
Abstract
To develop and validate an objective method for calculating the annoyance caused by snoring sounds. 53 subjects assessed 50 different snoring and breath sounds on a visual analog scale for level of annoyance. A linear regression analysis was used to correlate these subjective assessments with objectively calculated psychoacoustic parameters (loudness, roughness, sharpness, and fluctuation strength, calculating the maximum, mean, and 5th percentile in each case). The quality of the resulting formula was checked, and additional validation was performed using subjective assessments of 60 new snoring and breath sounds by 52 new subjects. Receiver operating characteristic (ROC) analysis was used to scale the annoyance ranges obtained with the formula. A score consisting of the 5th percentile of loudness and the mean of roughness was developed. The formula displays high goodness of fit (R 2 = 0.91) and quality. In the validation phase, a highly significant correlation (r s = 0.95; p < 0.01) was obtained between the scores calculated with the formula and the subjective assessments. ROC analysis was able to define the annoyance ranges with a discriminatory power between 52 and 73 % (optimum sensitivity/specificity). The subjective assessments made by the participants were distinctly scaled and were reflected in a psychophysical algorithm. In the setting of polygraphy and polysomnography, this means that a reliable annoyance score that is not dependent on the bed partner can be obtained to establish the indication for anti-snoring treatments and to review their utility.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Snoring is caused by vibrations primarily of the pharyngeal soft tissues during breathing. It is a sign of narrowing and hence of increased resistance of the upper airways during sleep [1–4].
Snoring has consequences for the bed partner. The noise of snoring can lead to sleep disturbances and, consequently, to fatigue, exhaustion, and morning headaches in the bed partner too [5–7]. Links with relationship quality, greater disharmony and higher divorce rates due to snoring have been reported [5, 8, 9]. In the setting of habitual snoring in particular, it is, therefore, often the symptoms experienced by the partner that primarily prompt patients to seek treatment [7].
Objectively measurable parameters are needed to reliably classify the degree of disturbance produced by snoring sounds. Unfortunately, there is to date no generally accepted and, particularly, no validated method, a fact that is attributable not least to the still inadequate definition of the phenomenon of snoring [1, 3].
In noise research, the most commonly studied effect of noise is annoyance. It is regarded as an indicator for negative reactions (including anger, irritation, and stress-related symptoms) in response to unpleasant sounds [10–13]. Annoyance is typically measured subjectively using questionnaires or scales [13, 14]. It has been demonstrated that for the assessment of annoyance—alongside noise patterns over time—it is not only the sound pressure level but also the special acoustic character of the sounds that plays a role [12, 15]. In addition, personal, social, and situation-dependent factors have to be considered [10].
For various types of noise, especially those relating to technology and traffic, reproducible objective methods are now available that provide an approximate measure of the annoyance experienced [16]. However, no validated method yet exists for snoring sounds.
In this study, on the basis of many subjective assessments, a method was, therefore, developed and validated that permits snoring sounds to be categorized objectively in terms of the degree of annoyance they cause. The foundation for this method is provided by parameters from the field of psychoacoustics that objectively reflect the character of sounds (e.g., loudness, roughness or sharpness) [16].
Materials and methods
The study was approved by the local Ethics Committee and was performed in accordance with the ethical standards laid down in the Declaration of Helsinki. All persons gave their informed consent prior to their inclusion in the study.
Study subjects
Snoring sounds and breath sounds of 14 male and 10 female subjects (age 49.1 ± 12.5 years; range 24–73 years) were recorded during sleep. Half of the subjects had obstructive snoring [apnea–hypopnea index (AHI) ≥10], and the other half non-obstructive snoring. The mean AHI for these subjects was 15.7 (±24.8; range 0–128).
In the method development phase, 53 subjects (27 female; age 45.1 ± 15.2 years; range 23–75 years) with normal hearing (self-reported, not tested objectively) assessed 50 snoring sounds and breath sounds. The subjects were selected in such a way that they belonged in almost equal numbers to the following age categories (23–29 years; 30–39 years; 40–49 years; 50–59 years; and 60–75 years) and had a range of experience (none to professional) with snoring sounds.
In the validation phase, 52 other subjects (26 female; age 29.5 ± 6.7 years; range 22–50 years), also with normal hearing, assessed 60 newly selected snoring sounds and breath sounds.
