
Abstract
Objective
To analyze the relationship between the symptoms of pelvic floor dysfunction (PFD) and quality of life (QoL), as well as the function of the pelvic floor muscle (PFM) in women with urinary incontinence (UI).
Methods
A cross-sectional study conducted in two centers in Brazil (Northeast and Southeast regions) with women with stress urinary incontinence (SUI) and mixed urinary incontinence (MUI). Data on pelvic floor symptoms, discomfort and impact on QoL were collected using the Pelvic Floor Distress Inventory-short form (PFDI-SF-20) and the Pelvic Floor Impact Questionnaire (PFIQ-7) instruments. PFM function was assessed by palpation (PERFECT scale) and manometry. Pearson’s correlation test, analysis of variance (ANOVA) and the Student’s t test were used to discriminate the differences, adopting a significance level of 5%.
Results
A total of 72 women participated in the study (mean age 51.7 ± 11.9 years). The presence and discomfort of pelvic floor symptoms (PFDI-SF-20) were correlated with QoL (PFIQ-7) (r = 0.52, p < 0.001). Deficits in PFM function (power and pressure) were observed, however, there was no correlation between these with the presence and discomfort of the pelvic floor symptoms (PFDI-SF-20).
Conclusion
Greater discomfort due to PFD symptoms were correlated with a worse QoL. However, the relationship between symptoms and PFM function was not significant. These results reinforce the need to assess the aspects of activity and participation which compose functionality and QoL, and not only the PFM functions in women with UI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to the International Urogynecology Association (IUGA)/International Continence Society (ICS), urinary incontinence (UI) is defined as a complaint of involuntary loss of urine, with the most common types being stress urinary incontinence (SUI), urgency urinary incontinence (UUI) and mixed urinary incontinence (MUI). This health condition has a prevalence ranging from 5 to 69% in women depending on the population studied, with most studies in the range of 25–45% [1,2,3].
Studies have shown that UI has a great impact on the quality of life (QoL) of women, affecting functionality, mental or emotional health, social life, sexuality, self-perception and interpersonal relationships. These aspects can make women more depressed, anxious, frustrated and/or nervous and impair their daily, work, physical and entertainment activities [4, 5].
In addition to urinary symptoms, other pelvic floor symptoms may be present in women with UI, some of which are fecal urgency, anal incontinence, constipation, a feeling of vaginal bulging, pelvic pressure, dyspareunia and vaginal laxity [1]. These symptoms are associated with other pelvic floor disorders (PFD) such as pelvic organ prolapse (POP), anorectal and sexual disorders, which commonly have a strong association with each other, as well as a propensity for coexistence in women [6].
These symptoms can have significant impacts on the QoL of women, whether associated or not with UI. A study carried out with a general population of adult women (n = 539) showed that women with symptomatic POP have worse QoL scores when compared to asymptomatic women and that the presence of this dysfunction reveals years of life lost due to premature mortality and disability [7]. Regarding intestinal symptoms, constipation impacts QoL, with worse scores found in women with persistent constipation compared to those who had transient constipation or who had no symptoms [8]. Most women with anal incontinence (AI) have a change in QoL, being even worse in those who lose liquid stools [9].
Regarding the coexistence of these pelvic floor symptoms, worse QoL scores were found in women complaining of UI and/or POP who had AI or other associated intestinal symptoms [10]. Worse scores in QoL domains related to fecal incontinence (FI) were observed such as coping behavior, depression or self-perception, lifestyle and level of embarrassment [11]. A worse QoL was also found in patients with severe FI with more severe colorectal/anal and urinary symptoms [12].
An evaluation of QoL in women with incontinence is a recommendation from the ICS and the use of specific tools is considered more sensitive for measuring QoL when compared to the use of generic questionnaires [13]. Contemplating the subjectivity of the patient is of paramount importance to complement the assessment and assist in clinical decision-making centered on functionality.
