
Abstract
Objective
This study investigates the mismatch between the National Institutes of Health Stroke Scale (NIHSS) score and the computed tomography (CT) findings measured by the Alberta Stroke Program Early CT Score (ASPECTS) for predicting the functional outcome and safety of intravenous thrombolysis (IVT) treatment in patients with acute ischemic stroke (AIS).
Methods
This prospective observational study includes patients with AIS who underwent CT imaging within 4.5 h of the onset of symptoms. Patients were divided into the NIHSS–ASPECTS mismatch (NAM)-positive and NAM-negative groups (group P and N, respectively). The clinical outcome was assessed using the Modified Rankin Scale (mRS). Safety outcomes included progression, symptomatic intracerebral hemorrhage (sICH), intracerebral hemorrhage (ICH), adverse events, clinical adverse events, and mortality.
Results
A total of 208 patients were enrolled in the study. In group P, IVT treatment was associated with a good functional outcome at 3 months (p = 0.005) and 1 year (p = 0.001). A higher percentage of patients with favorable mRS (0–2) (p = 0.01) and excellent mRS (0–1) (p = 0.011) functional outcomes was obtained at 1 year in group P with IVT treatment. Group N did not benefit from the same treatment (p = 0.352 and p = 0.480 at 3 months and 1 year, respectively). There were no statistically significant differences in sICH, ICH, mortality rates, or other risks between the IVT and conventional treatment groups.
Conclusion
IVT treatment is associated with a good functional outcome in patients with NAM, without increasing the risks of sICH, ICH, mortality, or other negative outcomes. NAM promises to be an easily obtained indicator for guiding the treatment decisions of AIS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute ischemic stroke (AIS) accounts for approximately 70–80% of strokes and is among the leading causes of death and disability worldwide [1, 2]. Restoration of blood perfusion in the ischemic penumbra is a determining factor in the functional outcome of patients with AIS. Intravenous thrombolysis (IVT) treatment with recombinant tissue plasminogen activator (rt-PA) within 4.5 h of the onset of the stroke is an effective treatment for AIS [3]. However, because of the narrow time window for IVT treatment, patients may not receive the treatment, even if the ischemic penumbra persists for up to 24 h [4]. Therefore, there is an urgent need for effective ways to identify the state of the ischemic penumbra and to evaluate the accompanying risks to extend the time window for safe and effective IVT treatment.
The mismatch between stroke severity and lesions detected by imaging has been shown to predict the occurrence of ischemic penumbra and to guide AIS treatment [5, 6]. Previous research implied that a clinical–diffusion mismatch could serve as an indicator of infarct growth in patients with AIS [7]. However, as there can be a significant delay associated with magnetic resonance imaging (MRI), owing to the limited availability of this technology, ischemic infarction volume can progress to the point where IVT is no longer an option. Some studies have suggested that computed tomography (CT) findings measured by the Alberta Stroke Program Early CT Score (ASPECTS) are an accurate indicator of the clinical outcome [8, 9]. A previous study implied that clinical–ASPECT mismatch does not identify patients who would benefit from IVT treatment with rt-PA [10]. However, there have been no further studies evaluating whether the combination of ASPECTS and clinical deficits can reliably serve as a surrogate for ischemic penumbra and predict functional outcome, which would help to identify patients who have experienced a stroke who may benefit from IVT treatment beyond the accepted post-stroke time window. To address this question, the present study investigates the correlation between the National Institutes of Health Stroke Scale (NIHSS) score and ASPECTS mismatch (NAM) and the IVT treatment outcome in patients with ischemic stroke. An NIHSS score ≥ 8 has been suggested as a clinical indicator of a large volume of ischemic brain tissue [5], while an ASPECTS ≤ 7 is associated with severe radiological findings [10]. We, therefore, defined NAM as having an NIHSS score ≥ 8 and an ASPECTS ≥ 8 and examined its utility for detecting ischemic penumbra and guiding IVT treatment.
