
Abstract
Purpose
Our purpose was to study retinal pigment epithelium (RPE) wound healing in patients with age-related macular degeneration (AMD).
Patients and methods
Abrasive debridement of nasal RPE was performed with a metal cannula during pars plana vitrectomy for foveal choroidal neovascularization (CNV) membrane excision combined with simultaneous autologous RPE transplantation. Fundus autofluorescence, fluorescein angiography images, and red-free pictures were taken initially within 1–2 weeks postoperatively, subsequently in 2-week intervals until 3 months, monthly until 6 months, and every 3 months thereafter. The borders of these lesions were measured; areas were calculated and compared using ArchiCad Software. Fourteen eyes of 14 patients suffering from AMD were included (nine women and four men, mean age 75.6 years ±6.6 years).
Results
Six of 14 (42.9 %) patients showed a reduction of the RPE debrided area. The size of these lesions reduced 5.6–20% within 2 postoperative months compared with their size at first examination (from a mean of 13.7 mm2 ± 7.2 at baseline to a mean of 12.8 mm2 ± 6.7 at 2 months postoperatively). No further reduction of the lesions was seen after the 2 months. In eight cases, borders of the RPE debrided areas stayed stable during observation time.
Conclusions
Wound healing of abrasively debrided RPE monolayer defects in patients with AMD occurs to a certain extent in nearly half of the cases. This process seems to stop after 2 months.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The retinal pigment epithelium (RPE) cell differentiates from the outer leaflet of the neuroepithelium of the invaginated embryonic eyecup [1]. Several mitotic rounds occur during ocular development to reach adult cell counts at around 6 months of postnatal age [2, 3]. The RPE monolayer, thereafter, undergoes age-related rearrangements in cell density [4]. Approximately 0.3% of the total RPE cell number are lost each year in normal eyes [5]. Interestingly, however, macular cell densities seem to increase throughout life [4], despite a higher central apoptotic activity [6]. It remains unclear to date though, whether adult RPE undergoes mitosis in situ under physiologic conditions.
Nevertheless, disturbances of the homeostasis in the RPE photoreceptor complex through laser burns, sodium iodate or light toxicity, retinal detachments, choroidal melanoma, or following experimental RPE debridement are capable of inducing proliferation in adulthood [7–10]. Thus, there appears to be sufficient evidence that certain stimuli will induce proliferation in adult RPE.
In its function, the RPE serves as an intermediary between an epithelial and a glial cell (for review, see Marmor, 1998 or Strauss, 2005 [11, 12]). Yet, healing of a monolayer defect is similar to other epithelia, with sliding migration from the edges, which in larger defects is followed by proliferation to close the wound [3, 13]. During this process, cells at the edges loose their characteristic cuboidal hexagonal shape and adopt spindle-shaped hypopigmented morphologies [8]. This is paralleled on the molecular level with loss of cellular polarity during the growth phase, which is regained upon wound closure, a process that has been compared with the maturation of the RPE during development [13]. Microenvironmental “dynamic reciprocity” reactions, i.e., the influence of extracellular matrix composition of the wound bed on the maturation of the RPE phenotype, have been implicated into wound healing patterns [3]. Defects of up to 2–3 mm in diameter have been reported to heal into “tight” mono- and multilayers in animal models [8–10, 14].
