
Abstract
Due to the requirement to minimise exposure to radiation, it is desirable to develop non-ionising imaging procedures for the analysis of skeletal maturation for forensic age diagnostics in living individuals. The present pilot study analyses the applicability of ultrasound examinations for the evaluation of apophyseal ossification of the iliac crest. With reference to the sonographic staging of clavicular ossification, the maturation stages of the iliac crest apophysis of 23 male and 16 female subjects, aged 11–20 years, were determined. Ossification stage I occurred in the male subjects at a minimum age of 15.7 years. Ossification stage II was diagnosed in boys at a minimum age of 14.1 years and in girls at a minimum age of 11.7 years. The earliest observation of ossification stage III was at a chronological age of 16.2 years in males and 15.2 years in females. The earliest age of occurrence of ossification stage IV was at least 18.0 years in male test persons and at least 17.1 years in female test persons. The results obtained should be reassessed in a larger number of cases. It is to be expected that sonographic examination of the iliac crest apophysis will become established as a valid and efficient method for forensic age diagnostics in living individuals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A sustained extensive increase in knowledge has been recorded in the scientific field of forensic age estimation in living individuals [2, 12–14, 19–21, 31–33]. Thus, the international and interdisciplinary Study Group on Forensic Age Diagnostics (AGFAD; http://agfad.uni-muenster.de) was able to gather and develop recommendations for age diagnostics in various relevant legal fields [28, 30].
In contexts of criminal law, this process will help to determine whether individuals without valid identity papers have reached the age of criminal responsibility and whether juvenile criminal law is applicable. In civil guardianship and trusteeship matters, as well as in questions concerning the right of asylum of victims of political persecution, where the age of the individuals concerned is not proven, there is a need to investigate whether the relevant age limits have been exceeded. In most countries, the age thresholds between the completed 14th and 18th year of life are relevant for the legal assessment of numerous aspects of criminal, civil and asylum law [9].
Within the area where forensic age estimation in living individuals can be applied, those maturity indicators that develop with easily differentiable morphological changes within the forensically relevant age interval are particularly important. Apart from the clavicula and the skeletal elements of the hand, the apophysis of the iliac crest provides good possibilities for determining skeletal age due to a relatively late completion of maturation [34]. The age-dependent ossification process of this apophysis and its fusion with the iliac bone are well studied, in particular by means of radiography and computed tomography [5, 8, 16]. In the field of clinical orthopaedics, determination of the maturation stage of the apophyseal iliac crest to identify the so-called Risser sign has long been established and can be referred to here as a standard instrument for bone age determination.
In accordance with the current recommendations of the Study Group on Forensic Age Diagnostics, the degree of maturity of the skeletal system should be combined with signs of maturity in physical and dental development in cases of medico-legal age estimations [30]. To determine skeletal age and the degree of mineralisation of the wisdom teeth, the individual must be exposed to radiation. In the absence of a legal basis for authorising X-ray examinations, age estimations in asylum and civil proceedings may only be based on a physical examination as well as a dental inspection of the oral cavity. As a result, the accuracy of the age diagnosis is considerably limited [17].
The establishment of non-ionising imaging procedures for skeletal age determination is an essential research desideratum of all fields of application of forensic age estimation in living individuals in order to minimise the individual radiation exposure of the examined individual, whilst still being able to rely on important skeletal maturity indicators. The present paper presents the results of a pilot study that analyses the forensic applicability of a sonographic evaluation of the apophyseal ossification of the iliac crest for skeletal age assessment.
Test persons and methods
In this study, we prospectively evaluated the individual stage of apophyseal ossification of the left iliac crest in a group of voluntary subjects by means of sonography. The research project had been given favourable opinion by the competent ethics committee.