The Pelvic Floor Distress Inventory-short form (PFDI-SF-20) is a questionnaire which evaluates the presence of multiple PFD symptoms (urinary, vaginal and intestinal) and how much they bother a patient, while the Pelvic Floor Impact Questionnaire (PFIQ-7) proposes to assess QoL taking into account how much the pelvic floor symptoms (bladder, vagina/pelvis and intestine) impact physical, social and emotional aspects, and consequently the functionality of women [14, 15].
Considering that these questionnaires cover questions on activity and participation, and in view of the need to understand these aspects, the present study aimed to analyze the relationship between the symptoms of PFD and QoL, as well as the pelvic floor muscle (PFM) function in women with SUI or MUI.
Methods
Study design and setting
This is a cross-sectional study carried out in two centers: Women’s Health Research Laboratory (LAMU), Physical Therapy Department, Federal University of São Carlos, in São Carlos, SP, Brazil; and in the Physiotherapy service of the Urogynecology Outpatient Clinic of Maternidade Escola Assis Chateaubriand (MEAC), in Fortaleza, CE, Brazil. Data collection was carried out from October 2015 to July 2018.
Inclusion and exclusion criteria
Women with SUI or MUI aged 18 and older who answered the following questions were included: “Do you lose urine during physical exertion, such as coughing, sneezing, running, etc.?”; and “Do you feel a strong urge to urinate, with loss of urine, before you get to the bathroom?”. Women who answered “yes” to the first question or both questions were recruited for this study [16].
Women who had only urge-incontinence, neuromuscular diseases, asthma, tumors, heart failure, PERFECT scale “P” value graded at 0, urinary tract infection, cognitive deficit, uncontrolled arterial hypertension, presence of severe prolapses (visible prolapse in the vaginal opening) and who had undergone physiotherapy treatment in the last 12 months ago were excluded from the study [17].
Data collection
Sample recruitment
The sample was recruited non-probabilistically by convenience, with women being recruited from the MEAC outpatient clinic or from LAMU. Socioeconomic, demographic and clinical data were collected after signing the Free and Informed Consent Form (ICF), as well as a PFM functional assessment, manometry and application of the instruments to evaluate the PFD symptoms and QoL in sequence.
Socioeconomic and demographic information (age, BMI, education, occupation, annual family income and marital status), clinical data (main complaint, associated diseases and pelvic organ prolapse), obstetric history, bladder storage and voiding and postmicturition symptoms and information on physical activity were collected through a structured evaluation form.
Assessment of pelvic floor muscle function
For evaluating PFM function, the participant was placed in the supine position with their hips and knees flexed and the evaluator performed unidigital vaginal palpation. Muscle function was assessed using the PERFECT scale. The variable was categorized according to the ICS classification based on the Power (P) value of the PERFECT scale, which categorizes the PFM contraction function as absent, weak, normal or strong (P0 to 2 = Weak, P3 = Normal, and P4 and P5 = Strong) [17, 18].
Next, the PFM contraction pressure was assessed while still in the same position using a Peritron device (Cardio Design Pty Ltd, Oakleigh, Victoria, Australia), which has a 0–300 cm H2O graduation and is equipped with a vaginal probe (28 × 55 mm). The value of the vaginal pressure at rest was collected, meaning in the absence of voluntary PFM contraction. Soon after, the device was calibrated and the participant received a verbal command to perform maximum voluntary contraction of the PFM for five seconds in duration, 3 times, with an interval of 30 s between contractions. The researcher visually analyzed whether the PFM contractions were performed correctly, observing an “in and up” movement of the vaginal probe and minimal contractions of the accessory musculature [19]. The mean of the three measurements found was used for data analysis.
