
Abstract
Background
Measures to define treatment response, such as no evidence of disease activity (NEDA), are routinely used in multiple sclerosis (MS) clinical practice. Although spinal cord involvement is a frequent feature of MS, its magnetic resonance imaging (MRI) monitoring is not routinely performed.
Objective
To assess the impact of spinal cord MRI in the definition of NEDA in a cohort of people with MS (pwMS) with available spinal cord imaging performed as for routine monitoring.
Methods
We included 115 pwMS undergoing treatment with first-line disease-modifying therapies (DMTs) and retrospectively analyzed the presence of NEDA in the whole cohort, either considering or not spinal cord imaging.
Results
When considering only clinical and brain MRI measures, 97 out of 115 pwMS (84.3%) satisfied the criteria for NEDA. In the same cohort, the number of pwMS with NEDA significantly decreased to 88 (76.5%) (p < 0.01) when considering also spinal cord imaging.
Conclusion
These findings suggest that, in routine clinical practice, spinal cord MRI monitoring in pwMS under first-line DMTs leads to a slight but significant change in the proportion of subjects classified as clinically and radiologically stable according to the NEDA definition.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and degenerative disease of the central nervous system (CNS) that typically affects young adults, causing irreversible physical and cognitive disability. Disease-modifying therapies (DMTs) can influence the disease course by reducing disease activity and slowing down the accumulation of disability. The growing availability of effective treatments led to an increasing interest in the issue of treatment algorithms. Early diagnosis and intervention are crucial, as well as a rapid switching to other therapies if lack of response or a suboptimal response is detected by clinical and magnetic resonance imaging (MRI) measures [1,2,3,4]. Currently, an ideal therapeutic goal to achieve in clinical practice is thought to be the ‘no evidence of disease activity’ (NEDA) status, which is based on a ‘zero tolerance concept’ entailing for the absence of relapses, no confirmed disability worsening, and no MRI disease activity [5]. However, in monitoring treatment response with MRI measures, NEDA definition does not take into account lesions topography (i.e., infratentorial and/or spinal cord lesions), which could be more related to disability accrual over time than the overall lesion count [2, 6]. Evidence suggests that spinal cord lesions are present in up to 90% of all people with MS (pwMS), and spinal involvement is strongly correlated with future disability accrual [7,8,9]. While the role of spinal cord MRI in the diagnosis of subjects with suspected MS is consolidated [10], the opportunity of its use in the monitoring of pwMS and in the assessment of treatment response is debated [11, 12]. Spinal cord MRI is technically more demanding and it requires considerable expertise compared to brain imaging because of the small size of the spinal cord and artifacts due to vessels and cerebrospinal fluid (CSF) pulsation [12]. Moreover, spinal lesions are believed to be mostly symptomatic, likely because of the tightly packed white matter tracts within the spinal cord. Accordingly, the 2021 Magnetic Resonance Imaging in MS (MAGNIMS)—Consortium of MS Centers (CMSC)—North American Imaging in MS Cooperative (NAIMS) consensus recommendations on the use of MRI in pwMS established that, in monitoring MS, regular brain MRI scans are essential, while spinal imaging is still not routinely recommended except for specific clinical situations [12].
It is, however, recognized that asymptomatic spinal cord lesions (a-SLs) may occur [12,13,14,15,16,17], even alone, i.e., without associated subclinical brain MRI activity. Currently, the impact of missing a-SLs on the overall definition of disease activity and treatment response needs to be clarified. For this reason, we analyzed data from a retrospective cohort of pwMS treated with first-line DMTs to explore the role and the impact of including spinal cord MRI data in the routine monitoring of treatment response and, specifically, in the definition of the NEDA status.
