
Abstract
Increasingly, evidence implicates an important role of neuroinflammation in neurodegeneration progression. Yet, brain imaging has not reached a consistent conclusion that neuroinflammation is involved in the pathogenesis of Parkinson's disease (PD). We aimed to review the evidence to quantitatively assess the existence and spatial distribution of neuroinflammation in the brain of PD patients. We systematically searched literature databases for case–control studies which used positron emission tomography to detect neuroinflammation represented by translocator protein (TSPO) levels in PD patients compared with healthy controls (HC). Standardized mean differences (SMD) were selected as effect sizes and random-effects models were used to combine effect sizes. Subgroup analyses for separate brain regions were conducted. Fifteen studies comprising 455 (HC = 198, PD = 238) participants and 19 brain regions were included. Compared to HC, PD patients had elevated TSPO levels in midbrain, putamen, anterior cingulate, posterior cingulate, thalamus, striatum, frontal, temporal, parietal, occipital, cortex, hippocampus, substantia nigra, pons, cerebellum, and caudate when using 1st-generation ligands. TSPO levels were elevated in the midbrain of PD patients when 2nd-generation ligands were used. We discussed the possible explanations of contrasting difference between these outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson's disease (PD) has the fastest-growing incidence among neurological disorders and is characterized by movement disorder[1]. Beyond motor symptoms, non-motor symptoms are present already at disease onset and some even precede motor symptoms[2]. Characteristic neuropathology of PD includes dopaminergic neurons loss in substantia nigra and widespread intraneuronal α-synuclein accumulation named Lewy bodies [3]. PD is considered to be a disease with a genetic component, and some genes including α-synuclein, LRRK2, PINK1, parkin, and DJ-1 are related to the pathogenesis of PD [4].
The phenomenon of α-synuclein-induced neuronal loss accompanied by inflammatory changes in the brain has been gradually revealed in the last decade [5]. Thus, neuroinflammation may play an important role in PD. Neuroinflammation may not only be a trigger for the onset, but may also promote the progression of PD [6]. Furthermore, clarifying the profile of neuroinflammation offers the possibility to develop neuroprotective therapies and immunotherapy targets [7]. Microgliosis is the hallmark of neuroinflammation and receives more and more attention. It is supported by fluid biomarker, brain imaging and post-mortem studies that microglia have capacity to mediate immunity and initiate neuroinflammation in PD. A meta-analysis showed that PD was accompanied by the increased cerebrospinal fluid inflammatory cytokines, including TGF-β1, IL-6, and IL-1β [8]. Multiple post-mortem analysis found that α-synuclein accumulation and neurodegeneration were accompanied by microglial activation [9]. And positron emission tomography (PET) imaging provides evidence to confirm the ongoing microglial activation in PD [10].
The translocator protein (TSPO) is a mitochondrial translocator protein and has minimal levels in the normal brain [11]. The expression of TSPO is greatly enhanced in neuroinflammation and therefore widely regarded as a suitable biomarker of activated microglia [10]. Thus, PET imaging based on TSPO and its ligand is applied to measure in vivo microglia-mediated neuroinflammation (e.g., multiple sclerosis [12] and Alzheimer's disease [13]). There are mainly two generations of ligands that can be used for quantitative imaging of TSPO. [11C]PK11195 is the first PET ligand of TSPO and the most widely used. However, in vivo PET applications of the [11C]PK11195 ligand are technically challenged, because high lipophilicity of this molecule hampered its specific binding [14]. Compared to 1st-generation ligands, 2nd-generation ligands have improved signal-to-noise ratio and lower nonspecific binding. 2nd-generation ligands show different affinities for TSPO in brain tissue from different subjects, including high-affinity binders, low-affinity binders, and mixed affinity binders (HABs, LABs, and MABs) [15]. Although numerous studies have used TSPO PET in PD patients, they are often limited by relatively few subjects and conflicting results [16]. Therefore, integration of previous independent studies would increase the credibility of the findings and reveal the role of neuroinflammation in the pathogenesis of PD.
Based on the current state of research described above, we performed the first meta-analyses to investigate TSPO levels in controls and PD to systematically assess spatial progression patterns of neuroinflammation in brain.
Methods
Search strategy
All methods were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [17]. We searched peer-reviewed English-language articles from PubMed, Web of Science, The Cochrane Library, EBSCO, and Embase, up to 20st July 2021. The database search terms were as follows: ("positron emission tomography" OR "PET") AND ("TSPO" OR "translocator Protein" OR "18 kDa" OR "neuroinflammation" OR "microglia" OR "benzodiazepine") AND ("Parkinson’s disease" OR "Parkinson disease"). To find additional relevant references, we also manually searched the reference articles included in the retrieved articles. A standardized review protocol (CRD42020218445) has been published in PROSPERO (https://www.crd.york.ac.uk/PROSPERO).