Data collection instruments
The Pelvic Floor Distress Inventory-short form (PFDI-SF-20) and the Pelvic Floor Impact Questionnaire (PFIQ-7) questionnaires, validated for the Portuguese language (Brazil), were applied. The PFDI-SF-20 questionnaire is an instrument of 20 questions distributed among 3 domains (Bladder, Intestine and Pelvis) in the subscales: Pelvic Organ Prolapse Disorder Inventory (POPDI-6) with 6 questions, Colorectal-Anal Disorder Inventory (CRADI-8) with 8 questions, and Urinary Disorder Inventory (UDI-6) with 6 questions. Each item asks if the patient has a certain symptom, considering the last 3 months. If the answer is “yes”, it should classify how much this symptom bothers them among the alternatives: nothing, a little, moderately, or a lot. The score for each subscale ranges from 0 to 100 and the total score between 0 and 300. In turn, the PFIQ-7 questionnaire is an instrument composed of seven questions and divided into three subscales: the Urinary Impact Questionnaire (UIQ-7), the Colorectal-Anal Impact Questionnaire (CRAIQ-7) and the Pelvic Organ Prolapse Impact Questionnaire (POPIQ-7). In each question, the patient answers how much the bladder, intestine or vaginal symptoms affect her activities, relationships and feelings by choosing an alternative, on the Likert scale which best describes the distress (not even a little, a little, moderately or a lot). The score for each subscale varies from 0 to 100 and the total score is between 0 and 300. Both instruments are used to assess QoL, with PFDI-SF-20 being related to the discomfort of symptoms and PFIQ-7 related to the impact on physical, social and emotional aspects. Higher scores in these questionnaires identify a greater impact on QoL [14, 15].
Statistical methods
The collected data were tabulated in Excel® and analyzed using the “Statistical Package for the Social Sciences”—SPSS version 22.0 program. The data normality was assessed by the Shapiro–Wilk test. The data were arranged in means and standard deviations or in absolute and relative frequency, depending on the variable evaluated. Pearson’s correlation test was used to analyze the correlation between the total and partial scores of the PFIQ-7 questionnaire and the PFM function (Power and manometry), with the means of the total and partial scores of the PFDI-SF-20 questionnaire. A comparison of PFM strength classification in three categories (ICS classification—weak, normal or strong) with the total score of the PFDI-SF-20 was performed by analysis of variance (ANOVA). A level of significance of 5% was adopted.
Ethical approval
The study refers to a secondary analysis of an intervention study on pelvic floor muscle training in women with UI, approved by the Research Ethics Committee (CEP) of the Federal University of São Carlos (CAAE: 42677115.5.0000.5504, report 2.579.162), with the consent of the CEP of MEAC, on April 4, 2018 [20].
Results
A total of 72 women participated in the study, 54.2% with complaints of MUI and 45.8% of SUI, with a mean age of 51.7 ± 11.9 years, and the majority having low educational and economic levels (Class C and D = 66.7%) (Table 1).
Regarding urinary complaints, urine loss when sneezing and coughing (97.2%), urgency (62.5%), urge-incontinence (59.7%) and feeling of incomplete emptying (58.3%) were the symptoms most reported by the studied sample (Table 2).
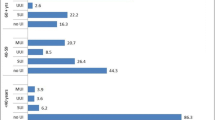
Pelvic floor dysfunction symptoms prevalent by subscales of the PFDI-SF-20 questionnaire were: urine loss during laughter, coughing or sneezing (93.1%) and small amount of urine loss (87.5%) in the subscale of urinary symptoms (UDI-6), fecal urgency (56.9%) and feeling of incomplete evacuation (20.8%) in the subscale of intestinal symptoms (CRADI-8) and pelvic pressure and feeling of incomplete emptying (23.6% each) in the prolapse symptom subscale (POPDI-6). A prevalence of 11.2% of women with fecal incontinence and 25% with pelvic organ prolapse was also found considering the data from the anamnesis and the symptoms questionnaire (data not shown in the tables).
We observed a moderate positive correlation (r = 0.52) between the total scores of the PFDI-SF-20 and PFIQ-7 instruments, (p < 0.001), showing that the presence and greatest discomfort of the pelvic floor dysfunction symptoms (PFDI -SF-20) has a correlation with the worst evaluated QoL (PFIQ-7). A significant positive correlation was found in all when the subscales of PFDI-SF-20 (UDI-6, POPDI-6 and CRADI-8) and the corresponding scales of PFIQ-7 (UIQ-7, POPIQ-7 and CRAIQ-7) were analyzed, being moderate among the subscales related to urinary symptoms (UDI-6 and UIQ-7), and weak in relation to the other subscales (Table 3).