Aged macular degeneration (AMD) is the leading cause of blindness in populations over 55 years of age in industrial nations [15]. Herein, the RPE and adjacent tissues are thought to have incurred a sequence of pathologic alterations over a lifetime, which through stages ultimately have lead to abnormal cellular behavior and/or atrophy (for review, see Zarbin [16]). A late-stage complication, occurring in roughly 20% of AMD patients, leads to the development of choroidal neovascularization (CNV) in the subepithelial (RPE) and/or subretinal space [17]. Surgical excision of the CNV membrane is often followed by development of choriocapillaris atrophy, with progressive extension beyond the original CNV lesion [18, 19]. This phenomenon was explained by the simultaneous removal of RPE during submacular surgery. Experimental RPE destruction has been shown to induce choriocapillaris atrophy [7, 20]. It appears that abnormalities of aged submacular RPE [21] and/or Bruch’s membrane (BM) [22, 23] may inhibit effective restoration of the macular monolayer. Removal of RPE trophic paracrine function on the choriocapillaris [24] and possibly also mechanical trauma to BM and choriocapillaris during subretinal manipulation [10, 25] may contribute to choriocapillaris atrophy. Despite one report to the contrary [26], the above strongly suggests failure of RPE wound healing following extraction of CNV secondary to AMD. Whether this is an intrinsic RPE defect in AMD is unclear to date; however, it is noteworthy that viable RPE samples obtained from AMD patients during CNV removal did not grow in culture [27]. Thus, the ability of the RPE to resurface monolayer defects may be altered in AMD.
The latter dilemma has been recognized for some time, and clinical trials have been initiated on retinal and iris pigment epithelial transplantation [28–31]. Here we report on postoperative observations of the nasal RPE harvesting site from previously published clinical trials with autologous RPE transplantation [29, 30]. The RPE autografts were mechanically scraped off BM with a custom-made metallic canula (Binder-Parel-Lee). The wound bed thus created may resemble in some aspects the surgical trauma induced with dissection of the CNV underneath the macula [9, 10, 21, 22]. Although some degree of RPE wound healing has been demonstrated in an animal model with our technique [32], we hypothesize that it may be altered in AMD. The patients were studied with fundus autofluorescence imaging (FAF), fluorescein angiography (FA), and red-free pictures (RF) for a mean of 11 months for RPE resurfacing in nasally debrided harvesting sites.
Patients and methods
Patients
Fourteen patients (nine women and five men) with foveal CNV neither suitable for laser treatment nor photodynamic therapy (PDT) who had transplantation surgery and agreed to participate were included into the study (Table 1). We examined nine right and five left eyes. Postoperatively, patients were studied as soon as clear examination of the entire fundus was possible and hemorrhages had absorbed (between 1 and 2 weeks). Examinations were performed in 2-week intervals until 3 months, monthly until 6 months, and every 3 months thereafter.
The study conformed to the Declaration of Helsinki and was approved by the ethics committee of the Rudolf Foundation Clinic, government of the City of Vienna. After careful oral explanation of the purpose of this study, a written consent was signed by each patient. Patient data are summarized in Table 1.
RPE transplantation surgery
The procedure followed what has been published elsewhere [29, 30]. All surgeries were performed by the same surgeon (SB). In brief; after pars plana vitrectomy, a shallow retinal detachment was created by subretinal injection of Ca++ and Mg++ free balanced salt solution (BSS) (BSS+ part 1, Alcon Surgical, Fort Worth, TX, USA) nasally from the optic disc to facilitate separation between the retina and the pigment epithelium. RPE cells were subsequently mobilized and aspirated over an area of two-to-four disc diameters with a specially designed cannula (Binder, Parel unpublished data) in order to remove the RPE as gently as possible. The cannula was connected with a silicone tube to a tuberculin syringe. While the surgeon guided the cannula subretinally, the assistant aspirated under microscopic control.
The purpose of this study was to investigate the behavior of the RPE nasal defects the optic disc where cells were harvested for transplantation.
Examination
All images (30° field of view) were performed with the Heidelberg Retina Angiograph (Heidelberg Engineering GmbH, Heidelberg, Germany) by two different examiners uninvolved in patient selection and treatment. After pupil dilatation, FAF was recorded, 6–8 FA images were taken in the early phase after injection, then every 15 s, after 1 and 2 min, and finally late pictures after 5 and 10 min. For FAF imaging, an argon blue laser (488 nm) was used for excitation [33]. Emitted light was detected above 500 nm with a barrier filter. For RF reflectance, a monochromatic green band pass filter was used that transmits light with wavelengths between 540 and 575 nm.