Eligibility criteria
The following criteria were applied to include studies in the meta-analysis: (1) studies were written in English; (2) PET was used to measure TSPO binding; (3) participants were stratified into PD and healthy controls (HC) groups; (4) studies must perform regional analysis; (5) TSPO levels were reported.
Studies should be excluded if they: (1) contained a duplicate study population; (2) did not perform a regional analysis; (3) were an interventional study design.
Data extraction
The following data were extracted from each included study: (1) the sample size in each group; (2) brain regions with data available; (3) the mean value and standard deviation (SD) for TSPO levels in each group; (4) the mean age of subjects in each group; (5) the TSPO ligand used; (6) the outcome used to measure TSPO levels; (7) the proportion of male subjects in each group; (8) the average Unified Parkinson Disease Rating Scale motor (UPDRS-III) scores of subjects in PD group.
Where studies reported separate results for both hemispheres [18,19,20], results were averaged across hemispheres. When studies reported results in graphical format [21,22,23], mean and SD values were estimated using the measurement tool (WebPlotDigitizer-4.2). Where multiple studies utilized the same study population, we selected the study containing the larger study population for inclusion and excluded the duplicate population. When the data were given in terms of median and interquartile spacing, we used an online calculator (http://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html) edited by Professor Tie-Jun Tong to convert the data. Because MABs and HABs differ in TSPO binding [24], we extracted data from patients with HABs and MABs separately to explore the effect of genotype on second-generation ligand analysis.
Quality assessment
We used the Newcastle–Ottawa quality assessment scale for case–control studies to assess the quality of included studies. A maximum score of 9 can be awarded, whereby studies with ≥ 7 points are generally considered to be of high quality.
Statistical analysis
Meta-analysis was performed using Stata 16, when there were ≥ 2 studies for the same region. Effect sizes (ES) were primarily generated from sample size and mean (SD) values. Since TSPO levels were determined using different PET ligands and analytical methods, effect sizes were calculated as standardized mean differences (SMD) between controls and PD groups. A positive result indicates higher TSPO levels in the PD, compared to the HC. Results were meta-analyzed using a random-effects model and reported as SMD and 95% confidence intervals (CI). If significant heterogeneity is found in the studies analyzed, the random-effects model will produce a wider 95% CI than the fixed-effects model [25]. Thus, the random-effects model is regarded as a more conservative approach. The TSPO ligand used in PET studies predominantly included 1st-generation or 2nd-generation ligands. As these have different characteristics, we conducted separate meta-analyses of these ligands.
Statistical heterogeneity across studies was assessed by Cochrane Q test and I2 statistic. I2 statistics of 0.25, 0.50, and 0.75 indicated small, moderate, and high heterogeneity, respectively. To investigate the potential source of heterogeneity, we performed subgroup analysis according to the genotype of TSPO. Sensitivity analysis was undertaken to assess the stability of the result in those regions of statistical heterogeneity. Specifically, the leave-1-out method was applied to investigate the potential effect of single study on the outcome. Egger regression test was performed to test publication bias when the number of studies > 2 in same region. Publication bias was further tested using trim-and-fill analysis, which can impute possible missing studies and correct funnel plot asymmetry.
Results
Study selection
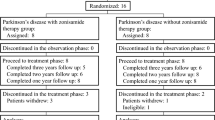
The initial search identified 998 articles, of which 176 were excluded after removal of duplicate results. 789 articles were excluded after scanning of titles and abstracts. The full text of 33 articles was examined. Following this, 18 articles were excluded because they did not meet our inclusion criteria: 8 articles are ongoing clinical trials, 3 articles lack of control group, 4 articles contain a duplicate population, and 3 articles did not report outcomes. In final, a total of 15 articles were included in the meta-analyses (Fig. 1).

Flowchart showing the inclusion of studies for the meta-analysis
Study characteristics
The overall study characteristics, including sample sizes, mean age of subjects, proportion of male subjects, the type of PET ligand used, outcome measures, and subject UPDRS-III scores for each included study is presented in Table 1. Quality scores of the included studies were between 5 and 9 points (see Supporting Information Appendix 2), and the majority them are high quality (≥ 7 points).