Table 4 demonstrates the assessment of PFM function by the PERFECT scale and manometry using Peritron®, showing that there was no significant correlation between the Power and Peritron average with the PFDI-20 average.
Likewise, there was no statistically significant difference when comparing the PFDI-20 values between the ICS classification categories (Table 5).
Discussion
Our results showed that the presence and greater discomfort of pelvic floor dysfunction symptoms correlate with the worst QoL regarding the impact on activities, feelings and relationships in women with UI. However, no significant relationship was observed between the presence of PFD symptoms and the worst PFM function.
UI is the most prevalent pelvic floor dysfunction (PFD) according to data from Brazilian and international studies. National studies show a prevalence of UI ranging between 23% and 52.3% [21]. A study carried out in the United States showed that 23.7% women had PFD, with the majority (15.7%) having UI [22].
Studies show a higher prevalence of SUI, however, MUI was found in a greater number of women in our sample [23, 24]. This can be justified by the fact that the sample is composed of women with advanced age who are more predisposed to UI associated with urgency, in addition to the fact that more severe forms of UI are directly referred for surgical treatment, while women with mild to moderate UI are referred for conservative treatment such as physiotherapy. This low UI severity may explain the fact that the discomfort and impact scores on QoL found in our collection instruments do not present such high values, therefore not contributing to an observation of drastic QoL reduction.
For urinary symptoms, more symptoms related to UI were observed in our study such as urinary loss when sneezing and coughing, urgency and urge-incontinence in relation to other urinary and POP and intestinal symptoms. These findings were also found in other studies that reported incontinence, loss upon exertion, coughing, sneezing, laughing and carrying weight, and urinary urgency as the complaints most stated by the participants [25]. This is justified by the fact that UI is the main complaint and the reason for seeking care, even in the presence of other PFD in this sample [26, 27].
The results of the present study also showed higher scores of symptom discomfort and impact on the QoL of the subscales related to urinary symptoms (IDU-6 and UIQ-7), with a stronger correlation between them. According to the findings of a cross-sectional study with 3,684 women, this probably occurs because the severity of UI symptoms is the main predictor for reducing generic and specific QoL [28]. Although urinary symptoms are responsible for most of the impact on QoL in this sample, the fact that the sample does not have women with severe UI makes the reduction in QoL not so significant.
Our results also showed anorectal symptoms such as fecal urgency, feeling of incomplete evacuation and fecal incontinence, and prolapse symptoms such as pelvic pressure and feeling of incomplete emptying in the studied sample. The association of UI with POP and other symptoms related to anorectal disorders is commonly reported in studies [27].
These symptoms associated with UI brought discomfort and worse QoL to the participants of the present study, as evidenced by the significant correlation between the total scores and the subscales of the two instruments. This is explained by the greater impact of the coexistence of pelvic floor symptoms in relation to isolated dysfunction. A study which reported the prevalence, discomfort and impact on the QoL of intestinal symptoms in women treated for UI and POP found that women with UI and intestinal symptoms, such as anal incontinence, constipation or fecal urgency, had worse QoL compared to those who only had UI [27]. However, the subscale scores related to intestinal symptoms (CRADI-8 and CRAIQ-7) and prolapse (POPDI-6 and POPIQ-7) showed a weak correlation with QoL, perhaps due to the low prevalence of these symptoms in the present sample.
A feasibility study analyzed the relationship of PFDI-SF-20 and PFIQ-7 with generic QoL in women with fecal incontinence, observing a moderate to strong correlation between the PFDI-20 and PFIQ-7 instruments and three instruments which measure self-reported QoL in a generic way. Worse scores on the generic QoL instruments correlated with greater severity of symptoms and worse QoL specific to PFD [26]. We did not evaluate the generic QoL in our study, but understanding this correlation is important to measure the dimensional impact of PFD symptoms.
