
Abstract
Background
Cairo university hospitals are at the heart of Cairo with close proximity to Tahrir (Liberation) square and had received the vast majority of casualties during the Egyptian revolution. The aim of this study was to analyze the eye injuries during the uprising.
Design
Retrospective cohort study.
Methods
Data were obtained from patients’ paper records, interview with treating ophthalmologists, and whenever possible patients were interviewed and examined. An electronic medical template had been specially developed for recording these data. Main outcome measures were the flow of patients and their demographics, diagnoses, visual acuities pre and post interventions, investigations and management. Whenever required results were compared at 95 % confidence interval.
Results
There were 184 patients (mean age 27.3 ± 9.6 years) with 195 injured eyes of whom 96.7 % were males and 11 patients had both eyes injured. Seventy seven percent of patients had been admitted within 24 h of injury. Open globe injuries comprised 87 % of the eyes of which 147 eyes received 259 imaging investigations. The presenting visual acuities were worse than 3/60 in 72.5 % of eyes which were even worse post interventions and that was significantly dependent on the presenting vision. Wound repair was the primary intervention in 85 % of eyes while 50 % of the secondary interventions were vitrectomies.
Conclusions
Presenting visual acuity is a valid prognostic factor in the setting of mass eye casualty. Management of open globe injuries continues to pose difficult challenges especially bilateral ones.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mass casualty is an incident of a sudden and unpredictable occurrence with disruption of societal infrastructure that gives rise to chaos, and an overwhelming of medical resources by the urgent medical needs and sudden presentation of large numbers of casualties [1]. This is much more than just a large emergency. In addition, mass casualty management is neither taught in medical or nursing schools, nor in the training program of residents [4]. The 2011 Egyptian revolution took place following an uprising that started on 25th January 2011. There were up to 840 reported deaths, while injures were over 6000 [4]. Cairo University hospitals (Kasr El Aini) is not just the biggest hospital providing free service to the people of Cairo and Egypt, but also, is the nearest hospital (1 km away) from ‘Tahrir’ (Liberation) square which was the heart of confrontations and incidents, and subsequently casualties during the uprising. The aim of this study is to analyze cases admitted to the Emergency eye service of the Ophthalmology Department-Cairo University Hospitals (Kasr El Aini) during the uprising.
Methods
Patients admitted to Emergency eye service of Cairo University Hospitals during the uprising (from 25th Jan 2011 to 11th Feb of the same year) have been included in this retrospective cohort study. Data were collected by ophthalmologists from patients’ paper records, interviews with treating ophthalmologists, and whenever possible patients were examined and interviewed. An electronic medical template had been specially developed for recording patients’ data. This study was approved regarding Ethics by the Ophthalmology Department, Faculty of Medicine, Cairo University, and was done under the supervision of the same body. Tenets of Helsinki Declaration and the World Medical Association declaration on Ethical considerations regarding Health Database had been respected. Ophthalmologists, who were responsible for data collection, were not involved in analyzing and interpreting the results to avoid performance bias. Data collected include: demographic data, whether or not patients provided their contact details, diagnosis, investigations, whenever possible presenting visual acuity, time lag between patient first presenting to hospital and first seen by an eye doctor, time lag between patient admission to hospital and his primary intervention, primary interventions, secondary and further interventions, and post interventions visual acuity. We also recorded dates of admission during the review period to indentify the amount of patients admitted per day during the 18 days of the uprising.
Data were statistically represented in terms of range, mean, standard deviation (SD) and percentages. Whenever required, comparisons were done using analysis of variance for parametric data. A probability value (P value) less than 0.05 was considered significant. For comparing nonparametric data, chi square test was performed. All statistical calculations were done using computer programs Microsoft Excel version 7 (Microsoft Corporation, NY) and SPSS (Statistical package for the social science) and statistical programs (SPSS Inc., Chicago, IL).
Results
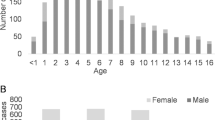
One hundred and eighty four patients, of whom only six were females (3.3 %), had been admitted to the Emergency eye service of Cairo University Hospitals due to eye trauma which had affected one hundred and ninety five of their eyes due to confrontations during the Egyptian uprising. Their age (collected from 138 patients) ranged from 8 to 56 years (mean 27.3 ± 9.6). Only 81 patients (44 %) had provided their contact details either because they were afraid to provide their details to avoid being chased by secret police or they just didn’t want to provide their full details.