In total, there were 19 available regions for meta-analysis. These regions are as follows: midbrain, putamen, anterior cingulate (including: cortex and gyrus), posterior cingulate (including: cortex and gyrus), thalamus, striatum, frontal (including: cortex and lobe), temporal (including: cortex and lobe), medial temporal lobe, parietal (including: lobe, cortex, and lateral), occipital (including: cortex, lobe, medial, and lateral region), cortex (including: whole cortex and cortical), amygdala, hippocampus, substantia nigra, pons, cerebellum, precuneus, caudate.
Seven brain regions were unavailable for meta-analysis because there was only one study in same region. These brain areas include precentral gyrus pallidum, dorsal lateral prefrontal cortex, insula, gray matter, white matter, nucleus accumbens, and limbic cortices.
Studies using 1st-generation ligands
ES estimates pooled by random-effects models demonstrated that PD subjects had significantly higher TSPO levels compared to HC subjects in midbrain, putamen, anterior cingulate, posterior cingulate, thalamus, striatum, frontal, temporal, parietal, occipital, cortex, hippocampus, substantia nigra, pons, cerebellum, and caudate (Fig. 2). The largest effects were seen in temporal. In contrast, medial temporal lobe and amygdala yielded nonsignificant ES estimates (Fig. 2). Significant heterogeneity was detected in 7 of 18 regions. Medial temporal lobe, amygdala, and substantia nigra showed high levels of heterogeneity, whereas putamen, anterior cingulate, temporal, and caudate showed moderate levels of heterogeneity (Supporting Information Appendix 3). Sensitivity analysis was used to investigate sources of heterogeneity. For medial temporal lobe, the quantities of studies were limited. So, we mainly investigated heterogeneity in models of putamen, anterior cingulate, temporal, amygdala, substantia nigra, and caudate. Sensitivity analysis through leave-1-out found the results in anterior cingulate and temporal were stable. In contrast, a single study could influence the statistically significant difference in putamen, amygdale, substantia nigra, and caudate. Importantly, single study could explain the significant heterogeneity in putamen, anterior cingulate, temporal, amygdale, and caudate (Supporting Information Appendix 6). There was no significant publication bias in all brain regions. Analyses by trim-and-fill showed that one missing study was required for midbrain and one missing study for posterior cingulate, two studies for frontal, four studies for temporal, three studies for parietal, four studies for hippocampus. In addition, after imputing potential missing studies, effects did not change (Supporting Information Appendix 8).

Overall standardized mean difference for each region in the comparison between HC and PD subjects was measured by 1st-generation ligands. Results are organized by regional effect size
Studies using 2nd-generation ligands
ES estimates pooled by random-effects models demonstrated that PD subjects had significantly higher TSPO levels compared to HC subjects in midbrain (Fig. 3). In contrast, putamen, thalamus, frontal, temporal, parietal, occipital, cerebellum, precuneus, and caudate yielded nonsignificant ES estimates (Fig. 3). Significant heterogeneity was detected in 4 of 10 regions. Precuneus showed high levels of heterogeneity, whereas putamen, parietal, and caudate showed moderate levels of heterogeneity (Supporting Information Appendix 4). Subgroup analysis was performed based on the genotype of TSPO in models of putamen, temporal, occipital, cerebellum, and caudate. Results showed that the effect of heterogeneity was reduced in most models (Fig. 4). Sensitivity analysis through leave-1-out found the results in parietal and caudate were stable. In contrast, a single study could influence the statistically significant difference in putamen and precuneus. Furthermore, single study could explain the significant heterogeneity in putamen, parietal, and caudate (Supporting Information Appendix 7). There was no evident publication bias in the included brain regions. Analyses from trim-and-fill showed that two missing studies were required for midbrain. After imputing potential missing studies, effects did not change (Supporting Information Appendix 9).

Overall standardized mean difference for each region in the comparison between HC and PD subjects was measured by 2nd-generation ligands. Results are organized by regional effect size

Overall and subgroups standardized mean difference for putamen, temporal, occipital, cerebellum, and caudate measured by 2nd-generation ligands
Discussion
To the best of our knowledge, this study is the first meta-analysis to investigate neuroinflammation in PD, relative to controls. We found significant elevated levels of neuroinflammation in most brain regions of PD patients when using 1st-generation ligands, but only the midbrain showed significant differences when using 2nd-generation ligands.