Methods
Study design and participants
We performed a retrospective study based on data collected in the real-world setting. We analyzed data of people with relapsing MS diagnosed according to the 2017 revision of the McDonald criteria [18], regularly attending the MS Center at the S. Maria Misericordia Hospital, Section of Neurology, University of Perugia, Perugia (IT). Eligible subjects were identified within the MS registry of the Center according to the following inclusion criteria: (1) age ≥ 18 years old; (2) treatment with first-line agents, specifically interferons (INF-beta, all formulations), glatiramer acetate (GA), dimethyl fumarate (DMF), or teriflunomide (TF); (3) having performed spinal cord imaging for the routine monitoring of the disease. Only pwMS with an outpatient visit performed in the period between January 2018 and December 2018 were selected from the Center database; the first visit in this period has been defined as the timepoint 1 visit (V1), and the previous reference visit performed between 6 and 12 months before as the timepoint 0 visit (V0). With reference to the V1 visit, a recent brain + spinal cord (cervical ± thoracolumbar regions) MRI with post-contrast sequences (V1-MRI), performed at the same clinical site and with the same MRI scanner of a previous MRI (V0-MRI) extended to the same anatomical districts should have been available.
MRI protocol
For this study, we analyzed MRI scans performed in the context of the routine clinical monitoring of pwMS. MRIs were performed according to the guidelines from the Italian Neurological and Neuroradiological Societies [19]. MRIs were performed on a 1.5 T magnet (GE Optima 360 Advance, General Electric Healthcare Systems, Chicago, Illinois, USA) or a 3 T magnet (Philips Achieva, Philips, Amsterdam, NL). For all the scans, 3-mm thick contiguous slices were obtained. As per study definition, the V1-MRI and V0-MRI were performed in the same clinical site with the same MRI scanner. The definition of focal brain MRI activity on V1-MRI included the presence of new or unequivocally enlarged lesions on T2 and on fluid attenuated inversion recovery (FLAIR) sequences and/or contrast-enhancing lesions (CELs) when compared with V0-MRI. Focal spinal cord MRI activity on V1-MRI was defined by the presence of new or unequivocally enlarged lesions on T2 and on short tau inversion recovery (STIR) sequences and/or CELs, when compared with V0-MRI. Presence of CELs was detected on T1-weighted images of the brain and spinal cord after gadolinium administration.
Definition of the NEDA status and impact of spinal cord imaging
We defined the NEDA status between V1 and V0. For this study, we used the definition of NEDA-3 [2, 20]. Specifically, pwMS were classified as satisfying NEDA if all of the following criteria were met: (1) absence of relapses, i.e., newly developed neurological symptoms or reactivation of pre-existing neurological deficits lasting for at least 24 h in the absence of an increase in body temperature or infections [21]; (2) absence of clinical progression, defined as a 6 months-confirmed increase in the Expanded Disability Status Scale (EDSS) score by ≥ 1.5 point if baseline EDSS 0, by 1 point if baseline EDSS 1–5, and by 0.5 points if baseline EDSS ≥ 5.5 [22]; (3) absence, in the period between V1-MRI and V0-MRI, of focal MRI activity. For each individual, we calculated the impact of including spinal cord MRI data (new/enlarged lesions in the spinal cord or enhancing lesions) in the proportion of pwMS satisfying the NEDA definition.
Statistical analysis
Continuous variables have been reported as mean ± standard deviation if normally distributed; median and interquartile range (IQR) were also reported if not normally distributed. Categorical variables have been reported as number and percentage. Chi-squared test was used to test the difference between frequencies. A p value ≤ 0.05 was considered to define the statistical significance.
Results
Demographical and clinical characteristics
According to the inclusion criteria, we recruited in the study 115 people with relapsing MS (F: 84; M: 31; F/M ratio 2.7/1; mean age at V1 41.5 ± 11.2 years). The mean disease duration, calculated from the diagnosis, was 7.3 ± 5.5 years (median 6.5, IQR 10.9). At V1, 42 patients (36.5%) were under treatment with DMF, 40 (34.8%) with GA, 25 (21.7%) with IFN-beta, and 8 (7%) with TF. The mean duration of the first-line treatment was 35.5 ± 39.7 months (median 24 months, IQR 38.5) in the whole cohort. The mean distance between V1 and V0 was 11.7 ± 4.3 months (median 11.4, IQR 4.7) while the mean time between V1-MRI and V0-MRI was 11.2 ± 3.9 months (median 11.1, IQR 4). Demographical and clinical characteristics at V1 are shown in detail in Table 1. All the 115 pwMS underwent a brain and cervical spinal cord MRI and in 42 patients (36.5%) V1-MRI was also extended to the thoracolumbar region.