Regarding the PFM assessment, a recent study evaluated 216 postmenopausal women with and without PFD and found no statistically significant relationship between the PFM function and QoL assessed by the King’s Health Questionnaire [29]. Another study which used a modified Oxford scale with 15 categories, manometry and two generic QoL questionnaires (EuroQoL-5D and SF-12) also found no correlation between the generic QoL assessment and PFM function [30]. Therefore, PFM function does not seem to be able to determine QoL, but it can determine the severity of symptoms, as found in the present study. The musculature may be weaker in individuals with more severe symptoms but it is the presentation of the symptoms that defines how much the QoL will be impaired. The relationship between the severity of symptoms by the PFDI-20 and the PFM function by the PERFECT scale and manometry was also analyzed in the present sample, however, no significant relationship was found.
Unlike the other studies, this study does not only assess the impact of UI on QoL, but also the impact of other pelvic floor symptoms which are often neglected. In addition, the study also correlated two instruments, and therefore is not only limited to presenting the QoL findings but establishing their relationship with the symptoms.
The main limitations of the study were the sample being composed of women diagnosed with UI with a low prevalence of other PFD, and not including women with severe prolapses, which constitute conditions that would certainly contribute to a greater impact on QoL.
The PFDI-SF-20 and PFIQ-7 questionnaires can be allied instruments for assessing QoL and detecting PFD, which are often underreported. In addition, these instruments can be used as aids to the International Classification of Functionality (ICF), providing information related to structure and function through the PFDI-20, and activities and participation through the PFIQ-7. This information will contribute to treatment centered on functionality, an important aspect of the QoL of individuals, thereby contrasting the biomedical model centered on the disease. Thus, it would contemplate the functioning aspects related to health conditions, establishing conducts centered on the individual and improvement in QoL.
Conclusion
The existence of urinary, intestinal and vaginal symptoms in women with SUI or MUI presented discomfort and a negative impact on QoL, revealing a relationship between the greatest discomfort of PFD symptoms and the worst QoL. Reduced PFM strength, resistance and pressure were observed using the PERFECT scale and manometry, however, there were no significant relationships between these variables and the presence and discomfort of pelvic floor symptoms.
We emphasize the importance of assessing the aspects of activity and participation which compose functionality and QoL, and not only the PFM functions in women with UI. Finally, we highlight the need to better understand the discomfort dimension and impact of these symptoms, reinforcing the importance of evaluating other PFD in this population and establishing conducts focused on functionality.
Data availability
The corresponding author and co-authors declare the data in this manuscript to be completely transparent.
Code availability
Not applicable.
References
Haylen BT, de Ridder D, Freeman RM et al (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J 21:5–26. https://doi.org/10.1007/s00192-009-0976-9
Abrams P, Andersson KE, Birder L et al (2010) Fourth international consultation on incontinence recommendations of the international scientific committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 29:213–240. https://doi.org/10.1002/nau.20870
Abrams P, Cardozo L, Khoury S, Wein A (2013) Incontinence. 5a. Paris: ICUD-EAU
Schimpf MO, Patel M, O’Sullivan DM, Tulikangas PK (2009) Difference in quality of life in women with urge urinary incontinence compared to women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 20:781–786. https://doi.org/10.1007/s00192-009-0855-4
Firdolas F, Onur R, Deveci SE, Rahman S, Sevindik F, Acik Y (2012) Effect of urinary incontinence and its subtypes on quality of life of women in eastern Turkey. Urology 80:1221–1226. https://doi.org/10.1016/j.urology.2012.08.023
