
Abstract
Drug-induced sleep endoscopy (DISE) and simulated snoring (SimS) are performed as part of the diagnostic procedure in patients with suspected sleep-disordered breathing (SDB). Despite both techniques frequently performed, they have rarely been evaluated yet in terms of agreement of the obtained results. Both diagnostic procedures were performed consecutively in 40 patients with SDB and documented identically. The obtained data were analysed with respect to the agreement of both procedure at different levels of the oropharynx as well as different patterns of obstruction and vibration. The anterior–posterior collapsibility of the soft palate/uvula revealed a moderate agreement between SimS and DISE (κ = 0.42; 95 % CI 0.22–0.63). The dorsal shift of the tongue base agreed moderate for patients with an AHI below 10 (κ = 0.47) and above 25 (κ = 0.44) between SimS ad DISE. The lateral and circular pharyngeal collapsibility at velum and tongue base level did not agree between SimS and DISE, was higher for DISE and could be partially reversed by mandibular protrusion. Collapse patterns of the soft palate and uvula can be induced by SimS and resemble the patterns induced by DISE. The dorsalization of the tongue base can be simulated to a lower extent by SimS. Lateral and circular patterns of collapse at the upper and lower oropharynx induced by DISE do not seem to be simulated by SimS. SimS seems to be an additional method to screen the collapsibility of the soft palate and uvula prior to DISE.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Drug-induced sleep endoscopy (DISE) and simulated snoring (SimS) are performed as part of the diagnostic procedure on a routine base in patients with sleep-disordered breathing (SDB). Both methods aim to identify structures of the upper airway which are suspected to cause snoring and/or obstructions related to night-time respiratory events.
A standardised procedure for SimS has been proposed on base of examinations of 622 patients with SDB [1]. A correlation between the collapsibility of the oropharynx at tongue base level and the apnea–hypopnea index (AHI) was observed. The advantages of SimS are the non-invasiveness, the performance under wake conditions, low logistical efforts and the lack of side effects. As a major disadvantage of SimS, it needs to be kept in mind that the anatomical situation might differ from wake to sleep.
Contrary to SimS under wake conditions, vibrations and collapsibility of the upper airway can also be investigated by DISE. This procedure intends to examine the upper airway under sleep-like conditions [2, 3]. Several authors reported modifications of the technique in terms of applied drugs, documentary standards and/or correlations to nocturnal respiratory events [4–10]. At present, DISE is frequently performed as part of the diagnostic procedure in patients with SDB. There are reported similarities in the patterns of vibration and/or obstructions between drug-induced sleep and natural sleep. Sedation and its associated side effects and logistic efforts are mentioned as major disadvantages.
The aim of the study was to perform SimS and DISE in the same patients to detect similarities and differences in patterns of vibration and obstruction of both procedures.
Methods
Patient acquisition
This prospective observational study was carried out between the Department of Otorhinolaryngology, Head and Neck Surgery and the Department of Anaesthesiology at Halle University Hospital, Martin-Luther-University, Germany. Forty-three consecutive patients with suspected SDB who were referred to the authors’ sleep outpatient clinic participated in the study. The investigation by DISE and SimS was part of the regular diagnostic procedure in patients with SDB and was performed by the first author (M.H.). No additional invasive procedures were performed. As exclusion criteria, the disability of undergoing general anaesthesia and the disability to simulate snoring were defined.
Polygraphy
Ambulant polygraphy (PG) was performed prior to the study (Sleep Doc Porti6®, Dr. Fenyves und Gut, Hechingen, Germany). The AHI was calculated by computer-assisted analysis according to the update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events [11]. An AHI was available for 25 patients.