The test group consisted of a total of 23 male and 16 female children, adolescents and adults from Germany aged 11 to 22 years. Table 1 shows details of the test group figures subdivided by sex and chronological age. None of the subjects displayed any signs of a disease affecting skeletal maturation. All subjects or their legal guardians gave their informed consent for the performance of the examination. The ultrasound examinations were performed using a Pro Focus 2202 (B-K Medical, Herlev, Denmark) equipped with an 8-MHz linear transducer. In prone position, it was possible to scan the apophysis of the iliac crest in all subjects by parallel translation of the transducer in the longitudinal sectional plane setting along its full anterolateral–posteromedial segment. The study results were reached by an examiner certified in the field of skeletal sonography who did not know the subjects’ chronological age.
Corresponding to the constellation of the sonomorphological findings, the ossification stage of the apophyseal iliac crest was determined with reference to the definition of the four stages of clavicular ossification according to Schulz et al. [33].
-
Stage I. The upper margin of the iliac crest is configured at an acute angle. A secondary ossification centre (apophysis) is not educible in the entire region under examination.
-
Stage II. The upper margin of the iliac crest is separated from a secondary ossification centre (apophysis) by an ultrasound gap in the entire region under examination.
-
Stage III. Both section planes with an ultrasound gap between the upper margin of the iliac crest and the secondary ossification centre (apophysis), as well as section planes with a convex curve of the upper margin of the iliac crest without a separate ossification centre (apophysis), are educible in the region under examination.
-
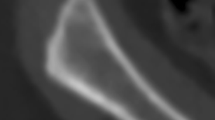
Stage IV. The upper margin of the iliac crest presents a convex curve in the entire region under examination. A separate ossification centre is not definable.
Figure 1 shows the diagram of the sonomorphological staging of apophyseal ossification of the iliac crest. The sonograms in Figs. 2 and 3 show the characteristic sonomorphological findings of stages II and IV.

Diagram of the sonomorphological staging of apophyseal ossification of the iliac crest

Sonomorphology of ossification stage II of the iliac crest apophysis

Sonomorphology of ossification stage IV of the iliac crest apophysis
Results
Classification of the respective sonographic ossification stage of the iliac crest apophysis was possible in all 39 of the examined cases.
Table 2 shows the established minimum and maximum ages, as well as the calculated mean values and standard deviations of ossification stages I to IV, categorised by sex. According to this, the mean values of the subjects’ chronological age increase with progressive ossification stage. The minimum age for ossification stage I was 15.7 years in boys; ossification stage I could not be established in any of the female subjects of this study group. The earliest observation of ossification stage II was at a chronological age of 14.1 years in males and 11.7 years in females. Ossification stage III first occurred at the age of 16.2 years in males and 15.2 years in females. The earliest age of occurrence of ossification stage IV was at least 18.0 years in males and at least 17.1 years in females.
Discussion
Skeletal maturity can be considered to be the most important indicator of growth and differentiation processes of the human organism as a whole. In the course of ontogenesis, the genetically determined maturation sequences of the various skeletal elements occur with great regularity within a certain variation range [3, 15, 23, 29]. This chronological dependency of skeletal development is therefore an essential basis for clinical and forensic estimation of the age of the individual.
There are very close relationships between the maturation processes of different parts of the human skeletal system [22]. For this reason, the stage of maturity of individual-defined skeletal elements can be interpreted as a manifestation of general skeletal maturity. In this context, the ossification process of the iliac crest apophysis was also analysed dependent on the skeletal age of the hand according to Greulich and Pyle, as well as on chronological age [6, 10, 34]. The majority of authors sees a reliable maturity indicator in the developmental progress of the iliac crest apophysis. Thus, Scoles et al. [34] conclude in view of the data they collected that the degree of maturity of this skeletal element in connection with secondary sexual characteristics allows for sufficient conclusions regarding the general progress of ossification in relation to chronological age. Even when the hand skeleton is fully developed, further reaching conclusions regarding chronological age can be drawn by reference to the iliac crest apophysis [4, 18, 38].