It is now well established that the main clinical features of PD are caused by damage to dopamine neurons in the midbrain. Our study found significantly elevated TSPO levels in midbrain, suggesting a close interrelationship between microglia activation and PD pathology. On the one hand, aggregates of α‑synuclein promote microglial activation in the early stage of disease. α-synuclein acts as a chemoattractant in migration of microglia [26]. And microglia interacting with different forms of α-synuclein show different phenotypes and display different functional status [27, 28]. Microglia bridge neuroinflammation and α-synuclein-induced neuronal injury, which has profound consequences in the progression of PD [29]. On the other hand, microglia are regarded as the main cell for the removal of extracellular a-synuclein [30]. Phagocytosis of microglia prevents the spread of pathology in brain. However, impaired microglia phagocytosis in PD patients exacerbates the aggregation of pathological α-synuclein, leading to neurodegeneration [31].
This meta-analysis did not find elevated TSPO binding in medial temporal lobe, amygdala, and precuneus. However, some previous studies were inconsistent with our findings. Extensive activation of microglia in amygdala was observed in PD animal models and PD patients [32,33,34], and activated microglia were significantly associated with α-synuclein pathology [32]. The lack of TSPO signal in these regions may be explained by limited sample size and number of studies. This study also found that the cerebellum of PD subjects showed significantly elevated TSPO binding when using 1st-generation ligands. The cerebellum had been selected as the best reference region when TSPO PET images were analyzed in AD subjects [35]. This approach has also been used for PET images of PD patients [20, 36]. Based on our findings, the cerebellum is not recommended as an appropriate reference region, which is supported by other study [37].
The heterogeneity across brain regions ranged from 0 to 90.9%. In this meta-analysis, we combined sensitivity analysis with subgroup analyses to quantify the sources of heterogeneity. The sensitivity analysis suggested that Iannaccone S et al. (2013) partially explained the heterogeneity in 1st-generation ligands group. The reason could be that the PD patients in this study were on average much older compared to the control group. For 2nd-generation ligands group, subgroup analysis suggested that different binding patterns between TSPO and ligands were main source of heterogeneity. Sensitivity analysis showed that Terada T. et al. [19] did not group patients by genotype, which had a significant impact on heterogeneity. However, it should be noted that heterogeneity may also come from other clinical variables, including duration and severity of disease and medication history. Because most of the included studies did not provide detailed information on these clinical variables, this limited our further analysis. Nevertheless, these limitations highlight the value of continuing research to investigate neuroinflammation levels in PD after controlling for relevant clinical variables. Another challenge is that some regional analyses contained relatively few studies, which limits the power of these analyses and limits the detection of publication bias. Obviously, additional studies are warranted, especially those covering more regions.
The result differences between groups using 1st-generation ligands and 2nd-generation ligands could be explained by several influencing factors. First, 2nd-generation ligands display different uptake from [11C]-PK11195 in healthy elderly individuals. Some studies observed no significant relationship between age and [11C]-PK11195 binding [38, 39]. However, the binding of [11C]-DPA713 showed a significant increase in the elderly participants compared with the young participants [40]. Thus, healthy elderly people may not be a useful benchmark for PD patients when using 2nd-generation ligands. Second, the difference in 2nd-generation ligands binding affinity is induced by single-nucleotide polymorphism rs6971 [41]. And rs6971 polymorphism can result in a nonconservative alanine to threonine substitution at position 147 in the TSPO protein, which has been shown to affect the biological functions of TSPO [42, 43]. Lastly, although 1st-generation ligands showed maximal binding in histopathological brain, there was also increased binding on microglia outside the histopathologically defined boundaries [44].
In this study, there are several limitations that need to be disclosed. A major weakness of current PET studies on TSPO is that the ligands used only show the overall level of microglia activation and do not distinguish between the anti-inflammatory and pro-inflammatory states of microglia. With the development of PET imaging techniques, there is a need for ligands that have the ability to differentiate between different inflammatory states. These ligands will be useful to clarify the relationship between neuroinflammation and disease progression and provide further potential for therapeutic monitoring. Second, considering the availability of data, the average level of TSPO in bilateral brain regions was used in this study. Although one study showed no significant difference in binding between the healthy and affected side [19], it remains a potential limitation of the present study. In addition, although SMD somewhat avoids bias from differences in measurement scales, it does not eliminate bias from variability between study populations [45].
This is the first comprehensive meta-analysis to investigate microglia-mediated neuroinflammation in PD. Taken together, our study indicated that neuroinflammation is widely distributed in various brain regions of PD patients when 1st-generation ligands were used for the assay. When 2nd-generation ligands were used, there were significant differences only in the midbrain. To fully understand the spatiotemporal sequence of neuroinflammation, the development of better quality TSPO ligands and further PET longitudinal studies are needed.
