
Abstract
The present paper analyses the applicability of the clinically prevalent skeletal age determination method of Tanner and Whitehouse for forensic age estimation in living individuals. For this purpose, the hand X-rays from 48 boys and 44 girls aged 12–16 years were evaluated retrospectively. The minima and maxima, the mean values with their standard deviations as well as the medians with upper and lower quartiles, are presented for the skeletal ages 12–16 years estimated by the TW2 and TW3 methods. In the legally relevant skeletal age group 14–16 years, the differences between the skeletal age and the mean value of the chronological age were between −0.1 and +1.4 years for the TW2 method. For the TW3 method, the differences between the skeletal age and the mean value of the chronological age were between −0.4 and +0.2 years in the relevant age group. Due to the risk of serious overestimations, the TW2 method seems to be unsuitable for forensic age diagnostics. The application of the TW3 method for forensic age estimations can be recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
An important issue regarding the assessment of the sentence in criminal proceedings is the clarification of the defendant’s age. Especially in foreigners without valid identification documents, difficulties arise when it comes to deciding whether juvenile or adult criminal law is to be applied. In most countries, the relevant limits are between 14 and 18 years of age [10].
In recent years, age estimations of living individuals in criminal proceedings have become an essential part of forensic science [5, 7, 24, 25, 36, 37, 39, 40].
Today, in accordance with the recommendations of the Arbeitsgemeinschaft für Forensische Altersdiagnostik (Study Group on Forensic Age Diagnostics; http://rechtsmedizin.klinikum.uni-muenster.de/agfad/index.htm), the examination findings of the signs of maturity from three independent developmental systems are combined to achieve the maximum possible diagnostic accuracy and to improve the estimation precision.
The physical examination includes the determination of anthropometric measurements as well as the inspection of the signs of sexual maturity. At the same time, it provides the opportunity to reveal diseases that might have an impact on maturation.
The dental examination includes both an inspection of the oral cavity and the assessment of an orthopantomogram to determine the signs of maturity of the dental development.
The signs of maturity of the skeletal development are evaluated by means of a radiologic examination of the left hand. In addition, a conventional X-ray or computed tomography examination of the clavicles is done to decide whether an individual has completed the 18th year of life.
The X-ray examination of the hand skeleton is particularly important among the applied methods due to the differentiation, occurring at different points in time, of the varying epiphyses until maturation is completed at the age of 18.
The established methods for the determination of the hand ossification follow two different basic principles.
By use of the atlas methods, bone age can be determined by comparing the total maturity pattern of an X-ray with standard X-rays of corresponding age and sex [14, 46, 47]. The most commonly used and most accepted method of this group worldwide is the atlas method of Greulich and Pyle. Both its clinical [18, 23, 26–28] and its forensic applicability [38] have been demonstrated in several studies. Due to the more relevant reference population, the atlas method of Thiemann and Nitz can be recommended for forensic age diagnostics as well [31, 34, 35].
The single bone method is based on the determination of the degree of maturity of selected skeletal elements on an X-ray. Specific scores allow the assessment of the total bone age by calculating the sum of the assigned maturity scores [29, 42, 43, 45]. Especially in Europe, the radius, ulna, short bones (RUS) score of Tanner and Whitehouse is widely applied in clinical examinations and research [12].
Within the present paper, the forensic applicability of the skeletal age determination method of Tanner and Whitehouse for the forensic age estimation is studied.
Materials and methods
The X-rays of the left hand from 48 male and 44 female children and adolescents aged 12–16 years were evaluated retrospectively.
Table 1 shows the number of cases by sex and chronological age.
These images had been prepared between 1986 and 2002 at an orthopaedic practice in Papenburg (Lower Saxony, Germany) for the purpose of predicting adult height. All patients included in the study were children and adolescents displaying normal physical development for their respective age group. Individuals with signs of bone development disorders were excluded from the study.
The dorsopalmar X-rays of the left hand were available in a digitalized form at a scale of 1:1. An expert for the assessment of hand radiograms determined the skeletal age according to the method of Tanner and Whitehouse by means of the sex-specific RUS score. For this, the respective degree of maturity of the distal epiphyses of radius and ulna and/or the epiphyses of the ossa metacarpalia I, III and V, the basophalanges I, III and V, the mesophalanges III and V as well as the telephalanges I, III and V was assessed with a scoring system. Corresponding to the sum of these scores, the respective bone age was assessed in conformity with the second (TW2) and third version (TW3) of the atlas by Tanner and Whitehouse [43, 45].
