
Abstract
Evaluation of hand ossification is a main pillar of radiological age diagnosis in living subjects. In the present study, we comparatively assessed the Greulich–Pyle and Thiemann–Nitz methods for accuracy of age estimation and degree of acceleration in the respective reference populations. For this, the skeletal age of 649 hand X-rays from German subjects aged 1–18 years was determined by both methods. Accuracy of the age estimates was determined based on regression and measures of certainty. In terms of accuracy, both methods seem to be equally well suited for forensic age diagnostics. The degree of acceleration in the reference populations for the two methods was calculated as the mean difference between the estimated skeletal age and the actual age of a test subject. Compared to the Greulich–Pyle population, the Thiemann–Nitz population was accelerated by 0.44 years in both male and female subjects. When an expert opinion is required and one cannot exclude the possibility that the investigated subject may come from a population with a high acceleration status, the Thiemann–Nitz method should preferably be used to prevent overestimation of age.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Increasing transnational migratory movement is a prominent feature of the steadily advancing process of globalization. In Germany and other countries, the number of foreigners whose date of birth cannot be proven beyond doubt has therefore grown in recent years. Since the mid-1990s, forensic institutes have been receiving more and more court orders to conduct forensic age estimations because of missing or false age-defining information from subjects under investigation. Expert appraisal of juvenile offenders has meanwhile become an integral part of forensic practice.
In Germany, the ages of 14, 16, 18, and 21 are of relevance in criminal law [8]. Age thresholds of relevance to criminal prosecution fall between the 14th and 18th years of life in many other European countries as well, but age of criminal responsibility is reached much sooner in some countries [6].
To be useful in a court of law, age estimates of criminal offenders must meet particularly strict validity standards. The development of scientific age determination methods that are suitable for use in the justice system has led to the establishment of an autonomous and productive new branch of forensic science [2–4, 10–13, 16–18].
The international interdisciplinary Study Group on Forensic Age Diagnostics ( http://www.charite.de/rechtsmedizin/agfad/index.htm) has, by general consensus, developed a three-part procedure for the production of forensic age assessments of maximum reliability for use in criminal proceedings. This procedure calls for physical and dental examinations as well as for a roentgenographic examination. In the physical examination, the subject is evaluated with regard to anthropometric data, signs of sexual maturity, and questionable developmental disorders of relevance to age. The dental examination should include a determination of dental status and assessment of a panoramic radiographic. The radiographic examination should always include an evaluation of an X-ray of the left hand. If the question of whether the subject has completed the 21st year of life is relevant, then additional radiographic assessment of the clavicle should also be considered [15].
In addition to the forensic age diagnostics in live subjects, skeletal age determination by Greulich–Pyle and Thiemann–Nitz is of particular importance in regard to clinical questions and to investigations of human cadavers.
Modern conventional methods for assessing skeletal development of the hand can be divided into two groups by a methodological approach. The single-bone method is based on determination of the degree of maturity of selected skeletal elements. The atlas method, on the other hand, determines bone age by comparing an X-ray of the test subject’s hand with standard roentgenograms from age and sex-matched controls.
As various studies have shown, the atlas-based method is less time-consuming than the single bone method, yet produces results of comparable accuracy [1, 5, 9]. Greulich and Pyle’s atlas method is the best-established method used on an international scale. Thiemann and Nitz’s radiographic atlas, on the other hand, is mainly used in German-speaking countries.
The accuracy of age assessment of the two methods as well as the degree of acceleration in the populations on which the age assessments are based will be determined and compared in the scope of the present study.
Materials and methods
A total of 649 roentgenograms of the left hand of 303 female and 346 male subjects of ages ranging from 1 to 18 years were analyzed retrospectively. The X-rays were taken at an orthopedic practice in Papenburg, Germany, during the years 1986 to 2002 for the purpose of preparing a final height prediction. The number of cases studied, by age and sex, is shown in Table 1. All patients included in the study were children and adolescents displaying normal physical development for their respective age group. Individuals with signs of bone development disorders were excluded from the study. One can assume that, in terms of average composition, the study population was roughly representative of the German population.
The roentgenograms were digitized on a scale of 1:1 and processed with Adobe Photoshop (version 5.0). The bone age of each test subject was then determined by the atlas methods of Greulich and Pyle and Thiemann and Nitz using sex and age-matched standard roentgenograms, schematic diagrams with descriptions of the indicators of maturity, and skeletal measurements. The observer performing these age estimations was blinded to the chronological ages of the test sample.
