
Abstract
The aim of this study was to examine the feasibility of stature estimation by measuring the pelvic bones of Japanese cadavers using three-dimensional (3D) computed tomography (CT). We assessed 3D reconstructed images of 210 Japanese subjects (108 males, 102 females) who had undergone postmortem CT between May 2011 and November 2013. We defined the linear distance from the anterosuperior margin of the left and right anterior superior iliac spines (ASIS) to the posterior margin of the left and right ischial spines as the LSS and RSS, respectively. We also defined the linear distance from the anterosuperior margin of the left and right ASIS to the anteroinferior margin of the left and right ischial tuberosities as the LST and RST, respectively. The correlation between the cadaver stature (CS) and each parameter (LSS, LST, RSS, and RST) was evaluated using Pearson product–moment correlation coefficients and regression analysis was performed for stature estimation. All four parameters correlated significantly with stature independent of sex, suggesting that they can be used as a tool for stature estimation. The LST had the closest correlation with stature in both sexes.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
One of the goals of forensic analysis is the identification of skeletonized or decomposed human remains. Together with sex, age, and ancestry, stature is a biological parameter that characterizes individuals and can be evaluated from the skeleton even when many years have passed after death [1–4]. These parameters expedite the analysis of remains to narrow down the pool of cadavers needing to be matched and allow for more definitive markers, such as DNA, to be used for the confirmation of final identification [5].
There are two methods to estimate stature from human remains. One is the anatomical method, which requires a whole skeleton to calculate the combination of several bone lengths [6]. Although this method is held to be the most accurate method for stature estimation, it is often unavailable because a complete and well-preserved skeleton is very uncommon after serious events such as natural disasters, plane crashes, and terrorist attacks. The other is the mathematical method, which employs sex- and population-specific regression formula derived from correlations between stature and the measurements of some skeletal elements. Many previous studies used extremity measurements for stature estimation because comparatively accurate estimates can be produced from long bone regression equations [6–9]. However, if corpses are on the ground surface, the extremities are often unavailable, having been chewed and removed from the cadaver by animals [10]. In addition, intact long bones may not be available in some mass disaster, burn, and skeletal cases [11]. Thus, there is still a need to assess the correlation of bones other than long bones with stature.
Several studies have examined the relationship between stature and skeletal elements, such as the size of the cranium [12], scapula [13], sternum [14–16], vertebrae [17–20], and sacrum [10, 11, 21, 22]. However, despite the fact that the pelvis has been used all over the world for the determination of sex [23] and age estimation [24–31], few studies have investigated the correlation between measurements of the pelvic bones and stature. Although Giroux and Wescott [11] examined the utility of pelvic bone measurements for stature estimation in dry bones of American Black and White males and females, our search of the literature revealed that the correlation between stature and pelvic measurements using three-dimensional (3D) multidetector computed tomographic (MDCT) images in a Japanese population has not been investigated. We previously reported that the length of the sacrum and coccyx using MDCT can predict stature with precision [21]. In addition, the coxa and femoral head are often preserved in skeletonized, mutilated, and burned human remains that have an intact sacrum, and measurements of these bones are commonly collected by anthropologists [32]. Thus, we hypothesized that pelvic measurements using MDCT images may also be useful in stature estimation.
Recently, postmortem computed tomography (PMCT) has been routinely performed using MDCT in forensic departments and institutes equipped with computed tomography (CT) [33]. 3D images of the pelvis can be easily generated from MDCT data. In particular, forensic investigators can assess and evaluate bones on CT images without the removal of surrounding tissues when a subject of measurement is not a skeletonized bone sample. Therefore, if CT for the evaluation of pelvic bones is available, it may result in the reduction of the time and cost of forensic investigations.
The aim of this retrospective study was to examine the feasibility of stature estimation based on measurements of the pelvic bones of Japanese cadavers using 3D CT images.
Materials and methods
The experimental protocol was approved by the ethics committee of our university and did not require approval of the subjects’ next of kin.
The present study reviewed the data of 210 cadavers (108 males and 102 females) of known age and sex who had undergone PMCT with subsequent forensic autopsy at the department of legal medicine at our university between May 2011 and November 2013. Cases were excluded if the history highlighted conditions or events that could have affected the pelvis; cases of pelvic fracture, burning, buttock injuries, and acquired or congenital abnormalities were excluded from this study.