The statistical analysis of the data was carried out with the help of Statistical Package for the Social Sciences (version 12).
Results
Tables 2 and 3 show the results of the analysis for the skeletal ages 12 to 16 by sex. The minima and maxima, the mean values with their standard deviations as well as the medians with upper and lower quartiles, are presented as statistical parameters. As the number of cases was too low for TW3 in females, no parameters are indicated for the skeletal age of 16 years.
Both for TW2 and TW3, a strong correlation between skeletal age and chronological age was determined; this means that, in most cases, the mean values and medians of the chronological age increased with increasing skeletal age.
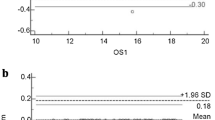
The statistical parameters for the skeletal ages of 14, 15 and 16 years are particularly important in forensic age estimation practice to establish whether a person is at least 14 years old. For the TW2 method, the standard deviations for the girls in this age group were between 0.4 and 1.0 years and for the boys between 0.9 and 1.1 years. For the TW3 method, the standard deviations in this age group were between 0.6 and 1.0 years for girls and between 0.6 and 1.1 years for boys. In this age group, the differences between the skeletal age and the mean value of the chronological age were between −0.1 and +1.4 years for the TW2 method. Here, a negative sign means that the skeletal age is lower than the chronological age. For the TW3 method, the differences between the skeletal age and the mean value of the chronological age were −0.4 to +0.2 years in the relevant age group.
Discussion
In 1962, Tanner et al. developed a skeletal age determination method by means of the degree of maturity of individual bones of the hand (Tanner–Whitehouse method 1, TW1) on the basis of the Oxford method [1, 41]. In the second version of this method (TW2), which was published in 1975, the stages that are difficult to determine were eliminated and the maturity scores were revised [42, 43]. The reference population of the TW2 method included about 3,000 British children from the lower and middle classes. The X-rays had been taken between 1946 and 1970. Particularly, the RUS score is widely applied in clinical practice due to its restriction to radius, ulna and the short bones of the first, third and fifth digit ray. For the TW3 method, which was published in 2001, the reference population was adjusted to the secular trend. The updated reference values are based on studies from Belgium [4], Spain [17] and the USA [44]. The stage descriptions and the assigned scores, however, have not been changed since the TW2 version. Ahmed and Warner [2] criticized that the TW3 method had hitherto hardly been known in Great Britain and, thus, had rarely been applied.
The suitability of the Tanner–Whitehouse method for clinical issues has been studied in numerous papers [3, 6, 9, 16, 48].
An important advantage of the Tanner–Whitehouse method for clinical concerns, in comparison with the atlas methods, is the applicability in dissociated bone maturation, a possible consequence of diencephalic and/or hypothalamic disorders [13, 33]. But as these developmental disorders contraindicate forensic age estimations, this advantage of the Tanner–Whitehouse method is of no significance for forensic age estimations.
The relatively high time exposure per skeletal age determination needs to be mentioned as a disadvantage of the Tanner–Whitehouse system. Several papers demonstrate that this time exposure is out of all proportion to a possible improvement of the estimation accuracy of established atlas methods [3, 8, 20, 21, 49]. The required processing time per X-ray can be reduced with increasing experience, but compared to the atlas method of Greulich and Pyle it takes four to five times longer even for an experienced examiner [20, 21].
Furthermore, the practicability of the skeletal age determination method of Tanner–Whitehouse is limited because it is relatively difficult to learn. Like all single bone methods, it is based on the assessment of the degree of maturity of selected skeletal elements of the hand. Thus, in the RUS score, the distal epiphyses of the radius and ulna as well as the epiphyses of the short bones of the first, third and fifth ray are considered. Depending on their degree of ossification, their size and shape as well as the degree of fusion with the metaphysics, a stage of maturity can be defined for each bone. Both textual descriptions and illustrations of the feature characteristics in form of schematic diagrams and comparison X-rays help to determine the stage of maturity. In all cases of doubt, it is the written description that should be followed; the diagrams should serve as an aide-memoire, not as the sole means of comparison [42]. However, many examiners believe that the texts are slightly too difficult to understand, promoting an ostensible concentration on the attached illustrations [9], but the primary use of diagrams which are reduced to the basic characteristics is a possible source of diagnostic errors [15].