In the statistical analysis, correlations between actual age and skeletal age were determined by means of a simple linear regression analysis. The regression formulae express the mathematical relation between chronological and skeletal age at the best possible rate and allow determination of estimates beyond direct observation. The corresponding coefficients of determination (R 2) were calculated to evaluate the degree of reliance on the dependence between age variables given in these formulae. R 2 specifies the proportion of total bone age variance that may be attributed to chronological age based on regression.
To detect potential acceleration or retardation in the reference population in comparison to the test population, Bland–Altman plots were used to determine the mean differences between skeletal age and actual age in each subgroup.
Results
The following regression equations and measures of certainty were used to assess the correlation between skeletal age (x) and actual age (y):
Figure 1 shows a regression diagram for actual age vs skeletal age as determined in the male test subjects according to the Greulich–Pyle method.

Regression line with confidence limits for actual age vs skeletal age, as determined by the Greulich–Pyle (G/P) method, in male subjects
The mean differences (in years)±double standard deviation between skeletal age and actual age were as follows:
Greulich–Pyle method (males): −0.49 ± 2.02
Greulich–Pyle method (females): −0.39 ± 2.16
Thiemann–Nitz method (males): −0.05 ± 1.65
Thiemann–Nitz method (females): +0.05 ± 1.74
When the mean difference is negative, the chronological age was greater than the bone age; consequently, the respective study population was accelerated compared to the reference population used for the corresponding test method.
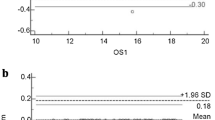
Figure 2 shows a Bland–Altman plot for actual age vs skeletal age as determined in the male test subjects according to the Greulich–Pyle method.

Bland–Altman plot of the relationship between actual age and skeletal age, as estimated according to the Greulich–Pyle (G/P) method, in male subjects
Discussion
Greulich and Pyle’s radiographic atlas method is currently the most commonly used method worldwide for determining skeletal age. The selective sample on which their method is based consists of 1,000 Americans of northern European descent living in Cleveland, OH, aged between 0 and 18 years. Greulich and Pyle’s research of the hand X-rays produced by the Brush Foundation longitudinal study dates back to the period from 1931 to 1942. In contrast, the Thiemann–Nitz radiographic atlas method is based on a much more recent study conducted in 1977. It is based on an analysis of hand X-rays taken of a representative sample of 5,200 healthy children and adolescents aged between 0 and 18 years at 20 medical institutions in the former German Democratic Republic.
In the present study, we compared the Greulich–Pyle and Thiemann–Nitz methods of age assessment in terms of accuracy of age estimation and degree of acceleration in the reference populations upon which the estimates were based.
The degree of certainty of regression was used as a measure of accuracy. The calculated degree of certainty of the male test subjects was 0.953 for the Greulich–Pyle method and 0.955 for the Thiemann–Nitz method. The degree of certainty for the female subjects was 0.922 for the Greulich–Pyle method and 0.927 for the Thiemann–Nitz method. The differences in the degrees of certainty of the two methods were small, with those for the Thiemann–Nitz method being slightly higher. This suggests that, in terms of accuracy, both methods are equally well suited for use in forensic age assessment.
The degree of acceleration in the reference populations for the two methods was measured as the mean difference between the estimated skeletal age and the actual age of the test subjects. The mean difference between skeletal age, as calculated using the Greulich and Pyle method, and actual age was −0.49 years for boys and −0.39 years for girls. Compared to the Greulich–Pyle reference population, the boys in our test population were therefore accelerated by 0.49 years and the girls by 0.39 years. In the Thiemann–Nitz group, the mean difference between bone age and actual age was −0.05 years for boys and +0.05 years for girls. In other words, our study population differed only slightly from the Thiemann–Nitz reference population in terms of acceleration status. These results suggest that the Thiemann–Nitz population is accelerated by 0.44 years relative to the Greulich–Pyle population. The reason for this difference in acceleration status may be that the studies on which the Thiemann–Nitz atlas is based were conducted several decades later than the study performed by Greulich and Pyle.
This gives rise to an important question: What are the practical consequences of using the Greulich–Pyle or Thiemann–Nitz method to obtain forensic age assessments for individuals who do not belong to the population studied by us? After an extensive review of the research literature on the chronological course of hand ossification in numerous populations of all the main ethnic groups, Schmeling et al. [14] came to the conclusion that, within the relevant age group, ethnic origin does not seem to have a significant effect on the ossification rate. The medical and economic modernization status of a population, on the other hand, has a decisive impact on the ossification rate, and a relatively low acceleration rate leads to a delay in development. Consequently, the use of data from reference populations with a high acceleration status to estimate the age of individuals from populations with a low acceleration status will therefore lead to underestimation of age; in criminal proceedings, this will not result in negative consequences for the affected individual [17]. In the case of court-ordered age estimates, one can usually assume that the individuals to be investigated come from populations with a relatively low acceleration status. Both of the investigated methods of skeletal age determination lead to underestimation of age in these cases. In cases where one cannot exclude the possibility that the investigated subject may come from a population with a high acceleration status, the Thiemann–Nitz method should preferably be used to avoid overestimation of age. At any rate, the expert report accompanying a radiological age assessment should always point out the consequences of acceleration status discrepancies on the age diagnosis.
