
Abstract
Introduction
Identifying risk factors associated with the development of work-related neck pain in office workers is necessary to facilitate the development of prevention strategies that aim to minimise this prevalent and costly health problem. The aim of this systematic review is to identify individual worker (e.g., lifestyle activity, muscular strength, and posture) and workplace (e.g., ergonomics and work environment) physical factors associated with the development of non-specific neck pain in office workers.
Methods
Studies from 1980 to 2016 were identified by an electronic search of Pubmed, CINAHL, EMBASE, Psychlnfo and Proquest databases. Two authors independently screened search results, extracted data, and assessed risk of bias using the epidemiological appraisal instrument (EAI). A random effect model was used to estimate the risk of physical factors for neck pain.
Results
Twenty papers described the findings of ten prospective cohort studies and two randomized controlled trials. Low satisfaction with the workplace environment (pooled RR 1.28; CI 1.07–1.55), keyboard position close to the body [pooled RR 1.46; (CI 1.07–1.99)], low work task variation [RR 1.27; CI (1.08–1.50)] and self-perceived medium/high muscular tension (pooled RR 2.75/1.82; CI 1.60 /1.14–4.72/2.90) were found to be risk factors for the development of neck pain.
Conclusions
This review found evidence for a few number of physical risk factors for the development of neck pain, however, there was also either limited or conflicting factors. Recommendations for future studies evaluating risk factors are reported and how these may contribute to the prevention of neck pain in office workers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-specific neck pain is a diagnosis often attributed to neck pain of postural and mechanical origin (Côté et al. 2004; Hansson and Hansson 2005). It is a common problem in society and the workplace with two-thirds of individuals affected at some point in their life (Côté et al. 2004; Manchikanti et al. 2009; Haldeman et al. 2010). Office workers have a higher annual prevalence (ranged 17.7–63%) and incidence (ranged 34–49%) of neck pain than other occupations (Korhonen et al. 2003; Sillanpaa et al. 2003; Côté et al. 2004; Wahlstrom et al. 2004; Janwantanakul et al. 2008; Cote et al. 2009; Hush et al. 2009). This condition places a significant burden on both the individual with neck pain and industry due to the costs associated with treatment, reduced productivity and work absenteeism (Hansson and Hansson 2005; Cote et al. 2009; Van Eerd et al. 2011). A study conducted in Sweden found that almost 10% of a sample of office workers (n = 1283) reported reduced productivity due to musculoskeletal symptoms with the neck (33.3%) and shoulder regions (13.8%) being the most commonly reported sites (Hagberg et al. 2002). Neck pain can also result in long periods of work absenteeism (Cote et al. 2013) with a study in the Netherlands reporting 17% of the working population taking sick leave due to neck/shoulder pain at some point over a 2-year period (Burdorf et al. 1998). In light of the rising prevalence and incidence of neck pain and escalating costs due to direct (e.g., treatment costs) and indirect (e.g., loss of productivity) health care costs (Hansson and Hansson 2005), it is not surprising that work-related neck pain is a research priority (Hoy et al. 2014).
Numerous studies have evaluated treatment strategies to resolve the symptoms of neck pain. However, more recently, there has been a shift towards the prevention of neck pain (primary prevention), or the prevention of recurrence of neck pain (secondary prevention) (Leyshon et al. 2010; Aas et al. 2011; Andersen et al. 2011; Hoe et al. 2012; Kay et al. 2012; Bertozzi et al. 2013). This distinction is relevant as the Neck Pain Task Force (Guzman et al. 2008) has defined neck pain as an episodic and recurrent disorder potentially affecting individuals through their lifespan. It is reported that greater than 60% of workers experience another episode of neck pain within 1 year of their initial episode (Carroll et al. 2009). Van Erd et al. showed that 14.2% of workers that make health claims due to neck pain will have multiple episodes of work absenteeism due to recurrence of the disorder within two years of their initial claim (Van Erd et al. 2011). This has led some investigators to identify risk factors for the development of neck pain in office workers (Korhonen et al. 2003; Wahlstrom et al. 2004; Hannan et al. 2005; Tornqvist et al. 2009; Sihawong et al. 2014).
Workplace psychosocial factors (recorded from self-reported questionnaires) have been shown to be strong predictors for the development of neck pain in office workers (Linton 2000; McLean et al. 2010; Kraatz et al. 2013). In particular high job strain (high job demand and low job support) has consistently been identified as a significant risk factor for the development of neck pain in office workers (adjusted RR 2.15, 95% CI 1.16–3.99) (Tornqvist et al. 2009). A recent systematic review demonstrated a causal relationship between high job strain and low social support, with reported neck/shoulder complaints in office workers (Kraatz et al. 2013). While psychosocial risk factors have received some attention in the literature, other potential risk factors for the development of neck pain specific to the office worker have not been comprehensively explored. In particular, Cote and colleagues have identified that quantifiable, and potentially modifiable, physical risk factors may be relevant to the development of neck pain in the general work population. As such the focus of this systematic review will be on the identification of physical risk factors (e.g., ergonomic, workplace physical environment, worker physique, time-related work behaviour) specific to the development of neck in office workers.
There has been some attention in the literature regarding the relationship between physical factors in the workplace, and the physical condition of the individual (e.g., strength, flexibility, physical activity during leisure time and posture), and the development of neck pain. Some of these studies have been specific to office workers while others have not. For example sustained sitting, mostly associated with computer use, have been linked with the rising prevalence and incidence of neck pain in office workers (Gerr et al. 2002; Andersen et al. 2008; Cote et al. 2009; Tornqvist et al. 2009). A national based study of 5400 office workers in the Netherlands found computer use for more than 6 h/day was associated with an 88% increased chance of developing neck pain, compared to individuals using computers less than 2 h/day (Blatter and Bongers 2002). Other physical risk factors identified for the development of neck pain in the workplace include the inappropriate placement of computer devices such as monitor, keyboard and mouse (Marcus et al. 2002; Kiss et al. 2012; Darivemula et al. 2016). Several studies have also reported physical inactivity during leisure time as a risk factor for neck pain (Korhonen et al. 2003; Brandt et al. 2004; Huysmans et al. 2012a).
To date, only one systematic review has specifically investigated physical risk factors for the development of neck pain, but that review was in the general population (Ariens et al. 2000). While this previous systematic review identified a positive relationship between physical factors (excessive neck extension, twisting/bending of the trunk) and neck pain, the findings of the review were based on low quality cross-sectional studies and were not specific to office workers. As a number of longitudinal studies in office workers have been conducted over the past decade (Wahlstrom et al. 2004; Hagberg et al. 2007; Lapointe et al. 2009, 2013; Tornqvist et al. 2009; Ijmker et al. 2011; Huysmans et al. 2012a, b; Lindegard et al. 2012; Paksaichol et al. 2014; Shahidi et al. 2015; Sitthipornvorakul et al. 2015), it now seems timely to undertake a systematic review addressing physical risk factors for the development of neck pain specific to office workers. Therefore, the purpose of this systematic review was to identify physical workplace and individual risk factors for the onset and development of non-specific neck pain in office workers.