Recording and selection of sounds
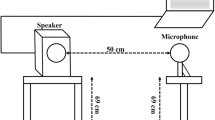
During the course of polygraphy (WatchPat200, Itamar Medical Ltd., Caesarea, Israel) or polysomnography (Alice Sleepware 2.8, Respironics Inc., Murrysville, USA), the sounds were recorded using an audio and acoustic analyzer with a class 1 microphone (XL2 with M2210, NTi Audio AG, Schaan, Liechtenstein). All recordings were made under standardized acoustic conditions (rooms with the same construction and furnishings, identical recording setup, microphone placed precisely 50 cm over the tip of the patient’s nose).
Sequences of two successive snoring sounds or breath sounds in each case that were as acoustically different as possible were selected and trimmed using Adobe Audition 3.0 software (Table 1). Low-frequency interference sounds were filtered out with an FFT filter (high pass, 39 Hz). The recordings were stored in WAV format (Windows PCM) with 48,000 Hz, 32-Bit as mono signals. The mean duration of a sequence was 8.3 s (range 5.2 12.0 s).
Subjective and objective parameters
The subjective (psychometric) assessments of the sound sequences were performed by the subjects under standardized conditions. The sound was reproduced by a speaker with an integrated sound card (nuPro A-20, Nubert electronic, Schwäbisch Gmünd/Germany) positioned 50 cm in front of the subject. The sound pressure level was calibrated, so that it was identical for all subjects. To eliminate disturbing exterior noise, the tests were performed in a soundproof room, which is usually used for audiological examinations (room size 11.5 m2, high 2.5 m; reverberation time <0.1 s). To ensure a comparable degree of alertness among the subjects, the assessments in each case were performed in the afternoon/early evening between 15:00 and 20:00 h.
Software programmed in-house (programming language: Visual Basic) was used for playback. The assessment of sound sequences in terms of their annoyance level was performed on color-, number- and description-coded analog scales (Fig. 1). The subjects were given the option for multiple playback repeats of the sequence being assessed.

Visual analog scale (VAS). The subjects were asked to mark a vertical line on the VAS to indicate in each case the level of annoyance of the sound sequence currently being played back
Objective psychometric parameters of the sound sequences were determined using dBSONIC software, version 4.13 (01 dB-Metravib technologies, Limonest cedex/France). In each case, these were the maximum (X max), mean (X mean), and 5th percentile (X 5) of loudness N (sone), roughness R (asper), sharpness S (acum), and fluctuation strength F (vacil).
Developing and validating the score
Statistical analysis, regression analysis, and graph plotting were performed using Microsoft Excel 2008 software for the Mac (Microsoft Corporation) und SPSS Statistics 21.0 software (IBM Corporation, Armonk/USA).
The subjective annoyance of the snoring sounds was to be modeled as accurately as possible in a formula using objective psychoacoustic parameters. The multiple linear regression method was used to derive the formula. For this purpose, scatter diagrams were prepared for the subjective annoyance associated with the individual psychoacoustic parameters. In the event of a logarithmic relationship, the psychoacoustic values were logarithmized, so that the linear regression method could be used.
For the regression analysis, all the psychoacoustic parameters in succession were correlated with the subjective assessments of annoyance. This process started with the parameter with the strongest correlation, and then, the other parameters were tested in sequence for significant additional explanatory value. If this was found, then the parameter was included in the regression equation, although each parameter was permitted to feature in the equation in only one form (maximum, mean or 5th percentile). The coefficient of determination R 2 was calculated to assess the goodness of fit of the regression model in each case.
The resulting formula was tested for quality using various methods: between-variable correlation (collinearity analysis; rejection range where tolerance <0.25 and variance inflation factor >5), heteroscedasticity, and possible auto-correlation of the function per se (rejection range for values <1.63 or >2.37 according to Durbin–Watson where N = 50, k = 2 and α = 0.05 with D LOW = 1.46 and D UPPER = 1.63 [17]).
Validation of the regression equation was performed using the psychometric results from the second group of subjects (Spearman’s rank correlation).
On the basis of the psychometric results for all subjects (method development and validation groups), various value ranges from the resulting formula were assigned to the five annoyance categories (from ‘not annoying’ to ‘extremely annoying’). Receiver operating characteristic (ROC) analysis was used for this purpose.