The magnitude of patients admitted per day is shown in Fig. 1. Although confrontations ended by 11th of Feb, patients kept presenting for admission on a reduced scale on the following few weeks. The time taken in days between onset of trauma and patient presenting to hospital ranged from presenting same day of trauma up to 30 days, mean 2.9 ± 6 days. The mean waiting period between patient first presenting to emergency department and getting examined by an ophthalmologist was 35 ± 1.3 min. The time consumed from being seen by ophthalmologist to getting the primary intervention, ranged from 1 to 24 h, mean 5.6 ± 3.2 h. We encountered a variable amount of missing data during this retrospective analysis. The percentages of missing data were 23.6 %, 4.1 %, 13.3 %, 17.9 %, 39.5 % and 67.7 % corresponding to investigations done, diagnosis recorded, types of primary intervention, presenting visual acuity, and visual acuity post primary and second interventions respectively.

Frequency of admissions during the uprising
Eighty seven percent of patients were presenting with open globe injuries in which cases with intraocular foreign bodies (IOFB) were all conceiving metallic ones due to gunshot injuries. Five percent of patients were having lid wounds in addition to globe injuries. The diagnoses of patients are described in Fig. 2. One hundred and forty seven eyes received 259 imaging investigations in the form of CT scans, plain x-rays and B scan ultrasounds at rates of 78 %, 65 % and 33 % respectively. Primary and secondary interventions are tabulated in Table 1. Wound repair was the primary intervention in 85 % of eyes while 50 % of the secondary interventions were vitrectomies.

Diagnosis of Patients
Eleven patients were presenting with bilateral globe injury. Nine of them were bilateral open globe injuries whereas, the remaining two were presenting with one eye open globe injury while the other with closed injury. Seven of the bilateral eyes were having No perception of light (no PL) vision, of which one patient was bilateral no PL. Post interventions, two eyes suffered worsening of vision to PL whereas four eyes gained improvement of vision; 2 eyes improved from PL to hand motions (HM) while the other 2 improved from HM to better than hand motions but less than 3/60.
On first presentation, measurement of the presenting visual acuity was not possible in 23.1 % of patients. In more than two thirds (72.5 %), vision was worse than 3/60. There wasn’t considerable change in this pattern after primary (92.3 %) and further interventions (84.1 %) (Fig. 3). When comparing presenting vision with that post primary interventions, results are statistically significant (p = 0.004) which is not the case when comparing vision post primary compared to that recorded post secondary intervention (p = 0.893). Presenting visual acuity showed a statistically significant negative correlation with diagnosis, with vision tending to get worse with open globe injuries (r = −0.159, p = 0.047). In addition, a positive correlation exists between presenting vision and post primary intervention visual acuity (r = 0.840, p < 0.001).

Patterns of visual acuities, PL––perception of light; No PL––no perception of light; HM––Hand Motions
Discussion
Ocular injuries are a worldwide important cause of visual impairment [4]. Advances in the study of eye trauma have been facilitated by the accumulation of the related epidemiological data [5]. In 2008, an Egyptian study was conducted over 6 months on 153 eyes of 147 patients (80 % males) sustaining serious ocular injury requiring hospitalization. There were 80.4 % open globe injuries while closed globe injuries were 19.6 %. Of the open globe injuries, intraocular foreign bodies were present in 24 %. On leaving the hospital, 77 % were having vision worse than 1/60. They reported a rate of endophthalmitis of 8 % [6]. On the other hand an analysis for eye injuries conducted during Palestinian Intifada between 1987 and 1993 revealed male preponderance of 84.7 % in 567 injured eyes of which 25.2 % lost perception of light and 12.6 % had vision less than or equal to 6/60. In addition, there were 3 cases of endophthalmitis [7]. In this report of the 2011 Egyptian uprising eye injuries, the magnitude of cases of which 77 % occurred in 24 h, was almost one third of that recorded for Intifada eye injuries over 6 or more years, and even more than that recorded in an earlier Egyptian study over 6 months. This is emphasizing that we were facing a situation of mass eye casualty. In addition, the Egyptian uprising percentage male predominance (97 %) was higher than all reports. As a matter of fact, the poor presenting visual acuity in our report was similar to the previous Egyptian report [6] but at higher rates compared to regional ones [7, 8]. This could be explained by the higher rates of penetrating injuries with metallic intraocular foreign bodies in our report.