Methods
Literature search
This study followed the PRISMA statement for reporting systematic reviews (Moher et al. 2009). An electronic database search was conducted in April 2014 by the first author (DJ) using PubMed, CINAHL, EMBASE, Psycinfo and Proquest databases from January 1980 to April 2014. An updated search was completed in April 2016 for the period of 2014 to 2016 using the same search strategy. The search strategy consisted of a combination of keywords including neck pain, office workers, and physical risk factors (“Appendix A”). The reference list of included studies and relevant systematic reviews were also screened for any potentially eligible studies missed by the database search.
Inclusion criteria
Prospective studies [cohort and randomised controlled trials (RCT)] were included if they met the following inclusion criteria; (1) recruited a cohort of office workers without neck pain at baseline (2) office workers primary role was computer-based (3) measured at least one physical risk factor at baseline (workplace physical factors or individual worker physical factors) (4) assessed the onset of neck pain as an outcome (5) reported the association and strength of association between the physical risk factor and the development of neck pain (e.g., odds ratio (OR) or hazard ratio (HR)), and (6) full-text articles published in English.
Definition of outcome: neck pain
The variable of interest in this review was the onset of an episode of neck pain that could include a first episode or a recurrent episode after at least a 3-month absence of symptoms. There is significant variation in how a new episode of neck pain is defined in previous studies. Some studies define ‘episode’ by the duration of painful symptoms (e.g., >7 days) (Jensen 2003), severity of painful symptoms (based on pain visual analogue scale) (Gerr et al. 2000), or pain that results in activity limitations (Lapointe et al. 2009). To ensure the inclusion of all relevant studies in this systematic review, we included those studies that reported episodes of neck pain/symptoms in office workers over the study period irrespective of the duration or severity of symptoms. Specific details regarding the operational definition of neck pain used in each study is provided in Table 1.
Definition of physical risk factors
A physical risk factor was defined as either workplace physical factors (an attribute of the workplace environment/ergonomic setting and work practices) or individual worker physical factors (physical condition of the worker or physical activity). Potential workplace environment/ergonomic setting risk factors are those variables such as keyboard position, monitor height, and temperature/lightning/acoustic condition of the room. Work practices are those which influence how the work or task is performed, and includes variables such as posture and duration of computer devices use (Gerr et al. 2000; Van Eerd et al. 2012). Potential risk factors associated with physical condition of the worker and physical activity may include muscle strength and flexibility, frequency of leisure activity.
Risk of bias assessment
The risk of bias of included studies was independently assessed by two reviewers (DJ, ZM) using the Epidemiological Appraisal Instrument (EAI) appropriate for cohort (prospective and retrospective), intervention (randomized and non-randomized), case-control, cross-sectional, and hybrid studies (e.g., nested case–control) (Genaidy et al. 2007). The instrument tool comprises 43 questions categorized into five domains of risk of bias: (1) reporting (17 items), (2) subject/record selection (seven items), (3) measurement quality, (4) data analysis (seven items), and (5) generalization of results (two items).
For each item on the list, a study was rated on the following levels: “yes” (verifies the information is complete); “partial” (verifies the information is partially complete); “no” (verifies the information is not described but should have been provided); “unable to determine” (when the provided information is unclear or insufficient to answer the question); and “Not applicable” (absent of the item). Except for the score for “not applicable” response, all scores for each items in the same categories made up the average of the scores for each measurement scale (yes = 2, partial = 1, no/unable to determine = 0). The average scores of the 43 items defined the level of quality of the study, ranging from 0 to 2 with three levels of quality; high quality (low bias) (≥1.4), moderate quality (moderate bias) (1.1 to <1.4), or poor quality (serious bias) (<1.1). Any disagreement with the quality assessment scores was resolved with discussion between the two authors.
Data extraction
Data extraction was performed by one reviewer (DJ) and checked for accuracy by a second reviewer (ZM). Data extracted from eligible studies included publication details (author, year, place of study), participant demographics (age, sex, sample size, participation rate, drop-out rate), study methods (follow-up duration, case definition, analysis method, covariates administration), and assessed risk factors (see Table 1). The estimate of effect size (e.g. odds ratios) and the standard error of the effect size (e.g. 95% confidence intervals) for each physical factor were extracted for data synthesis. Contact with authors was made if further information regarding a study was required.
Statistical methods
The reliability of the risk of bias assessment scores between the two assessors was examined by κ Statistics using SPSS V.22 software (Chicago, IL. 2013) in which greater than 0.81 kappa value was considered as almost perfect (Landis and Koch 1977). Data management and data analysis for meta-analysis were executed with Review Manager 5.3 (The Nordic Cochrane Centre. 2014). A random effect model was chosen because of the variability between study definitions for physical factors and neck pain. The statistically significant heterogeneity among studies was assessed by Chi square value test indicating heterogeneity when p values were lower than 0.05. In addition higher I 2 values supplemented a solely expected chance of variability among studies (range 0–100%).
Studies reporting adjusted risk estimates (adjusted for relevant covariates as determined by authors and reviewers) were included in the analysis. This strategy of study selection is recommended in the Cochrane Handbook (Chap. 13. 6. 2.2. Combining studies) to minimize confounding between dependent and independent variables. Hazard ratios were reported as the common measure of risk estimate in the studies; however, odds ratios were also derived from the few studies. As odds ratio’s tend to be an overestimate (odds ratio is always higher than risk ratio when the value is greater than 1, and it is always smaller than risk ratio when the value is smaller than 1) (Zhang and Yu 1998; Di Lorenzo et al. 2014), odds ratios were converted to risk ratio (RR) format for meta-analysis (Wang 2013). Hazard ratios tend to be similar to risk ratio values when calculated over a similar time period (Zhang and Yu 1998; Spruance et al. 2004; van Dooren et al. 2013; van de Vorst et al. 2016) and therefore were included in the meta-analysis. When exposure group were divided in multiple levels of exposure categories, the alternative combining method proposed by Hamling et al. (2008) was used to generate a combined risk estimate. For double reported risk estimate in different studies but from the same cohort group, the less significant risk estimate was chosen for meta-analysis. Summary statistics for the meta-analysis were, therefore, presented in the form of adjusted risk ratio with a 95% confidence intervals. Pooled risk estimates (e.g., RR) of >1 indicate negative effects of physical factors, while RR < 1 indicate positive effects of physical factors. The effect size was defined as small (<1.25 but >1 or >0.8 but <1), medium (1.25–2 or 0.5–0.08), large (>2 or <0.5) (Cohen 1988).
Pooled summary estimates were not appropriate for some physical factors due to heterogeneity between studies due to different exposure measurement use, different study period, or single study existence. For studies not included in the meta-analysis, a narrative synthesis was performed.
