
Abstract
In this study, our objective was to identify the characteristic morphological features of brain MRI associated with a positive cerebrospinal fluid (CSF) tap test in patients with idiopathic normal pressure hydrocephalus (iNPH). Patients diagnosed with clinical suspected iNPH were evaluated. All patients underwent a mini-mental state examination, a brain MRI, and a CSF tap test. The severities of clinical symptoms were rated before and after the CSF tap test. Characteristic brain MRI findings including frontal convexity narrowing, parietal convexity narrowing, upward bowing of the corpus callosum, empty sella, narrowing of the CSF space at the high convexity, marked dilatation of the Sylvian fissure, and disproportion between narrowing of the CSF space at the high convexity and dilatation of the Sylvian fissure (“mismatch” sign) on T1-weighted or FLAIR image were analyzed. Forty-three patients (33 males/ten females, mean age 76.9 ± 6.9 years) with possible iNPH participated in this study. The presence versus absence of empty sella (52.4 vs. 14.3%, OR 6.6, 95% CI 1.5–29.4, p = 0.02) and “mismatch” sign (45.5 vs. 9.5%, OR 7.9, 95% CI 1.5–42.5, p = 0.02) were associated with positive CSF tap test responses. The sensitivity, specificity, positive predictive value, and negative predictive value of the presence of either of these two MRI features in the prediction of CSF tap response were 72.7, 81, 80, and 73.9%, respectively. Specific brain MRI features can be used as markers for the identification of potential CSF tap test responders in iNPH patients. These features may serve as supplemental evidence in the diagnosis of iNPH patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Normal pressure hydrocephalus (NPH) is a clinical syndrome that was first described in 1965 as presenting a triad of symptoms including dementia, gait disturbance, and urinary incontinence [1]. The causes of NPH can be idiopathic or can be secondary to traumatic brain injury, meningitis, subarachnoid hemorrhage (SAH) or intracranial surgery [2]. The exact pathologic process of idiopathic normal pressure hydrocephalus (iNPH) remains unclear. The underlying pathophysiological mechanism appears to include impaired cerebrospinal fluid (CSF) flow within the ventricles and/or subarachnoid space, defective CSF absorption through the arachnoid granulation, or impaired intracranial vascular compliance [3, 4].
Relkin et al. [5] proposed diagnostic criteria for the classification of patients into probable, possible, and unlikely iNPH, based solely on clinical symptoms in combination with interpretation of brain-imaging studies but not the response to shunt replacement. Nevertheless, they applied the term “shunt-responsive iNPH” to any diagnostic category, probable, possible, or unlikely, that responds favorably to surgical intervention [5–7]. In contrast, the Japanese guidelines for management of iNPH [8] suggested that definitive diagnosis of iNPH was based on a patient’s response to shunt surgery. The shunt-associated complications should be the first concern when treating iNPH patients. Recent literature of shunt-associated complications in iNPH was controversial [6, 9]. One review [9] suggested that there are no long-term detrimental effects, but the other meta-analysis [6] showed that the procedure was associated with a 38% complication rate, resulting in permanent neurological deficits, intracerebral hemorrhage, subdural hemorrhage, meningeal infection, and death.
Many supplemental diagnostic tools have been used to improve the diagnostic procedure in iNPH, including magnetic resonance imaging (MRI) of the brain [10–13], radionuclide cisternogram [14, 15], cine phase-contrast MRI for aqueductal CSF stroke volume [16–18], CSF tap test [19–21], external lumbar CSF drainage [22, 23], and lumbar infusion test [24–26].
The CSF tap test is a simple method that has been proven to have a high positive predictive value of successful shunt surgery [19, 23]. However, it should not be used as a test for exclusion from shunt surgery because of the relatively low sensitivity (26–62%) predicting a favorable surgical outcome [27]. While external lumbar CSF drainage has a higher sensitivity than the CSF tap test, its disadvantages include a prolonged hospital stay and a relatively higher complication rate [28].
Some specific morphological patterns of brain MRI, including enlarged basal cisterns and Sylvian fissures, narrowing of the CSF space at high convexity and high midline areas, and focally dilated sulci, have been useful in the diagnosis of iNPH [10, 11]. A recent review [29] summarized the structural imaging features in NPH with the conclusion that there was not enough evidence to support the diagnosis of NPH by specific MRI morphological patterns alone. In addition, previous studies on MRI findings in patients with iNPH have either had a small subject size or did not provide prospective data [10, 11].