So far, collection and interpretation of radiological characteristics of maturity of the pelvis have played a decisive role mainly in the clinical area of application. The first basic knowledge of the development of the iliac crest apophysis goes back to Risser and Ferguson [27]. Their studies led to the development of a classification of maturity based on X-rays of the pelvis (so-called Risser stages), which could be correlated with the residual potential for overall growth of an individual. The potential degree of deformability of the spine dependent on the Risser stages was considered an indication of disease progression in patients with idiopathic scoliosis and thus determines the respective therapeutic approach to this day [25, 26]. According to Risser and other authors, the ossification process starts at the time of the biggest growth spurt in the antolateral area of the spina iliaca anterior superior (ASIS) (Risser stage I) and progresses posteromedially towards the spina iliaca posterior superior (PSIS); apophyseal fusion with more extensive parts of the iliac crest (Risser stage V) is only observed on completion of skeletal development [16, 25, 34]. Diedrichs et al. [8] updated the standard values for the ossification stages according to Risser with due regard to secular acceleration and thus reconfirmed their normal sequence. Determination of the Risser stage by radiographic or computer tomographic means requires a gonadal radiation exposure of the examined children and adolescents that cannot be ignored. Particularly due to the risk of generating germ line mutations through ionising radiation, Exner et al. [10] favour the determination of the skeletal age of the hand rather than making Risser images of the pelvis. With their attempt to perform a sonographic evaluation of the ossification progress of the iliac crest apophysis, Wagner et al. [37] were able to combine requirements for radiation protection and the advantages of a dynamic examination procedure. In a subsequent study, the comparison between sonographic and radiographic detection of the Risser stage in 41 subjects showed a total accuracy of the ultrasound examination of 90.2% [7].
The establishment of non-ionising imaging procedures for determining skeletal maturity is also a priority in forensic age estimation research. In the fields in which skeletal age estimation has been applied so far, the minimisation of radiation exposure required for application to human beings could be met using these methods. Only with them, the use of crucial maturity indicators becomes possible in legal proceedings without a basis for authorising X-ray examinations for the purpose of age estimation. As a radiation-free examination technology, sonography is one of the low-risk imaging procedures that do not require any radiation protection measures or instructions. Furthermore, ultrasound examinations can be performed rapidly and deliver the desired sectional view in real time. Suitable sonography devices occasion relatively low acquisition and operating costs [33]. Not least because of that, they are generally available. The limitations of ultrasound include its operator dependence, the likely lower intrarater and interrater reliability of assessment, and the difficulties with standardisation of documentation and imaging transfer. Therefore, an investigator must have sufficient experience in the field of skeletal sonography and in assessing the degree of ossification of the medial clavicular epiphyseal cartilage. In practical application, the sonographic evaluation of apophyseal ossification of the iliac crest should be completed by a physical examination to increase the diagnostic accuracy and to improve the identification of any relevant developmental disorders.
So far, only a few studies on the applicability of skeletal sonography in forensic age diagnostics are available [24, 33]. With regard to the development of the iliac crest apophysis, there are no forensically useable reference data. Within the scope of the present pilot study, the suitability of ultrasound diagnostics for determining this maturity indicator in criminal, civil and asylum proceedings was studied for the first time.
In order to determine the critical percentage of the sonographically representable apophysis within the total expanse of the iliac crest for staging according to Risser, it is necessary to determine the anatomic points of orientation (ASIS and PSIS) by palpatory means. In particular, the differentiation between Risser stages III and IV may cause significant problems in cases where the PSIS is insufficiently defined [7, 37]. Moreover, contrary to other reports, the apophysis of the iliac crest is formed from two separate secondary ossification centres according to the findings of several authors [11, 35]. These considerations prompted us to assess the sonomorphologically determined apophyseal stage of maturity in accordance with the staging of clavicular ossification laid down by Schulz et al. [33], which is independent of size.
A direct comparison of the median chronological age that we established with the values calculated in various radiographic studies [1, 8, 34, 36, 39] is out of question due to overlaps of the differently defined stages of apophyseal ossification of the iliac crest. However, in consideration of the deviating methodological approach, diverging results are on the whole to be expected. For forensic age diagnostics in living individuals, the earliest possible points in time, at which the ossification stages appear, are of tremendous importance. The age minima established within the scope of the present study indicate the possibility of a valid and efficient diagnosis of the legally decisive age of 14 years, as well as the age of 16 years, which is relevant in asylum proceedings. The obtained results should be checked in a larger number of cases.