Simulated snoring
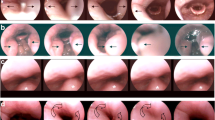
SimS was performed prior to DISE in the operation room in a supine position. The procedure was described in detail previously [12]. Briefly, the patients were examined under wake conditions in a supine position by flexible nasal endoscopy. SimS was induced by forced inspiration through the opened mouth. The alteration of a particular structure of the upper airway by SimS was documented (Fig. 1). The classification focuses on the cranial oropharynx at velum level with respect to the pattern of vibration (Fig. 1a lateral and circular collapse; Fig. 1b anterior–posterior collapse) as well as on the caudal oropharynx at tongue base level which is classified the same way (Fig. 1c anterior–posterior collapse; Fig. 1d lateral and circular collapse).

Classification of the vibration and collapsibility of the upper airway during SimS and DISE. a The pharyngeal collapse at velum level is graded 1–5 with respect to a lateral or circular pattern of collapsibility. b The contact of the uvula/soft palate to the posterior pharyngeal wall is classified 1–4 according to its anterior–posterior pattern of vibration. c The dorsal movement of the tongue base is classified depending on the visibility of the valleculae and contact to the posterior pharyngeal wall focusing on an anterior–posterior pattern of movement. d The pharyngeal collapse at tongue base level is graded 1–5 depending on a lateral and circular pattern of collapsibility
Drug-induced sleep endoscopy
After the successful performance of SimS, the patient was examined by DISE. The sedation was induced by bolus application of disoprivan (Propofol®-Lipuro 10 mg/mL; B.Braun Melsungen AG, Melsungen, Germany). The alterations of the upper airway were documented using the identical grading system as for SimS (Fig. 1). DISE was terminated when either complete obstructions of the pharynx with apneas occurred or central respiratory depression led to a decrease in SAO2 which was not tolerable in case of non-occurrence of obstructive apneas. At termination of DISE, a manoeuvre of mandibular protrusion was performed and graded identically.
Statistical analysis
Statistical analyses were conducted by SAS 9.3 (SAS Institute Inc., Cary, NC, USA). For the agreements between SimS and DISE parameters, the weighted Cohen’s Kappas were calculated. The analyses of the acoustic frequencies were performed by Wilcoxon test. The applied statistical tests are given at the specific paragraph of the results.
Results
Patients’ base line data
Of initially 43 patients, three patients were excluded from the study as they were not able to simulate snoring. Forty patients (31 male, 9 female) were included. The mean age was 45 years (min 26, max 53, SD 9.3). The mean body mass index was 27.8 (min 20.4, max 40.8, SD 4.2). A mean AHI of 20.7 was calculated (min 0, max 98, SD 23.3). The mean nocturnal blood oxygen saturation was 92.5 % (min 77, max 96, SD 3.3). The minimal nocturnal blood oxygen saturation was 71.7 % in mean (min 43, max 92, SD 10.6). The patients were divided into three subgroups according to the severity of SDB (AHI <10, n = 9, 10 ≤ AHI < 25, n = 11; 25≤ AHI, n = 5).
Descriptive analyses of patterns of obstruction and vibration under SimS and DISE
Lateral and circular pharyngeal collapse at velum level
Under SimS, approximately one-third of the patients did not reveal a lateral or circular collapse at velum level. Approximately half of the patients showed a light lateral collapse. Only a few patients could simulate a strong lateral or circular collapse. Under DISE, most patients revealed a strong lateral or circular collapse which is indicated by a shift of the histogram bars to the right. Mandibular protrusion was able to antagonise the collapse to some extent. The collapsibility shifted to a light lateral or circular collapse (Fig. 2a).

Grading of the collapsibility in anterior–posterior, lateral and circular direction under simulated snoring (SimS) and drug-induced sleep endoscopy (DISE) without and with mandibular protrusion. a The pharyngeal collapsibility at velum level increases under DISE and reverses partially under mandibular protrusion which is visualised by a shift of the bars towards higher grades under DISE and a backshift when a mandibular protrusion is performed. b The pattern of vibration at anterior–posterior direction at velum level reveals only a slight shift towards higher grades between SimS and DISE and under mandibular protrusion. c The pattern of movement at anterior–posterior direction of the tongue base reveals a slight shift towards higher grades between SimS and DISE. A shift towards lower grades under mandibular protrusion is present. d The pharyngeal collapsibility at tongue base level increases under DISE and reverses partially under mandibular protrusion which is visualised by a shift of the bars towards higher grades under DISE and lower grades under mandibular protrusion
Anterior–posterior vibration of the uvula/soft palate
The vibration at anterior–posterior direction could be simulated at all degrees under SimS. The uvula/soft palate revealed an almost equal distribution for all grades under DISE which did not differ from simulated vibration. Mandibular protrusion was able to reverse the vibration to some extent which is indicated by a shift to the left of the histogram bars (Fig. 2b).