During autopsy, the cadaver was laid on its back in full extension and a measuring tape was used against the board to measure the cadaver stature (CS) as the maximum length between the skull vertex and the heel in millimeters after the rigor mortis of the cadaver was fully resolved. To determine the intraobserver and interobserver errors of the measurements, stature was remeasured by both the original researcher and another pathologist not participating in the study.
PMCT was performed with a 16-row detector CT system (ECLOS; Hitachi Medical Corporation, Tokyo, Japan). The scanning protocol was as follows: collimation of 1.25 mm, reconstruction interval of 1.25 mm, tube voltage of 120 kVp, tube current of 200 mAs, and rotation time of 1 per second. A hard filter was used. Image data were processed on a workstation (SYNAPSE VINCENT; Fujifilm Medical, Tokyo, Japan) to obtain orthogonal multiplanar reconstruction images and volume-rendered images.
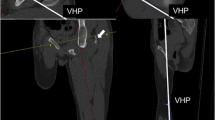
A 3D reconstructed image was used for assessment. The linear distances from the anterosuperior margin of the left and right anterior superior iliac spines (ASIS) to the posterior margin of the left and right ischial spines were defined as the LSS and RSS, respectively (Figs. 1a, c). The linear distances from the anterosuperior margin of the left and right ASIS to the anteroinferior margin of the left and right ischial tuberosities were defined as the LST and RST, respectively (Figs. 1b, c). These measurements were performed using electronic cursors and were recorded to the nearest 0.1 mm. Repeat measurements of 20 images selected randomly from the subjects were performed by both the original and another researcher to evaluate intraobserver and interobserver errors.

CT scan imaging with volume rendering reconstruction; a linear distances from the anterosuperior margin of the left and right anterior superior iliac spines to the posterior margin of the left and right ischial spines (LSS and RSS) in the coronal plane viewed from posterior side of the body; b linear distances from the anterosuperior margin of the left and right anterior superior iliac spines to the anteroinferior margin of the left and right ischial tuberosities (LST and RST) in the coronal plane viewed from anterior side of the body; c LSS and LST in the sagittal plane viewed from left side of the body
Statistical analyses were performed on a personal computer using Statistical Package for the Social Sciences (SPSS) version 21.0 computer software (IBM Corp., Armonk, NY) and Excel software (Microsoft 2010). The mean, standard deviation, and the range of the four parameters (LSS, LST, RSS, and RST) were calculated for all subjects as well as for the male and female subjects separately. To evaluate intraobserver and interobserver errors, the technical error of measurement (TEM), the relative technical error of measurement (rTEM), and the coefficient of reliability (R) were calculated. The acceptance ranges of rTEM (%) using beginner anthropometrist levels for intraobserver error was less than 1.5 % and for interobserver error, less than 2.0 % [34]. R values more than 0.95 were considered as sufficiently precise [35]. The correlation between the CS and each parameter (LSS, LST, RSS, and RST) was evaluated using Pearson product–moment correlation coefficients (r). P values less than 0.05 were considered statistically significant. Simple linear regression analysis was performed for the four parameters to derive regression formula for stature estimation. Multiple regression analysis for stature estimation was also performed using the multiple parameters to determine the most accurate formula. The coefficient of determination (r 2) and the standard error of estimation (SEE) were calculated to assess the significance of regression.
Results
Descriptive statistics of age, stature, and the four parameters are presented in Table 1. The calculated TEM, rTEM, and R are tabulated in Table 2. All the rTEMs for intraobserver error (0.261–0.497 %) were less than 1.5 % and for interobserver error (0.283–0.543 %) less than 2 %. All the R values (0.952–0.993) were more than 0.95.
Table 3 illustrates the correlation coefficients between stature and each parameter among all subjects, among male cadavers, and among female cadavers, respectively. All measurements presented statistically significant correlation with stature (P < 0.001) (Fig. 2). The correlation coefficients for measurements with comparatively large values (LST and RST) were greater than those with small values (LSS and RSS). The highest correlation coefficient was found for LST (all subjects, r = 0.922; male subjects, r = 0.881; female subjects, r = 0.770), and the lowest correlation coefficient for RSS (all subjects, r = 0.873; male subjects, r = 0.758; female subjects, r = 0.705). The correlation coefficients of each of the four parameters were higher among male subjects than among female subjects.