References
Anderson M, Hwang SC, Green WT (1965) Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 47:1554–1564
Baumann U, Schulz R, Heinecke A, Schmeling A, Schmidt S (2009) Reference study on the time frame for ossification of the distal radius and ulnar epiphysis on the hand radiograph. Forensic Sci Int 191:15–18
Bernhard W (1988) Reifungsdiagnose an Lebenden. In Knußmann R (Hrsg): Wesen und Methoden der Anthropologie, 1. Teil. Wissenschaftstheorie, Geschichte, morphologische Methoden. 4. Aufl. Thieme, Stuttgart, New York
Coqueugniot H, Weaver TD (2007) Brief communication: infracranial maturation in the skeletal collection from Coimbra, Portugal: new aging standards for epiphyseal union. Am J Phys Anthropol 134:424–437
Dei-Anang J (1998) Die Entwicklung des knöchernen Beckens im Kindes- und Jugendalter im computertomografischen Bild. Dissertation, Mainz
Dhar S, Dangerfield PH, Dorgan JC, Klenerman L (1993) Correlation between bone age and Risser’s sign in adolescent idiopathic scoliosis. Spine 18:14–19
Diedrich V, Wagner UA, Walpert J, von Deimling U, Schmitt O (1995) Sonographische Diagnostik der Beckenkammapophyse (Risser-Zeichen). Orthop Prax 31:700–703
Diedrichs V, Wagner UA, Seiler W, Schmitt O (1998) Referenzwerte zur Entwicklung der Beckenkammapophyse (Risser-Zeichen). Z Orthop 136:226–229
Dünkel F, Grzywa J, Horsfield P, Pruin I (2010) Juvenile justice systems in Europe. Forum, Godesberg
Exner GU, Kaufmann L, Schreiber A (1985) Beziehungen zwischen der Entwicklung der Beckenkammapophysen ("Rissersches Zeichen") und der Handskelettentwicklung bei Mädchen mit Skoliose. Z Orthop Ihre Grenzgeb 123:910–912
Frazer JE (1948) The anatomy of the human skeleton. 4. Aufl. Churchill, London
Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A (2010) Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis using an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med 124:321–325
Kellinghaus M, Schulz R, Vieth V, Schmidt S, Schmeling A (2010) Forensic age estimation in living subjects based on the ossification status of the medial clavicular epiphysis as revealed by thin-slice multidetector computed tomography. Int J Legal Med 124:149–154
Knell B, Ruhstaller P, Prieels F, Schmeling A (2009) Dental age diagnostics by means of radiographical evaluation of the growth stages of lower wisdom teeth. Int J Legal Med 123:465–469
Knussmann R (1996) Vergleichende Biologie des Menschen. Lehrbuch der Anthropologie und Humangenetik, Fischer, Stuttgart
Kotwicki T (2008) Improved accuracy in Risser sign grading with lateral spinal radiography. Eur Spine J 17:1676–1685
Lockemann U, Fuhrmann A, Püschel K, Schmeling A, Geserick G (2004) Empfehlungen für die Altersdiagnostik bei Jugendlichen und jungen Erwachsenen außerhalb des Strafverfahrens. Rechtsmedizin 14:123–125
McKern TW, Stewart TD (1957) Skeletal Age changes in young American males. Analyzed from the standpoint of age identification. Technical report EP-45, Natick, Ma., Quartermaster Research and Development Center, US Army
Olze A, Pynn BR, Kraul V, Schulz R, Heinecke A, Pfeiffer H, Schmeling A (2010) Studies on the chronology of third molar mineralization in First Nations people of Canada. Int J Legal Med. doi:10.1007/s00414-010-0483-z
Olze A, Solheim T, Schulz R, Kupfer M, Pfeiffer H, Schmeling A (2010) Assessment of the radiographic visibility of the periodontal ligament in the lower third molars for the purpose of forensic age estimation in living individuals. Int J Legal Med. doi:10.1007/s00414-010-0488-7