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
References
Dorsey ER, Bloem BR (2018) The Parkinson pandemic-A call to action. JAMA Neurol 75(1):9–10. https://doi.org/10.1001/jamaneurol.2017.3299
Pont-Sunyer C, Hotter A, Gaig C, Seppi K, Compta Y, Katzenschlager R, Mas N, Hofeneder D, Brücke T, Bayés A, Wenzel K, Infante J, Zach H, Pirker W, Posada IJ, Álvarez R, Ispierto L, De Fàbregues O, Callén A, Palasí A, Aguilar M, Martí MJ, Valldeoriola F, Salamero M, Poewe W, Tolosa E (2015) The onset of nonmotor symptoms in Parkinson’s disease (the ONSET PD study). Mov Disord 30(2):229–237. https://doi.org/10.1002/mds.26077
Poewe W, Seppi K, Tanner CM, Halliday GM, Brundin P, Volkmann J, Schrag AE, Lang AE (2017) Parkinson disease. Nat Rev Dis Primers 3:17013. https://doi.org/10.1038/nrdp.2017.13
Martin I, Dawson VL, Dawson TM (2011) Recent advances in the genetics of Parkinson’s disease. Annu Rev Genomics Hum Genet 12:301–325. https://doi.org/10.1146/annurev-genom-082410-101440
Ransohoff RM (2016) How neuroinflammation contributes to neurodegeneration. Science 353(6301):777–783. https://doi.org/10.1126/science.aag2590
Joers V, Tansey MG, Mulas G, Carta AR (2017) Microglial phenotypes in Parkinson’s disease and animal models of the disease. Prog Neurobiol 155:57–75. https://doi.org/10.1016/j.pneurobio.2016.04.006
Sanchez-Guajardo V, Barnum CJ, Tansey MG, Romero-Ramos M (2013) Neuroimmunological processes in Parkinson’s disease and their relation to α-synuclein: microglia as the referee between neuronal processes and peripheral immunity. ASN Neuro 5(2):113–139. https://doi.org/10.1042/an20120066
Chen X, Hu Y, Cao Z, Liu Q, Cheng Y (2018) Cerebrospinal fluid inflammatory cytokine aberrations in Alzheimer’s Disease, Parkinson’s Disease and Amyotrophic Lateral Sclerosis: a systematic review and meta-analysis. Front Immunol 9:2122. https://doi.org/10.3389/fimmu.2018.02122
Doorn KJ, Moors T, Drukarch B, van de Berg W, Lucassen PJ, van Dam AM (2014) Microglial phenotypes and toll-like receptor 2 in the substantia nigra and hippocampus of incidental Lewy body disease cases and Parkinson’s disease patients. Acta Neuropathol Commun 2:90. https://doi.org/10.1186/s40478-014-0090-1
Papadopoulos V, Baraldi M, Guilarte TR, Knudsen TB, Lacapère JJ, Lindemann P, Norenberg MD, Nutt D, Weizman A, Zhang MR, Gavish M (2006) Translocator protein (18kDa): new nomenclature for the peripheral-type benzodiazepine receptor based on its structure and molecular function. Trends Pharmacol Sci 27(8):402–409. https://doi.org/10.1016/j.tips.2006.06.005
Banati RB (2002) Visualising microglial activation in vivo. Glia 40(2):206–217. https://doi.org/10.1002/glia.10144
Högel H, Rissanen E, Vuorimaa A, Airas L (2018) Positron emission tomography imaging in evaluation of MS pathology in vivo. Mult Scler 24(11):1399–1412. https://doi.org/10.1177/1352458518791680
Lagarde J, Sarazin M, Bottlaender M (2018) In vivo PET imaging of neuroinflammation in Alzheimer’s disease. J Neural Transm 125(5):847–867. https://doi.org/10.1007/s00702-017-1731-x
Owen DR, Matthews PM (2011) Imaging brain microglial activation using positron emission tomography and translocator protein-specific radioligands. Int Rev Neurobiol 101:19–39. https://doi.org/10.1016/b978-0-12-387718-5.00002-x
Guo Q, Owen DR, Rabiner EA, Turkheimer FE, Gunn RN (2012) Identifying improved TSPO PET imaging probes through biomathematics: the impact of multiple TSPO binding sites in vivo. Neuroimage 60(2):902–910. https://doi.org/10.1016/j.neuroimage.2011.12.078