The single bones considered in the RUS score provide a varied information content regarding the determination of the total maturity of the hand skeleton. Therefore, they have a differentiated emphasis in age diagnoses. It should be critically considered that, in the Tanner–Whitehouse system, the scores were assigned to the individual criteria completely arbitrarily [11]. Unlike the Fels method [29], the skeletal maturity score of this method does not consider the probabilities of the inter-individually different presence of maturity indicators in the reference population [22].
The single bone scores of the distal epiphyses of radius and ulna are of particular importance for the calculation of the skeletal age of the hand according to Tanner–Whitehouse. The difference in the score determination of two adjacent stages already bares the risk of severe miscalculations. Considering the great influence on the overall diagnosis, the present differentiation of stages for radius and ulna must be regarded as being too rough. Weber [49] came to similar conclusions. For both bones, an additional differentiation of the development would be appropriate especially in the final stage. In consideration of the forensic importance of the disappearance of the epiphyseal scar of the radius [37], this characteristic may be distinguished from the processes occurring at the beginning of ossification, for example, and/or the completed ossification of the epiphyseal cartilage.
According to the authors’ knowledge, the present paper is the first one to study the applicability of the skeletal age determination method of Tanner and Whitehouse for forensic age estimation in criminal proceedings.
Methods, which determine the chronological age as precisely as possible, are desirable for forensic age estimation. For normal distributions, the standard deviation of the mean value is a measure of precision. It can be assumed that the chronological age is almost normally distributed. In the present study, the standard deviations in the skeletal age from 14–16 years, which is particularly relevant for forensic age estimation, were between 0.4 and 1.1 years for the TW2 method and between 0.6 and 1.1 years for the TW3 method. For the atlas method of Greulich and Pyle, the standard deviations in this age group were between 0.3 and 1.7 years [38]. For the atlas method of Thiemann and Nitz, the standard deviations in the relevant age group were between 0.3 and 1.2 years [34]. However, attention should be paid here to the higher number of cases in the reference studies of these atlas methods, which might have led to an increase of the range. This assumption is supported by the fact that, in clinical studies, only insignificant differences have been established between the estimation accuracy of the TW2 method and the Greulich–Pyle method [3, 18, 19].
Age overestimations, meaning that the examined individual was estimated to be older than the actual chronological age, have to be prevented by all means in age estimations in criminal proceedings. Therefore, a consideration of the differences between the skeletal ages and the mean values of the chronological age is of interest. There is an age overestimation when the difference between the skeletal age and the mean value of the chronological age has a positive sign. For the TW2 method, there were considerably more age overestimations, with a difference between the skeletal age and the mean value of the chronological age of up to +1.4 years. For the TW3 method, however, the maximum age overestimation in the legally relevant age group was merely +0.2 years. This forensically important difference is caused by the degree of acceleration of the reference population of the respective methods because a relatively high socioeconomic status leads to an acceleration of the skeletal maturation [30, 32]. While the TW2 method is based on British individuals from the lower and middle classes who had been examined between 1946 and 1970, the TW3 method is based on a considerably more accelerated reference population. Due to the risk of serious overestimation, the TW2 method cannot be recommended for forensic age estimations.
Conclusions
-
1.
Due to the risk of serious overestimation, the TW2 method seems to be unsuitable for forensic age estimations.
-
2.
The application of the TW3 method for forensic age estimations can be recommended.
-
3.
The applicability of this single bone method in dissociated bone maturation is an important advantage for clinical issues but irrelevant for forensic age estimations.
-
4.
Compared to the atlas methods, the higher time expenditure of the TW method, the difficulty to learn it, the arbitrary assignment of the scores to the degrees of maturity as well as the rough staging of ossification of ulna and radius must be considered as disadvantages.