Scatter plots comparing a LSS and cadaver stature (CS), b LST and CS, c RSS and CS, and d LST and CS. Closed circles represent male subjects and open circles represent female subjects
Table 4 shows the simple linear regression equations, the SEEs, and the coefficients of determination derived for stature estimation in all subjects, male subjects, and female subjects from each of the four parameters. The SEEs were in the range of 4.40–5.56 cm for all subjects, 3.72–5.14 cm for male subjects, and 5.02–5.57 cm for female subjects, respectively. The SEEs calculated from the simple linear regression equations for male subjects were lower than those for female subjects.
Table 5 shows the multiple regression equations formulated using multiple variables. The SEEs calculated from multiple regression equations were lower (4.34–4.56 cm for all subjects; 3.69–3.89 cm for male subjects; 4.93–5.15 cm for female subjects) than those calculated from simple linear regression equations.
Discussion
The main findings of this study were the significantly positive correlations between stature and the four parameters independent of sex, indicating that measurements of the pelvic bones on 3D CT images may be a reliable predictor of stature in Japanese cadavers. In particular, the LST is the best single-element estimator in both sexes. Studies on the correlations between stature and the pelvic bones are summarized in Table 6. Compared with previous studies, the correlation coefficients in this study were the largest and the SEEs were the smallest. Giroux and Wescott [11] reported that hip height exhibited stronger correlation with stature than sacral height. The present study also demonstrated similar results in comparison to our previous study [21]. Giroux and Wescott [11] reported that interobserver error and differences are the most serious problems in the measurements of cadaver stature. In our study, the TEM, rTEM, and R values were calculated and the intraobserver and interobserver errors for measurements of stature and pelvic bones were found to be very small. Taken together, these findings suggest that measurements of the pelvic bones, especially the ilium and ischium, may be appropriate and reliable for stature estimation if CT scanning with 3D reconstruction is available.
Note that Sakuma et al. [36] performed the measurements of the skull with calipers, and then also performed the measurements of the 3D CT reconstructed images in our department, revealing that there was no significant difference between the actual measurements and the measurements on the 3D CT images. Thus, the measurements of the pelvic bones on the 3D CT images are also considered similar to real measurements on dry bones performed with calipers.
To date, few researchers have applied CT scanning to the field of anthropometry. Giurazza et al. [37] evaluated the correlation between stature and the measurements of femur and skull through CT scans and derived regression equations for stature estimation in the Caucasian population, concluding that a CT scan is a valuable technique to measure bone length. Giurazza et al. [38] assessed the correlation between scapula size and stature by CT scan evaluation and reported that CT is one of the most accurate radiographic techniques for the study of bone morphometry. We previously evaluated the relationship between stature and the length of the sacrum and coccyx using MDCT and derived regression equations for stature estimation in the modern Japanese population, and the calculated SEEs were lower than those calculated from the real measurements of dry bones, probably because of the difficulty in measuring dry bones with precision [21]. In addition, MDCT enables forensic investigators to perform measurements on bone images instead of fresh bones that require preparations such as removing and cleansing the skeleton if surrounding tissues remain [21]. Moreover, digital CT images can be preserved almost permanently in little or no physical space, enabling repeated measurements and potentially decreasing intraobserver and interobserver error [10].
In this study, the multiple regression equations provided better estimates (lower SEEs and higher r 2) than the simple linear regression equations in all cases. In accordance with the previous studies using pelvic bones, these results suggest that the multiple regression equations for the estimation of stature are more reliable than the single linear regression equations [11, 22, 39]. Hasegawa et al. [40] estimated stature from the long bones of the limbs of Japanese living subjects and showed lower SEEs using the lower limbs (2.63–3.03 cm) than those in our study (3.64–4.88 cm). However, the SEEs calculated using the humerus were in the range of 3.75–4.45 cm, which were similar to those in our study, again suggesting that measuring the size of the pelvic bones with 3D CT may be a useful tool for stature estimation in bodies with no lower limbs.