Belloli S, Morari M, Murtaj V, Valtorta S, Moresco RM, Gilardi MC (2020) Translation imaging in Parkinson’s disease: focus on neuroinflammation. Front Aging Neurosci 12:152. https://doi.org/10.3389/fnagi.2020.00152
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Ouchi Y, Yoshikawa E, Sekine Y, Futatsubashi M, Kanno T, Ogusu T, Torizuka T (2005) Microglial activation and dopamine terminal loss in early Parkinson’s disease. Ann Neurol 57(2):168–175. https://doi.org/10.1002/ana.20338
Terada T, Yokokura M, Yoshikawa E, Futatsubashi M, Kono S, Konishi T, Miyajima H, Hashizume T, Ouchi Y (2016) Extrastriatal spreading of microglial activation in Parkinson’s disease: a positron emission tomography study. Ann Nucl Med 30(8):579–587. https://doi.org/10.1007/s12149-016-1099-2
Lavisse S, Goutal S, Wimberley C, Tonietto M, Bottlaender M, Gervais P, Kuhnast B, Peyronneau MA, Barret O, Lagarde J, Sarazin M, Hantraye P, Thiriez C, Remy P (2021) Increased microglial activation in patients with Parkinson disease using [(18)F]-DPA714 TSPO PET imaging. Parkinsonism Relat Disord 82:29–36. https://doi.org/10.1016/j.parkreldis.2020.11.011
Ghadery C, Koshimori Y, Christopher L, Kim J, Rusjan P, Lang AE, Houle S, Strafella AP (2020) The interaction between neuroinflammation and β-Amyloid in cognitive decline in Parkinson’s disease. Mol Neurobiol 57(1):492–501. https://doi.org/10.1007/s12035-019-01714-6
Koshimori Y, Ko JH, Mizrahi R, Rusjan P, Mabrouk R, Jacobs MF, Christopher L, Hamani C, Lang AE, Wilson AA, Houle S, Strafella AP (2015) Imaging striatal microglial activation in patients with Parkinson’s disease. PLoS ONE 10(9):e0138721. https://doi.org/10.1371/journal.pone.0138721
Varnäs K, Cselényi Z, Jucaite A, Halldin C, Svenningsson P, Farde L, Varrone A (2019) PET imaging of [(11)C]PBR28 in Parkinson’s disease patients does not indicate increased binding to TSPO despite reduced dopamine transporter binding. Eur J Nucl Med Mol Imaging 46(2):367–375. https://doi.org/10.1007/s00259-018-4161-6
Kreisl WC, Jenko KJ, Hines CS, Lyoo CH, Corona W, Morse CL, Zoghbi SS, Hyde T, Kleinman JE, Pike VW, McMahon FJ, Innis RB (2013) A genetic polymorphism for translocator protein 18 kDa affects both in vitro and in vivo radioligand binding in human brain to this putative biomarker of neuroinflammation. J Cereb Blood Flow Metab 33(1):53–58. https://doi.org/10.1038/jcbfm.2012.131
Masi A, Quintana DS, Glozier N, Lloyd AR, Hickie IB, Guastella AJ (2015) Cytokine aberrations in autism spectrum disorder: a systematic review and meta-analysis. Mol Psychiatry 20(4):440–446. https://doi.org/10.1038/mp.2014.59
Wang S, Chu CH, Stewart T, Ginghina C, Wang Y, Nie H, Guo M, Wilson B, Hong JS, Zhang J (2015) α-Synuclein, a chemoattractant, directs microglial migration via H2O2-dependent Lyn phosphorylation. Proc Natl Acad Sci U S A 112(15):E1926-1935. https://doi.org/10.1073/pnas.1417883112
Barkholt P, Sanchez-Guajardo V, Kirik D, Romero-Ramos M (2012) Long-term polarization of microglia upon α-synuclein overexpression in nonhuman primates. Neuroscience 208:85–96. https://doi.org/10.1016/j.neuroscience.2012.02.004
Sanchez-Guajardo V, Febbraro F, Kirik D, Romero-Ramos M (2010) Microglia acquire distinct activation profiles depending on the degree of alpha-synuclein neuropathology in a rAAV based model of Parkinson’s disease. PLoS ONE 5(1):e8784. https://doi.org/10.1371/journal.pone.0008784
Gao HM, Zhang F, Zhou H, Kam W, Wilson B, Hong JS (2011) Neuroinflammation and α-synuclein dysfunction potentiate each other, driving chronic progression of neurodegeneration in a mouse model of Parkinson’s disease. Environ Health Perspect 119(6):807–814. https://doi.org/10.1289/ehp.1003013