The aim of the present study was to examine the correlation between the specific morphological patterns of brain MRI and CSF tap test responses in patients with possible iNPH. The results may be used as a supplemental aid in clinical diagnosis for patients with iNPH.
Methods
Patients
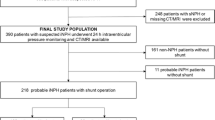
Patients (n = 48) with physical and cognitive symptoms and brain image findings (Brain CT or MRI) suggestive of iNPH were evaluated at Taipei Veterans General Hospital. Diagnosis of iNPH was based on the criteria proposed by Relkin et al. [5]. Patients must be older than 40 years of age with insidious progression of symptoms (gait disturbance plus at least one other area of impairment in cognition, urinary symptoms, or both) for at least 3–6 months and have normal CSF opening pressure. Brain scans (MRI or CT) of all participants showed widening of the ventricles (Evans ratio >0.3) and no macroscopic obstruction to CSF flow. The evidence for diagnostic value of other imaging results (e.g., cine phase-contrast MRI and radionuclide cisternogram) is weak [5, 17, 18, 27] and therefore, these supportive measures were not included as criteria.
Procedures
History taking and clinical severity rating
Age, gender, body mass index (BMI), past histories, personal histories, and initial and full-blown symptoms for all patients were recorded. Patients also underwent the mini-mental state examination (MMSE) [30] and a serum total cholesterol level check. A four-point subscale modified from Krauss et al. [31] was used to rate the severity of each fundamental symptom of iNPH (gait disturbance, cognitive impairment, and urinary incontinence) (Table 1) after an unstructured interview with patients and caregivers. All subjects underwent CSF tap test and brain MRI.
CSF tap test
The CSF tap test was performed by lumbar puncture (LP) followed by measurement of CSF opening pressure and finally CSF collection. We collected 40 cc of CSF or as much as possible until the patients could no longer tolerate the procedure. One day after the procedure we re-evaluated the severity of patients’ symptoms using the four-point scale and MMSE as mentioned above. The following criteria were used to identify responders: improvement on any one of the three fundamental symptoms using the four-point scale or a three-point or greater improvement on the follow-up MMSE results [22].
Brain MRI
Axial and sagittal spin-echo T1-weighted images were obtained by using a 1.5-T MRI unit (Signa Excite, General Electric, Milwaukee, WI, USA). We also obtained axial fast spin-echo T2-weighted and fluid-attenuated inversion recovery (FLAIR) images in order to exclude other illnesses. The following items were recorded according to visual analysis of brain MRIs: (1) frontal convexity narrowing on sagittal T1-weighted images, (2) parietal convexity narrowing on sagittal T1-weighted images, (3) upward bowing of the corpus callosum on sagittal T1-weighted images (Fig. 1), (4) empty sella on sagittal T1-weighted images (Fig. 2), (5) narrowing of the CSF space at the high convexity (according to the upper two axial sections) on axial T1-weighted or FLAIR images [10, 11], (6) marked dilatation of the Sylvian fissure on axial T1-weighted or FLAIR images, and (7) disproportion between narrowing of the CSF space at the high convexity and dilatation of the Sylvian fissure (“mismatch” sign) on axial T1-weighted or FLAIR image (Fig. 3). Visual analyses were conducted independently by two neuroradiologists who were experienced in MRI correlates of NPH patients and who were blind to both diagnosis and CSF tap test results of subjects. The inter-rater reliability was high (Kappa values range from 0.732 to 0.836). All borderline findings during the visual analyses were considered negative.