Dorsal movement of the tongue base
The dorsal movement of the tongue base could be simulated from grade 1 to 3. None of the individuals was able to simulate a complete obstruction under SimS. Contrary to those results, the dorsal movement of the tongue base shifted to a higher grade under DISE and reversed by one grade under mandibular protrusion (Fig. 2c).
Lateral and circular pharyngeal collapse at tongue base level
The pharyngeal collapsibility at tongue base level under SimS revealed low grades (grade 1 and 2) for more the two-thirds of the patients. Contrary to that, a lateral and circular collapse occurred under DISE to various degrees. A partial reversion was observed under mandibular protrusion (Fig. 2d).
Agreement of patterns of obstruction and vibration under SimS and DISE
The agreement of the grading between SimS and DISE is given as weighted Cohen’s Kappa for all individuals (independent) as well as with respect to the severity of SDB AHI <10, 10 ≤ AHI < 25, AHI ≥25). The value of Cohen’s Kappa can reach 1 at a perfect agreement between SimS and DISE. Levels below 0.25 are interpreted to have no agreement. Values between 0.25 and 0.75 indicate a moderate agreement. Values above 0.75 indicate a high agreement.
Lateral and circular pharyngeal collapse at velum level
For all individuals, there is no agreement between the pharyngeal collapsibility at velum level between SimS and DISE. The weighted Cohen’s Kappa is 0.18 (95 % CI 0.05–0.31) indicating no agreement between SimS and DISE. With respect to the severity of SDB at an AHI <10, no agreement (weighted Cohen’s Kappa 0.09) and at 10 ≤ AHI < 25 (weighted Cohen’s Kappa 0.14) is present. At AHI values above 25, a moderate agreement between SimS and DISE could be detected (weighted Cohen’s Kappa 0.57). At an independent AHI, patients graded as I° during SimS revealed a higher grading during DISE in 84.6 %. Grade II° during SimS was graded higher during DISE in 72.2 % (Tables 1A, 2; Fig. 3a).

Agreement between grading values under simulated snoring (SimS) and drug-induced sleep endoscopy (DISE) independent from the AHI. High agreement is present when the single square areas are located along the diagonal line. A shift away from the diagonal line indicates a lower agreement. Exact agreement is marked by a dark blue area, partial agreement by a light blue area. a Lateral and circular collapsibility at velum level. The agreement between SimS and DISE for all individuals is low which is demonstrated by a shift of the boxes of agreement away from the diagonal line to the lower right corner of the diagram. b Anterior–posterior collapsibility of the uvula and soft palate. The agreement between SimS and DISE is moderate to high which is demonstrated by a distribution of the boxes of agreement along the diagonal line in the diagram. c Dorsal movement of the tongue base. The agreement between SimS and DISE is moderate to low which is demonstrated by a distribution of the boxes of agreement along the diagonal line in the diagram but a shift to the lower right corner. d Lateral and circular collapsibility at tongue base level. The agreement between SimS and DISE is low to moderate which is demonstrated by a shift of the boxes of agreement away from the diagonal line to the lower right corner of the diagram for grades 2–4
Anterior–posterior vibration of the uvula/soft palate
The grading revealed a moderate agreement between SimS and DISE for the contact of the uvula/palate to the posterior pharyngeal wall independent from the AHI (weighted Cohen’s Kappa 0.42; 95 % CI 0.22–0.63). With respect to the severity of SDB at an AHI <10 a moderate agreement (weighted Cohen’s Kappa 0.62) and at 10 ≤ AHI < 25 (weighted Cohen’s Kappa 0.27) is present. At AHI values above 25, a high agreement between SimS and DISE is present (weighted Cohen’s Kappa 0.80). Grade 2 agreed in 38.5 %, grade 3 in 35.7 % and grade 4 in 72.7 % (Tables 1B, 2; Fig. 3b).