Clinical and MRI activity
In the period between V1 and V0, 3 out of 115 pwMS (2.6%) experienced clinical relapses, namely, optic neuritis, and hemispheric syndromes (right leg dysesthesia, and right leg hypoesthesia and weakness, with concomitant brain MRI activity consistent with the described symptoms ). No spinal cord relapses were recorded in the whole cohort. None of the pwMS showed progression in the absence of relapses. Signs of brain MRI activity were detected in 17 (14.8%) out of 115 pwMS. Specifically, 17 pwMS out of 115 (14.8%) had at least one new T2/FLAIR brain lesion while 1 subject out of 115 (0.9%) had an enlarged T2/FLAIR brain lesion. Five subjects out of 115 (4.3%) had at least one brain CEL. Signs of spinal MRI activity were detected in 15 (13%) out of 115 pwMS. In particular, 12 pwMS out of 115 (10.4%) had at least one new T2/STIR spinal cord lesion, while 3 pwMS out of 115 (2.6%) had enlarged T2/STIR spinal cord lesions. Of note, all the 3 pwMS with enlarged T2/STIR lesions also showed brain MRI activity. One subject out of 115 (0.9%) had at least one contrast-enhancing spinal cord lesion. Nine out of 115 pwMS (7.8%) presented only a-SLs without concomitant brain MRI activity. All of the 9 pwMS showed a-SLs in the thoracolumbar region, and only 1 (11.1%) both in the cervical and thoracolumbar regions. Of interest, most of the subjects with a-SLs previously experienced a myelitis (6 out of 9, 66.7%). Treatment type and duration, as well as disease duration did not differ between the nine subjects with a-SLs if compared with the rest of the cohort.
Changes in NEDA status if considering spinal cord MRI data
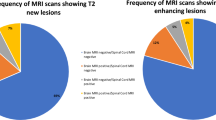
If considering clinical and brain MRI activity, the status of NEDA was achieved in 97 out of 115 pwMS (84.3%), while it was not in 18 out of 115 subjects (15.7%). Among pwMS not classified as NEDA, most of the subjects (15/18, 83.3%) had subclinical brain MRI activity, while a minority experienced relapses (3/18, 16.7%) with (2/18, 11.1%) or without (1/18, 5.6%) concomitant detectable MRI activity. When spinal cord data were taken into account, 88 out of 115 pwMS (76.5%) satisfied NEDA criteria, and the remaining 27 (23.5%) did not (Fig. 1). Among pwMS not achieving NEDA when spinal cord data were considered, 24 out of 27 (88.9%) experienced subclinical brain and/or spinal cord MRI activity. Of these latter, 9 out of 24 (37.5%) showed signs of brain MRI activity only, 6 (25%) of concomitant brain and spinal cord MRI activity, and 9 (37.5%) presented with isolated spinal cord MRI activity. In the cohort of 27 pwMS not achieving NEDA when considering spinal cord imaging data, 3 (11.1%) experienced relapses with (2/27, 7.4%) or without (1/27, 3.7%) concomitant detectable brain MRI activity (Fig. 2). The difference in the proportion of pwMS satisfying NEDA changed significantly when spinal cord data were included (p < 0.01).