Image processing
Images were analyzed by one investigator (DR) using ArchiCad (Version 8.1 training-software, Graphisoft 2003). The following scaling procedure was applied: the distance between two vessel branch points near the denuded area in the first postoperative image of each patient was measured, and this length was taken as the standard distance for all following pictures. Images were enlarged or shrunk without changing proportions until the distance between the vessel branch points conformed with the standard distance. Only borders and periphery of the debrided areas were investigated. We compared the borders of RPE wounds with borders of reduced FAF, and the outer boundaries of window defects in FA or RF pictures to debrided or absent RPE. On each obtained FAF image, the contour of the RPE debridement was outlined with a freehand selection tool. The outlined area in the first postoperative FAF image was saved and superimposed onto subsequently obtained images from each patient. Area and maximum centripetal growth of borders in RPE defects outlined in FAF was then calculated using ArchiCad. The borders of atrophic areas in FAF were compared (and correlated) with boundaries of lesions in RF and FA images performed on the same day and with subsequent images. A decrease of the debrided area in FAF images over time was considered to be RPE wound healing if we also observed an according reduction of the debrided area in RF and FA. FAF were superimposed, and an averaged picture was created to improve image quality. We only used FA pictures where the hyperfluorescent area did not change from early to late phase within the examination to distinguish leakage from RPE atrophy.
Results
Clinical observations
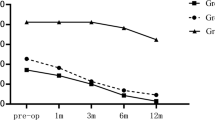
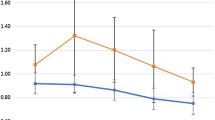
A series of 14 eyes from 14 consecutive patients (nine women and five men; mean age 75.6 ± 6.6 years) was examined. Data of all 14 patients are summarized Table 1. The observation time ranged from 6 to 27 months (mean 11 ±7.2 months). The size of the debrided RPE areas at first examination ranged between 2.5 and 21 mm2; mean 13.7 mm2 (± 7.2). Six of 14 (42.9 %) patients showed a 12.6% (±5.6) mean reduction in size of their debrided areas. The lesions diminished ranging 0.5 mm2 to 4.1 mm2 (Table 1). No further changes were observed after a 2-month period postoperatively, and no enlargement of any lesion occurred. In 8/14 cases, borders of the RPE debrided areas remained stable during observation time. There was no correlation between size of the nasal RPE harvest site and the extent of its reduction. As opposed to an expected uniformly centripetal pattern, RPE wound healing of nasal areas occurred in an inhomogeneous way. At one side of the lesion, resurfacing of RPE occurred to a certain extent, whereas other wound edges were unchanged (Fig. 1).

Individual measurements of retinal pigment epithelium (RPE) monolayer lesions over time. Ordinate in (a) shows absolute values in mm2 and in (b) values in percent at baseline (size of nasal lesion at week 2)
The RPE’s capacity to resurface various distances from the wound edge may be limited. We therefore analyzed absolute distances of border change to determine whether this would be a more uniform comparison of lesion differences. The maximum growth of borders toward the lesion center ranged between 0.19 mm and 0.98 mm (mean 0.58 mm) (Figs. 2 and 3 and Table 1). There appears to be neither a correlation with original wound size nor wound reduction. We found no association between age and tendency of RPE repair; on the contrary, the two oldest patients in the study (both aged 83) showed a reduction in lesion size, whereas the youngest patients (age 62 and 65 years) showed no changes.