Dorsal movement of the tongue base
Moderate agreement between SimS and DISE for the dorsal movement of the tongue base independent from the AHI (weighted Cohen’s Kappa 0.26; 95 % CI 0.11–0.41). With respect to the severity of SDB at an AHI <10, a moderate agreement (weighted Cohen’s Kappa 0.47) is detected. At 10 ≤ AHI < 25 (weighted Cohen’s Kappa 0.18), no agreement is present. At AHI values above 25, a moderate agreement between SimS and DISE is present (weighted Cohen’s Kappa 0.44). Grade 2 and 3 agreed in 50 % of the patients between SimS and DISE (Table 1C, 2; Fig. 3c).
Lateral and circular pharyngeal collapse at tongue base level
Independent from the AHI, a moderate agreement between SimS and DISE is present (weighted Cohen’s Kappa 0.26; 95 % CI 0.11–0.41). With respect to the severity of SDB at an AHI <10, a moderate agreement (weighted Cohen’s Kappa 0.38) is detected. At 10 ≤ AHI < 25 (weighted Cohen’s Kappa 0.22) and at AHI values above 25 (weighted Cohen’s Kappa 0.22), no agreement is present. For all individuals, an agreement of 39.1 % between SimS and DISE was present at grade 1. At higher grades, a shift towards a higher grading during DISE could be detected. 82.5 % of the patients were grade 1 or 2 during SimS, whereas higher grades were only detected in 17.5 % of the patients under wake conditions. (Tables 1D, 2; Fig. 3d).
Discussion
SimS and DISE are common diagnostic methods in patients with SDB. At present, only few comparative data are available for both procedures. The aim of the study was to compare the patterns of vibration and collapse of the upper airway during SimS and DISE.
The data of the presented study reveal different grading levels between SimS and DISE in terms of lower grading for SimS concerning a lateral or circular pharyngeal collapse pattern at velum and tongue base level. Contrary to that, a collapse pattern in anterior–posterior direction at velum and tongue base level revealed a more similar grading for SimS and DISE. Moreover, there is evidence that the agreement between patterns during SimS and DISE is partially influenced by the severity of SDB which is confirmed by similar levels of agreement for all individuals and the subgroups with low, moderate or high AHI.
The optimal method of investigating patterns of obstruction would be an examination in vivo by natural sleep endoscopy. This aim is still out of reach at the moment due to logistical and personal efforts. Drug-induced sleep endoscopy is propagated as an appropriate alternative tool to locate the locus of vibration and/or obstruction in the upper airway. It is assumed that the patterns of obstructions are similar to natural nocturnal patterns. DISE is considered a high validity. Modifications in the therapeutic surgical concept result from DISE when the obtained findings differ from findings of the clinical examination awake [13, 14]. Keeping in mind that DISE requires certain logistical efforts and might cause discomfort and side effects, an easy and safe alternative to DISE would be desirable.
The clinical examination of the upper airway is part of the standard diagnostic procedure in snoring and obstructive sleep apnea. A recent publication reports a positive correlation between Friedman staging and the oropharyngeal collapsibility, whereas other static clinical examinations reveal only poor or no correlation to findings under DISE [15]. Apart from that, the modified Mallampati score does not reveal a predictive value for an obstruction at tongue base level under DISE [5].