Change in the percentage of pwMS satisfying NEDA definition when extending MRI monitoring to the spinal cord. The percentage of pwMS with NEDA decreases significantly from 84.3 to 76.5% if spinal cord MRI is considered (right bar) in addition to brain MRI data only (left bar). NEDA no evidence of disease activity, MRI magnetic resonance imaging

Reasons for the change in the proportion of pwMS not satisfying NEDA definition when extending MRI monitoring to the spinal cord. PwMS shifted from NEDA to EDA exclusively for the evidence of subclinical MRI activity in the spinal cord. EDA evidence of disease activity, NEDA no evidence of disease activity, EDA CLIN-/MRI+ evidence of disease activity demonstrated by subclinical MRI activity in the absence of clinical relapses, EDA CLIN+ evidence of disease activity in the form of clinical relapses
Discussion
Despite the relevance of spinal cord pathology in MS, spinal imaging is not routinely recommended in the longitudinal monitoring of pwMS apart from specific clinical situations [12], and its role in assessing the response to MS treatments has not been clarified so far. The total number of new spinal cord lesions occurring over a period of 1 year was previously found to be lower than that in the brain (new brain lesions/new spinal cord lesions ratio around 8:1), and up to two-thirds of spinal cord lesions have been found to be asymptomatic [13, 23]. In our cohort of pwMS undergoing regular outpatient clinical follow-up and MRI monitoring, 15 out of 115 subjects (13%) showed MRI signs of disease activity in the spinal cord. All the subjects were asymptomatic for spinal cord relapses. Thus, all the observed spinal lesions were asymptomatic in our cohort. Interestingly, 9 out of 15 subjects (60%) did not show, in the same time window, brain MRI activity. Therefore, 7.8% subjects of the entire cohort (9 out of 115) presented only with a-SLs that would have not been detected in the absence of spinal cord imaging. We found that, in this subgroup of 9 pwMS with spinal cord MRI activity only, thoracolumbar region was the most involved region by new a-SLs, while most of the subjects with new and/or enlarged a-SLs in the cervical region had concomitant subclinical brain MRI activity.
The presence of a-SLs has an important role in predicting clinical outcomes even in the very early phases of the disease. For instance, it was previously found that a-SLs in subjects with radiologically isolated syndrome (RIS) are associated with the risk of subsequent development of a relapsing or progressive form of MS, independently of brain lesion load [14]. Furthermore, spinal cord lesions are robust predictors of long-term disease outcomes in relapse-onset MS [24] and early spinal cord lesions (both at time of presentation and over the first three years) are independently associated with physical disability and with development of secondary progressive MS at 15 years [25].
Previous works found an even higher frequency of a-SLs compared to our study. For instance, Zecca et al. found that 25.2% of 103 clinically stable pwMS developed at least one new a-SL over a median follow-up of 17 months, and more than one-third of them were free from asymptomatic brain lesions in the same time window [16]. Recently, a study retrospectively evaluated the frequency of asymptomatic spinal cord combined unique activity (CUA, i.e., new/enlarging T2 lesions or CELs ) on MRI in a cohort of 230 subjects diagnosed with clinically isolated syndrome (CIS) or relapsing-remitting MS (RRMS). The authors found that out of 340 spinal cord MRI scans with spinal cord CUA, 31.2% were from clinically asymptomatic pwMS, and 12.1% were from asymptomatic pwMS without concomitant brain MRI activity, i.e., pwMS with only spinal cord MRI activity [17]. In another retrospective study focused on the occurrence of spinal cord CELs, it was found that 25.2% out of 1180 MRI scans with contrast-enhancing lesions showed CELs in the spinal cord only, in 58% of cases being asymptomatic [26]. These data suggest that asymptomatic spinal cord activity can be found in up to 25% of the subjects undergoing spinal cord MRI monitoring. However, the impact of this evidence on combined measures of disease activity still needs to be defined. For this reason, the main aim of our work was to define if spinal cord imaging significantly influences NEDA definition in pwMS. NEDA is a composite outcome to monitor the disease status and the effectiveness of DMTs in pwMS, and it represents the most stringent standard of therapeutic efficacy in clinical practice [27,28,29]. Whereas brain MRI monitoring in MS is universally accepted, the role of spinal cord monitoring for NEDA definition is debated. Previously, a 7-year longitudinal study evaluating NEDA in a real-world cohort showed that the inclusion of spinal cord imaging to the assessment of MRI activity led to annual variations in the percentage of subjects free of MRI disease activity ranging from 7% to 12% [29]. Recently, a study investigated the role of 3 T spinal cord MRI in the 1-year evaluation of NEDA in a cohort of 61 subjects with CIS, RRMS or secondary progressive MS, among whom 56 received first- or second-line DMTs. This study showed that spinal cord MRI had a low value in addition to brain MRI in the definition NEDA. Indeed, out of 39 pwMS achieving NEDA based on brain imaging, only one subject had activity on spinal cord imaging while showing NEDA on brain imaging [30].