Fornell EU, Wingren G, KjOlhede P (2004) Factors associated with pelvic floor dysfunction with emphasis on urinary and fecal incontinence and genital prolapse: an epidemiological study. Acta Obstet Gynecol Scand 83:383–389. https://doi.org/10.1111/j.0001-6349.2004.00367.x
Svihrova V, Svihra J, Luptak J, Swift S, Digesu GA (2014) Disability-adjusted life years (DALYs) in general population with pelvic organ prolapse: a study based on the prolapse quality-of-life questionnaire (P-QOL). Eur J Obstet Gynecol Reprod Biol 182:22–26. https://doi.org/10.1016/j.ejogrb.2014.08.024
Koloski NA, Jones M, Wai R, Gill RS, Byles J, Talley NJ (2013) Impact of persistent constipation on health-related quality of life and mortality in older community-dwelling women. Am J Gastroenterol 108:1152–1158. https://doi.org/10.1038/ajg.2013.137
Boreham MK, Richter HE, Kenton KS et al (2005) Anal incontinence in women presenting for gynecologic care: Prevalence, risk factors, and impact upon quality of life. Am J Obstet Gynecol 192:1637–1642. https://doi.org/10.1016/j.ajog.2004.11.030
Bezerra LRPS, Vasconcelos Neto JA, Vasconcelos CTM et al (2014) Prevalence of unreported bowel symptoms in women with pelvic floor dysfunction and the impact on their quality of life. Int Urogynecol J. https://doi.org/10.1007/s00192-013-2317-2
Portella PM, Feldner PC Jr, da Conceição JC, Castro RA, Sartori MG, Girão MJ (2012) Prevalence of and quality of life related to anal incontinence in women with urinary incontinence and pelvic organ prolapse. Eur J Obstet Gynecol Reprod Biol 160:228–231. https://doi.org/10.1016/j.ejogrb.2011.11.009
Bordeianou L, Hicks CW, Olariu A et al (2015) Effect of coexisting pelvic floor disorders on fecal incontinence quality of life scores. Dis Colon Rectum 58:1091–1097. https://doi.org/10.1097/DCR.0000000000000459
Tamanini JTN, Dambros M, D’Ancona CAL, Palma PCR, Netto NR Jr (2004) Validação para o português do “International Consultation on Incontinence Questionnaire—Short Form” (ICIQ-SF). Rev Saúde Pública 38:438–444. https://doi.org/10.1590/S0034-89102004000300015
Barber MD, Kuchibhatla MN, Pieper CF, Bump RC (2001) Psychometric evaluation of 2 comprehensive condition-specific quality of life instruments for women with pelvic floor disorders. Am J Obstet Gynecol 185:1388–1395. https://doi.org/10.1067/mob.2001.118659
Arouca MAF, Duarte TB, Lott DAM et al (2016) Validation and cultural translation for Brazilian Portuguese version of the Pelvic Floor Impact Questionnaire (PFIQ-7) and Pelvic Floor Distress Inventory (PFDI-20). Int Urogynecol J 27:1097–1106. https://doi.org/10.1007/s00192-015-2938-8
Rohr G, Christensen K, Ulstrup K, Kragstrup J (2004) Reproducibility and validity of simple questions to identify urinary incontinence in elderly women. Acta Obstet Gynecol Scand 83:969–972. https://doi.org/10.1111/j.0001-6349.2004.00557.x
Laycock J, Jerwood D (2001) Pelvic floor muscle assessment: the PERFECT scheme. Physiotherapy 87:631–642. https://doi.org/10.1016/S0031-9406(05)61108-X
Messelink B, Benson T, Berghmans B et al (2005) Standardization of terminology of pelvic floor muscle function and dysfunction: report from the pelvic floor clinical assessment group of the International Continence Society. Neurourol Urodyn 24:374–380. https://doi.org/10.1002/nau.20144
Bo K, Talseth T, Holme I (1999) Single blind, randomised controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women. BMJ 318:487–493. https://doi.org/10.1136/bmj.318.7182.487
Figueiredo VB, Nascimento SL, Martínez RFL, Lima CTS, Ferreira CHJ, Driusso P (2020) Effects of individual pelvic floor muscle training vs individual training progressing to group training vs group training alone in women with stress urinary incontinence: a randomized clinical trial. Neurourol Urodyn 39(5):1447–1455. https://doi.org/10.1002/nau.24370
Reigota RB, Pedro AO, Souza SMV, Costa-Paiva L, Pinto-Neto AM (2016) Prevalence of urinary incontinence and its association with multimorbidity in women aged 50 years or older: a population-based study. Neurourol Urodyn 35:62–68. https://doi.org/10.1002/nau.22679
Nygaard I, Barber MD, Burgio KL et al (2008) Prevalence of symptomatic pelvic floor disorders in US women. JAMA 300:1311–1316. https://doi.org/10.1001/jama.300.11.1311