Contrary to static clinical examinations, semi-dynamic method, such as Müller manoeuvre and SimS under awake conditions, seems to reveal a higher agreement to DISE. The Müller manoeuvre revealed similar patterns of obstruction as DISE at the levels of the soft palate and tongue base [16]. Interestingly, the same study reports discrepancies between both methods for the laryngeal level. Contrary to these data, the oropharyngeal site revealed an increased collapsibility during DISE in 27 % of the examined patients compared to the Müller manoeuvre. With respect to the hypopharyngeal site, 51 % of the individuals revealed a higher collapsibility under DISE [17]. The authors report a shift of obstruction patterns from lateral under awake condition towards circular or anterior–posterior patterns under DISE. Apart from the Müller manoeuvre, SimS has been reported to serve as an alternative non-invasive way to examine the upper airway under semi-dynamic conditions [1, 12]. A diagnostic agreement between SimS and Müller manoeuvre was stated for retroglossal obstruction [18]. On base of the cited results above, the data of the present study need to be interpreted more in detail with regard to different levels and patterns of obstruction.
The levels and patterns of obstruction which are classified in the present study are shown in Fig. 1. The levels of the soft palate/uvula and the tongue base were classified according to obstruction in an anterior–posterior direction. The upper oropharynx at velar level and the lower oropharynx at tongue base level were classified by lateral or circular collapsibility.
The present data reveal an increased grade of collapsibility of the upper airway during DISE compared to SimS as reported previously [17]. Interestingly, a lateral or circular collapse was more prominent during DISE. In other words, a lateral or circular collapse seems difficult to simulate under wake conditions. Contrary to that, vibrations in an anterior–posterior direction seem more likely to be simulated under wake conditions than other patterns. Especially at velum level, an anterior–posterior vibration can be simulated awake. But also at tongue base level, the movement of the tongue from anterior to posterior can be simulated awake in patients with an AHI below 10 or above 25.
Concluding that anterior–posterior vibrations and movements can be visualised by SimS, a potential targeted therapy such as palate surgery or mandibular advancement devices can be discussed with the patients at the beginning of a further topodiagnosis by DISE. Of course, additional patterns of collapse seem not observable as easy as anterior–posterior ones. The pattern of collapse can shift from anterior–posterior to lateral or circular which might lead to a change in the surgical treatment plan as reported by other studies [13, 14]. Therefore, DISE still remains the standard diagnostic procedure for the topodiagnostic evaluation of vibrations and obstructions.
Conclusion
SimS serves as a semi-dynamic method of investigating the collapsibility of the upper airway in snoring patients. Taking the results of the presented study into account, it can be stated that an agreement between SimS and DISE is present for an anterior–posterior pattern of vibration at the soft palate and uvula and to a smaller extent at the tongue base. The lateral and circular collapsibility of the upper oropharynx at velum level and lower oropharynx at tongue base level seems difficult to be simulated under wake conditions. Lack of side effects, low logistical efforts and the performance under wake conditions remain advantages of SimS. Nevertheless, DISE remains the method of choice for the topodiagnosis of the site of obstruction. Both procedures should not be considered as competing diagnostic methods but SimS might serve as an initial screening method to obtain an overview about possible patterns of collapse. Surgical options of soft palate surgery could be discussed with the patient on base of the results of SimS in advance of DISE.