Strength of evidence
To determine the level of evidence for each physical factor (Van Tulder et al. 2003; McLean et al. 2010; Dowling et al. 2014) they were defined as; (1) strong evidence: pooled results obtained from three or more studies with minimum of two high quality studies (statistically homogenous) or consistent findings from narrative synthesis in multiple high-quality studies, (2) moderate evidence: statistically significant pooled results obtained from multiple studies with at least one high quality study (statistically homogenous) or consistent findings from narrative synthesis in multiple studies including at least one high quality study, (3) limited evidence: findings from one high quality study or consistent findings from multiple moderate quality study or low quality studies, (4) very limited evidence: findings from one moderate quality study or one low quality study (5) conflicting evidence: inconsistent findings with regardless of study quality, (6) no evidence: insignificant pooled results derived from multiple studies in which statistical heterogeneous found with regardless of quality.
Results
Study selection
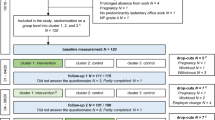
The electronic database search yielded a total of 5952 citations (Fig. 1). Initial screening excluded 3950 citations through the identification of irrelevant key words such as animal, rheumatism, and cancer. The title and abstract of the remaining 2002 citations were screened independently by two reviewers (Kappa = 0.90; 95% CI 0.864–0.926) with 45 articles remaining for full text review. A further 25 papers were excluded when the full text articles were reviewed (kappa = 0.648; 95% CI 0.426–0.870). The remaining 20 papers described the findings of the ten prospective cohort studies (Marcus et al. 2002; Jensen 2003; Korhonen et al. 2003; Brandt et al. 2004; Wahlstrom et al. 2004; Hagberg et al. 2007; Andersen et al. 2008; Hush et al. 2009; Lapointe et al. 2009, 2013; Tornqvist et al. 2009; Ijmker et al. 2011; Huysmans et al. 2012a, b; Lindegard et al. 2012; Paksaichol et al. 2014; Shahidi et al. 2015; Sitthipornvorakul et al. 2015) and two prospective randomised controlled trial (Sihawong et al. 2014; Gerr et al. 2005). Papers reporting the same cohort of participants were grouped and referenced as a single cohort as follows; cohort 1 (Wahlstrom et al. 2004; Tornqvist et al. 2009; Lindegard et al. 2012; Hagberg et al. 2007), cohort 2 (Hush et al. 2009), cohort 3 (Jensen 2003), cohort 4 (Lapointe et al. 2009, 2013), cohort 5 (Andersen et al. 2008; Brandt et al. 2004), cohort 6 (Ijmker et al. 2011; Huysmans et al. 2012a, b), cohort 7 (Marcus et al. 2002), cohort 8 (Korhonen et al. 2003), cohort 9 (Paksaichol et al. 2014; Sitthipornvorakul et al. 2015), cohort 10 (Gerr et al. 2005), cohort 11 (Shahidi et al. 2015), cohort 12 (Sihawong et al. 2014) (Table 1: Characteristics of included studies).

Study selection procedure. Flow diagram depicting the process for selection of studies included in the systematic review
Description of the studies
Studies varied in terms of location, years, and population size. The publication years of included studies ranged from 2002 to 2016. Three cohort studies were conducted in USA, two in Denmark, and one each in Sweden, Australia, Canada, Netherland, Finland, and Thailand. Table 1 presents the characteristics of study population, participant rates, length / frequency of follow-up, and drop-out rates. The number of office workers in the studies ranged from 53 (Hush et al. 2009) to 6943 (Brandt et al. 2004) participants. Four cohort studies enrolled more than 1000 subjects, and five cohort studies achieved more than 200 subjects. The lowest participation rate was 27% (cohort 6); however, the majority of studies (63.6%) achieved more than 50% participation rates. The shortest follow-up period was 10 months (cohort1) and the longest follow-up period was 3 years (cohort 4). Multiple follow-up methods (e.g., monthly or weekly) were chosen by cohort 1, cohort 2, cohort 5, cohort 6, cohort 7, cohort 9, cohort 10, cohort 11, and cohort 12 for the outcome measure. The follow-up response rate in the studies ranged from 51% (cohort 6) to 100% (cohort 2).
Risk of bias
Risk of bias assessment using the EAI showed the majority of the studies rated as high quality. Thirteen studies of the included 20 studies were rated as high quality (Marcus et al. 2002; Jensen 2003; Korhonen et al. 2003; Gerr et al. 2005; Lapointe et al. 2009, 2013; Ijmker et al. 2011; Huysmans et al. 2012a, b; Paksaichol et al. 2014; Sihawong et al. 2014; Shahidi et al. 2015; Sitthipornvorakul et al. 2015), and seven studies were classified as moderate quality (Hush et al. 2009; Brandt et al. 2004; Wahlstrom et al. 2004; Hagberg et al. 2007; Andersen et al. 2008; Tornqvist et al. 2009; Lindegard et al. 2012). The quality scores ranged from 1.11 to 1.76 (out of a possible score of 2.0) (see “Appendix B”). The inter-rater reliability of the two assessors overall (all 860 decisions) demonstrated substantial agreement (κ = 0.69, 95% CI 0.65–0.74) (Landis and Koch 1977). Over each of the 43 items, 20 items had perfect agreement (>80%), 18 items had substantial agreement (61–80%), and 5 items had moderate agreement (41–60%; item 19, 21, 25, 26 and 42, 43) (“Appendix B”: Results of quality assessment).
Measurement of physical risk factors (workplace and individual worker)
The physical risk factors identified from included studies are reported in Table 2. Nine cohort studies and one RCT reported a relationship between at least one workplace physical factor and the onset of neck pain, and seven cohort studies and another RCT showed a relationship between the individual worker physical factors and neck pain. Self-report questionnaires were the most widely used measurement of physical risk factors (cohorts 1–6, 8–9). Six cohort studies (cohorts 2, 5, 6, 7, 9, 11) objectively measured individual worker and workplace physical factors (isometric muscle endurance, cervical range of motion, and neurophysiological deficient, working posture, and duration of computer device use). It should be noted that while most studies account for psychosocial factors as covariates in analysis, two cohorts (cohort 4 and 9) use combined risk categories (e.g., high postural risk/high job strain) in their final regression models.
Identification of a new episode of neck pain
There was large variation between studies in the definition of a new episode of neck pain (Table 1: Characteristics of included studies). Identification of a new episode of neck pain was defined by self-reported neck pain intensity level (e.g., pain greater than 3 on a 0–10 pain scale or medication use for relief) in three cohorts (cohorts 6, 7, 10) with two of these cohorts additionally confirming pain localized to the cervical spine via a physical examination (cohorts 7, 10). A new episode of neck pain was defined by self-reported duration of neck pain (e.g., pain lasting more than 7 days during preceding year) in four cohorts (cohort 1, 2, 3, 8), and by a combination of duration and intensity of neck pain in other cohorts (cohort 9 and 12—pain lasting more than 24 h with greater than 3 on a 0–10 pain scale). Functional limitations associated with neck pain were also used to define an episode of neck pain in two cohorts (cohort 4, 11).
