generally show weak to moderate effect estimates, subjects are often exposed to several risk factors. The relative risk for symptoms increases with increasing number of risk factors and their concomitant effect may explain the relatively high incidence of symptoms observed (Wigaeus Tornqvist et al. 2001). Preventive strategies should therefore be multifactorial and focus on risk factors confirmed in independent studies, e.g., comfort of the work environment, duration of computer mouse use and job strain (Korhonen et al. 2003; IJmker et al. 2007; Bongers et al. 2006). Interventions to confirm the preventive impact of reducing these exposures are warranted.
Conclusion
The results suggest that preventive strategies to reduce neck and upper limb symptoms among computer users should include measures to reduce mouse use, to increase the comfort of the computer work environment and to reduce job strain (high demands and low decision latitude). Although the effect estimates were relatively weak to moderate, preventive measures may have a marked impact on the incidence of neck and upper limb symptoms in the general population because of the widespread use of computers in working life as well as at home.
References
Andersen JH, Thomsen JF, Overgaard E, Lassen CF, Brandt LP, Vilstrup I, Kryger AI, Mikkelsen S (2003) Computer use and carpal tunnel syndrome: a 1-year follow-up study. JAMA 289(22):2963–2969. doi:10.1001/jama.289.22.2963
Andersen JH, Harhoff M, Grimstrup S, Vilstrup I, Lassen CF, Brandt LPA, Kryger AI, Overgaard E, Hansen KD, Mikkelsen S (2008) Computer mouse use predicts acute pain but not prolonged or chronic pain in the neck and shoulder. Occup Environ Med 65(2):126–131. doi:10.1136/oem.2007.033506
Blatter BM, Bongers PM (2002) Duration of computer use and mouse use in relation to musculoskeletal disorders of neck or upper limb. Int J Ind Ergon 30:295–306. doi:10.1016/S0169-8141(02)00132-4
Bongers PM, Ijmker S, van den Heuvel S, Blatter BM (2006) Epidemiology of work related neck and upper limb problems: psychosocial and personal risk factors (part I) and effective interventions from a bio behavioural perspective (part II). J Occup Rehabil 16(3):279–302. doi:10.1007/s10926-006-9044-1
Brandt LP, Andersen JH, Lassen CF, Kryger A, Overgaard E, Vilstrup I, Mikkelsen S (2004) Neck and shoulder symptoms and disorders among Danish computer workers. Scand J Work Environ Health 30(5):399–409
Ekman A, Andersson A, Hagberg M, Hjelm EW (2000) Gender differences in musculoskeletal health of computer and mouse users in the Swedish workforce. Occup Med (Lond) 50(8):608–613
Faucett J, Rempel D (1996) Musculoskeletal symptoms related to video display terminal use. An analysis of objective and subjective exposure estimates. AAOHN J 44:33–39
Fogelman M, Lewis R (2002) Factors associated with self-reported musculoskeletal discomfort in video display terminal (VDU) users. Int J Ind Ergon 29:311–318. doi:10.1016/S0169-8141(01)00071-3
Gerr F, Marcus M, Ensor C, Kleinbaum D, Cohen S, Edwards A, Gentry E, Ortiz DJ, Monteilh C (2002) A prospective study of computer users: I. Study design and incidence of musculoskeletal symptoms and disorders. Am J Ind Med 41(4):221–235. doi:10.1002/ajim.10066
Hagberg M, Wigaeus Tornqvist E, Toomingas A (2002) Self-reported reduced productivity due to musculoskeletal symptoms: associations with workplace and individual factors among white-collar computer users. J Occup Rehabil 12(3):151–162
Hagberg M, Vilhemsson R, Wigaeus Tornqvist E, Toomingas A (2007) Incidence of self-reported reduced productivity owing to musculoskeletal symptoms: association with workplace and individual factors among computer users. Ergonomics 50(11):1820–1834. doi:10.1080/00140130701674539
Hallin RG (2003) Smärta mer smärtsam hos kvinnor. Genusperspektiv eftersatt i forskning om smärtans biologiska mekanismer (in Swedish) (Pain more painful in women. Gender perspective neglected in research on the biological mechanisms of pain). Lakartidningen 100(46):3738–3741