a–c A paramedian-sagittal T1-weighted brain MRI obtained from a CSF tap test responder showing frontal convexity tightness, parietal convexity tightness (arrowheads), and upward bowing of the corpus callosum (arrows). d–f A paramedian-sagittal T1-weighted brain MRI obtained from a CSF tap test non-responder without frontal convexity tightness, parietal convexity tightness (arrowheads), and upward bowing of the corpus callosum (arrows)

a, b A paramedian-sagittal T1-weighted brain MRI obtained from a CSF tap test responder showing an enlarged and empty sella (arrows). c, d A paramedian-sagittal T1-weighted brain MRI obtained from a CSF tap test non-responder showing no abnormality of sella turcica (arrows)

a, b An axial T1-weighted brain MRI obtained from a CSF tap test responder, showing disproportion between narrowing of the CSF spaces at the high convexity and dilatation of the Sylvian fissures (narrowing of the high convexity CSF spaces (arrows) with relative dilated Sylvian fissures). c, d An axial T1-weighted brain MRI obtained from a CSF tap test non-responder showing no narrowing of the high convexity CSF spaces (arrows) and non-dilated Sylvian fissures
Statistics
All statistical analyses were performed on the statistical software package SPSS for Windows (version 13.0.; SPSS Inc., Chicago, IL, USA). The patients were divided into two groups: CSF tap test responders and non-responders. The clinical profile and MRI characteristic features were compared between these two groups. Chi-square and t test were used when appropriate. The predictors of MRI features were presented as odds ratios (ORs) with 95% confidence intervals (CIs). The sensitivity and specificity along with the positive and negative predictive value of MRI characteristic features were assessed. The statistical significance level was set at p < 0.05.
Results
Of the 48 patients with NPH evaluated for this study, three were excluded because of known secondary causes (SAH, n = 2 and meningitis, n = 1), one because of pacemaker interference with MRI examination, and one due to the absence of a reliable caregiver to provide history. The remaining 43 patients (33 males and ten females, mean age 76.9 ± 6.9 years, range 52–89) constituted the final sample for analysis. All patients had gait disturbance, 97.7% (42/43) had cognitive impairments, and 55.8% (24/43) had urinary incontinence. The mean initial MMSE score was 18.3 ± 6.7. The mean duration of symptoms was 26.6 ± 25.1 months (range 3–96). The mean score on the four-point scale was 1.4 ± 0.6 for gait, 1.4 ± 0.7 for cognition, and 1.0 ± 1.0 for urinary control. The mean total score was 3.7 ± 1.9.
According to the results of the CSF tap test, 22 of the 43 patients (51.2%) were classified as responders while the rest (n = 21, 48.8%) were non-responders. The mean drainage volume of CSF during the tap test was 25.5 ml in the tap test responder group and 22.4 ml in the tap test non-responder group. Among the 22 CSF tap test responders, 19 patients showed gait improvement (86.4%), seven patients showed cognitive improvement (31.8%), two patients showed improvement of urinary incontinence (9.1%), five patients showed both gait and mental improvement (22.7%), and no patients showed improvement of all three clinical symptoms. The personal histories, past histories, initial symptoms, full-blown symptoms, duration of the symptoms, the four-point subscale scores, initial MMSE scores, and the volumes of CSF drainage did not differ between the responders and non-responders (Table 2).
The results of visual analysis of brain MRI are summarized in Table 3. One sagittal brain MRI exam was excluded due to marked motion artifacts. The CSF tap test responders were associated with the presence of empty sella (52.4 vs. 14.3%, responders vs. non-responders, respectively; OR = 6.6, 95% CI = 1.48–29.36, p = 0.02) and the “mismatch” sign (45.5 vs. 9.5%, responders vs. non-responders, respectively; OR = 7.9, 95% CI = 1.47–42.54, p = 0.02). The sensitivity, specificity, positive predictive value, and negative predictive value of empty sella were 52.4, 85.7, 78.6, and 64.3%, respectively, and for “mismatch” sign were 45.4, 90.5, 83.3, and 61.3%, respectively. The presence of either empty sella or “mismatch” sign was the best predictor for the CSF tap test response (72.7 vs. 19.0%, responders vs. non-responders, respectively; OR = 11.3, 95% CI = 2.69–47.72, p = 0.001). The sensitivity, specificity, positive predictive value, and negative predictive value for showing one of these features were 72.7, 81, 80, and 73.9%, respectively.
Discussion
Using the routinely performed axial and sagittal spin-echo MRI to evaluate patients with iNPH, we found that empty sella and disproportion between narrowing of the CSF space at the high convexity and dilatation of the Sylvian fissure (“mismatch” sign) were correlated with CSF tap test response or non-response. The specificity and positive predictive value of each MRI feature were high while the sensitivity was relatively low.