Materials and methods
Patient selection and study design
This prospective observational study enrolled patients with AIS who were admitted to the Shanghai Ninth People’s Hospital between October 2015 and January 2018. The inclusion criteria were as follows: (1) patients with symptoms of AIS, (2) less than 4.5 h from the onset of the stroke to admission, (3) age 18–80 years, and (4) informed consent signed by the patient or their relatives. Exclusion criteria were as follows: (1) history of severe brain trauma or stroke in the previous 3 months, (2) intracranial hemorrhage, (3) previous thrombectomy or other endovascular treatment, and (4) missing clinical 3-month or 1-year Modified Rankin Scale (mRS) scores. A total of 208 patients were included in the study.
We carried out a controlled clinical study, in which we defined group P as patients with an NIHSS score ≥ 8 points and an ASPECTS ≥ 8 points. The remaining subjects were placed into group N. NIHSS and mRS scores were determined by the neurologist who treated the patient, and ASPECTS was determined by consensus between two stroke neurologists, with one rater blinded to the clinical information of the patients. Each group was further divided into two subgroups according to whether thrombolytic treatment was administered. Therefore, there was a total of four groups: group P with thrombolytic or conventional treatment (PT and PC subgroups, respectively), and group N with thrombolytic or conventional treatment (NT and NC subgroups, respectively). Patients in the thrombolytic treatment group were treated by intravenous administration of rt-PA (0.9 mg/kg). The total dose was divided and 10% was injected within 1 min, and the remaining 90% was continuously administered over the next hour using a pump. A brain CT was performed 24 h later. If there was no obvious intracerebral hemorrhage (ICH), anti-platelet drugs and circulation-enhancing drugs, such as butylphthalide and human urinary kininogenase (included in the Guidelines for Ischemic Stroke in China), were added. Patients in the conventional treatment group were only given anti-platelet and circulation-enhancing drugs.
Outcome measures
The clinical outcome was determined based on the mRS score at the 3-month and 1-year follow-ups, through outpatient visits or telephone calls. The physician who performed the NIHSS and the mRS score assessments was specially trained. Safety outcomes, such as progression, symptomatic ICH (sICH), ICH, adverse events, clinical adverse events, and mortality, were compared between the corresponding subgroups. Progression was defined as an NIHSS score ≥ 2 points higher at discharge than at admission. sICH was defined as any hemorrhage with neurologic deterioration or resulting in death within 2 weeks after admission. Adverse events were progression and ICH, and clinical adverse events were progression and sICH. Mortality was defined as the percentage of deaths between the time of admission and the 1-year follow-up.
Statistical analysis
Data are expressed as mean ± standard deviation. SPSS 19.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The Student’s t test or the Mann–Whitney U test was used to evaluate differences in continuous variables between two groups, while comparisons between three groups were carried out using one-way analysis of variance followed by the Dunnett’s test or the Kruskal–Wallis H test. Pearson’s χ2 test or Fisher’s exact test was used to compare categorical variables. The Kolmogorov–Smirnov test was used to evaluate whether data were normally distributed. All reported p values in the study are two-sided, and p < 0.05 was considered statistically significant.
Results
Clinical characteristics of the study population
Between October 2015 and January 2018, 345 patients with AIS were recorded in the endovascular registry, of which 208 patients (60.2%) were enrolled in the present study after 18 patients were excluded because of severe brain trauma or stroke in the previous 3 months, 35 for ICH, 10 for thrombectomy or other endovascular treatments, and 9 for missing follow-up data (Fig. 1). The characteristics and risk factors of the patient subgroups are shown in Table 1. There was no statistically significant difference in the NIHSS score at admission between the PT and PC groups (p = 0.62) or between the NT and NC groups (p = 0.06). In addition, there was no significant difference in the mRS score at admission between the PT and PC groups (p = 0.99) or between the NT and NC groups (p = 0.26). There were no differences in other variables between each pair of subgroups (p > 0.05).