Our study showed that extending MRI to spinal cord in monitoring pwMS under a first-line DMT slightly but significantly influences the definition of the NEDA status. The percentage of pwMS classified as NEDA decreased indeed from 84.3 to 76.5% if the MRI study was extended to the spinal cord. Our findings, thus, demonstrate that spinal cord MRI monitoring has a significant impact in definition of NEDA, reducing by 7.8% the proportion of pwMS satisfying this criterion under first-line DMTs. Whether spinal cord MRI monitoring has practical consequences on therapeutic decisions and long-term outcomes still needs to be demonstrated. Nevertheless, if we consider NEDA as the outcome to be reached in clinical practice, spinal cord MRI could increase the proportion of pwMS that would be considered suboptimal or non-responders to treatments.
Since NEDA is a stringent treatment goal to achieve [20], tolerance of a minimal evidence of disease activity (MEDA) has been claimed as a more realistic goal to strive for [2]. Notably, Prosperini et al. demonstrated that in the first few years of treatment, a marginal MRI activity of one to two new T2 lesions, in the absence of both relapses and CELs, could be tolerated without exposing pwMS at risk of future disability [31]. In this scenario, it would be interesting to test whether spinal cord monitoring also influences MEDA status and/or shifts from NEDA to MEDA.
Our study has several limitations, mostly due to its retrospective design. A selection bias could have been present since inclusion criteria only allowed to recruit subgroup of subjects with first-line DMTs undergoing routine clinical follow-up and MRI monitoring extended to the spinal cord with MRIs always performed in the same scanner. Additionally, for quantitative assessment of brain and spinal lesions we used the inspection-based method. In this context, it is worth noting that enlarged MS lesions lack a universal definition and their detection is subjective and strongly limited by operator-dependent variability [2]. However, only 3 out of 115 subjects (2.6%) in our cohort were classified as having enlarged T2/STIR spinal lesions and all of them also had new T2/FLAIR brain lesions. Thus, neither NEDA definition nor the study results would have been modified by excluding spinal cord lesions classified as enlarged in the follow-up MRI. Interestingly, we detected a low overall clinical disease activity in the cohort (3 out of 115 subjects, 2.6%). A possible explanation deals with the fact that all the subjects were under first-line treatment and that most of them were on such established therapy since a long time (mean treatment duration 35 months). Thus, such selection bias could have led to recruit first-line responder patients with low disease activity. Future prospective studies including subjects under high-efficacy treatments and with longer follow-up times would be useful.
Despite these limitations, our findings are derived by a relatively large sample and by a ‘real-world’ clinical and MRI routine setting, which makes them appliable to the clinical practice of MS monitoring. Further efforts are now warranted to replicate these findings in other independent cohorts, even with a prospective design, and to evaluate if adding spinal cord MRI to brain MRI in MS monitoring in asymptomatic subjects could eventually impact on prognostic evaluation and therapeutic decisions in clinical practice.