References
Acheson RM (1954) A method of assessing skeletal maturity from radiographs: a report from the Oxford Child Health Survey. J Anat 88:498–508
Ahmed ML, Warner JT (2007) TW2 and TW3 bone ages: time to change. Arch Dis Child 92:371–372
Andersen E (1971) Comparison of Tanner–Whitehouse and Greulich–Pyle methods in a large scale Danish survey. Am J Phys Anthropol 35:373–376
Beunen G, Lefevre J, Ostyn M, Renson R, Simons J, van Gernen D (1990) Skeletal maturity in Belgian youths assessed by the Tanner–Whitehouse method (TW2). Ann Hum Biol 17:355–376
Braga J, Treil J (2007) Estimation of pediatric skeletal age using geometric morphometrics and three-dimensional cranial size changes. Int J Legal Med 121:439–443
Bull RK, Edwards PD, Kemp PM, Fry S, Hughes IA (1999) Bone age assessment: a large scale comparison of the Greulich and Pyle, and Tanner and Whitehouse (TW2) methods. Arch Dis Child 81:172–173
Cameriere R, De Angelis D, Ferrante L, Scarpino F, Cingolani M (2007) Age estimation in children by measurement of open apices in teeth: a European formula. Int J Legal Med 121:449–453
Cole AJL, Webb L, Cole TJ (1988) Bone age estimation: a comparison of methods. Br J Radiol 61:683–686
Cox LA (1996) Tanner–Whitehouse method of assessing skeletal maturity: problems and common errors. Horm Res 45(Suppl 2):53–55
Dünkel F, van Kalmthout A, Schüler-Springorum H (1997) Entwicklungstendenzen und Reformstrategien im Jugendstrafrecht im europäischen Vergleich. Forum, Mönchengladbach
Fendel H (1976) Die Methodik der radiologischen Skeletalterbestimmung. Radiologe 16:370–380
Gilli G (1996) The assessment of skeletal maturation. Horm Res 45 Suppl 2:49–52
Graham CB (1972) Assessment of bone maturation—methods and pitfalls. Radiol Clin N Amer 10:185–202
Greulich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press, Stanford
Haavikko K, Kilpinen E (1973) Skeletal development of Finnish children in the light of hand–wrist roentgenograms. Proc Finn Dent Soc 69:182–190
Helm S (1979) Skeletal maturity in Danish schoolchildren assessed by the TW2 method. Am J Phys Anthropol 51:345–352
Hernandez M, Sanchez E, Sobradillo B, Rincon JM (1991) Skeletal maturation and height prediction: atlas and scoring methods. Diaz de Santos, Madrid
Johnston FE (1971) The use of the Greulich–Pyle method in a longitudinal growth study. Am J Phys Anthropol 35:353–357
Kemperdick HF (1981) Skelettalter-Bestimmung bei Kindern mit normalem und abweichendem Wachstumsverlauf. Fortschr Med 99:152–156
Kemperdick H (1986) Die Skelettalterbestimmung beim Kind. Radiologe 26:216–221
King DG, Steventon DM, O’Sullivan MP, Cook AM, Hornsby VP, Jefferson IG (1994) Reproducibility of bone ages when performed by radiology registrars: an audit of Tanner and Whitehouse II versus Greulich and Pyle methods. Br J Radiol 67:848–851
van Lenthe FJ, Kemper HC, van Mechelen W (1998) Skeletal maturation in adolescence: a comparison between the Tanner–Whitehouse II and the Fels method. Eur J Pediatr 157:257–261
Low WD (1975) Assessing skeletal maturity by inspection and bone-specific methods with the atlas of Greulich and Pyle. Z Morphol Anthropol 67:1–5
Meijerman L, Maat GJR, Schulz R, Schmeling A (2007) Variables affecting the probability of complete fusion of the medial clavicular epiphysis. Int J Legal Med 121:463–468
Olze A, van Niekerk P, Ishikawa T, Zhu BL, Schulz R, Maeda H, Schmeling A (2007) Comparative study on the effect of ethnicity on wisdom tooth eruption. Int J Legal Med 121:445–448
Rikhasor RM, Qureshi AM, Rathi SL, Channa NA (1999) Skeletal maturity in Pakistani children. J Anat 195:305–308
Roche AF, Roberts J, Hamill PVV (1975) Skeletal maturity of children 6–11 years: racial, geographic area and socioeconomic differentials, United States. National Center for Health Statistics, series 11, no. 149. DHEW Publication no. (HRA) 76-1631. DHEW, Rockville
Roche AF, Roberts J, Hamill PVV (1978) Skeletal maturity of youth 12–17 years. Racial, geographic area and socioeconomic differentials. (Vital and health statistics. US Dept. of Health, Education and Welfare. Series 11. No. 167). US Government Printing Office, Washington, D.C.