Olze A, Solheim T, Schulz R, Kupfer M, Schmeling A (2010) Evaluation of the radiographic visibility of the root pulp in the lower third molars for the purpose of forensic age estimation in living individuals. Int J Legal Med 124:183–186
Pelech L, Pechstein J (1976) Vergleichende Untersuchungen über die Entwicklung des Skelettalters bei tschechischen und süddeutschen Kindern. Ärztl Jugendkd 67:23–28
Pelsmaekers B, Loos R, Carels C, Derom C, Vlietinck R (1997) The genetic contribution to dental maturation. J Dent Res 76:1337–1340
Quirmbach F, Ramsthaler F, Verhoff MA (2009) Evaluation of the ossification of the medial clavicular epiphysis with a digital ultrasonic system to determine the age threshold of 21 years. Int J Legal Med 123:241–245
Risser JC (1948) Important practical facts in the treatment of scoliosis. Instr Course Lect 5:248–260
Risser JC (1958) The iliac apophysis: an invaluable sign in the management of scoliosis. Clin Orthop 11:111–118
Risser JC, Ferguson AB (1936) Scoliosis: its prognosis. J Bone Joint Surg 18:667–670
Ritz-Timme S, Kaatsch H-J, Marré B, Reisinger W, Riepert T, Rösing FW, Rötzscher K, Schmeling A, Geserick G (2002) Empfehlungen für die Altersdiagnostik bei Lebenden im Rentenverfahren. Rechtsmedizin 12:193–194
Rösing FW (2000) Forensische Altersdiagnose: Statistik, Arbeitsregeln und Darstellung. In: Oehmichen M, Geserick G (Hrsg): Osteologische Identifikation (Research in Legal Medicine/Rechtsmedizinische Forschungsergebnisse). Schmidt-Römhild, Lübeck
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rösing FW, Rötzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Legal Med 122:457–460
Schmidt S, Nitz I, Schulz R, Tsokos M, Schmeling A (2009) The digital atlas of skeletal maturity by Gilsanz and Ratib: a suitable alternative for age estimation of living individuals in criminal proceedings? Int J Legal Med 123:489–494
Schulz R, Mühler M, Reisinger W, Schmidt S, Schmeling A (2008) Radiographic staging of ossification of the medial clavicular epiphysis. Int J Legal Med 122:55–58
Schulz R, Zwiesigk P, Schiborr M, Schmidt S, Schmeling A (2008) Ultrasound studies on the time course of clavicular ossification. Int J Legal Med 122:163–167
Scoles PV, Salvagno R, Villalba K, Riew D (1988) Relationship of iliac crest maturation to skeletal and chronologic age. J Pediatr Orthop 8:639–644
Stevenson PH (1924) Age order of epiphyseal union in man. Am J Phys Anthropol 7:53–93
Urbaniak JR, Schaffer WW, Stelling FH (1976) Iliac apophyses: prognostic value in idiopathic scoliosis. Clin Orthop 116:80–85
Wagner UA, Diedrich V, Schmitt O (1995) Determination of skeletal maturity by ultrasound: a preliminary report. Skeletal Radiol 24:417–420
Webb O, Suchey M (1985) Epiphyseal union of the anterior iliac crest and medial clavicle in a modern multiracial sample of American males and females. Amer J Phys Anthropol 68:457–466
Zaoussis AL, James JIP (1958) The iliac apophysis and the evaluation of curves in scoliosis. J Bone Joint Surg 40:442–453
Acknowledgements
The authors would like to thank the Förderverein Rechtsmedizin Münster e.V. for its financial support and the DRK-Kliniken Köpenick for providing the ultrasound scanner and examination rooms.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schmidt, S., Schmeling, A., Zwiesigk, P. et al. Sonographic evaluation of apophyseal ossification of the iliac crest in forensic age diagnostics in living individuals. Int J Legal Med 125, 271–276 (2011). https://doi.org/10.1007/s00414-011-0554-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-011-0554-9