Results
Method development phase
All psychoacoustic values except the sharpness showed a logarithmic behavior; therefore, they were logarithmized. Regression analysis revealed the highest coefficient of determination for N 5 (R 2 = 0.87). The result was further improved by the additional inclusion of R mean as a second parameter (R 2 = 0.91). A third parameter did not bring any further gain (Table 2). This, therefore, yielded the following formula, which we have called the Psychoacoustic Snore Score (PSS):
In view of the logarithmic elements, the PSS was defined as 0 where N 5 < 1 or R mean < 1.
Collinearity analysis revealed a tolerance of 0.33 and a variance inflation factor of 3.0 for this formula. In addition, the residuals did not produce any heteroscedasticity (p = 0.7). The Durbin–Watson test statistic for autocorrelation was 1.7.
Validation phase
A very good and highly significant correlation (r s = 0.95, p < 0.01) was found when the PSS was compared with the subjective assessments of the validation group (Fig. 2).

Validation phase, scatter diagram. The subjective assessments displayed a highly significant (p < 0.01) very good correlation (r s = 0.95) with the objectively determined results on the Psychoacoustic Snore Score
Scaling
On the basis of the subjective assessments of the method development and validation groups, ROC analysis was used to determine value ranges for the annoyance categories on the PSS (Table 3). Optimum sensitivity and specificity in each case were between 0.70 and 0.73; these fell to 0.52 only in the categories ‘annoying’ and ‘extremely annoying’. To facilitate classification in clinical practice, the cutoffs were rounded to the nearest 5 or 10 (<40; 40–59.9; 60–74.9; 75–89.9; ≥90) (Fig. 3). This rounding of the cutoffs produced only discrete changes in sensitivity and specificity in each case (Table 3).

PSS score ranges. The scale shows the annoyance categories with the relevant score ranges on the Psychoacoustic Snore Score (PSS), together with the corresponding rounded score range for routine clinical use in each case
Discussion
To the best of our knowledge, the Psychoacoustic Snore Score (PSS) is the first instrument that can be used to calculate the perceived annoyance of snoring sounds in an objective and validated manner, independently of the bed partner.
The PSS is designed to address a typical problem associated with the assessment of the acoustic phenomenon of snoring: namely, the contradiction that often exists between subjective assessments (e.g., supplied by the bed partner) and the results of objective methods [9, 18–22]. The latter typically reflects the volume and duration of snoring. However, results from different sleep laboratories or polygraph devices permit only an inadequate degree of comparison, because the measurement methods used sometimes differ markedly. While the sound pressure level is used in most cases as the sole parameter or as the basis for a snoring index, the cutoffs to differentiate snoring sounds from breath sounds range from 40 up to 76 dB in some instances [2, 4, 6, 18, 22–24]. The continuing lack of a generally recognized acoustic definition of snoring is certainly the main reason for this problem of poor standardization [2, 3].
Various studies have shown that a simple measurement of the sound pressure level is inadequate to assess the annoyance level of sounds and that psychoacoustic parameters are in some cases definitely superior [16, 25, 26].
The PSS does not register volume or snoring per se. Instead, it reflects the annoyance of the sound produced by the sleeper and thus provides objective evidence of the level of nuisance to the bed partner.
During the PSS development phase, regression analysis showed that the 5th percentile of loudness (5 % of the sound is louder, 95 % quieter) is the most relevant parameter to reflect the subjective level of annoyance. This is in agreement with Zwicker et al., who also found this value to be most relevant in noise measurements [16]. A further study has also shown that the 5th percentile of loudness in snoring sounds correlates best with subjective annoyance [27].
Mean roughness showed the second-best correlation with subjective annoyance. In another study involving primarily obstructive snoring sounds [27], fluctuation strength was identified as a key parameter, but in this study, this played only a subordinate role. Seen against the background of the data presented by Herzog et al. [28, 29], this can also be interpreted as evidence that alternative parameters may have to be considered for purely obstructive snoring. Both parameters are influenced by temporal variations in frequency, but in different frequency ranges [16, 27, 30]. Herzog et al. were able to show that roughness is clearly more pronounced in primary—especially velar—snoring, whereas fluctuation strength is most pronounced in post-apnoeic snoring [28, 29]. In this study, our concern was to develop a method that was as generally valid as possible for a balanced ratio of obstructive and primary snoring sounds.