References
Giovannoni G, Butzkueven H, Dhib-Jalbut S et al (2016) Brain health: time matters in multiple sclerosis. Mult Scler Relat Disord 9(Suppl. 1):S5–S48. https://doi.org/10.1016/j.msard.2016.07.003
Gasperini C, Prosperini L, Tintoré M et al (2019) Unraveling treatment response in multiple sclerosis: a clinical and MRI challenge. Neurology 92:180–192. https://doi.org/10.1212/WNL.0000000000006810
Rotstein D, Montalban X (2019) Reaching an evidence-based prognosis for personalized treatment of multiple sclerosis. Nat Rev Neurol 15:287–300. https://doi.org/10.1038/s41582-019-0170-8
Sormani MP, De Stefano N (2013) Defining and scoring response to IFN-β in multiple sclerosis. Nat Rev Neurol 9:504–512. https://doi.org/10.1038/nrneurol.2013.146
Giovannoni G, Tomic D, Bright JR, Havrdová E (2017) “No evident disease activity”: the use of combined assessments in the management of patients with multiple sclerosis. Mult Scler 23:1179–1187. https://doi.org/10.1177/1352458517703193
Kearney H, Altmann DR, Samson RS et al (2015) Cervical cord lesion load is associated with disability independently from atrophy in MS. Neurology 84(4):367–373. https://doi.org/10.1212/WNL.0000000000001186
Langer-Gould A, Popat RA, Huang SM et al (2006) Clinical and demographic predictors of long-term disability in patients with relapsing–remitting multiple sclerosis: a systematic review. Arch Neurol 63:1686–1691. https://doi.org/10.1001/archneur.63.12.1686
Kearney H, Miller DH, Ceccarelli O (2015) Spinal cord MRI in multiple sclerosis—diagnostic, prognostic and clinical value. Nat Rev Neurol 11:327–338. https://doi.org/10.1038/nrneurol.2015.80
Arrambide G, Rovira A, Sastre-Garriga J et al (2018) Spinal cord lesions: a modest contributor to diagnosis in clinically isolated syndromes but a relevant prognostic factor. Mult Scler 24:301–312. https://doi.org/10.1177/1352458517697830
Rovira À, Wattjes MP, Tintoré M et al (2015) Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis-clinical implementation in the diagnostic process. Nat Rev Neurol 11(8):471–482. https://doi.org/10.1038/nrneurol.2015.106
Wattjes MP, Rovira A, Miller D et al (2015) Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis—establishing disease prognosis and monitoring patients. Nat Rev Neurol 11:597–606. https://doi.org/10.1038/nrneurol.2015.157
Wattjes MP, Ciccarelli O, Reich DS et al (2021) 2021 MAGNIMS–CMSC–NAIMS consensus reccomandations on the use of MRI in patients with multiple sclerosis. Lancet Neurol S1474–4422(21):00095–00098. https://doi.org/10.1016/S1474-4422(21)00095-8
Thorpe JW, Kidd D, Moseley IF et al (1996) Spinal MRI in patients with suspected multiple sclerosis and negative brain MRI. Brain 119(Pt 3):709–714. https://doi.org/10.1093/brain/119.3.709
Okuda DT, Mowry EM, Cree BAC et al (2011) Asymptomatic spinal cord lesions predict disease progression in radiologically isolated syndrome. Neurology 76(8):686–692. https://doi.org/10.1212/WNL.0b013e31820d8b1d
Sombekke MH, Wattjes MP, Balk LJ et al (2013) Spinal cord lesions in patients with clinically isolated syndrome: a powerful tool in diagnosis and prognosis. Neurology 80:69–75. https://doi.org/10.1212/WNL.0b013e31827b1a67
Zecca C, Disanto G, Sormani MP et al (2016) Relevance of asymptomatic spinal MRI lesions in patients with multiple sclerosis. Mult Scler 22(6):782–791. https://doi.org/10.1177/1352458515599246
Granella F, Tsabtes E, Graziuso S et al (2019) Spinal cord lesions are frequently asymptomatic in relapsing–remitting multiple sclerosis: a retrospective MRI survey. J Neurol 266(12):3031–3037. https://doi.org/10.1007/s00415-019-09526-3
Thompson AJ, Banwell BL, Barkhof F et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17:162–173. https://doi.org/10.1016/S1474-4422(17)30470-2