Lee HJ, Suk JE, Bae EJ, Lee SJ (2008) Clearance and deposition of extracellular alpha-synuclein aggregates in microglia. Biochem Biophys Res Commun 372(3):423–428. https://doi.org/10.1016/j.bbrc.2008.05.045
Choi YR, Kang SJ, Kim JM, Lee SJ, Jou I, Joe EH, Park SM (2015) FcγRIIB mediates the inhibitory effect of aggregated α-synuclein on microglial phagocytosis. Neurobiol Dis 83:90–99. https://doi.org/10.1016/j.nbd.2015.08.025
Kouli A, Camacho M, Allinson K, Williams-Gray CH (2020) Neuroinflammation and protein pathology in Parkinson’s disease dementia. Acta Neuropathol Commun 8(1):211. https://doi.org/10.1186/s40478-020-01083-5
Leal MC, Casabona JC, Puntel M, Pitossi FJ (2013) Interleukin-1β and tumor necrosis factor-α: reliable targets for protective therapies in Parkinson’s Disease? Front Cell Neurosci 7:53. https://doi.org/10.3389/fncel.2013.00053
Gordon R, Albornoz EA, Christie DC, Langley MR, Kumar V, Mantovani S, Robertson AAB, Butler MS, Rowe DB, O’Neill LA, Kanthasamy AG, Schroder K, Cooper MA, Woodruff TM (2018) Inflammasome inhibition prevents α-synuclein pathology and dopaminergic neurodegeneration in mice. Sci Transl Med. https://doi.org/10.1126/scitranslmed.aah4066
Schuitemaker A, van Berckel BN, Kropholler MA, Kloet RW, Jonker C, Scheltens P, Lammertsma AA, Boellaard R (2007) Evaluation of methods for generating parametric (R-[11C]PK11195 binding images. J Cereb Blood Flow Metab 27(9):1603–1615. https://doi.org/10.1038/sj.jcbfm.9600459
Kang Y, Mozley PD, Verma A, Schlyer D, Henchcliffe C, Gauthier SA, Chiao PC, He B, Nikolopoulou A, Logan J, Sullivan JM, Pryor KO, Hesterman J, Kothari PJ, Vallabhajosula S (2018) Noninvasive PK11195-PET image analysis techniques can detect abnormal cerebral microglial activation in Parkinson’s disease. J Neuroimaging 28(5):496–505. https://doi.org/10.1111/jon.12519
Bartels AL, Willemsen AT, Doorduin J, de Vries EF, Dierckx RA, Leenders KL (2010) [11C]-PK11195 PET: quantification of neuroinflammation and a monitor of anti-inflammatory treatment in Parkinson’s disease? Parkinsonism Relat Disord 16(1):57–59. https://doi.org/10.1016/j.parkreldis.2009.05.005
Debruyne JC, Versijpt J, Van Laere KJ, De Vos F, Keppens J, Strijckmans K, Achten E, Slegers G, Dierckx RA, Korf J, De Reuck JL (2003) PET visualization of microglia in multiple sclerosis patients using [11C]PK11195. Eur J Neurol 10(3):257–264. https://doi.org/10.1046/j.1468-1331.2003.00571.x
Yasuno F, Ota M, Kosaka J, Ito H, Higuchi M, Doronbekov TK, Nozaki S, Fujimura Y, Koeda M, Asada T, Suhara T (2008) Increased binding of peripheral benzodiazepine receptor in Alzheimer’s disease measured by positron emission tomography with [11C]DAA1106. Biol Psychiatry 64(10):835–841. https://doi.org/10.1016/j.biopsych.2008.04.021
Yokokura M, Terada T, Bunai T, Nakaizumi K, Takebayashi K, Iwata Y, Yoshikawa E, Futatsubashi M, Suzuki K, Mori N, Ouchi Y (2017) Depiction of microglial activation in aging and dementia: Positron emission tomography with [(11)C]DPA713 versus [(11)C]( R)PK11195. J Cereb Blood Flow Metab 37(3):877–889. https://doi.org/10.1177/0271678x16646788
Owen DR, Yeo AJ, Gunn RN, Song K, Wadsworth G, Lewis A, Rhodes C, Pulford DJ, Bennacef I, Parker CA, StJean PL, Cardon LR, Mooser VE, Matthews PM, Rabiner EA, Rubio JP (2012) An 18-kDa translocator protein (TSPO) polymorphism explains differences in binding affinity of the PET radioligand PBR28. J Cereb Blood Flow Metab 32(1):1–5. https://doi.org/10.1038/jcbfm.2011.147