Additional inclusion of a third parameter did not yield any improvement in the formula. Any improvement was also hardly to be expected, because the two parameters N 5 and R mean had already yielded a coefficient of determination of R 2 = 0.91 and, hence, a correlation of r = 0.95. This is an extremely good result, particularly since we are describing a subjective impression. Both values used have positive coefficients on the PSS, i.e., the greater the loudness and the greater the roughness of the snoring sounds, the more annoying they are.
The quality of the PSS has been demonstrated using mathematical methods. First, there is an absence of heteroscedasticity. This means that the residuals that are always present in a regression model display constant variance. Therefore, there is no trend that deviates from the regression equation that might skew the results. Second, there is no autocorrelation in the Durbin–Watson test [17]. This means that a possible deviation from the calculated formula is independent of previous residuals and, consequently, distortion of results, and hence, an inaccurate assessment can be virtually ruled out. Collinearity analysis also confirmed the quality of the formula: the two parameters N 5 and R mean do not correlate to a significant extent, and therefore, both make an autonomous, independent contribution to the result.
The PSS is not the first formula designed to reflect the annoyance caused by snoring. For example, Caffier et al. published details of the Berlin Snore Score in 2007 [31]. This also presents a formula to calculate the acoustic annoyance of snoring sounds, consisting of various levels to describe noise exposure and noise character in combination with a time factor.
However, this and other methods lack adequate validation [2, 3, 32]. To the best of our knowledge, the PSS is the first formula that has been based on subjective assessments and has been validated using further subjective data. As previously during the method development phase, but using completely new subjects and sounds under the same temporal and spatial conditions, the correlation found between the calculated objective results and the subjective assessments was 95 %. This confirms the powerful validity of the PSS.
The objective of the PSS is not to reflect precisely the annoyance experienced by each individual. Admittedly, it has been shown that a high degree of reproducibility is found in the assessment of snoring sounds and that there are no gender-, age- or experience-related differences [25]. However, it is known from noise research that sound level is not the only factor of relevance for the feeling of annoyance [10, 12, 13, 33–35]. Other important aspects include personal sensitivity to noise and attitude to noise. Relationship quality with the bed partner and possible pressure to get enough sleep (e.g., due to the work situation) should also be considered [36].
The PSS is intended to provide the therapist with an impression that is as generally valid as possible of the annoyance of the sounds produced by the sleeper. In terms of subject, selection care was, therefore, taken to ensure a balanced distribution in terms of age, gender, and snoring-related experience. The assessments were always conducted at approximately the same time of day, because annoyance assessments are dependent on time of day [2, 16, 37]. Because such formulae are also always dependent on the sounds selected [26], care was further taken to ensure a balanced distribution of obstructive and non-obstructive sounds. Breath sounds were also integrated. This was done first, because snoring cannot be distinguished unequivocally from breath sounds [38], and second, because louder breath sounds can also be annoying. Maximum sound pressure levels as low as 33 dB have been shown to induce physiological reactions during sleep, e.g., changes in heart rate, body movements or regaining of waking consciousness [12, 15].
Annoyance ranges for the PSS were defined using an ROC analysis (Table 3). The annoyance categories were clearly differentiated from each other with a sensitivity and specificity of approximately 70 %. Differences between subjects were detected more often only when deciding whether a sound was ‘annoying’ or ‘extremely annoying’. This is reflected in the fact that discrimination between these two categories was lower, with a sensitivity and specificity of 52 %. To facilitate classification in routine clinical practice, the cutoffs were rounded up or down (Fig. 3), resulting in only a slight loss of discriminatory power.
When using the PSS, it should be remembered that, while it provides an objective assessment of the annoyance caused by snoring sounds, it does not yield any information about resulting problems with falling asleep or waking reactions experienced by the bed partner. As with other measuring instruments in current use, supplementary information on these aspects will still have to be elicited from the bed partner [37].
Although the PSS is based on a solid foundation of subjective assessments, the number of subjects and sounds included was naturally limited. The validity of the score will have to be demonstrated in routine clinical use in large numbers of patients.
The intention is for use of the PSS to be integrated into sleep laboratories and polygraphy studies. As an objective validated instrument, it should provide effective help in establishing the indication for and reviewing the utility of anti-snoring treatments. Here, it is important to bear in mind the usual shortcomings of current measurement and recording techniques: contact microphones produce marked acoustic changes and are not to be recommended [39]. A different microphone distance alters the sound pressure level in a predictable manner [40], and therefore, a correction factor must be incorporated, depending on the distance. The patient’s body position also influences the result. If the patient moves out of the supine position, the sound pressure level changes by 3–5 dB [32, 41, 42]. In terms of scale and in the context of a longer recording period, however, such variations are probably negligible.