Autofluorescence (a, c), red-free image (b, d), and late (7:04 min) fluorescein angiography (FA) (e) of patient 5. The orange line in (a, b) marks the debrided retinal pigment epithelium (RPE) area at 2 weeks postoperatively. Blue line (c–e) outlines RPE defect at 6 weeks postoperatively. Black arrows (c, d) show area of main reduction. White arrows (c) are areas of hypofluorescence (window defect) in (e), consistent with choriocapillaris atrophy adjacent to a zone of wound healing (asterisks) at 6 weeks postoperatively. Green arrow indicates the maximum centripetal displacement of borders (0.60 mm)

Autofluorescence (a, c, f), red-free (RF) images (b, d, g) and fluorescein angiography (FA) (e, h) of patient 7. One week postoperatively (a, b). Orange line marks the retinal pigment epithelium (RPE)-debrided area 2 weeks postoperatively, blue line indicates the reduced area, white arrows indicate the intravitreal gas bubble. Pictures taken at 1 month postoperatively (c–e) continued to show reduction of the RPE monolayer defect; however, no further change was observed at 3 months postoperatively (f–h). Black arrows (f, g) indicate the main area of wound healing. Green arrow indicates the maximum centripetal displacement of borders (0.98 mm). Compare lesion borders in c, d and f, g with corresponding late FA at 1 month (e) and 3 months (h) postoperatively. Green line (c–h) indicates area obscured by intravitreal gas bubble on initial postoperative pictures (a, b)
Lesion sizes were calculated by using changes of borders in autofluorescence pictures. In some cases, areas of more normal appearance of autofluorescence seemed to occur in the center of the lesions. Correlation with FA, however, excluded wound healing and, instead, revealed a window defect suggesting choriocapillaris atrophy within the debrided area (Fig. 2). The area of window defect in the FA images could be distinguished from leakage, as there was no change in size from early to late phase during the examination.
Statistical evaluation
To investigate reduction of the RPE debrided area, Wilcoxon signed rank tests were used to investigate differences between time points 4–10 (week 4–10) and baseline (week 2). The confidence interval (CI) for the proportion of patients with lesion reductions was calculated. Wilcoxon analysis did not show a significant difference between time points 2 and 4 (2 and 4 weeks postoperatively) (p = 0.125),but found a significant difference between all other time points (weeks 6, 8, 10) and time point 2 (all three p values = 0.031). CI: lower bound 17.66 %; upper bound 71.13 %. We found no correlation between the size of the nasal RPE harvest site and the dimension of its reduction (r = −0.50).
Discussion
Mechanically debrided RPE monolayer defects were investigated in patients with CNV secondary to AMD for changes of borders with fundus autofluorescence imaging, FA, and RF pictures. A 12.6% reduction of lesion size occurring within 2 months after surgery in roughly half of the subjects suggests that some small extent of RPE regeneration is possible in patients with AMD. This is, to the best of our knowledge, the first report on in vivo wound healing of human RPE following its iatrogenic abrasive removal in eyes suffering AMD.
Aged RPE monolayer defects created in organ cultures of human submacular BM have shown some degree of wound healing. The presence of the RPE basal lamina supports resurfacing to a significantly higher degree than if deeper layers of BM are exposed [21]. BM is known to thicken and accumulate age-related debris [34], which in turn appears to hamper attachment and growth of RPE cells [35]. There are numerous reports on differences between young and aged RPE [36, 37]. In this context, it might be noteworthy that cultured aged RPE compared with fetal RPE seem generally less efficient in repopulating various layers of submacular BM [38]. Thus, aging of deeper layers of BM and senescence of the RPE very likely played a role in wound healing in aged eyes and our study.
Animal studies have demonstrated repopulation of a RPE defect after experimental debridement within 1–2 weeks [8–10, 14, 32]. Fundoscopic observations show in the initial postoperative days the appearance of a hypopigmented ring around the pale-appearing wound bed [8]. Histopathologically, this coincides with sliding migration and spindle-shaped elongation of the RPE cells surrounding the lesion. After 2 weeks, the area of the original lesion will adopt a hypo- and hyperpigmented appearance, corresponding histologically to mono- and multilayered newly proliferating RPE cells, respectively [8]. Interestingly, the peripheral hypopigmented ring persisted also at this latter stage. We found a reduction of debrided areas of up to 20% in this study. However, we did not observe a hypopigmented ring surrounding the original defect or find hypo- or hyperpigmentation in the original wound bed.