The disproportion between narrowing of the CSF space at the high convexity and dilatation of the Sylvian fissure was highly correlated with the CSF tap test response. In line with previous studies [10, 11], these features may be useful in making the diagnosis of iNPH. However, isolated narrowing of the high convexity CSF space or marked dilation of the Sylvian fissure alone did not correlate with the CSF tap test response. One hypothesis suggested that patients with iNPH presenting defective CSF absorption due to “supraSylvian subarachnoid block” [11] have high CSF pressure in the ventricles/Sylvian fissures and low pressure in the supraSylvian subarachnoid space resulting in both of these MRI findings [10]. This hypothesis was supported by the diminished size of the Sylvian fissure and ventricular system together after shunt surgery [11]. When only one sign develops, it may signify that dilation of the Sylvian fissure is secondary to brain atrophy or no pressure gradient between the ventricles/Sylvian fissures and supraSylvian subarachnoid spaces. When the pressure gradient is present, the high CSF pressure in the ventricles/Sylvian fissures compresses brain tissue and influences vascular compliance [3]. A positive response to the CSF tap test can be predicted when the pressure gradient is present because the CSF tap test releases the pressure. However, our results showed that not all CSF responders demonstrated “mismatch” signs. The absence of “mismatch” signs in responders may be explained by different sites of CSF stagnation in addition to the supraSylvian region, or may be due to defective CSF absorption at the arachnoid villi without CSF circulation block.
The association between empty sella and idiopathic intracranial hypertension is well known, and the validity of the detection of empty sella based on the sagittal T1 images has also been demonstrated [32]. The relationship between empty sella and iNPH was rarely mentioned [33, 34]. According to Bradley’s hypothesis [35], increased compression of brain tissue may result in the pathogenesis of iNPH. Other reports [4, 36, 37] described periods of increased intraventricular pressure in the pathological course of iNPH. The extension of the subarachnoid space of the sella turcica may result from mildly or intermittently increased intraventricular pressure. The sensitivity of determining CSF tap test responders was increased with either the presence of an empty sella or “mismatch” sign. These results may indicate other causes of iNPH besides supraSylvian subarachnoid blockage [10, 11].
The current management of iNPH patients is based on clinical symptoms and the results of supplemental prognostic tests, including brain imaging studies or CSF drainage tests [27]. According to the Japanese guidelines for the management of iNPH [8], symptomatic improvement after the CSF tap test or external lumbar drainage is essential to the decision of whether shunt surgery should be performed. A prior study [27] recommended one or more of the following three tests as supplemental prognostic tools in the treatment of iNPH: CSF tap test, outflow resistance determination, and/or external lumbar drainage. However, the selection of supplemental tests may be based on personal experience, favorable prognostic value, and equipment/personnel availability. The results of our study suggest that if brain MRI of a suspected iNPH patient shows “mismatch” sign or an empty sella, we can predict a high probability of positive response of the CSF tap test. Our brain MRI findings, therefore, may provide supplemental information in the diagnosis of iNPH patients.
Other MRI findings in our patients with possible iNPH did not show significant associations with response to the CSF tap test. A previous study found a high correlation between a narrowing of the posterior aspect of the cingulate sulcus (similar to our MRI features including frontal convexity narrowing, parietal convexity narrowing, and upward bowing of the corpus callosum) and iNPH in a small-size population [38]. However, our study did not replicate this finding.
We reduced the potential bias of clinical evaluation before and after CSF tap tests by using an objective grading scale and MMSE in place of subjective statements by patients or caregivers. Although there is no consensus about the extent of improvement in MMSE score after CSF tap test to represent clinical improvement of NPH symptoms, most of our CSF tap test responders showed gait improvement. Therefore, the possibility of misclassification (responder vs. non-responder) resulting from improvement in MMSE score alone was low [19]. Further, the mean drainage volume of CSF during the tap test in our study was 25.5 ml in the tap test responder group and 22.4 ml in the tap test non-responder group. The volume in both groups was less than optimal (30–50 ml) [8, 39]. We therefore, cannot exclude the possibility that some patients in the non-responder group might have become responders if more CSF was drained.