Patient selection algorithm
Clinical outcomes
We compared the clinical outcomes of IVT treatment in the NAM-positive and NAM-negative groups (group P and N, respectively). There were significant differences in the mRS scores between the PT and PC groups at the 3-month (p = 0.005) and the 1-year (p = 0.001) follow-ups (Table 2). The scores were lower in the PT (1.55 ± 1.55) than in the PC group (3.15 ± 1.87). There were no differences in the mRS scores between the NT and NC groups at 3 months (p = 0.352) and 1 year (p = 0.480). This implies that in the absence of NAM, IVT treatment did not lead to a better functional outcome. We compared the mRS scores over time in groups P and N and found that they decreased over time in the PT group (p < 0.001) when compared with the PC group (p = 0.299) (Fig. 2a), indicating a better long-term outcome in the former group. However, there was no declining trend in the mRS score over time in the NT and NC groups (Fig. 2b).

mRS score at admission, discharge, and at the 3-month and 1-year follow-ups. a, b mRS score of PT and PC groups (P group; a) and NT and NC groups (N group; b). **p < 0.01; ***p < 0.001
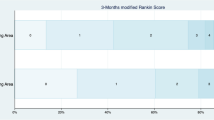
At 1 year follow-up, in group PT, a favorable functional outcome (mRS score ≤ 2) was achieved in 26 patients (83.9%), compared with 10 (50%) in group PC (p = 0.01). In group PT, an excellent functional outcome (mRS score ≤ 1) was achieved in 19 patients (61.3%), compared with 5 (25%) in group PC (p = 0.011) (Fig. 3). These results suggest that thrombolytic therapy in group P is associated with a favorable or excellent functional outcome.

Distribution of mRS scores at the 1-year follow-up in the P group
In terms of safety outcomes, there was no significant difference in the incidence of ICH between the PT and PC groups (19.4% vs 5.0%, p = 0.223) or between the NT and NC groups (7.2% vs 1.1%, p = 0.087). sICH occurred in one patient in each of the PT and PC groups (3.2% and 5.0%, respectively), with no significant difference between the two groups (p = 1.000). Five patients (9.8%) in group P died, including two (6.5%) in group PT and three (15%) in group PC (p = 0.369). Two patients (2.9%) in group N died, group [both in the NT group (p = 0.192)]. There were no differences in progression, adverse events, or clinical adverse events between the PT and PC groups or between the NT and NC groups (p > 0.05) (Table 2).
Discussion
The results of this prospective observational study show that in patients with AIS and NAM, i.e., group P, IVT treatment given within 4.5 h resulted in neurological improvement and a favorable clinical outcome at 3 months and 1 year, without an increased risk of ICH, sICH, or mortality. In contrast, patients without a mismatch, i.e., group N, did not benefit from IVT treatment when compared with conventional therapy. In addition, IVT treatment resulted in a higher percentage of patients with an excellent functional outcome (mRS score ≤ 1) when compared with conventional treatment in group P.