In this study, we did not apply any correction to the recorded cadaver stature measurements. It is well known that cadaver stature is different from living stature because of the physiologic changes that occur in the human body after death [37]. Therefore, the possibility cannot be excluded that the formula derived in this study may not be expected to accurately estimate stature. In addition, standing living stature may also not be used in identification. Willey and Falsetti [41] reported that forensic stature, which is the stature recorded on driver’s licenses, medical records, and other documents, is often greater than the stature directly measured from a corpse. However, in some cases, measured stature is greater than the stature on the driver’s license probably because the individual failed to update the driver’s license information after growth [41, 42]. Thus, if the information about stature that is used in the identification process is derived from personal documents, it tends to further confound stature estimation.
In conclusion, our measurements of the pelvic bones performed on 3D CT images significantly correlated with stature in all cases, indicating that they may be a reliable stature predictor in the Japanese population and can be used as a tool for stature estimation, especially for corpse identification, when long bones are unavailable or not intact. However, owing to the physiologic changes that occur in the human body after death, the possibility cannot be excluded that the formula developed in this study may not be used to accurately estimate stature. In particular, the LST had the best correlation with stature among Japanese cadavers regardless of sex. Similar studies in other age groups and in different populations are warranted.
References
Krishan K, Sharma A (2007) Estimation of stature from dimensions of hands and feet in a North Indian population. J Forensic Legal Med 14:327–332
Cunha E, Cattaneo C (2006) Forensic pathology and forensic anthropology: the state of art. In: Schmitt A, Cunha E, Pinheiro J (eds) Forensic anthropology and medicine. Humana Press, New Jersey, pp 39–53
Scheuer L (2002) Application of osteology to forensic medicine. Clin Anat 15:297–312
Cordeiro C, Muñoz-Barús JI (2009) Predicting adult stature from metatarsal length in a Portuguese population. Forensic Sci Int 193:131.e1–131.e4
Ahmed AA (2013) Estimation of stature from the upper limb measurements of Sudanese adults. Forensic Sci Int 228:178.e1–178.e7
Raxter MH, Auerbach BM, Ruff CB (2006) Revision of the fully technique for estimating statures. Am J Phys Anthropol 130:374–384
Krishan K, Kanchan T, Asha N (2012) Estimation of stature from index and ring finger length in a North Indian adolescent population. J Forensic Legal Med 19:285–290
Bidmos MA (2008) Stature reconstruction using fragmentary femora in South Africans of European descent. J Forensic Sci 53:1044–1048
Hauser R, Smoliński J, Gos T (2005) The estimation of stature on the basis of measurements of the femur. Forensic Sci Int 147:185–190
Karakas HM, Celbis O, Harma A et al (2011) Total body height estimation using sacrum height in Anatolian Caucasians: multidetector computed tomography-based virtual anthropometry. Skelet Radiol 40:623–630
Giroux CL, Wescott DJ (2008) Stature estimation based on dimensions of the bony pelvis and proximal femur. J Forensic Sci 53:65–68
Krishan K, Kumar R (2007) Determination of stature from cephalo-facial dimensions in a North Indian population. J Legal Med 9:128–133
Burke RM (2005) Can we estimate stature from the scapula? A test considering sex and ancestry. Thesis, BSc, University of Idaho
Singh J, Pathak RK, Chavali KH (2011) Skeletal height estimation from regression analysis of sternal lengths in a Northwest Indian population of Chandigarh region: a postmortem study. Forensic Sci Int 206:211.e1–211.e8
Marinho L, Almeida D, Santos A et al. (2012) Is the length of the sternum reliable for estimating adult stature? A pilot study using fresh sterna and a test of two methods using dry sterna. Forensic Sci Int 220:292.e1–292.e4
Menezes RG, Nagesh KR, Monteiro FN et al (2011) Estimation of stature from the length of the sternum in South Indian females. J Forensic Legal Med 18:242–245
Tibbets GL (1981) Estimation of stature from the vertebral column in American Blacks. J Forensic Sci 26:715–723
Terazawa K, Takatori T, Mizukami K et al (1985) Estimation of stature from somatometry of vertebral column in Japanese. Nihon Hoigaku Zasshi 30:35–40