Statistics describing risk associated with physical variables and the onset of neck pain
Five cohorts reported adjusted Hazard Ratios (cohorts 1, 2, 5, 7, 10) for the time-dependent risk of physical factors and the onset of neck pain. Seven cohorts reported adjusted Odds Ratio (cohorts 3, 4, 6, 8, 9, 11, 12) or for the cumulative absolute risk of physical factors for the onset of neck pain.
Meta-analysis
Eight cohorts (cohorts 1–3, 5–7–9) were included in the meta-analysis and pooled summary estimates of risk factors for the development of neck pain in office workers were calculated for variables; satisfaction/comfort of work environment, screen height, close keyboard position, insufficient work breaks, duration of mouse use, duration of keyboard use, duration of computer use, low work task variation and self-perceived muscular tension.
Workplace physical factors
The summary of pooled risk ratio for eight workplace physical factors are reported in Table 2. Three significant relationships were found for workplace physical factors. Specifically, an increased risk of developing neck pain in those with lower satisfaction/comfort with their workplace environment (Pooled RR 1.28 (CI 1.07–1.55), I 2 0%) (Fig. 2.1) (Korhonen et al. 2003; Tornqvist et al. 2009; Huysmans et al. 2012a), and close keyboard position to the body (RR 1.46 (CI 1.07–1.99), I2 0%) (Fig. 2.2) (Korhonen et al. 2003; Marcus et al. 2002) were found. Another meta-analysis showed that low work task variation to have a medium adverse effect on the development of neck pain (RR 1.27 (CI 1.08–1.50), I 2 = 0%) (Tornqvist et al. 2009; Huysmans et al. 2012a). However, screen height above eye level showed no significant effect on the development of neck pain (polled OR of 1.12 (CI 0.88–1.42), I 2 37%) (Jensen 2003; Huysmans et al. 2012a). Another four meta-analyses included workplace physical factors (duration of computer use, mouse use, keyboard use, and work break time) showing no effect on the development of neck pain (Fig. 2.4–7) (Brandt et al. 2004; Tornqvist et al. 2009; Huysmans et al. 2012a, b).


2.1–2.8 Represent risk ratio of each workplace physical factor for the development of neck pain for individual studies and pooled analysis based on random effects model. Individual risk ratio (95% CI) by each study is denoted by rectangular box. The pooled risk ratio for each physical factor is represented by a diamond box, where diamond width corresponds to 95% CI bounds. Boxes heights are inversely proportional to precision of the risk estimation. 2.1 Forest plot for the risk of low satisfaction/comfort of workplace environment on the development of neck pain from pooled analysis of three studies. 2.2 Forest plot for the risk of close keyboard position to worker’s body on the development of neck pain from pooled analysis of two studies. 2.3 Forest plot for the risk of screen height above eye level compare to lower or at eye level on the development of neck pain from pooled analysis of two studies. 2.4 Forest plot for the risk of longer than 3 h of mouse use per day on the development of neck pain from pooled analysis of three studies. 2.5 Forest plot for the risk of longer than 3 h of keyboard use per day on the development of neck pain from pooled analysis of two studies. 2.6 Forest plot for the risk of longer than 4 h of computer use per day on the development of neck pain from pooled analysis of three studies. 2.7 Forest plot for the risk of prolonged work without frequent break on the development of neck pain from pooled analysis of three studies. 2.8 Forest plot for the risk of low work task variations on the development of neck pain from pooled analysis of two studies
Individual worker physical factors
High or medium self-perceived muscular tension during computer use had a large adverse effect on the development of neck pain (High tension: RR of 2.75 (CI 1.60–4.72), I 2 74%; medium tension: RR of 1.82 (CI 1.14–290), I 2 79%) (Fig. 3) and these findings were concluded as strong evidence (Wahlstrom et al. 2004; Huysmans et al. 2012b; Paksaichol et al. 2014).

3.1, 3.2 Represent risk ratio of each individual physical factor for the development of neck pain for individual studies and pooled analysis based on random effects model. Individual risk ratio (95% CI) by each study is denoted by rectangular box. The pooled risk ratio for each physical factor is represented by a diamond box, where diamond width corresponds to 95% CI bounds. Boxes heights are inversely proportional to precision of the risk estimation. 3.1 Forest plot for the risk of self-perceived high intensity muscular tension on the development of neck pain from pooled analysis of three studies. 3.2 Forest plot for the risk of self-perceived medium intensity muscular development of neck pain from pooled analysis of three studies
Narrative synthesis for studies not included in meta-analysis
Workplace physical factors
Moderate evidence for each long duration of mouse use and keyboard use (recorded by a software programme) were concluded showing no effect on the development of neck pain (Brandt et al. 2004; Andersen et al. 2008; Ijmker et al. 2011). Another moderate evidence was found for the performance of repetitive or precision work on the development of neck pain, however the association was not significant (Wahlstrom et al. 2004; Huysmans et al. 2012a). Majority of workplace physical factors, e.g., placement of mouse, and chair arm rest, were investigated by a single study, resulted in limited evidence for its risk relationship with neck pain (Table 2).
Individual worker physical factors
There was strong evidence for the frequency of physical activity in leisure time showing no effect on the development of neck pain (Korhonen et al. 2003; Brandt et al. 2004; Hush et al. 2009; Huysmans et al. 2012a; Shahidi et al. 2015). Although a large prevention effect of frequent leisure activity on the development of neck pain (OR 0.44 CI 0.21–0.089) was reported in one study (Shahidi et al. 2015), another four studies found no effect of leisure activity on the development of neck pain (Korhonen et al. 2003; Brandt et al. 2004; Hush et al. 2009; Huysmans et al. 2012a) (Table 2). The effect of physical condition of worker was investigated by only two cohorts (cohort 2 and cohort 11) that reported greater range of cervical flexion/extension motion (HR 0.97 CI 0.94–0.97) (Hush et al. 2009), longer isometric cervical extensor endurance (OR 0.92 CI 0.87–0.97), efficient diffuse noxious inhibitory control (OR 0.90 CI 0.83–0.98) (Shahidi et al. 2015), and specified cervical muscle endurance exercise (HR 0.45 CI 0.28–0.71) (Tornqvist et al. 2009) had prevention effect on the development of neck pain (Table 2). However, those relationships were concluded as limited or very limited evidence due to insufficient number of studies.
Discussion
The findings of the meta-analysis indicate that self-perceived muscular tension, low levels of satisfaction/comfort with workplace environment, close keyboard position to the body, as well as low task variation, represented significant physical risk factors for the development of neck pain in office workers. However, a series of meta-analyses revealed no association between longer duration of computer device use (mouse and keyboard), break time and the development of neck pain. This finding of no effect of prolonged computer use is supported by the finding from the narrative synthesis in this review (software programme analysis). The strong evidence for the frequency of physical activity is derived from the narrative synthesis reporting no effect on the development of neck pain.