The time window for IVT treatment in patients with AIS is 4.5 h [11]. However, recent studies have demonstrated that IVT treatment beyond 4.5 h has clinical benefits in some patients with salvageable brain tissue [12, 13]. Therefore, there is a need for ways to identify patients with ischemic penumbra who are candidates for IVT treatment beyond 4.5 h. Several methods have been proposed for evaluating ischemic penumbra. Diffusion-weighted imaging (DWI)–perfusion-weighted imaging (PWI) mismatch, DWI–fluid-attenuated inversion recovery mismatch, or NIHSS–DWI–ASPECTS mismatch is indicative of ischemic penumbra, and these cases were shown to benefit from rt-PA treatment [6, 14, 15]. However, MRI is inaccessible in many places, time-consuming, and complicated, which limits its clinical utility within the AIS timeframe. Other trials have reported that CT perfusion (CTP) is useful for identifying the final infarction core and measuring hypoperfusion volume, which can predict the functional outcome of patients with AIS [16, 17]. CTP imaging does not involve whole-brain imaging or a lengthy procedure. Non-contrast CT images evaluated with ASPECTS, which is the most common approach in clinical practice, overcome the limitations of other methods with its availability and simplicity, without the need for time-consuming image processing. Especially in unusual times, such as the coronavirus period, CT is more accessible in remote areas. ASPECTS has been used to accurately predict infarction volume and functional outcomes in patients with AIS receiving endovascular therapy [18, 19]. NIHSS has also been validated for selecting candidate patients for IVT treatment [20]. Therefore, we speculate that a more accurate prediction of functional outcome can be achieved by combining the NIHSS score with the imaging results measured by ASPECTS. We found that IVT treatment within 4.5 h resulted in a lower mRS score at 3 months and 1 year when compared with conventional treatment in NAM-positive patients. However, in NAM-negative patients, the type of treatment had no effect on the mRS score at these time points. Regarding the safety of IVT treatment, a higher percentage of patients experienced ICH in group PT than in group PC (6% vs 1%), but the difference was not statistically significant. This implies that thrombolytic therapy benefits NAM-positive patients without increasing the associated risks. The better long-term functional outcome of IVT treatment in group P than in group N may be attributable to the presence of salvageable brain tissue, i.e., the ischemic penumbra, in the former patients. NAM is indicative of a disparity between the severity of clinical symptoms and imaging findings, implying the existence of an ischemic penumbra that was not detected by CT at the time of admission. Therefore, an ischemic penumbra is a selection criterion for IVT treatment beyond the limited AIS time window.
This study had some limitations. First, the patients were admitted within 4.5 h of AIS, and we did not examine those who received IVT treatment after 4.5 h. However, a previous study reported that in cases with a DWI–PWI mismatch, the proportion of salvageable brain tissue is independent of the time since the ischemic event [14]. Second, given the single-center design and small sample size of our study, further research is needed to confirm our findings.
Conclusions
In conclusion, we demonstrated, for the first time, that IVT treatment resulted in neurologic improvement and a better functional outcome at 3 months and 1 year in patients with AIS and NAM-positive. Nevertheless, there is no significant difference in the outcome of NAM-negative patients whether to receive IVT treatment. These results suggest that NAM can serve as a marker for ischemic penumbra to select patients who would benefit from IVT treatment beyond the 4.5 h post-stroke time window and to predict their functional outcome, thereby improving the long-term prognosis of patients with AIS.