In conclusion, an empty sella and disproportion between narrowing of the CSF space at the high convexity and dilatation of the Sylvian fissure (“mismatch” sign) on brain MRI are important imaging findings for iNPH. These findings could help to identify the potential CSF tap test responder and may serve as additional support in diagnosis in iNPH. Further studies on the predictive value of these MRI findings on response to shunt surgery are warranted in the future.
References
Adams RD, Fisher CM, Hakim S et al (1965) Symptomatic occult hydrocephalus with “normal” cerebrospinal-fluid pressure. A treatable syndrome. N Engl J Med 273:117–126
Sheehan JP, Polin RS, Sheehan JM et al (1999) Factors associated with hydrocephalus after aneurysmal subarachnoid hemorrhage. Neurosurgery 45:1120–1127
Bateman GA (2000) Vascular compliance in normal pressure hydrocephalus. Am J Neuroradiol 21:1574–1585
Vanneste JA (1994) Three decades of normal pressure hydrocephalus: are we wiser now? J Neurol Neurosurg Psychiatry 57:1021–1025
Relkin N, Marmarou A, Klinge P et al (2005) Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 57(Suppl 3):S4–S16
Hebb AO, Cusimano MD (2001) Idiopathic normal pressure hydrocephalus: a systematic review of diagnosis and outcome. Neurosurgery 49:1166–1184
Kahlon B, Sjunnesson J, Rehncrona S (2007) Long-term outcome in patients with suspected normal pressure hydrocephalus. Neurosurgery 60:327–332
Ishikawa M, Hashimoto M, Kuwana N et al (2008) Guidelines for management of idiopathic normal pressure hydrocephalus. Neurol Med Chir (Tokyo) 48(Suppl):S1–S23
Klinge P, Marmarou A, Bergsneider M et al (2005) Outcome of shunting in idiopathic normal-pressure hydrocephalus and the value of outcome assessment in shunted patients. Neurosurgery 57(Suppl 3):S40–S52
Sasaki M, Honda S, Yuasa T et al (2008) Narrow CSF space at high convexity and high midline areas in idiopathic normal pressure hydrocephalus detected by axial and coronal MRI. Neuroradiology 50:117–122
Kitagaki H, Mori E, Ishii K et al (1998) CSF spaces in idiopathic normal pressure hydrocephalus: morphology and volumetry. Am J Neuroradiol 19:1277–1284
Ishii K, Kawaguchi T, Shimada K et al (2008) Voxel-based analysis of gray matter and CSF space in idiopathic normal pressure hydrocephalus. Dement Geriatr Cogn Disord 25:329–335
Ishii K, Kanda T, Harada A et al (2008) Clinical impact of the callosal angle in the diagnosis of idiopathic normal pressure hydrocephalus. Eur Radiol 18:2678–2683
Vanneste J, Augustijn P, Davies GA et al (1992) Normal-pressure hydrocephalus. Is cisternography still useful in selecting patients for a shunt? Arch Neurol 494:366–370
Larsson A, Moonen M, Bergh AC et al (1990) Predictive value of quantitative cisternography in normal pressure hydrocephalus. Acta Neurol Scand 814:327–332
Al-Zain FT, Rademacher G, Meier U et al (2008) The role of cerebrospinal fluid flow study using phase contrast MR imaging in diagnosing idiopathic normal pressure hydrocephalus. Acta Neurochir 102(Suppl):119–123
Kahlon B, Annertz M, Stahlberg F et al (2007) Is aqueductal stroke volume, measured with cine phase-contrast magnetic resonance imaging scans useful in predicting outcome of shunt surgery in suspected normal pressure hydrocephalus? Neurosurgery 60:124–129
Dixon GR, Friedman JA, Luetmer PH et al (2002) Use of cerebrospinal fluid flow rates measured by phase-contrast MR to predict outcome of ventriculoperitoneal shunting for idiopathic normal-pressure hydrocephalus. Mayo Clin Proc 776:509–514
Kahlon B, Sundbarg G, Rehncrona S (2002) Comparison between the lumbar infusion and CSF tap tests to predict outcome after shunt surgery in suspected normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 736:721–726