Heinrich J, Blatter BM, Bongers PM (2004) A comparison of methods for the assessment of postural load and duration of computer use. Occup Environ Med 61(12):1027–1031. doi:10.1136/oem.2004.013219
Hellström B, Lundberg U (2000) Pain perception to the cold pressor test during the menstrual cycle in relation to estrogen levels and a comparison with men. Integr Physiol Behav Sci 35(2):132–141. doi:10.1007/BF02688772
Homan MM, Armstrong TJ (2003) Evaluation of three methodologies for assessing work activity during computer use. AIHA J (Fairfax, Va) 64(1):48–55. doi:10.1080/15428110308984784
IJmker S, Huysmans MA, Blatter BM, van der Beek AJ, van Mechelen W, Bongers PM (2007) Should office workers spend fewer hours at their computer? A systematic review of the literature. Occup Environ Med 64(4):211–222. doi:10.1136/oem.2006.026468
Jensen C (2003) Development of neck and hand-wrist symptoms in relation to duration of computer use at work. Scand J Work Environ Health 29(3):197–205
Jensen C, Finsen L, Sogaard K, Christensen H (2002a) Musculoskeletal symptoms and duration of computer work and mouse use. Int J Ind Ergon 30:265–275. doi:10.1016/S0169-8141(02)00130-0
Jensen C, Ryholt C, Burr H, Villadsen E, Christensen H (2002b) Work-related psychosocial, physical and individual factors associated with musculoskeletal symptoms in computer users. Work Stress 16(2):107–120. doi:10.1080/02678370210140658
Juul-Kristensen B, Jensen C (2005) Self-reported workplace related ergonomic conditions as prognostic factors for musculoskeletal symptoms: the “BIT” follow up study on office workers. Occup Environ Med 62(3):188–194. doi:10.1136/oem.2004.013920
Juul-Kristensen B, Sogaard K, Stroyer J, Jensen C (2004) Computer users’ risk factors for developing shoulder, elbow and back symptoms. Scand J Work Environ Health 30(5):390–398
Karasek R (1979) Job demands, job decision latitude, and mental strain: implications for job redesign. Adm Sci Q 24:285–308. doi:10.2307/2392498
Karlqvist LK, Hagberg M, Koster M, Wenemark M, Ånell R (1996) Musculoskeletal symptoms among computer-assisted design (CAD) operators and evaluation of a self-assessment questionnaire. Int J Occup Environ Health 2(3):185–194
Karlqvist L, Bernmark E, Ekenvall L, Hagberg M, Isaksson A, Rostö T (1999) Computer mouse and trackball operation: similarities and differences in posture, muscular load and perceived exertion. Int J Ind Ergon 23:157–169. doi:10.1016/S0169-8141(97)00031-0
Karlqvist L, Wigaeus Tornqvist E, Hagberg M, Hagman M, Toomingas A (2002) Self-reported working conditions of VDU operators and associations with musculoskeletal symptoms: a cross-sectional study focussing on gender differences. Int J Ind Ergon 30:277–294. doi:10.1016/S0169-8141(02)00131-2
Korhonen T, Ketola R, Toivonen R, Luukkonen R, Hakkanen M, Viikari-Juntura E (2003) Work related and individual predictors for incident neck pain among office employees working with video display units. Occup Environ Med 60(7):475–482. doi:10.1136/oem.60.7.475
Kryger AI, Andersen JH, Lassen CF, Brandt LP, Vilstrup I, Overgaard E, Thomsen JF, Mikkelsen S (2003) Does computer use pose an occupational hazard for forearm pain; from the NUDATA study. Occup Environ Med 60(11):e14. doi:10.1136/oem.60.11.e14
Lassen CF, Mikkelsen S, Kryger AI, Brandt LP, Overgaard E, Thomsen JF, Vilstrup I, Andersen JH (2004) Elbow and wrist/hand symptoms among 6, 943 computer operators: a 1-year follow-up study (the NUDATA study). Am J Ind Med 46(5):521–533. doi:10.1002/ajim.20081
Lindegård A, Karlberg C, Wigaeus Tornqvist E, Toomingas A, Hagberg M (2005) Concordance between VDU-users’ ratings of comfort and perceived exertion with experts’ observations of workplace layout and working postures. Appl Ergon 36:319–325. doi:10.1016/j.apergo.2004.12.004
Lundberg U (2002) Psychophysiology of work: stress, gender, endocrine response, and work-related upper extremity disorders. Am J Ind Med 41(5):383–392. doi:10.1002/ajim.10038
Marcus M, Gerr F, Monteilh C, Ortiz DJ, Gentry E, Cohen S, Edwards A, Ensor C, Kleinbaum D (2002) A prospective study of computer users: II. Postural risk factors for musculoskeletal symptoms and disorders. Am J Ind Med 41(4):236–249. doi:10.1002/ajim.10067