Availability of data and materials
Raw data and information for patients in this study are not publicly available to protect their privacy, but are available from the corresponding author on reasonable request and with the permission of the local ethics committee.
References
Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Wolf ME, Hennerici MG (2013) The ASCOD phenotyping of ischemic stroke (Updated ASCO Phenotyping). Cerebrovasc Dis (Basel, Switz) 36:1–5. https://doi.org/10.1159/000352050
Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS (2019) Heart Disease and Stroke Statistics-2019 update: a report from the American Heart Association. Circulation 139:e56–e528. https://doi.org/10.1161/cir.0000000000000659
Xiong Y, Manwani B, Fisher M (2019) Management of acute ischemic stroke. Am J Med 132:286–291. https://doi.org/10.1016/j.amjmed.2018.10.019
Kate M, Wannamaker R, Kamble H, Riaz P, Gioia LC, Buck B, Jeerakathil T, Smyth P, Shuaib A, Emery D, Butcher K (2018) Penumbral imaging-based thrombolysis with tenecteplase is feasible up to 24 hours after symptom onset. J Stroke 20:122–130. https://doi.org/10.5853/jos.2017.00178
Tei H, Uchiyama S, Usui T (2007) Clinical-diffusion mismatch defined by NIHSS and ASPECTS in non-lacunar anterior circulation infarction. J Neurol 254:340–346. https://doi.org/10.1007/s00415-006-0368-8
Terasawa Y, Kimura K, Iguchi Y, Kobayashi K, Aoki J, Shibazaki K, Kaji R (2010) Could clinical diffusion-mismatch determined using DWI ASPECTS predict neurological improvement after thrombolysis before 3 h after acute stroke? J Neurol Neurosurg Psychiatry 81:864–868. https://doi.org/10.1136/jnnp.2009.190140
Nogueira RG, Kemmling A, Souza LM, Payabvash S, Hirsch JA, Yoo AJ, Lev MH (2017) Clinical diffusion mismatch better discriminates infarct growth than mean transit time-diffusion weighted imaging mismatch in patients with middle cerebral artery-M1 occlusion and limited infarct core. J Neurointerv Surg 9:127–130. https://doi.org/10.1136/neurintsurg-2014-011602
Raza SA, Barreira CM, Rodrigues GM, Frankel MR, Haussen DC, Nogueira RG, Rangaraju S (2019) Prognostic importance of CT ASPECTS and CT perfusion measures of infarction in anterior emergent large vessel occlusions. J Neurointerv Surg 11:670–674. https://doi.org/10.1136/neurintsurg-2018-014461
Sarraj A, Hassan AE, Grotta J, Sitton C, Cutter G, Cai C, Chen PR, Imam B, Pujara D, Arora A, Reddy S, Parsha K, Riascos RF, Vora N, Abraham M, Edgell R, Hellinger F, Haussen DC, Blackburn S, Kamal H, Barreto AD, Martin-Schild S, Lansberg M, Gupta R, Savitz S, Albers GW (2020) Optimizing patient Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT): a prospective multicenter cohort study of imaging selection. Ann Neurol. https://doi.org/10.1002/ana.25669
Kent DM, Hill MD, Ruthazer R, Coutts SB, Demchuk AM, Dzialowski I, Wunderlich O, von Kummer R (2005) “Clinical-CT mismatch” and the response to systemic thrombolytic therapy in acute ischemic stroke. Stroke 36:1695–1699. https://doi.org/10.1161/01.STR.0000173397.31469.4b
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL (2019) Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 50:e344–e418. https://doi.org/10.1161/str.0000000000000211
Ma H, Campbell BCV, Parsons MW, Churilov L, Levi CR, Hsu C, Kleinig TJ, Wijeratne T, Curtze S, Dewey HM, Miteff F, Tsai CH, Lee JT, Phan TG, Mahant N, Sun MC, Krause M, Sturm J, Grimley R, Chen CH, Hu CJ, Wong AA, Field D, Sun Y, Barber PA, Sabet A, Jannes J, Jeng JS, Clissold B, Markus R, Lin CH, Lien LM, Bladin CF, Christensen S, Yassi N, Sharma G, Bivard A, Desmond PM, Yan B, Mitchell PJ, Thijs V, Carey L, Meretoja A, Davis SM, Donnan GA (2019) Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N Engl J Med 380:1795–1803. https://doi.org/10.1056/NEJMoa1813046
Tang TY, Jiao Y, Cui Y, Zhao DL, Zhang Y, Wang Z, Meng XP, Yin XD, Yang YJ, Teng GJ, Ju SH (2020) Penumbra-based radiomics signature as prognostic biomarkers for thrombolysis of acute ischemic stroke patients: a multicenter cohort study. J Neurol. https://doi.org/10.1007/s00415-020-09713-7