Conclusion
The Psychoacoustic Snore Score uses a psychophysical algorithm to reflect the subjective assessments of the participants. The annoyance caused by snoring sounds can thus be calculated objectively. In the setting of polygraphy and polysomnography, this means that a reliable annoyance score that is not dependent on the bed partner can be obtained to establish the indication for anti-snoring treatments and to review their utility.
References
Stuck BA, Dreher A, Heiser C, Herzog M, Kühnel T, Maurer JT, Pistner H, Sitter H, Steffen A, Verse T (2015) Diagnosis and treatment of snoring in adults-S2k Guideline of the German Society of Otorhinolaryngology, Head and Neck Surgery. Sleep Breath 19:135–148
Pevernagie D, Aarts RM, de Meyer M (2010) The acoustics of snoring. Sleep Med Rev 14:131–144
Hoffstein V (1996) Snoring. Chest 109:201–222
Beck R, Odeh M, Oliven A, Gavriely N (1995) The acoustic properties of snores. Eur Respir J 8:2120–2128
Ulfberg J, Carter N, Talbäck M, Edling C (2000) Adverse health effects among women living with heavy snorers. Health Care Women Int 21:81–90
Blumen MB, Quera Salva MA, Vaugier I, Leroux K, d’Ortho M, Barbot F, Chabolle F, Lofaso F (2012) Is snoring intensity responsible for the sleep partner’s poor quality of sleep? Sleep Breath 16:903–907
McArdle N, Kingshott R, Engleman HM, Mackay TW, Douglas NJ (2001) Partners of patients with sleep apnoea/hypopnoea syndrome: effect of CPAP treatment on sleep quality and quality of life. Thorax 56:513–518
Troxel WM, Buysse DJ, Hall M, Matthews KA (2009) Marital happiness and sleep disturbances in a multi-ethnic sample of middle-aged women. Behav Sleep Med 7:2–19
Virkkula P, Bachour A, Hytönen M, Malmberg H, Salmi T, Maasilta P (2005) Patient- and bed partner-reported symptoms, smoking, and nasal resistance in sleep-disordered breathing. Chest 128:2176–2182
Laszlo HE, McRobie ES, Stansfeld SA, Hansell AL (2012) Annoyance and other reaction measures to changes in noise exposure—a review. Sci Total Environ 435–436:551–562
van Kempen E, van Kamp I, Nilsson M, Lammers J, Emmen H, Clark C, Stansfeld S (2010) The role of annoyance in the relation between transportation noise and children’s health and cognition. J Acoust Soc Am 128:2817–2828
Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, Stansfeld S (2014) Auditory and non-auditory effects of noise on health. Lancet 383:1325–1332
Lekaviciute J, Argalasova-Sobotova L (2013) Environmental noise and annoyance in adults: research in Central, Eastern and South-Eastern Europe and Newly Independent States. Noise Health 15:42–54
Kasess CH, Noll A, Majdak P, Waubke H (2013) Effect of train type on annoyance and acoustic features of the rolling noise. J Acoust Soc Am 134:1071–1081
Münzel T, Gori T, Babisch W, Basner M (2014) Cardiovascular effects of environmental noise exposure. Eur Heart J 35:829–836
Fastl H, Zwicker E (2007) Psychoacoustics: facts and models. Springer, Berlin
Durbin J, Watson GS (1951) Testing for serial correlation in least squares regression. Biometrika 38:159–177
Hoffstein V, Mateika S, Anderson D (1994) Snoring: is it in the ear of the beholder? Sleep 17:522–526
Hoffstein V (2007) Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 11:1–22
Wiggins CL, Schmidt-Nowara WW, Coultas DB, Samet JM (1990) Comparison of self- and spouse reports of snoring and other symptoms associated with sleep apnea syndrome. Sleep 13:245–252
Counter P, Wilson JA (2004) The management of simple snoring. Sleep Med Rev 8:433–441
Miljeteig H, Mateika S, Haight JS, Cole P, Hoffstein V (1994) Subjective and objective assessment of uvulopalatopharyngoplasty for treatment of snoring and obstructive sleep apnea. Am J Respir Crit Care Med 150:1286–1290
Sériès F, Marc I, Atton L (1993) Comparison of snoring measured at home and during polysomnographic studies. Chest 103:1769–1773