Roche AF, Chumlea WC, Thissen D (1988) Assessing the skeletal maturity of the hand–wrist: Fels method. Thomas, Springfield
Schmeling A, Reisinger W, Loreck D, Vendura K, Markus W, Geserick G (2000) Effects of ethnicity on skeletal maturation: consequences for forensic age estimations. Int J Legal Med 113:253–258
Schmeling A, Baumann U, Schmidt S, Wernecke K-D, Reisinger W (2006) Reference data for the Thiemann–Nitz method of assessing skeletal age for the purpose of forensic age estimation. Int J Legal Med 120:1–4
Schmeling A, Schulz R, Danner B, Rösing FW (2006) The impact of economic progress and modernization in medicine on the ossification of hand and wrist. Int J Legal Med 120:121–126
Schmid F (1974) Skelettentwicklung bei hirnorganischen Störungen. Kinderarzt 5:1045–1047
Schmidt S, Koch B, Mühler M, Reisinger W, Schmeling A (2007) Optimizing the Thiemann–Nitz method for skeletal age determination for forensic age diagnostics in live subjects. Scand J Forensic Sci 13:5–7
Schmidt S, Koch B, Schulz R, Reisinger W, Schmeling A (2007) Comparative analysis of the applicability of the skeletal age determination methods of Greulich–Pyle and Thiemann–Nitz for forensic age estimation in living subjects. Int J Legal Med 121:293–296
Schmidt S, Mühler M, Schmeling A, Reisinger W, Schulz R (2007) Magnetic resonance imaging of the clavicular ossification. Int J Legal Med 121:321–324
Schmidt S, Baumann U, Schulz R, Reisinger W, Schmeling A (2008) Study of age dependence of epiphyseal ossification of the hand skeleton. Int J Legal Med 122:51–54
Schmidt S, Koch B, Schulz R, Reisinger W, Schmeling A (2008) Studies in use of the Greulich–Pyle skeletal age method to assess criminal liability. Int J Legal Med DOI 10.1016/j.legalmed.2008.01.003
Schulz R, Mühler M, Reisinger W, Schmidt S, Schmeling A (2008) Radiographic staging of ossification of the medial clavicular epiphysis. Int J Legal Med 122:55–58
Schulz R, Zwiesigk P, Schiborr M, Schmidt S, Schmeling A (2008) Ultrasound studies on the time course of clavicular ossification. Int J Legal Med 122:163–167
Tanner JM, Whitehouse RH, Healy MJR (1962) A new system for estimating skeletal maturity from the hand and wrist with standards derived from a study of 2600 healthy British children. Part II. The scoring system. Int Child Centre, Paris
Tanner JM, Whitehouse RH, Marshall WA, Healy MJR, Goldstein H (1975) Assessment of skeletal maturity and prediction of adult height (TW2 method). Academic, London
Tanner JM, Whitehouse RH, Marshall WA, Healy MJR, Goldstein H (1983) Assessment of skeletal maturity and prediction of adult height (TW2 method), 2nd edn. Academic Press, London
Tanner JM, Oshman D, Bahhage F, Healy M (1997) Tanner–Whithouse bone age reference values for North American children. J Pediatr 131:34–40
Tanner JM, Healy MJR, Goldstein H, Cameron N (2001) Assessment of skeletal maturity and prediction of adult height (TW3 method). Saunders, London
Thiemann H-H, Nitz I (1991) Röntgenatlas der normalen Hand im Kindesalter. Thieme, Leipzig
Thiemann H-H, Nitz I, Schmeling A (2006) Röntgenatlas der normalen Hand im Kindesalter. Thieme, Stuttgart
Vignolo M, Milani S, Cerbello G, Coroli P, Di Battista E, Aicardi G (1992) FELS, Greulich–Pyle, and Tanner–Whitehouse bone age assessments in a group of Italian children and adolescents. Am J Hum Biol 4:493–500
Weber R (1978) Genauigkeit der Skelettalterbestimmungen und Größenprognosen nach den Methoden von Greulich and Pyle sowie Tanner and Whitehouse, Dissertation. Freie Universität, Berlin
Acknowledgements
The authors wish to thank Dr. Karl Minas for kindly permitting the use of the hand radiographs assessed here.
Author information
Authors and Affiliations
Corresponding author
Additional information
Dedicated to Prof. Dr. G. Geserick on the occasion of his 70th birthday.
Rights and permissions
About this article
Cite this article
Schmidt, S., Nitz, I., Schulz, R. et al. Applicability of the skeletal age determination method of Tanner and Whitehouse for forensic age diagnostics. Int J Legal Med 122, 309–314 (2008). https://doi.org/10.1007/s00414-008-0237-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-008-0237-3