Both in our study, and a study for perforating injuries of operation Iraqi freedom between 2003 and 2006, have reported that very few eyes had achieved visual acuity better than 6/60 post interventions [8]. Rahman et al. described that open globe injuries have shown that visual prognosis at presentation was often difficult to assess. They also have described that there are several factors that are associated with a poor prognostic outcome [9]. One of these factors is the presenting visual acuity being less than 6/60 before the primary repair, which is the case with our study which showed a statistically significant comparison between presenting visual acuity and that after primary repair. Furthermore; in our study the presenting visual acuity showed a statistically significant negative correlation with diagnosis, with vision tending to get worse with open globe injuries.
Mass casualty preparedness is an art in which preparation for all risks should be evaluated and expected. We have encountered in our study a variable amount of missing data that uncovers the fact that preparing for an event with mass casualty should have started long before the event. Despite advances in ophthalmology, management of eye injuries especially open globe ones continues to pose difficult management challenge which is of major impact for those who are facing a lifelong sight loss especially bilateral ones.
References
Waeckerle JF (1991) Disaster planning and response. N Engl J Med 324:815–821
Flint L (2008) Trauma. Contemporary Principles and Therapy. In: Meredith JW, Schwab CW, Trunkey DD, Rue LW, Taheri PA (eds) Lippincott Williams & Wilkins, Philadelphia PA, pp 9–21
Almasry-alyoum (2011) Health offices documented the fall of 840 martyr during the revolution of 25 January. Retrieved 04-04, 2011, from http://web.archive.org/web/20110429125656/http://www.almasryalyoum.com/node/385140
Negrel AD, Thylefors B (1998) The global impact of eye injuries. Ophthalmic Epidemiol 5:143–169
Pieramici DJ, Au Eong KG, Sternberg P Jr, Marsh MJ (2003) The prognostic significance of a system for classifying mechanical injuries of the eye (globe) in open-globe injuries. J Trauma 54:750–754
Soliman MM, Macky TA (2008) Pattern of ocular trauma in Egypt. Graefes Arch Clin Exp Ophthalmol 246:205–212
Jaouni ZM, O’Shea JG (1997) Surgical management of ophthalmic trauma due to the Palestinian Intifada. Eye 11:392–397
Colyer MH, Chun DW, Bower KS, Dick JS, Weichel ED (2008) Perforating globe injuries during operation Iraqi Freedom. Ophthalmology 115:2087–2093
Rahman I, Maino A, Devadason D, Leatherbarrow B (2006) Open globe injuries: factors predictive of poor outcome. Eye 20:1336–1341
Acknowledgments
The authors would like to thank the following ophthalmologists for participating in collection of data: Rasha AbdAllah, Ola ElSheikha, Heba Makled, Lameece Hassan, Karim Bakr, Mohamed Beshr, Mohamed Attia, Mohamed Khafagy, Heba Magdy, Ayman Rashed, Dina Abdelmenam, Mohamed Sabry, Khaled Elhusseiny, Dina Hossam, Mahmoud Osama, Ramy Reyad and Malak Adly.
Conflict of interest
No conflicting relationship exists for any author.
Financial support
None
Author information
Authors and Affiliations
Corresponding author
Additional information
This article has not been published anywhere previously and that it is not simultaneously being considered for any other publication.
Rights and permissions
About this article
Cite this article
Eldaly, M.A., AbdelHakim, M.A., Zaki, R.S. et al. Eye trauma during the 2011 Egyptian revolution. Graefes Arch Clin Exp Ophthalmol 251, 661–665 (2013). https://doi.org/10.1007/s00417-012-2202-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-012-2202-6