Terazawa K, Akabane H, Gotouda H et al (1990) Estimating stature from the length of the lumbar part of the spine in Japanese. Med Sci Law 30:354–357
Jason DR, Taylor K (1995) Estimation of stature from the length of cervical, thoracic and lumbar segments of spine in American whites and blacks. J Forensic Sci 40:59–62
Torimitsu S, Makino Y, Saitoh H et al (2014) Stature estimation in Japanese cadavers using the sacral and coccygeal length measured with multidetector computed tomography. Legal Med (Tokyo) 16:14–19
Pelin C, Duyar I, Kayahan EM et al (2005) Body height estimation based on dimensions of sacral and coccygeal vertebrae. J Forensic Sci 50:294–297
Steyn M, Işcan MY (2008) Metric sex determination from the pelvis in modern Greeks. Forensic Sci Int 179:86.e1–86.e6
Villa C, Hansena MN, Buckberry J et al (2013) Forensic age estimation based on the trabecular bone changes of the pelvic bone using post-mortem CT. Forensic Sci Int 233:393–402
Brooks S, Suchey J (1990) Skeletal age determination based on the Os Pubis: a comparison of the Acsadi-Nemeskeri and Suchey-Brooks methods. J Hum Evol 1990
Buckberry JL, Chamberlain AT (2002) Age estimation from the auricular surface of the ilium: a revised method. Am J Phys Anthropol 119:231–239
Todd TW (1930) Age changes in the pubic bone. VIII. Roentgenographic differentiation. Am J Phys Anthropol 14:255–271
Schmidt S, Schmeling A, Zwiesigk P et al (2011) Sonographic evaluation of apophyseal ossification of the iliac crest in forensic age diagnostics in living individuals. Int J Legal Med 125:271–276
Wittschieber D, Vieth V, Domnick C et al (2013) The iliac crest in forensic age diagnostics: evaluation of the apophyseal ossification in conventional radiography. Int J Legal Med 127:473–479
Wittschieber D, Vieth V, Wierer T et al (2013) Cameriere’s approach modified for pelvic radiographs: a novel method to assess apophyseal iliac crest ossification for the purpose of forensic age diagnostics. Int J Legal Med 127:825–829
López-Alcaraz M, Garamendi González PM, Alemán Aguilera I et al (2013) Image analysis of pubic bone for sex determination in a computed tomography sample. Int J Legal Med 127:1145–1155
Moore-Jansen PH, Ousley SD, Jantz RL (1994) Data collection procedures for forensic skeletal material. Department of Anthropology, University of Tennessee, Knoxville
Chiba F, Makino Y, Motomura A et al (2013) Age estimation by multidetector CT images of the sagittal suture. Int J Legal Med 127:1005–1011
Jamaiyah H, Geeta A, Safiza MN et al (2010) Reliability, technical error of measurements and validity of length and weight measurements for children under two years old in Malaysia. Med J Malays 65:131–137
Arroyo M, Freire M, Ansotegui L et al (2010) Intraobserver error associated with anthropometric measurements made by dietitians. Nutr Hosp 25:1053–1056
Sakuma A, Ishii M, Yamamoto S et al (2010) Application of postmortem 3D-CT facial reconstruction for personal identification. J Forensic Sci 55:1624–1629
Giurazza F, Del Vescovo R, Schena E et al. (2012) Determination of stature from skeletal and skull measurements by CT scan evaluation. Forensic Sci Int 222:398.e1–398.e9
Giurazza F, Del Vescovo R, Schena E et al (2013) Stature estimation from scapular measurements by CT scan evaluation in an Italian population. Legal Med (Tokyo) 15:202–208
Pininski M, Brits D (2014) Estimating stature in South African populations using various measures of the sacrum. Forensic Sci Int 234:182.e1–182.e7
Hasegawa I, Uenishi K, Fukunaga T et al (2009) Stature estimation formulae from radiographically determined limb bone length in a modern Japanese population. Legal Med (Tokyo) 11:260–266
Willey P, Falsetti T (1991) Inaccuracy of height information on driver's licenses. J Forensic Sci 36:813–819
Ousley SD (1995) Should we estimate biological or forensic stature? J Forensic Sci 40:768–773
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical standards
This study complies with the current laws of the country in which it was performed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Torimitsu, S., Makino, Y., Saitoh, H. et al. Stature estimation in Japanese cadavers based on pelvic measurements in three-dimensional multidetector computed tomographic images. Int J Legal Med 129, 633–639 (2015). https://doi.org/10.1007/s00414-014-1000-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-014-1000-6