References
Herzog M, Kuhnel T, Bremert T, Herzog B, Hosemann W, Kaftan H (2009) The upper airway in sleep-disordered breathing: a clinical prediction model. Laryngoscope 119(4):765–773. doi:10.1002/lary.20153
Croft CB, Pringle M (1991) Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci 16(5):504–509
Pringle MB, Croft CB (1993) A grading system for patients with obstructive sleep apnoea—based on sleep nasendoscopy. Clin Otolaryngol Allied Sci 18(6):480–484
Babar-Craig H, Rajani NK, Bailey P, Kotecha BT (2012) Validation of sleep nasendoscopy for assessment of snoring with bispectral index monitoring. Eur Arch Otorhinolaryngol 269(4):1277–1279. doi:10.1007/s00405-011-1798-1
den Herder C, van Tinteren H, de Vries N (2005) Sleep endoscopy versus modified Mallampati score in sleep apnea and snoring. Laryngoscope 115(4):735–739. doi:10.1097/01.mlg.0000161347.07881.6d
El Badawey MR, McKee G, Heggie N, Marshall H, Wilson JA (2003) Predictive value of sleep nasendoscopy in the management of habitual snorers. Ann Otol Rhinol Laryngol 112(1):40–44
Iwanaga K, Hasegawa K, Shibata N, Kawakatsu K, Akita Y, Suzuki K, Yagisawa M, Nishimura T (2003) Endoscopic examination of obstructive sleep apnea syndrome patients during drug-induced sleep. Acta Otolaryngol 550:36–40
Johal A, Battagel JM, Kotecha BT (2005) Sleep nasendoscopy: a diagnostic tool for predicting treatment success with mandibular advancement splints in obstructive sleep apnoea. Eur J Orthod 27(6):607–614. doi:10.1093/ejo/cji063
Kezirian EJ, Hohenhorst W, de Vries N (2011) Drug-induced sleep endoscopy: the VOTE classification. Eur Arch Otorhinolaryngol 268(8):1233–1236. doi:10.1007/s00405-011-1633-8
Steinhart H, Kuhn-Lohmann J, Gewalt K, Constantinidis J, Mertzlufft F, Iro H (2000) Upper airway collapsibility in habitual snorers and sleep apneics: evaluation with drug-induced sleep endoscopy. Acta Otolaryngol 120(8):990–994
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Ward SL, Tangredi MM (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events: deliberations of the sleep apnea definitions task force of the american academy of sleep medicine. J Clin Sleep Med 8(5):597–619. doi:10.5664/jcsm.2172
Herzog M, Metz T, Schmidt A, Bremert T, Venohr B, Hosemann W, Kaftan H (2006) The prognostic value of simulated snoring in awake patients with suspected sleep-disordered breathing: introduction of a new technique of examination. Sleep 29(11):1456–1462
Eichler C, Sommer JU, Stuck BA, Hormann K, Maurer JT (2013) Does drug-induced sleep endoscopy change the treatment concept of patients with snoring and obstructive sleep apnea? Sleep Breath 17(1):63–68. doi:10.1007/s11325-012-0647-9
Pilaete K, De Medts J, Delsupehe KG (2014) Drug-induced sleep endoscopy changes snoring management plan very significantly compared to standard clinical evaluation. Eur Arch Otorhinolaryngol 271(5):1311–1319. doi:10.1007/s00405-013-2795-3
Fernandez-Julian E, Garcia-Perez MA, Garcia-Callejo J, Ferrer F, Marti F, Marco J (2014) Surgical planning after sleep versus awake techniques in patients with obstructive sleep apnea. Laryngoscope 124(8):1970–1974. doi:10.1002/lary.24577
Cavaliere M, Russo F, Iemma M (2013) Awake versus drug-induced sleep endoscopy: evaluation of airway obstruction in obstructive sleep apnea/hypopnoea syndrome. Laryngoscope 123(9):2315–2318
Campanini A, Canzi P, De Vito A, Dallan I, Montevecchi F, Vicini C (2010) Awake versus sleep endoscopy: personal experience in 250 OSAHS patients. Acta Otorhinolaryngol Ital 30(2):73–77
Huo H, Li W, Tian X, Xu C, Wang J, Yang D (2014) Endoscopic upper airway evaluation in obstructive sleep apnea: Mueller’s maneuver versus simulation of snoring. Sleep Breath. doi:10.1007/s11325-014-1073-y
Conflict of interest
There are no institutional or corporate affiliations of the authors and there are no funding sources which supported the work.
Author information
Authors and Affiliations
Corresponding author
Additional information
M. Herzog and P. Kellner contributed equally to the project.
Rights and permissions
About this article

Cite this article
Herzog, M., Kellner, P., Plößl, S. et al. Drug-induced sleep endoscopy and simulated snoring in patients with sleep-disordered breathing: agreement of anatomic changes in the upper airway. Eur Arch Otorhinolaryngol 272, 2541–2550 (2015). https://doi.org/10.1007/s00405-015-3559-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-015-3559-z