Dalmasso F, Prota R (1996) Snoring: analysis, measurement, clinical implications and applications. Eur Respir J 9:146–159
Rohrmeier C, Fischer R, Merz A, Ettl T, Herzog M, Kuehnel TS (2015) Are subjective assessments of snoring sounds reliable? Eur Arch Otorhinolaryngol 272:233–240
Ellermeier W, Mader M, Daniel P (2004) Scaling the unpleasantness of sounds according to the BTL model: ratio-scale representation and psychoacoustical analysis. Acta Acust United Acust 90:101–107
Rohrmeier C, Herzog M, Haubner F, Kuehnel TS (2012) The annoyance of snoring and psychoacoustic parameters: a step towards an objective measurement. Eur Arch Otorhinolaryngol 269:1537–1543
Herzog M, Bremert T, Herzog B, Hosemann W, Kaftan H, Müller A (2011) Analysis of snoring sound by psychoacoustic parameters. Eur Arch Otorhinolaryngol 268:1386–1389
Herzog M, Kellner P, Plößl S, Glien A, Rohrmeier C, Kühnel T, Plontke S, Herzog B (2015) Drug-induced sleep endoscopy and simulated snoring in patients with sleep-disordered breathing: agreement of anatomic changes in the upper airway. Eur Arch Otorhinolaryngol 272:2541–2550
Ng AK, Koh TS, Baey E, Puvanendran K (2009) Role of upper airway dimensions in snore production: acoustical and perceptual findings. Ann Biomed Eng 37:1807–1817
Caffier PP, Berl JC, Muggli A, Reinhardt A, Jakob A, Möser M, Fietze I, Scherer H, Hölzl M (2007) Snoring noise pollution—the need for objective quantification of annoyance, regulatory guidelines and mandatory therapy for snoring. Physiol Meas 28:25–40
Wilson K, Stoohs RA, Mulrooney TF, Johnson LJ, Guilleminault C, Huang Z (1999) The snoring spectrum: acoustic assessment of snoring sound intensity in 1,139 individuals undergoing polysomnography. Chest 115:762–770
Ising H, Kruppa B (2004) Health effects caused by noise: evidence in the literature from the past 25 years. Noise Health 6:5–13
Menzel D, Fastl H, Graf R, Hellbrück J (2008) Influence of vehicle color on loudness judgments. J Acoust Soc Am 123:2477–2479
Ellermeier W, Eigenstetter M, Zimmer K (2001) Psychoacoustic correlates of individual noise sensitivity. J Acoust Soc Am 109:1464–1473
Kühnel T, Glas S, Herzog M, Gassner H, Rohrmeier C (2014) Psychosocial burden caused by snoring. Somnologie 18:80–86
Hoeger R, Schreckenberg D, Felscher-Suhr U, Griefahn B (2002) Night-time noise annoyance: state of the art. Noise Health 4:19–25
Rohrmeier C, Herzog M, Ettl T, Kuehnel TS (2014) Distinguishing snoring sounds from breath sounds: a straightforward matter? Sleep Breath 18:169–176
Herzog M, Kühnel T, Bremert T, Herzog B, Hosemann W, Kaftan H (2009) The impact of the microphone position on the frequency analysis of snoring sounds. Eur Arch Otorhinolaryngol 266:1315–1322
Abeyratne UR, Wakwella AS, Hukins C (2005) Pitch jump probability measures for the analysis of snoring sounds in apnea. Physiol Meas 26:779–798
Azarbarzin A, Moussavi Z (2013) Intra-subject variability of snoring sounds in relation to body position, sleep stage, and blood oxygen level. Med Biol Eng Comput 51:429–439
Lee BW, Hill PD, Osborne J, Osman E (1999) A simple audio data logger for objective assessment of snoring in the home. Physiol Meas 20:119–127
Acknowledgments
We are grateful to Eric Siegel for programming the software for sound sequence playback and to the many subjects who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure statement
There are no institutional or corporate affiliations of the authors and there are no funding sources which supported the work.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Fischer, R., Kuehnel, T.S., Merz, AK. et al. Calculating annoyance: an option to proof efficacy in ENT treatment of snoring?. Eur Arch Otorhinolaryngol 273, 4607–4613 (2016). https://doi.org/10.1007/s00405-016-4160-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-016-4160-9