Hannestad YS, Rortveit G, Sandvik H, Hunskaar S (2000) A community-based epidemiological survey of female urinary incontinence. J Clin Epidemiol 53:1150–1157. https://doi.org/10.1016/S0895-4356(00)00232-8
Minassian VA, Bazi T, Stewart WF (2017) Clinical epidemiological insights into urinary incontinence. Int Urogynecol J 28:687–696. https://doi.org/10.1007/s00192-017-3314-7
Rodrigues MP, Barbosa LJF, Ramos JGL et al (2016) Perfil das pacientes do ambulatório de uroginecologia de um Hospital Público de Porto Alegre com relação à incontinência urinária e à qualidade de vida. Clin Biomed Res 36:131–135. https://doi.org/10.4322/2357-9730.64817
Harvie HS, Arya LA, Saks EK, Sammel MD, Schwartz JS, Shea JA (2011) Utility preference score measurement in women with fecal incontinence. Am J Obstet Gynecol 204:72.e1–72.e6. https://doi.org/10.1016/j.ajog.2010.08.018
da Cunha RM, Leite LC, de Oliveira GND, Brito AG, de Figueiredo VB, do Nascimento SL (2016) Perfil epidemiológico e sintomas urinários de mulheres com disfunções do assoalho pélvico atendidas em ambulatório. Rev Fisioter S Fun 5(1):2–49
Barentsen JA, Visser E, Hofstetter H, Maris AM, Dekker JH, da Bock GH (2012) Severity, not type, is the main predictor of decreased quality of life in elderly women with urinary incontinence: a population-based study as part of a randomized controlled trial in primary care. Health Qual Life Outcomes 10:153. https://doi.org/10.1186/1477-7525-10-153
Frota IPR, Rocha ABO, Neto JAV et al (2018) Pelvic floor muscle function and quality of life in postmenopausal women with and without pelvic floor dysfunction. Acta Obstet Gynecol Scand 97:552–559. https://doi.org/10.1111/aogs.13305
Chevalier F, Fernandez-Lao C, Cuesta-Vargas AI (2014) Normal reference values of strength in pelvic floor muscle of women: a descriptive and inferential study. BMC Womens Health 14:143. https://doi.org/10.1186/s12905-014-0143-4
Acknowledgements
We are grateful for the contribution of physiotherapists from the Pelvic Physiotherapy Service/Rehabilitation Unit of the Maternidade Escola Assis Chateuabriand (MEAC) and contribution from the Physiotherapy Project in Women's Health (PROFISM).
Funding
This study was supported by the Foundation for Support in Scientific and Technological Development of Ceará (FUNCAP, Fortaleza, CE, Brazil), through doctoral fellowship, funder approval number: nº BDS‐0017‐00071.01.11/15 and São Paulo Research Foundation(FAPESP), Project Number 2016/0638‐4. This study was supported in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Author information
Authors and Affiliations
Contributions
MQSF: Protocol/project development, data collection or management, data analysis, manuscript writing/editing. MAM: Protocol/project development, data analysis, manuscript writing/editing. ACRM: data collection or management, manuscript writing/editing. VBF: Protocol/project development, data collection or management, data analysis, manuscript writing/editing. PD: Protocol/project development, manuscript writing/editing. SLN: Protocol/project development, data analysis, manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflict of interest.
Ethical approval
The study refers to a secondary analysis of an intervention study on pelvic floor muscle training in women with UI, approved by the Research Ethics Committee (CEP) of the Federal University of São Carlos (CAAE: 42677115.5.0000.5504, report 2.579.162), with the consent of the CEP of MEAC, on April 4, 2018.
Consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for publication
All participants were informed of the procedures, risks and benefits of participating in the study, and their data were included in the research after signing the Free and Informed Consent Form (ICF). The corresponding author and co-authors agree with the publication of the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fontenele, M.Q.S., Moreira, M.A., de Moura, A.C.R. et al. Pelvic floor dysfunction distress is correlated with quality of life, but not with muscle function. Arch Gynecol Obstet 303, 143–149 (2021). https://doi.org/10.1007/s00404-020-05770-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-020-05770-5