Previous animal studies have shown that the technique used for RPE removal has a direct influence on the cellular phenotype resurfacing the wound. Whereas a hydraulic (jet stream) debridement often results in restoration of a polarized monolayer [10], abrasive debridement with a silicone or metal-tipped instrument usually causes an incomplete defect closure in which RPE cells adopt a fibroblast-like phenotype with alternating degrees of mono- and multilayering [9, 10, 25]. Conceivably, the direct instrument contact with the RPE during abrasive removal compromises the integrity of BM to a larger degree than does hydraulic removal [25]. The contribution of species-specific differences in anatomy to the variability in RPE wound-healing patterns using abrasive denudement should also be taken into account. Whereas lesions in pigs and monkeys repopulate almost completely [9, 14], RPE defects in cats and rabbits show incomplete coverage [20, 25, 32]. However, the common denominator from these animal experiments relevant for the human setting appears to be abrasive debridement compromising RPE wound healing through exposure of deeper layers of BM. In contrast to an expected uniformly centripetal RPE wound healing pattern, we observed an inhomogeneous decrease in size of the wound bed. At one edge of the lesion, the transition between intact RPE and debrided area might advance toward the wound center, whereas other edges remained unchanged (Figs. 2 and 3). We speculate this to be due to different stages of damage in BM caused by the mechanical debridement of RPE during surgery. This exposure of deeper layers of BM in some eyes and an absence of RPE resurfacing consequently may also be the explanation why only in six of 14 eyes did a reduction in area size occur.
RPE wound healing has been suggested to be dependent on lesion size [3]. Regeneration the human RPE in situ into a polarized monolayer is thought to be reserved to only small defects [39]. We found no correlation between the size of the nasal RPE harvest site and the dimension of its reduction.
Differentiated mammalian cells can only undergo a limited amount of doublings. It has been reported that this capacity declines over age in the RPE cell [40]. The ability to resurface various distances from the wound edge may therefore decline accordingly. We found no apparent correlation with age. Interestingly, in our small number of patients, the two oldest patients (age 83 years) experienced a reduction of lesion size, whereas in two patients approximately 20 years younger (age 62 and 65), the debrided areas did not change.
The measurements in this study were performed on FAF images and correlated with RF pictures and FA. FAF has been shown to exhibit spectral characteristics of RPE lipofuscin [41]. It accumulates over life in RPE cells as a result of incompletely digested photoreceptor outer segments [42]. Monitoring FAF with noninvasive in vivo spectrophotometry or a confocal laser scanning ophthalmoscope has been suggested as a diagnostic tool for providing indirect information about metabolic activity of the RPE [43, 44]. Changes of “normal” FAF occurring in various retinal pathologies affecting the RPE have been described extensively and prompted us to utilize it for our study [33, 45]. Physiologically reduced FAF is seen in the absence of RPE cells (e.g., RPE-depleted lesions, optic disc) or may be due to absorption of the incident short wavelength by the retinal vessels [43]. Further, reduced or absent FAF is also observed in regions of geographic atrophy in AMD [45]. We considered a decrease of extinguished FAF toward the lesion center (when compared with earlier images) a reduction in size of lesions during follow-up. A diminished lesion size on FAF could be correlated with a corresponding window defect in FA and a hyperfluorescent area in RF images obtained the same day. This method, however, may not account for detecting newly proliferated cells, which split their cytoplasmic contents with every doubling, as it is observed with pigment granules (e.g., melanolipofuscin) in cell culture [46]. Diagnostic accuracy for detecting such changes would likely be compromised. Our study analyzed only FAF changes from extinguished to normal.
Some hypofluorescent areas on FAF when correlated with FA after 6 postoperative weeks showed decreased or absent choriocapillaris perfusion. The choriocapillaris will remain only partially patent after abrasive debridement of the RPE in animals [10]. Earlier work based on histologic examinations of over 500 human cases suggested choriocapillaris degeneration after RPE loss [47], which then gained support through animal experiments [7]. This suggests, in the context of our study, that areas with decreased or absent choriocapillaris perfusion on FA may represent regions where RPE is missing and/or dysfunctional. Decreased FAF over such regions would support this assumption, as it is frequently observed in regions with geographic atrophy of the RPE in AMD [45].