Ma H, Wright P, Allport L, Phan TG, Churilov L, Ly J, Zavala JA, Arakawa S, Campbell B, Davis SM, Donnan GA (2015) Salvage of the PWI/DWI mismatch up to 48 h from stroke onset leads to favorable clinical outcome. Int J Stroke 10:565–570. https://doi.org/10.1111/ijs.12203
Berthezene Y, Eker O, Makris N, Bettan M, Mansuy A, Chabrol A, Mikkelsenm IK, Hermier M, Mechtouff L, Ong E, Derex L, Berner LP, Ameli R, Pedraza S, Thomalla G, Ostergaard L, Baron JC, Cho TH, Nighoghossian N (2018) Collateral circulation assessment within the 4.5 h time window in patients with and without DWI/FLAIR MRI mismatch. J Neurol Sci 394:94–98. https://doi.org/10.1016/j.jns.2018.09.013
Rava RA, Snyder KV, Mokin M, Waqas M, Allman AB, Senko JL, Podgorsak AR, Shiraz Bhurwani MM, Hoi Y, Siddiqui AH, Davies JM, Levy EI, Ionita CN (2020) Assessment of a Bayesian Vitrea CT perfusion analysis to predict final infarct and penumbra volumes in patients with acute ischemic stroke: a comparison with RAPID. Am J Neuroradiol. https://doi.org/10.3174/ajnr.A6395
Feil K, Reidler P, Kunz WG, Kupper C, Heinrich J, Laub C, Muller K, Voglein J, Liebig T, Dieterich M, Kellert L (2020) Addressing a real-life problem: treatment with intravenous thrombolysis and mechanical thrombectomy in acute stroke patients with an extended time window beyond 4.5 h based on computed tomography perfusion imaging. Eur J Neurol 27:168–174. https://doi.org/10.1111/ene.14051
Yoo AJ, Berkhemer OA, Fransen PSS, van den Berg LA, Beumer D, Lingsma HF, Schonewille WJ, Sprengers MES, van den Berg R, van Walderveen MAA, Beenen LFM, Wermer MJH, Nijeholt G, Boiten J, Jenniskens SFM, Bot JCJ, Boers AMM, Marquering HA, Roos Y, van Oostenbrugge RJ, Dippel DWJ, van der Lugt A, van Zwam WH, Majoie C (2016) Effect of baseline Alberta Stroke Program Early CT Score on safety and efficacy of intra-arterial treatment: a subgroup analysis of a randomised phase 3 trial (MR CLEAN). Lancet Neurol 15:685–694. https://doi.org/10.1016/s1474-4422(16)00124-1
Goyal M, Menon BK, Coutts SB, Hill MD, Demchuk AM (2011) Effect of baseline CT scan appearance and time to recanalization on clinical outcomes in endovascular thrombectomy of acute ischemic strokes. Stroke 42:93–97. https://doi.org/10.1161/strokeaha.110.594481
Bandettini di Poggio M, Finocchi C, Brizzo F, Altomonte F, Bovis F, Mavilio N, Serrati C, Malfatto L, Mancardi G, Balestrino M (2019) Management of acute ischemic stroke, thrombolysis rate, and predictors of clinical outcome, Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of. Clin Neurophysiol 40:319–326. https://doi.org/10.1007/s10072-018-3644-3
Funding
This work was financially supported by the National Natural Science Foundation of China (Grant No. 81670735); Wu Jieping Medical Foundation (Grant No.320.6750.17259); Shanghai Wu Mengchao Medical Science Foundation (Grant No. JJHM‑2019009).
Author information
Authors and Affiliations
Contributions
GSB, HSX, and PPD conceived and designed the study. PPD, NW, and XJC collected the data. NW, FLC, and PPD contributed to the statistical analyses. PPD and NW wrote the manuscript. GSB, HSX, NW, and XJC critically revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical approval
The study was approved by the Ethics Committee of Shanghai Ninth People’s Hospital, School of Medicine, Shanghai Jiao Tong University. Patients or their relatives provided written, informed consent. The ID of the IRB was Ethical Review of the Shanghai Ninth Hospital 2018-89-T80.
Rights and permissions
About this article

Cite this article
Deng, PP., Wu, N., Chen, XJ. et al. NIHSS–the Alberta Stroke Program Early CT Score mismatch in guiding thrombolysis in patients with acute ischemic stroke. J Neurol 269, 1515–1521 (2022). https://doi.org/10.1007/s00415-021-10704-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10704-5