Comparison with previous reviews and literatures
A number of reviews with general or working populations have identified risk factors for neck pain (Hales and Bernard 1996; Ariens et al. 2000; McLean et al. 2010; Paksaichol et al. 2012), but only two of them were specifically related to the development of neck pain (McLean et al. 2010; Paksaichol et al. 2012) and only one depicted office worker focused risk factors (Paksaichol et al. 2012). The meta-analysis in this review has revealed new findings with evidence for physical risk factors previously considered as limited in previous reviews.
The strongest relationship with the development of neck pain in this review was self-perceived high muscular tension. This evidence was limited in a previous review due to fewer studies that have investigated this risk factor (Paksaichol et al. 2012). The evidence is further supported by a series of cross-sectional studies which have reported that perceived general tension, encompassing tensed muscles, sweating, hard breathing, and stomach tension, was associated with neck and shoulder symptoms (Vasseljen and Westgaard 1995; Vasseljen et al. 2001; Holte and Westgaard 2002). However, the authors of this review suggest this risk of self-perceived muscular tension for the development of neck pain is difficult to interpret. An intervention study from the same research team found that the physiotherapy and exercise intervention recorded significant reduction of pain and perceived general tension levels compared to pre-intervention, but unchanged muscle activity levels (EMG signals) in shoulder region (Vasseljen et al. 1995). One of their findings also indicated that the perceived tension increased during work and decreased during leisure time with similar time course changes for perceived stress (Holte and Westgaard 2002). This closer association to psychological stress (mental stress) rather than biological stress (EMG) may support that the perceived general tension correlates with individual psychosocial factors (Vasseljen and Westgaard 1995; Hales and Bernard 1996). Therefore, we contend that reported self-perceived muscular tension is a symptom, commonly reported in association with neck pain and raised level of mental stress, which may explain its strong relationship with the dependent variable of neck pain. It is acknowledged, however, that it may be a physical precursor to a more significant neck problem which may prompt the individual to seek remediation.
Low satisfaction or comfort with the workplace environment was also identified by the meta-analysis to have a medium adverse effect for the development of neck pain in office workers. The workplace environment was rated by workers and dichotomized into “unsatisfied” and “satisfied” using the total score from each component (e.g., lighting condition, room temperature, quality of the air, size of the working room, and acoustic conditions). This factor has been identified in previous reviews as potentially problematic but no definitive conclusions could be made due to a lack of study (Paksaichol et al. 2012). This review found strong evidence with two high quality studies and one moderate quality study for low satisfaction with ones workplace as a risk factor. Despite this finding, the validity of this subjective rating by subjects is questionable. Only one of the three studies used a validated tool to measure level of satisfaction to workstation environment and therefore may have resulted in a biased estimate. Future studies using validated measures are required to confirm this result however it does highlight the potential importance of the work environment as a predictor for the development of neck pain.
In this review, having the keyboard close to the body (less than 15 cm) was revealed as a moderate evidence which was reported as limited evidence in the previous review (Paksaichol et al. 2012). This finding is supported by several studies. Kotani et al. found that having the keyboard close to the body required greater ulnar deviation, wrist flexion, shoulder elevation, internal shoulder rotation and greater elbow flexion (Kotani et al. 2007). This altered position of upper arm may potentially create discomfort at the shoulder/neck region. The narrow space on the desk due to close keyboard position is also associated with the limited area of support for the upper arms on the desk, enabling the user to generate less torque for shoulder abduction and flexion during typing task (Onyebeke et al. 2014). A reduced incidence of neck pain (adjusted HR 0.49 CI 0.24–0.97) and significant reduction of right upper extremity discomfort were reported in an intervention group of workers being addressed a wide arm-board to support the forearms during computer work (Rempel et al. 2006; Conlon et al. 2008). Additionally, Marcus et al. in this review, characterized placement of computer devices in relation to body posture. They found that a specific angular posture may decrease or increase the risk of new episode of neck pain. For example, greater than 121° inner elbow angle when typing was shown to be less likely develop a new onset of neck pain (adjusted HR 0.16 CI 0.04–0.62) while smaller than 137° inner elbow angle when mouse use more likely develops the new onset of neck pain (adjusted HR 1.67 CI 1.09–2.55). Taken together, inadequate equipment location can negatively impact on the working posture of sufficient intensity to induce new onset of neck pain.
Low work task variation during the working day was firstly revealed as a risk factor for the development of neck pain in this review (Tornqvist et al. 2009; Huysmans et al. 2012a). Although computer work is regarded as a ubiquitous task in a similar office environment, different tasks that workers complete with a computer vary and require different patterns of movement and muscle activity of the upper extremities (Dennerlein and Johnson 2006). For example, Dennerlein and Johnson found that tasks requiring mouse intensive work (Graphical work or web browsing) were associated with greater shoulder flexion, abduction and external rotation posture while tasks involving keyboard intensive work (typing) were associated with less shoulder movement but greater ulnar deviation (Dennerlein and Johnson 2006). Therefore, performing such tasks for prolonged periods induce sustained low level muscle activity and static posture in specific body regions, resulting in the development of neck pain (Jensen et al. 1993). Quantifying and characterizing variation of work tasks is challenging in field-based research; thus, further investigations in this aspect are required.
Undertaking frequent physical activity has been argued as a preventive factor for neck pain. However, a systematic review of the association between physical activity and neck pain for general population found no association due to limited evidence (Sitthipornvorakul et al. 2011). This is in accordance with the finding of another systematic review within the office worker population (Paksaichol et al. 2012). Our review found that one study showed a strong preventive effect (OR 0.44, CI 0.21–0.89) (Shahidi et al. 2015), while four studies reported no effect of physical activity on the development of neck pain (Korhonen et al. 2003; Brandt et al. 2004; Hush et al. 2009; Huysmans et al. 2012a). Of those four studies, one study (Hush et al. 2009) showed a relatively strong tendency of decreased neck pain (HR 0.64) for the group with frequent physical activities although the relationship was not significant. This discrepancy may exist because of diverse definition for physical activities and different cut-off points for frequency of activities. Therefore, we contend that as the evidence for physical activity on the development of neck pain is insufficient or controversial, future research should be undertaken with a standardized risk assessment.
There were also several factors that showed limited (based on evaluation from single studies) significant evidence of a relationship with the development of neck pain in office workers. Individuals using a telephone shoulder rest were found to be two times more likely to develop neck pain (HR 2.05, CI 1.14–3.71) (Marcus et al. 2002). The interaction between self-reported postural risk and psychosocial risk were associated with a greater risk of neck pain in female workers only (risk estimates are presented in Table 2). Similarly, combined reduced physical activity and high mental stress and less physical activities were presented (cohort 9). The findings from these cohort indicated that adverse psychosocial work environment might affect physical work condition and vice versa. This review did also identify a significant relationship between increased cervical range of motion, greater cervical extensor endurance, and that undertaking a program of neck muscular training (Hush et al. 2009; Sihawong et al. 2014; Shahidi et al. 2015) are all associated with reduced incidence of future neck pain. These findings are consistent with observed improvements in neck pain with rehabilitation programmes aimed to strengthen neck muscles and improve joint mobility (Bertozzi et al. 2013).