Melin B, Wigaeus Tornqvist E (2005) Are psychosocial working conditions related to neck- and shoulder pain? In: Gustafsson R, Lundberg I (eds) Worklife and Health in Sweden 2004. National institute for Working Life, Swedish Work Environment Authority, Stockholm, pp 131–157
Mikkelsen S, Vilstrup I, Lassen CF, Kryger AI, Thomsen JF, Andersen JH (2007) Validity of questionnaire self-reports on computer, mouse and keyboard usage during a four-week period. Occup Environ Med 64(8):541–547. doi:10.1136/oem.2005.026351
Norman K, Nilsson T, Hagberg M, Wigaeus Tornqvist E, Toomingas A (2004) Working conditions and health among female and male employees at a call center in Sweden. Am J Ind Med 46:55–62. doi:10.1002/ajim.20039
Norman K, Floderus B, Hagman M, Toomingas A, Wigaeus Tornqvist E (2008) Musculoskeletal symptoms in relation to work exposures at call centre companies in Sweden. Work 30:201–214
Palm P, Hansson Risberg E, Mortimer M, Palmerud G, Toomingas A, Wigaeus Tornqvist E (2007) Computer use, neck and upper extremity symptoms, eyestrain, and headache among female and male upper secondary school students. Scand J Work Environ Health Suppl 3:33–41
Rempel DM, Krause N, Goldberg R, Benner D, Hudes M, Goldner GU (2006) A randomised controlled trial evaluating the effects of two workstation interventions on upper body pain and incident musculoskeletal disorders among computer operators. Occup Environ Med 63(5):300–306. doi:10.1136/oem.2005.022285
Rothman KJ, Greenland S (1998) Modern Epidemilology, 2nd edn. Lippincott-Raven Publishers, Philadelpia
Sluiter JK, Rest KM, Frings-Dresen MH (2001) Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorders. Scand J Work Environ Health 27(Suppl 1):1–102
Theorell T (1996) Possible mechanisms behind the relationship between the demand-control-support model and disorders from the locomotor system. In: Moon SD, Sauter SL (eds) Beyond biomechanics. Psychosocial aspects of musculoskeletal disorders in office work. Taylor & Francis, London, pp 65–73
Theorell T, Perski A, Akerstedt T, Sigala F, Ahlberg-Hulten G, Svensson J, Eneroth P (1988) Changes in job strain in relation to changes in physiological state. A longitudinal study. Scand J Work Environ Health 14(3):189–196
Toomingas A, Theorell T, Michélsen H, Nordemar R, Stockholm MUSIC I Study Group (1997) Associations between self-rated psychosocial work conditions and musculoskeletal symptoms and signs. Scand J Work Environ Health 23(2):130–139
Veierstedt KB, Nordberg T, Waerstedt M (2006) A critical review for a causal relationship between computer work and musculoskeletal disorders with physical findings of the neck and upper extremitiy. Dansk Selskab for Arbejds- og Miljomedicin (DASAM), Copenhagen
Wahlström J, Svensson J, Hagberg M, Johnson P (2000) Differences between work methods and gender in computer muse use. Scand J Work Environ Health 26(5):390–397
Wigaeus Tornqvist E, Kilbom Å, Vingård E, Alfredsson L, Hagberg M, Theorell T, Waldenström M, Wiktorin C, Hogstedt C, MUSIC-Norrtälje Study Group (2001) The influence on seeking care because of neck and shoulder disorders from work-related exposures. Epidemiology 12(5):537–545. doi:10.1097/00001648-200109000-00013
Work Environment Authority Statistics Sweden (2008) Arbetsmiljön 2007 (in Swedish) (The Work Environment in 2007). Work Environment Authority, Statistics Sweden, Stockholm
Acknowledgments
Financial support from the Swedish Council for Working Life and Social Research is greatly acknowledged. We are also grateful to all work sites and subjects who participated and to everybody in the “Epi-mouse group” who contributed with highly qualified work in the data collection.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wigaeus Tornqvist, E., Hagberg, M., Hagman, M. et al. The influence of working conditions and individual factors on the incidence of neck and upper limb symptoms among professional computer users. Int Arch Occup Environ Health 82, 689–702 (2009). https://doi.org/10.1007/s00420-009-0396-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-009-0396-7