Costa B, Pini S, Gabelloni P, Da Pozzo E, Abelli M, Lari L, Preve M, Lucacchini A, Cassano GB, Martini C (2009) The spontaneous Ala147Thr amino acid substitution within the translocator protein influences pregnenolone production in lymphomonocytes of healthy individuals. Endocrinology 150(12):5438–5445. https://doi.org/10.1210/en.2009-0752
Costa B, Pini S, Martini C, Abelli M, Gabelloni P, Landi S, Muti M, Gesi C, Lari L, Cardini A, Galderisi S, Mucci A, Lucacchini A, Cassano GB (2009) Ala147Thr substitution in translocator protein is associated with adult separation anxiety in patients with depression. Psychiatr Genet 19(2):110–111. https://doi.org/10.1097/YPG.0b013e32832080f6
Banati RB, Newcombe J, Gunn RN, Cagnin A, Turkheimer F, Heppner F, Price G, Wegner F, Giovannoni G, Miller DH, Perkin GD, Smith T, Hewson AK, Bydder G, Kreutzberg GW, Jones T, Cuzner ML, Myers R (2000) The peripheral benzodiazepine binding site in the brain in multiple sclerosis: quantitative in vivo imaging of microglia as a measure of disease activity. Brain 123(Pt 11):2321–2337. https://doi.org/10.1093/brain/123.11.2321
Lin L, Aloe AM (2021) Evaluation of various estimators for standardized mean difference in meta-analysis. Stat Med 40(2):403–426. https://doi.org/10.1002/sim.8781
Gerhard A, Pavese N, Hotton G, Turkheimer F, Es M, Hammers A, Eggert K, Oertel W, Banati RB, Brooks DJ (2006) In vivo imaging of microglial activation with [11C](R)-PK11195 PET in idiopathic Parkinson's disease. Neurobiol Dis 21(2):404–412. https://doi.org/10.1016/j.nbd.2005.08.002
Edison P, Ahmed I, Fan Z, Hinz R, Gelosa G, Ray Chaudhuri K, Walker Z, Turkheimer FE, Brooks DJ (2013) Microglia amyloid and glucose metabolism in Parkinson’s disease with and without dementia. Neuropsychopharmacology 38(6):938–949. https://doi.org/10.1038/npp.2012.255
Iannaccone S, Cerami C, Alessio M, Garibotto V, Panzacchi A, Olivieri S, Gelsomino G, Moresco RM, Perani D (2013) In vivo microglia activation in very early dementia with Lewy bodies comparison with Parkinson's disease. Parkinsonism Relat Disord 19(1):47–52. https://doi.org/10.1016/j.parkreldis.2012.07.002
Kobylecki C, Counsell SJ, Cabanel N, Wächter T, Turkheimer FE, Eggert K, Oertel W, Brooks DJ, Gerhard A (2013) Diffusion-weighted imaging and its relationship to microglial activation in Parkinsonian syndromes. Parkinsonism Relat Disord 19(5):527–532. https://doi.org/10.1016/j.parkreldis.2013.01.017
Fan Z, Aman Y, Ahmed I, Chetelat G, Landeau B, Ray Chaudhuri K, Brooks DJ, Edison P (2015) Influence of microglial activation on neuronal function in Alzheimer's and Parkinson's disease dementia. Alzheimer's Dement 11(6):608–610. https://doi.org/10.1016/j.jalz.2014.06.016
Grazia D, Siddharth F, Atkinson N, Fan Z, Brooks DJ, Edison P (2016) Does microglial activation influence hippocampal volume and neuronal function in Alzheimer’s disease and Parkinson’s disease dementia? J Alzheimer's Dis 51(4):1275–1289. https://doi.org/10.3233/JAD-150827
Ghadery C, Koshimori Y, Coakeley S, Harris M, Rusjan P, Kim J, Houle S, Strafella AP (2017) Microglial activation in Parkinson’s disease using [18F]-FEPPA. J Neuroinflamm. https://doi.org/10.1186/s12974-016-0778-1
Funding
This study was supported by grants from the National Natural Science Foundation of China (81771148).
Author information
Authors and Affiliations
Contributions
Peng-Fei Zhang and Fan Gao contributed equally to this study.
Corresponding author
Ethics declarations
Conflicts of interest
Nothing to declare.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zhang, PF., Gao, F. Neuroinflammation in Parkinson's disease: a meta-analysis of PET imaging studies. J Neurol 269, 2304–2314 (2022). https://doi.org/10.1007/s00415-021-10877-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10877-z