Evidence from RPE wound healing in animal experiments and perhaps also after extraction of CNV secondary to AMD suggests most changes occur in the first postoperative 1–2 weeks [8–10, 14, 25, 26]. It is unclear whether early recovery occurred in this study because of reduced visibility during the first 1–2 weeks related to the intravitreal gas bubble. Areas measured at the first examination showed a large variation, ranging from 2.5 to 21 mm2. However, based on frequent intraoperative video imaging, we knew that the depigmented areas created by cell harvesting were usually more uniform (two-to-four disc diameters/ ∼11.6– 46.3 mm2). Optic disc size is known to have considerable interindividual variation [48]. Nevertheless, this would not explain the up to tenfold difference between harvesting sites. As the RPE harvesting site was investigated over a long period (up to 27 months), we assume that changes from initially reduced FAF zones to “normal,” supported by normal-appearing RPE in RF and FA, reflects a reestablished functional subretinal environment. The process seems to stop after a 2 months. We can only speculate about the reasons: a reachievment of homeostasis (i.e., postoperative inflammatory) and consequently reduced stimulus inducing proliferation of RPE cells, for instance.
Previous work on RPE wound healing and findings of the present study suggest that a damaged BM and aged RPE are unlikely to result in a fully functional repair of the subretinal environment. The logical consequence is therefore to consider provision of a BM prosthesis and/or autologous RPE transplantation to improve or preserve vision in patients affected with RPE monolayer defects.
We present evidence that abrasive RPE lesions created during subretinal surgery in patients with AMD can occasionally undergo some degree of repair. We speculate that surgical damage as the main factor and age-related changes to BM, along with senescent changes to the RPE, may hinder functional restoration of the subretinal microenvironment.
References
Zhao S, Rizzolo LJ, Barnstable CJ (1997) Differentiation and transdifferentiation of the retinal pigment epithelium. Int Rev Cyt 171:225–266
Coulombre AJ (1979) Roles of the retinal pigment epithelium in the development of ocular tissues. In: Zinn KM, Marmor MF (eds) The retinal pigment epithelium. Harvard University Press, Cambridge, MA, pp 267–276
Grierson I, Hiscott P, Hogg P et al (1994) Development, repair and regeneration of the retinal pigment epithelium. Eye 8(Pt 2):255–262
Harman AM, Fleming PA, Hoskins RV, Moore SR (1997) Development and aging of cell topography in the human retinal pigment epithelium. Invest Ophthalmol Vis Sci 38:2016–2026
Panda-Jonas S, Jonas JB, Jakobczyk-Zmija M (1996) Retinal pigment epithelial cell count, distribution, and correlations in normal human eyes. Am J Ophthalmol 121:181–189
Del Priore LV, Kuo YH, Tezel TH (2002) Age-related changes in human RPE cell density and apoptosis proportion in situ. Invest Ophthalmol Vis Sci 43:3312–3318
Korte GE, Reppucci V, Henkind P (1984) RPE destruction causes choriocapillary atrophy. Invest Ophthalmol Vis Sci 25:1135–1145
Lopez PF, Yan Q, Kohen L et al (1995) Retinal pigment epithelial wound healing in vivo. Arch Ophthalmol 113:1437–1446
Valentino TL, Kaplan HJ, Del Priore LV et al (1995) Retinal pigment epithelial repopulation in monkeys after submacular surgery. Arch Ophthalmol 113:932–938
Leonard DS, Zhang XG, Panozzo G, Sugino IK, Zarbin MA (1997) Clinicopathologic correlation of localized retinal pigment epithelium debridement. Invest Ophthalmol Vis Sci 38:1094–1109