Filippi M, Rocca MA, Bastianello S et al (2013) Guidelines from The Italian Neurological and Neuroradiological Societies for the use of magnetic resonance imaging in daily life clinical practice of multiple sclerosis patients. Neurol Sci 34(12):2085–2093. https://doi.org/10.1007/s10072-013-1485-7
Parks NE, Flanagan EP, Lucchinetti CF, Wingerchuk DM (2017) NEDA treatment target? No evident disease activity as an actionable outcome in practice. J Neurol Sci 383:31–34. https://doi.org/10.1016/j.jns.2017.10.015
Lublin FD, Coetzee T, Cohen JA et al (2020) The 2013 clinical course descriptors for multiple sclerosis: a clarification. Neurology 94(24):1088–1092. https://doi.org/10.1212/WNL.0000000000009636
Río J, Nos C, Tintoré M et al (2006) Defining the response to interferon-beta in relapsing–remitting multiple sclerosis patients. Ann Neurol 59(2):344–352. https://doi.org/10.1002/ana.20740
Cortese R, Ciccarelli O (2018) Clinical monitoring of multiple sclerosis should routinely include spinal cord imaging—yes. Mult Scler 24(12):1536–1537. https://doi.org/10.1177/1352458518778010
Filippi M, Preziosa P, Barkhof F et al (2021) Diagnosis of progressive multiple sclerosis from the imaging perspective: a review. JAMA Neurol 78(3):351–364. https://doi.org/10.1001/jamaneurol.2020.4689
Brownlee WJ, Altmann DR, Prados F et al (2019) Early imaging predictors of long-term outcomes in relapse-onset multiple sclerosis. Brain 142(8):2276–2287. https://doi.org/10.1093/brain/awz156
Ruggieri S, Logoteta A, Tinelli E et al (2018) Measuring disease activity in multiple sclerosis: the essential role of spinal cord MRI monitoring. Mult Scler 24(S2):1–5. https://doi.org/10.1177/1352458518798575
Havrdova E, Galetta S, Stefoski D, Comi G (2010) Freedom from disease activity in multiple sclerosis. Neurology 74(Suppl 3):S3–S7. https://doi.org/10.1212/WNL.0b013e3181dbb51c
Bevan CJ, Cree BAC (2014) Disease activity free status: a new end point for a new era in multiple sclerosis clinical research? JAMA Neurol 71(3):269–270. https://doi.org/10.1001/jamaneurol.2013.5486
Rotstein DL, Healy BC, Malik MT et al (2015) Evaluation of no evidence of disease activity in a 7-year longitudinal multiple sclerosis cohort. JAMA Neurol 72:152–158. https://doi.org/10.1001/jamaneurol.2014.3537
Tummala S, Singhal T, Oommen VV et al (2017) Spinal cord as an adjunct to brain magnetic resonance imaging in defining “no evidence of disease activity” in multiple sclerosis. Int J MS Care 19(3):158–164. https://doi.org/10.7224/1537-2073.2016-068
Prosperini L, Mancinelli C, Haggiag S et al (2020) Minimal evidence of disease activity (MEDA) in relapsing-remitting multiple sclerosis. J Neurol Neurosurg Psychiatry 91(3):271–277. https://doi.org/10.1136/jnnp-2019-322348
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
EDS received travel grants from Sanofi and Biogen to attend national conferences. LG received travel grants from Almirall, Biogen, Euroimmun, Merck, Mylan, Novartis, Roche, Sanofi and Teva to attend national and international conferences. MDF participated on advisory boards for and received speaker or writing honoraria, research grants and funding for travelling from Bayer, Biogen Idec, Genzyme, Merck, Mylan, Novartis, Roche, Teva and Viatris. SP, AF, GG and LP report no conflict of interests.
Ethical standard statement
All the subjects gave their informed consent. The study was approved by the local ethics committee (CER Umbria, N. 3933/21).
Rights and permissions
About this article

Cite this article
Di Sabatino, E., Gaetani, L., Sperandei, S. et al. The no evidence of disease activity (NEDA) concept in MS: impact of spinal cord MRI. J Neurol 269, 3129–3135 (2022). https://doi.org/10.1007/s00415-021-10901-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10901-2