Strengths and weakness of the study
This is the first systematic review and meta-analysis specifically addressing physical risk factors for the development of neck pain in office workers. The review summarised the findings of 20 prospective studies, which is the greatest number of studies among reviews in this field. This review also selected strict inclusion criteria for the choice of risk estimates only from confounding adjusted analysis model. Therefore, we could minimize the biased conclusion that can be derived from unadjusted model and have also established less biased evidence for our findings. The purpose of this review was to identify physical risk factors to assist health professionals and researchers to minimise the negative impact of working with computer. It was evident from previous reviews that non-physical factors such as high work demands, low job authorities, and poor social support, female gender, and history of neck pain are strongly predictive of the development of neck pain from the previous reviews (Hales and Bernard 1996; Ariens et al. 2000; Linton et al. 2002; McLean et al. 2010; Kraatz et al. 2013). However, the findings of this review benefit workers as well as policy makers by providing valuable evidence for physical factors.
There were some limitations of this review. We included only studies published in English and as such potential publication and language bias may exist. Additionally, we did not report crude factor-outcome relationships which may have additional meaningful information for the relationship with the development of neck pain. There were some methodological issues in combining the findings of multiple studies. Inconsistency and a lack of standardisation between studies regarding the assessment and measurement of variables and outcome, hindered data synthesis, as a result, this review was able to conclude only five strong and seven moderate evidences for physical factors. The 42 investigated risk factors in the previous studies have been still remained limited evidence.
Implications
Future studies need to incorporate a more comprehensive range of potential physical risk factors with standardized methods of measurement to further clarify of physical risk factors for the development of neck pain in office workers. This review indicates that low satisfaction with the physical work environment, close keyboard position to the body, low work task variation, as well as perceived muscular tension are predictive for developing a new episode of neck pain in office workers. Yet current evidence is inconclusive with regard to many other potentially important physical workplace and individual variables. Further study in this field is essential as many of these variables are potentially modifiable and therefore informative for the prevention of neck pain in office workers.
Conclusions
Although a number of individual and workplace physical factors were identified as risks for neck pain in this review, there was either limited or conflicting evidence for many of the physical factors previously reported to be a potential risk factor for neck pain in this population. One of the major findings of the study was the paucity of prospective studies investigating the association between the physical work environment, the individuals work practices, physical condition of the worker, and the development of neck pain. Another important finding is the need to develop standardised risk and outcome assessments. Therefore, studies in the future will need to consider more comprehensive physical variables, as well as develop standardised methods for measurement and case definition when investing this area of health care for the integrated preventive of neck pain in office workers.
Appendix A
See Table 3.
Appendix B
See Table 4.
References
Aas RW, Tuntland H, Holte KA, Roe C, Lund T, Marklund S, Moller A (2011) Workplace interventions for neck pain in workers. Cochrane Database Syst Rev (4):Cd008160
Andersen JH et al (2008) Computer mouse use predicts acute pain but not prolonged or chronic pain in the neck and shoulder. Occup Environ Med 65:126–131. doi:10.1136/oem.2007.033506
Andersen JH, Fallentin N, Thomsen JF, Mikkelsen S (2011) Risk factors for neck and upper extremity disorders among computers users and the effect of interventions: an overview of systematic reviews. PloS one 6:e19691. doi:10.1371/journal.pone.0019691
Ariens GA, van Mechelen W, Bongers PM, Bouter LM, van der Wal G (2000) Physical risk factors for neck pain. Scand J Work Environ Health 26:7–19
Bertozzi L, Gardenghi I, Turoni F, Villafane JH, Capra F, Guccione AA, Pillastrini P (2013) Effect of therapeutic exercise on pain and disability in the management of chronic nonspecific neck pain: systematic review and meta-analysis of randomized trials. Phys Ther 93:1026–1036. doi:10.2522/ptj.20120412
Blatter BM, Bongers PM (2002) Duration of computer use and mouse use in relation to musculoskeletal disorders of neck or upper limb. Int J Ind Ergon 30:295–306
Brandt LP, Andersen JH, Lassen CF, Kryger A, Overgaard E, Vilstrup I, Mikkelsen S (2004) Neck and shoulder symptoms and disorders among Danish computer workers. Scand J Work Environ Health 30:399–409
Burdorf A, Naaktgeboren B, Post W (1998) Prognostic factors for musculoskeletal sickness absence and return to work among welders and metal workers. Occup Environ Med 55:490–495
Carroll LJ et al (2009) Course and prognostic factors for neck pain in workers: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther 32:S108–S116. doi:10.1016/j.jmpt.2008.11.015
Cohen J (1998) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, New York
Conlon CF, Krause N, Rempel DM (2008) A randomised controlled trial evaluating an alternative mouse and forearm support on upper body discomfort and musculoskeletal disorders among engineers. Occup Environ Med 65:311–318. doi:10.1136/oem.2006.032243
Cote P et al (2009) The burden and determinants of neck pain in workers: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther 32:S70–S86. doi:10.1016/j.jmpt.2008.11.012
Cote P, Yang X, Kristman V, Hogg-Johnson S, Van Eerd D, Rezai M, Vidmar M (2013) The association between workers’ compensation claims involving neck pain and future health care utilization: a population-based cohort study. J Occup Rehabil 23:547–556. doi:10.1007/s10926-012-9415-8
Côté P, Cassidy JD, Carroll LJ, Kristman V (2004) The annual incidence and course of neck pain in the general population: a population-based cohort study. Pain 112:267–273. doi:10.1016/j.pain.2004.09.004
Darivemula SB, Goswami K, Gupta SK, Salve H, Singh U, Goswami AK (2016) Work-related neck pain among desk job workers of tertiary care hospital in New Delhi, India: burden and determinants. Indian J Community Med 41:50–54
Dennerlein JT, Johnson PW (2006) Different computer tasks affect the exposure of the upper extremity to biomechanical risk factors. Ergonomics 49:45–61. doi:10.1080/00140130500321845
Di Lorenzo L, Coco V, Forte F, Trinchese GF, Forte AM, Pappagallo, M 2014. The use of odds ratio in the large population-based studies: Warning to readers. Muscles, Ligaments Tendons J 4:90–92.