Marmor MF (1998) Structure, function, and disease of the retinal pigment epithelium. In: Marmor MF, Wolfensberger TJ (eds) The retinal pigment epithelium: function and disease. Oxford University Press, New York, Oxford, pp 3–12
Strauss O (2005) The retinal pigment epithelium in visual function. Physiol Rev 85:845–881
Korte GE, Perlman JI, Pollack A (1994) Regeneration of mammalian retinal pigment epithelium. Int Rev Cytol 152:223–263
Del Priore LV, Hornbeck R, Kaplan HJ et al (1995) Debridement of the pig retinal pigment epithelium in vivo. Arch Ophthalmol 113:939–944
Klein R, Klein BE, Linton KL (1992) Prevalence of age-related maculopathy. The Beaver Dam Eye Study. Ophthalmology 99:933–943
Zarbin MA (2004) Current concepts in the pathogenesis of age-related macular degeneration. Arch Ophthalmol 122:598–614
Ferris FL, III, Fine SL, Hyman L (1984) Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol 102:1640–1642
Pollack JS, Del Priore LV, Smith ME, Feiner MA, Kaplan HJ (1996) Postoperative abnormalities of the choriocapillaris in exudative age-related macular degeneration. Br J Ophthalmol 80:314–318
Nasir MA, Sugino I, Zarbin MA (1997) Decreased choriocapillaris perfusion following surgical excision of choroidal neovascular membranes in age-related macular degeneration. Br J Ophthalmol 81:481–489
Del Priore LV, Kaplan HJ, Hornbeck R, Jones Z, Swinn M (1996) Retinal pigment epithelial debridement as a model for the pathogenesis and treatment of macular degeneration. Am J Ophthalmol 122:629–643
Wang H, Ninomiya Y, Sugino IK, Zarbin MA (2003) Retinal pigment epithelium wound healing in human Bruch’s membrane explants. Invest Ophthalmol Vis Sci 44:2199–2210
Tezel TH, Kaplan HJ, Del Priore LV (1999) Fate of human retinal pigment epithelial cells seeded onto layers of human Bruch’s membrane. Invest Ophthalmol Vis Sci 40:467–476
Gullapalli VK, Sugino IK, Van Patten Y, Shah S, Zarbin MA (2005) Impaired RPE survival on aged submacular human Bruch’s membrane. Exp Eye Res 80:235–248
Liu X, Ye X, Yanoff M, Li W (1997) Extracellular matrix of retinal pigment epithelium regulates choriocapillaris endothelial survival in vitro. Exp Eye Res 65:117–126
Leonard DS, Sugino IK, Zhang XG et al (2003) Ultrastructural analysis of hydraulic and abrasive retinal pigment epithelial cell debridements. Exp Eye Res 76:473–491
Sawa M, Kamei M, Ohji M et al (2002) Changes in fluorescein angiogram early after surgical removal of choroidal neovascularization in age-related macular degeneration. Graefe Arch Clin Exp Ophthalmol 240:12–16
van Meurs JC, ter Averst E, Croxen R, Hofland L, van Hagen PM (2004) Comparison of the growth potential of retinal pigment epithelial cells obtained during vitrectomy in patients with age-related macular degeneration or complex retinal detachment. Graefe’s Arch Clin Exp Ophthalmol 242:442–443
Del Priore LV, Kaplan HJ, Tezel TH et al (2001) Retinal pigment epithelial cell transplantation after subfoveal membranectomy in age-related macular degeneration: clinicopathologic correlation. Am J Ophthalmol 131:472–480
Binder S, Krebs I, Hilgers RD et al (2004) Outcome of transplantation of autologous retinal pigment epithelium in age-related macular degeneration: a prospective trial. Invest Ophthalmol Vis Sci 45:4151–4160
Binder S, Stolba U, Krebs I et al (2002) Transplantation of autologous retinal pigment epithelium in eyes with foveal neovascularization resulting from age-related macular degeneration: a pilot study. Am J Ophthalmol 133:215–225
van Meurs JC, ter Averst E, Hofland LJ et al (2004) Autologous peripheral retinal pigment epithelium translocation in patients with subfoveal neovascular membranes. Br J Ophthalmol 88:110–113