Damasceno BP, Carelli EF, Honorato DC et al (1997) The predictive value of cerebrospinal fluid tap-test in normal pressure hydrocephalus. Arq Neuropsiquiatr 552:179–185
Wikkelso C, Andersson H, Blomstrand C et al (1986) Normal pressure hydrocephalus. Predictive value of the cerebrospinal fluid tap-test. Acta Neurol Scand 73:566–573
Woodworth GF, McGirt MJ, Williams MA et al (2009) Cerebrospinal fluid drainage and dynamics in the diagnosis of normal pressure hydrocephalus. Neurosurgery 64:919–925
Walchenbach R, Geiger E, Thomeer RT et al (2002) The value of temporary external lumbar CSF drainage in predicting the outcome of shunting on normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 72:503–506
Kahlon B, Sundbarg G, Rehncrona S (2005) Lumbar infusion test in normal pressure hydrocephalus. Acta Neurol Scand 111:379–384
Ekstedt J (1977) CSF hydrodynamic studies in man. 1. Method of constant pressure CSF infusion. J Neurol Neurosurg Psychiatry 40:105–119
Ekstedt J (1978) CSF hydrodynamic studies in man. 2. Normal hydrodynamic variables related to CSF pressure and flow. J Neurol Neurosurg Psychiatry 41:345–353
Marmarou A, Bergsneider M, Klinge P et al (2005) The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery 57(Suppl 3):S17–S28
Governale LS, Fein N, Logsdon J et al (2008) Technique and complications of external lumbar drainage for normal pressure hydrocephalus. Neurosurgery 63(Suppl 2):379–384
Tarnaris A, Kitchen ND, Watkins LD (2009) Noninvasive biomarkers in normal pressure hydrocephalus: evidence for the role of neuroimaging. J Neurosurg 110:837–851
Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Krauss JK, Droste DW, Vach W et al (1996) Cerebrospinal fluid shunting in idiopathic normal-pressure hydrocephalus of the elderly: effect of periventricular and deep white matter lesions. Neurosurgery 39:292–299
Agid R, Farb RI, Willinsky RA et al (2006) Idiopathic intracranial hypertension: the validity of cross-sectional neuroimaging signs. Neuroradiology 48:521–527
Spagna VA, Maeder MC, Johnson JC et al (1978) Normal pressure hydrocephalus, parkinsonism, and primary empty sella-coincidence or cause-effect? Neurology 28:1191–1193
Casmiro M (1998) Idiopathic normal pressure hydrocephalus associated with empty sella. Neurosurg Rev 21:43–47
Bradley WG Jr, Whittemore AR, Kortman KE et al (1991) Marked cerebrospinal fluid void: indicator of successful shunt in patients with suspected normal-pressure hydrocephalus. Radiology 178:459–466
Crockard HA, Hanlon K, Duda EE et al (1977) Hydrocephalus as a cause of dementia: evaluation of computerized tomography and intracranial pressure motoring. J Neurol Neurosurg Psychiatry 40:736–740
Conner ES, Black PMcL, Goley L (1984) Experimental normal pressure hydrocephalus is accompanied by increased transmantle pressure. J Neurosurg 61:322–328
Adachi M, Kawanami T, Ohshima F et al (2006) Upper midbrain profile sign and cingulate sulcus sign: MRI findings on sagittal images in idiopathic normal-pressure hydrocephalus, Alzheimer’s disease, and progressive supranuclear palsy. Radiat Med 24:568–572
Shprecher D, Schwalb J, Kurlan R (2008) Normal pressure hydrocephalus: diagnosis and treatment. Curr Neurol Neurosci Rep 8:371–376
Acknowledgments
This study was supported in part by grants from the National Science Council of Taiwan (97-2314-B-075-049-MY3), Taipei Veterans General Hospital (V97C1-049 and V99C1-047) and the Ministry of Education (Aim for the Top University Plan), Taipei, Taiwan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, WJ., Wang, SJ., Hsu, LC. et al. Brain MRI as a predictor of CSF tap test response in patients with idiopathic normal pressure hydrocephalus. J Neurol 257, 1675–1681 (2010). https://doi.org/10.1007/s00415-010-5602-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-010-5602-8