Dowling GJ et al (2014) Dynamic foot function as a risk factor for lower limb overuse injury: a systematic review. J Foot Ankle Res 7:53. doi:10.1186/s13047-014-0053-6
Genaidy AM, Lemasters GK, Lockey J, Succop P, Deddens J, Sobeih T, Dunning K (2007) An epidemiological appraisal instrument - a tool for evaluation of epidemiological studies. Ergonomics 50:920–960. doi:10.1080/00140130701237667
Gerr F et al. (2000) Computer users’ postures and associations with workstation characteristics. AIHAJ 61:223–230
Gerr F et al (2002) A prospective study of computer users: I. Study design and incidence of musculoskeletal symptoms and disorders. Am J Ind Med 41:221–235
Gerr F, Marcus M, Monteilh C, Hannan L, Ortiz D, Kleinbaum D (2005) A randomised controlled trial of postural interventions for prevention of musculoskeletal symptoms among computer users. Occup Environ Med 62:478–487. doi:10.1136/oem.2004.015792
Guzman J et al (2008) A new conceptual model of neck pain: linking onset, course, and care: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine 33:S14–S23. doi:10.1097/BRS.0b013e3181643efb
Hagberg M, Tornqvist EW, Toomingas A (2002) Self-reported reduced productivity due to musculoskeletal symptoms: associations with workplace and individual factors among white-collar computer users. J Occup Rehabil 12:151–162
Hagberg M, Vilhemsson R, Tornqvist EW, Toomingas A (2007) Incidence of self-reported reduced productivity owing to musculoskeletal symptoms: association with workplace and individual factors among computer users. Ergonomics 50:1820–1834. doi:10.1080/00140130701674539
Haldeman S, Carroll L, Cassidy JD (2010) Findings from the bone and joint decade 2000 to 2010 task force on neck pain and its associated disorders. J Occup Environ Med 52:424–427. doi:10.1097/JOM.0b013e3181d44f3b
Hales TR, Bernard BP (1996) Epidemiology of work-related musculoskeletal disorders. Orthop Clin North Am 27:679–709
Hamling J, Lee P, Weitkunat R, Ambuhl M (2008) Facilitating meta-analyses by deriving relative effect and precision estimates for alternative comparisons from a set of estimates presented by exposure level or disease category. Stat Med 27:954–970. doi:10.1002/sim.3013
Hannan LM, Monteilh CP, Gerr F, Kleinbaum DG, Marcus M (2005) Job strain and risk of musculoskeletal symptoms among a prospective cohort of occupational computer users. Scand J Work Environ Health 31:375–386
Hansson EK, Hansson TH (2005) The costs for persons sick-listed more than one month because of low back or neck problems. A two-year prospective study of Swedish patients. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research. Society 14:337–345. doi:10.1007/s00586-004-0731-3
Hoe VC, Urquhart DM, Kelsall HL, Sim MR (2012) Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults. Cochrane Database Syst Rev 8:Cd008570. doi:10.1002/14651858.CD008570.pub2
Holte KA, Westgaard RH (2002) Daytime trapezius muscle activity and shoulder-neck pain of service workers with work stress and low biomechanical exposure. Am J Ind Med 41:393–405. doi:10.1002/ajim.10039
Hoy D et al (2014) The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis 73:1309–1315. doi:10.1136/annrheumdis-2013-204431
Hush JM, Michaleff Z, Maher CG, Refshauge K (2009) Individual, physical and psychological risk factors for neck pain in Australian office workers: a 1-year longitudinal study. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research. Society 18:1532–1540. doi:10.1007/s00586-009-1011-z
Huysmans MA, Ijmker S, Blatter BM, Knol DL, van Mechelen W, Bongers PM, van der Beek AJ (2012a) The relative contribution of work exposure, leisure time exposure, and individual characteristics in the onset of arm-wrist-hand and neck-shoulder symptoms among office workers. Int Arch Occup Environ Health 85:651–666. doi:10.1007/s00420-011-0717-5
Huysmans MA, Blatter BM, van der Beek AJ (2012b) Perceived muscular tension predicts future neck-shoulder and arm-wrist-hand symptoms. Occup Environ Med 69:261–267. doi:10.1136/oemed-2011-100279
Ijmker S, Huysmans MA, van der Beek AJ, Knol DL, van Mechelen W, Bongers PM, Blatter BM (2011) Software-recorded and self-reported duration of computer use in relation to the onset of severe arm-wrist-hand pain and neck-shoulder pain. Occup Environ Med 68:502–509. doi:10.1136/oem.2010.056267
Janwantanakul P, Pensri P, Jiamjarasrangsri V, Sinsongsook T (2008) Prevalence of self-reported musculoskeletal symptoms among office workers. Occup Med (Oxford, England) 58:436–438 doi:10.1093/occmed/kqn072
Jensen C (2003) Development of neck and hand-wrist symptoms in relation to duration of computer use at work. Scand J Work Environ Health 29:197–205
Jensen C, Nilsen K, Hansen K, Westgaard RH (1993) Trapezius muscle load as a risk indicator for occupational shoulder-neck complaints. Int Arch Occup Environ Health 64:415–423
Kay TM et al (2012) Exercises for mechanical neck disorders. Cochrane Database Syst Rev 8:Cd004250. doi:10.1002/14651858.CD004250.pub4
Kiss P, De Meester M, Kruse A, Chavee B, Braeckman, L (2012) Neck and shoulder complaints in computer workers and associated easy to assess occupational factors—a large-scale cross-sectional multivariate study. Int Arch Occup Environ Health 85:197–206
Korhonen T, Ketola R, Toivonen R, Luukkonen R, Hakkanen M, Viikari-Juntura E (2003) Work related and individual predictors for incident neck pain among office employees working with video display units. Occup Environ Med 60:475–482
Kotani K, Barrero LH, Lee DL, Dennerlein JT (2007) Effect of horizontal position of the computer keyboard on upper extremity posture and muscular load during computer work. Ergonomics 50:1419–1432. doi:10.1080/00140130701330587
Kraatz S, Lang J, Kraus T, Munster E, Ochsmann E (2013) The incremental effect of psychosocial workplace factors on the development of neck and shoulder disorders: a systematic review of longitudinal studies. Int Arch Occup Environ Health 86:375–395. doi:10.1007/s00420-013-0848-y
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Lapointe J, Dionne CE, Brisson C, Montreuil S (2009) Interaction between postural risk factors and job strain on self-reported musculoskeletal symptoms among users of video display units: a three-year prospective study. Scand J Work Environ Health 35:134–144
Lapointe J, Dionne CE, Brisson C, Montreuil S (2013) Effort-reward imbalance and video display unit postural risk factors interact in women on the incidence of musculoskeletal symptoms. Work (Reading, Mass) 44:133–143 doi:10.3233/wor-2012-1357
Leyshon R, Chalova K, Gerson L, Savtchenko A, Zakrzewski R, Howie A, Shaw L (2010) Ergonomic interventions for office workers with musculoskeletal disorders: a systematic review. Work (Reading, Mass) 35:335–348 doi:10.3233/wor-2010-0994