Phillips SJ, Sadda SR, Tso MO et al (2003) Autologous transplantation of retinal pigment epithelium after mechanical debridement of Bruch’s membrane. Curr Eye Res 26:81–88
von Ruckmann A, Fitzke FW, Bird AC (1997) Fundus autofluorescence in age-related macular disease imaged with a laser scanning ophthalmoscope. Invest Ophthalmol Vis Sci 38:478–486
Okubo A, Rosa RH, Jr., Bunce CV et al (1999) The relationships of age changes in retinal pigment epithelium and Bruch’s membrane. Invest Ophthalmol Vis Sci 40:443–449
Tezel TH, Del Priore LV, Kaplan HJ (2004) Reengineering of aged Bruch’s membrane to enhance retinal pigment epithelium repopulation. Invest Ophthalmol Vis Sci 45:3337–3348
Boulton M, Dayhaw Barker P (2001) The role of the retinal pigment epithelium: topographical variation and ageing changes. Eye 15:384–389
Boulton M, Roanowska M, Wess T (2004) Ageing of the retinal pigment epithelium: implications for transplantation. Graefe’s Arch Clin Exp Ophthalmol 242:76–84
Zarbin MA (2003) Analysis of retinal pigment epithelium integrin expression and adhesion to aged submacular human Bruch’s membrane. Trans Am Ophthalmol Soc 101:499–520
Tso MO (1997) Developmental, reactive and neoplastic proliferation of the retinal pigment epithelium. In: Zinn KM, Marmor MF (eds) The retinal pigment epithelium. Harvard University Press, Cambridge, pp 267–276
Del Monte MA, Maumenee IH (1980) New technique for in vitro culture of human retinal epithelium. Birth Defects Orig Atic Ser 16:327–338
Delori FC, Dorey CK, Staurenghi G et al (1995) In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium lipofuscin characteristics. Invest Ophthalmol Vis Sci 36:718–729
Sparrow JR, Boulton M (2005) RPE lipofuscin and its role in retinal pathobiology. Exp Eye Res 80:595–606
Delori FC (1994) Spectrophotometer for noninvasive measurement of the intrinsic fluorescence and reflectance of the ocular fundus. Appl Opt 33:7439–7452
von Ruckmann A, Fitzke FW, Bird AC (1995) Distribution of fundus autofluorescence with a scanning laser ophthalmoscope. Br J Ophthalmol 79:407–412
Schmitz-Valckenberg S, Bultmann S, Dreyhaupt J et al (2004) Fundus autofluorescence and fundus perimetry in the junctional zone of geographic atrophy in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci 45:4470–4476
Opas M (1994) Substratum mechanics and cell differentiation. Int Rev Cytol 150:119–137
Sarks S (1978). Changes in the region of the choriocapillaris in ageing and degeneration. In: Shimizu K, Oosterhuis J (eds) Concillium ophthalmologicum. Excerpta Medica, Kyoto, pp 228–238
Jonas JB, Gusek GC, Naumann GO (1988) Optic disc, cup and neuroretinal rim size, configuration and correlations in normal eyes. Invest Ophthalmol Vis Sci 29:1151–1158
Acknowledgements
The authors wish to thank Jean-Marie Parel Ing., PhD. and William Lee, MS, Ophthalmic Biophysics Center, Bascom Palmer Eye Institute, Miami, FL, USA, for developing the RPE harvesting canula. Statistical evaluation was performed by the Core Unit of Medical Statistics and Informatics, Medical University of Vienna (Head Prof. Dr. Bauer). Michael Marmor, M.D. is gratefully acknowledged for critical comments on the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by unrestricted research grant from the L. Boltzmann Institute to SB.
Rights and permissions
About this article
Cite this article
Rabenlehner, D., Stanzel, B.V., Krebs, I. et al. Reduction of iatrogenic RPE lesions in AMD patients: evidence for wound healing?. Graefes Arch Clin Exp Ophthalmol 246, 345–352 (2008). https://doi.org/10.1007/s00417-007-0658-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-007-0658-6