References
Andersen E (1971) Comparison of Tanner–Whitehouse and Greulich–Pyle methods in a large scale Danish survey. Am J Phys Anthropol 35:373–376
Braga J, Heuze Y, Chabadel O, Sonan NK, Gueramy A (2005) Non-adult dental age assessment: correspondence analysis and linear regression versus Bayesian predictions. Int J Legal Med 119:260–274
Cameriere R, Ferrante L, Cingolani M (2006) Age estimation in children by measurement of open apices in teeth. Int J Legal Med 120:49–52
Cameriere R, Ferrante L, Mirtella D, Cingolani M (2006) Carpals and epiphyses of radius and ulna as age indicators. Int J Legal Med 120:143–146
Cole AJL, Webb L, Cole TJ (1988) Bone age estimation: a comparison of methods. Br J Radiol 61:683–686
Dünkel F, van Kalmthout A, Schüler-Springorum H (1997) Entwicklungstendenzen und Reformstrategien im Jugendstrafrecht im europäischen Vergleich. Forum, Mönchengladbach
Greulich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist. Stanford Univ. Press, Stanford, California
Kaatsch H-J (2001) Juristische Aspekte der Altersschätzung. In: Oehmichen M, Geserick G (Hrsg) Osteologische Identifikation und Altersschätzung. Schmidt-Römhild, Lübeck, pp 243–254
King DG, Steventon DM, O´Sullivan MP, Cook AM, Hornsby VP, Jefferson IG (1994) Reproducibility of bone ages when performed by radiology registrars: an audit of Tanner and Whitehouse II versus Greulich and Pyle methods. Br J Radiol 67:848–851
Mühler M, Schulz R, Schmidt S, Schmeling A, Reisinger W (2006) The influence of slice thickness on assessment of clavicle ossification in forensic age diagnostics. Int J Legal Med 120:15–17
Olze A, Bilang D, Schmidt S, Wernecke K-D, Geserick G, Schmeling A (2005) Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med 119:22–26
Paewinsky E, Pfeiffer H, Brinkmann B (2005) Quantification of secondary dentine formation from orthopantomograms—a contribution to forensic age estimation methods in adults. Int J Legal Med 119:27–30
Prieto JL, Barberia E, Ortega R, Magana C (2005) Evaluation of chronological age based on third molar development in the Spanish population. Int J Legal Med 119:349–354
Schmeling A, Reisinger W, Loreck D, Vendura K, Markus W, Geserick G (2000) Effects of ethnicity on skeletal maturation—consequences for forensic age estimations. Int J Legal Med 113:253–258
Schmeling A, Kaatsch H-J, Marré B, Reisinger W, Riepert T, Ritz-Timme S, Rösing FW, Rötzscher K, Geserick G (2001) Empfehlungen für die Altersdiagnostik bei Lebenden im Strafverfahren. Rechtsmedizin 11:1–3
Schmeling A, Baumann U, Schmidt S, Wernecke KD, Reisinger W (2006) Reference data for the Thiemann–Nitz method of assessing skeletal age for the purpose of forensic age estimation. Int J Legal Med 120:1–4
Schmeling A, Schulz R, Danner B, Rösing FW (2006) The impact of economic progress and modernization in medicine on the ossification of hand and wrist. Int J Legal Med 120:121–126
Schulz R, Mühler M, Mutze S, Schmidt S, Reisinger W, Schmeling A (2005) Studies on the time frame for ossification of the medial epiphysis of the clavicle revealed by CT scans. Int J Legal Med 119:142–145
Thiemann H-H, Nitz I (1991) Röntgenatlas der normalen Hand im Kindesalter. Thieme, Leipzig
Acknowledgments
The authors wish to thank Dr. Karl Minas for kindly permitting the use of the hand radiographs assessed here.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schmidt, S., Koch, B., Schulz, R. et al. Comparative analysis of the applicability of the skeletal age determination methods of Greulich–Pyle and Thiemann–Nitz for forensic age estimation in living subjects. Int J Legal Med 121, 293–296 (2007). https://doi.org/10.1007/s00414-007-0165-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-007-0165-7