Lindegard A, Wahlstrom J, Hagberg M, Vilhelmsson R, Toomingas A, Tornqvist EW (2012) Perceived exertion, comfort and working technique in professional computer users and associations with the incidence of neck and upper extremity symptoms. BMC Musculoskelet Disord 13:38. doi:10.1186/1471-2474-13-38
Linton SJ (2000) A review of psychological risk factors in back and neck pain. Spine 25:1148–1156
Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA (2009) Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Phys 12:E35–E70
Marcus M et al (2002) A prospective study of computer users: II. Postural risk factors for musculoskeletal symptoms and disorders. Am J Ind Med 41:236–249
McLean SM, May S, Klaber-Moffett J, Sharp DM, Gardiner E (2010) Risk factors for the onset of non-specific neck pain: a systematic review. J Epidemiol Community Health 64:565–572. doi:10.1136/jech.2009.090720
Onyebeke LC, Young JG, Trudeau MB, Dennerlein JT (2014) Effects of forearm and palm supports on the upper extremity during computer mouse use. Appl Ergon 45:564–570. doi:10.1016/j.apergo.2013.07.016
Paksaichol A, Janwantanakul P, Purepong N, Pensri P, van der Beek AJ (2012) Office workers’ risk factors for the development of non-specific neck pain: a systematic review of prospective cohort studies. Occup Environ Med 69:610–618. doi:10.1136/oemed-2011-100459
Paksaichol A, Janwantanakul P, Lawsirirat C (2014) Development of a neck pain risk score for predicting nonspecific neck pain with disability in office workers: a 1-year prospective cohort study. J Manipulative Physiol Ther 37:468–475. doi:10.1016/j.jmpt.2014.07.004
Rempel DM, Krause N, Goldberg R, Benner D, Hudes M, Goldner GU (2006) A randomised controlled trial evaluating the effects of two workstation interventions on upper body pain and incident musculoskeletal disorders among computer operators. Occup Environ Med 63:300–306. doi:10.1136/oem.2005.022285
Shahidi B, Curran-Everett D, Maluf KS (2015) Psychosocial, physical, and neurophysiological risk factors for chronic neck pain: a prospective inception cohort study. J Pain 16:1288–1299. doi:10.1016/j.jpain.2015.09.00
Sihawong R, Janwantanakul P, Jiamjarasrangsi W (2014) Effects of an exercise programme on preventing neck pain among office workers: a 12-month cluster-randomised controlled trial. Occup Environ Med 71:63–70. doi:10.1136/oemed-2013-101561
Sillanpaa J, Huikko S, Nyberg M, Kivi P, Laippala P, Uitti J (2003) Effect of work with visual display units on musculo-skeletal disorders in the office environment. Occup Med (Oxford, England) 53:443–451
Sitthipornvorakul E, Janwantanakul P, Purepong N, Pensri P, van der Beek AJ (2011) The association between physical activity and neck and low back pain: a systematic review. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research. Society 20:677–689. doi:10.1007/s00586-010-1630-4
Sitthipornvorakul E, Janwantanakul P, Lohsoonthorn V (2015) The effect of daily walking steps on preventing neck and low back pain in sedentary workers: a 1-year prospective cohort study. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research. Society 24:417–424. doi:10.1007/s00586-014-3577-3
Spruance SL, Reid JE, Grace M, Samore M (2004) Hazard ratio in clinical trials. Antimicrob Agents Chemother 48:2787–2792. doi:10.1128/aac.48.8.2787-2792.2004
Tornqvist EW, Hagberg M, Hagman M, Risberg EH, Toomingas A (2009) The influence of working conditions and individual factors on the incidence of neck and upper limb symptoms among professional computer users. Int Arch Occup Environ Health 82:689–702. doi:10.1007/s00420-009-0396-7
van Tulder M, Furlan A, Bombardier C, Bouter L (2003) Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 28:1290–1299. doi:10.1097/01.brs.0000065484.95996.af
Van Eerd D, Cote P, Kristman V, Rezai M, Hogg-Johnson S, Vidmar M, Beaton D (2011) The course of work absenteeism involving neck pain: a cohort study of Ontario lost-time claimants. Spine 36:977–982. doi:10.1097/BRS.0b013e3181e9b831
Van Eerd D, Hogg-Johnson S, Cole DC, Wells R, Mazumder A (2012) Comparison of occupational exposure methods relevant to musculoskeletal disorders: Worker-workstation interaction in an office environment. J Electromyogr Kinesiol 22:176–185. doi:10.1016/j.jelekin.2011.12.001
van Dooren FE, Nefs G, Schram MT, Verhey FR, Denollet J, Pouwer F (2013) Depression and risk of mortality in people with diabetes mellitus: a systematic review and meta-analysis. PloS one 8:e57058. doi:10.1371/journal.pone.0057058
van de Vorst IE, Koek HL, de Vries R, Bots ML, Reitsma JB, Vaartjes I (2016) Effect of vascular risk factors and diseases on mortality in individuals with dementia: a systematic review and meta-analysis. J Am Geriatr Soc 64:37–46. doi:10.1111/jgs.13835
Vasseljen O Jr, Johansen BM, Westgaard RH (1995) The effect of pain reduction on perceived tension and EMG-recorded trapezius muscle activity in workers with shoulder and neck pain. Scand J Rehabil Med 27:243–252
Vasseljen O, Westgaard RH (1995) A case-control study of trapezius muscle activity in office and manual workers with shoulder and neck pain and symptom-free controls. Int Arch Occup Environ Health 67:11–18
Vasseljen O, Holte KA, Westgaard RH (2001) Shoulder and neck complaints in customer relations: individual risk factors and perceived exposures at work. Ergonomics 44:355–372. doi:10.1080/00140130010008101
Wahlstrom J, Hagberg M, Toomingas A, Wigaeus Tornqvist E (2004) Perceived muscular tension, job strain, physical exposure, and associations with neck pain among VDU users; a prospective cohort study. Occup Environ Med 61:523–528
Wang Z (2013) Converting Odds Ratio to Relative Risk in Cohort Studies with Partial Data Information. J Stat Softw 55:5. doi:10.18637/jss.v055.i05
Zhang J, Yu KF (1998) What is the relative risk?: A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 280:1690–1691. doi:10.1001/jama.28
Review Manager (RevMan) [computer program] (2014) Version 5.3 Copenhagen: the Nordic Cochrane Centre, The Cochrane Collaboration
Moher D, Liberati A, Tetzlaff J, Altman DG, The PG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. doi:10.1371/journal.pmed.1000097
SPSS Inc Version 22.0 Released (2013). PASW Statistics for Windows. Chicago
Acknowledgements
The authors wish to acknowledge all the authors for the included studies in this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Jun, D., Zoe, M., Johnston, V. et al. Physical risk factors for developing non-specific neck pain in office workers: a systematic review and meta-analysis. Int Arch Occup Environ Health 90, 373–410 (2017). https://doi.org/10.1007/s00420-017-1205-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-017-1205-3