
Abstract
Introduction
Due to technical improvements and growing experience, hysterectomies are performed laparoscopically more and more frequently. We analyzed 43 total laparoscopic hysterectomies (TLH) of the years 2005 and 2006 and compared them with 87 vaginal (VH) and 103 abdominal hysterectomies (AH).
Methods
Patients’ original files and surgery reports of the TLHs, VHs and AHs were analyzed retrospectively for the indication of surgery, patients’ age, weight, parity, time for surgery, uterus weight, blood loss, post-operative need of analgetics, hospital stay, complications and so on. Data were compared with Student’s t test and χ2 test.
Results
Indications for TLH were fibroids (n = 21), endometrial cancer (n = 10), bleeding anomalies (n = 7), dysplasia of the cervix uteri (n = 3) and others. In 23/43 cases salpingo-ovarectomy was added, in six cases laparoscopic pelvic or paraaortic lymphadenectomy (LNE) was performed. Looking at cases without LNE, patients’ median age was 46 years (32–72), median weight 68 kg (53–115), median time for TLH 130 min (75–270), median uterus weight 150 g (44–954), median blood loss 200 ml (50–600), post-operative analgetica were given for 1.5 days (0–12), and post-operative hospital stay was 6 days (2–15). Indications for VH were genital prolapse (n = 53, 61%), often combined with fixative procedures (n = 50). In this group, median age was significantly higher (median 56 years, P < 0.001). VH was the fastest (median 90 min, P < 0.001), but blood loss was highest (median 300 ml, P = 0.07). In cases with AH, uterus weight was significantly higher (median 290 g, P < 0.001), as well as the need for analgetics (median 4 days, P = 0.001), and the hospital stay was longest (median 8 days, P < 0.001). Major complications of TLH were bladder injury (3×), of VH rectum lesion (2×, both at pelvic repair measures), of AH post-operative ileus (2×) and vesico-vaginal fistula (1×).
Conclusion
For many patients TLH is a safe and less invasive alternative, especially towards AH, and shows significantly better post-operative reconstitution. Although VH is faster and shows comparable post-operative results, TLH offers the advantage to view the intra-abdominal situs and perform additional steps in case of pathologies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Hysterectomy (HE) belongs to the oldest surgical procedures in medicine. Originally performed vaginally for prolapse, probably even in ancient Egypt, and described first by Soranus of Ephesus in the year 120 ad [1], hardly any women at that time survived the removal of uterus with ligatures and installation of ice for hemostasis. Developments in anesthesia, asepsis and surgical skills in the nineteenth century led to an increasing number of hysterectomies mainly for oncologic diseases. In the twentieth century, further improvements in suture techniques, skills and the possibility of applying blood products or antibiotics made hysterectomies a standard operation of gynecologists [2]. This development led to approximately 600,000 hysterectomies in the USA in 1999, which resulted in a rate of more than 25% of women above the age of 60 years who underwent this operation [3]. Although this rate is lower in Europe, gynecologists occasionally face criticism about their indications for hysterectomy. Most frequent reasons to remove the uterus excluding malignancies are fibroids, bleeding irregularities, endometrial hyperplasia or cervical dysplasia, endometriosis and prolapse. Whereas the vaginal and the abdominal approaches to perform hysterectomy have been established long time ago, the development of laparoscopic surgery took several decades. Early attempts to view the abdominal or thoracic cavity by optical systems started at the beginning of the twentieth century. First reports on laparoscopic surgery within the female pelvis were made by Roul Palmer in Paris in 1944. But it was Kurt Semm in the 1960s and 1970s, who developed many instruments such as the CO2-insufflator, thermo-coagulator or rinse and vacuum device which were essential to go beyond diagnostic laparoscopy. Improvements in light sources, optics and cameras led to endoscopic appendectomies, cholecystectomies and salpingo-ovarectomies. From this, it was a small step towards laparoscopically assited vaginal hysterectomy (LAVH) [4], and finally total laparoscopic hysterectomy (TLH) was established from 1989 onwards [5, 6]. Till now, several studies have confirmed the feasibility of TLH as a safe method with better post-operative recovery, reduced need of analgetics and shorter hospital stay [7–10]. Although at the beginning, TLHs took longer intra-operative time, the surgeons’ learning curves reduced this time to the level of abdominal hysterectomy [11] and due to reduced hospital stay, total cost of different methods are comparable [12]. With further developments in techniques and experience, more complicated operations like radical hysterectomies and lymphadenectomies are performed laparoscopically nowadays and numbers are likely to increase in the future. We report here of our experiences with TLH at Munich university hospital in the years 2005 and 2006 in comparison to VH and AH in terms of intra- and post-operative results and complication rates.
Methods
Surgical ward reports have been analyzed for all HEs performed at First Department of Obstetrics and Gynecology, University of Munich, Germany, in the years 2005 and 2006. Radical HEs for cancer of the cervix uteri or higher stage endometrial cancer (pT2 or higher) have been excluded as well as HEs performed for ovarian cancer. Then, the patients’ original files and surgical reports have been analyzed. Laparoscopic supracervical hysterectomies (LSH) and LAVHs have also been excluded. Definition of TLH was that the uterus had to be removed completely laparoscopically and extracted in toto via the vaginal incision, and this circumferential vaginal incision had to be closed by laparoscopic sutures. The original reports were then analyzed for the indications of surgery, patients’ age, weight, parity, uterus weight, operation time, blood loss, post-operative need of analgetics (opioids or non-steroidal anti-inflammatives), hospital stay, and major complications. Data were gathered with the help of Microsoft Excel and analyzed with the SPSS (SPSS Inc., Chicago, IL, USA) statistical package 14.0. Continuous variables of the TLH, VH and AH groups were compared by Students’ t test. For correlation analysis, results of all patients (n = 220) were dichotomized according to their median values and correlated by χ2 test. Significance was stated at a P value below 0.05.
Procedure of TLH
Patients are recommended to have bowel rinsing the day before TLH. The operation is done under general anesthesia with the patients in a Trendelenburg position. Peri-operative antibiotics are given at the start of the operation (Cefuroxim 1.5 g i.v). After desinfection and sterile coverage, we start with a small vertical subumbilical incision for placing the Veres needle. After insufflation of CO2 to a limited pressure of 12 mmHg, a 10 mm re-usable optic trocar is placed and the camera is inserted. The whole abdominal cavity, including peritoneum, liver, gall bladder, stomach, spleen, appendix and bowels should be inspected for pathologies. Further three trocars are placed horizontally in the lower abdomen, usually a single-use 12 mm trocar laterally left and two 5 mm trocars laterally right and in the middle. After bringing the patient in a head-down position, bowels are moved out of the pelvis and the inner genital organs are inspected. If salpingo-ovarectomy is planned, this step is done prior to HE. Then we usually grab the right corner of the corpus uteri with a 10 mm endoscopical pincers and move the uterus to the left in order to stretch the right parametria. The use of an Ultracision device (Ethicon®) is helpful, but a conventional 5 mm bipolar coagulator and scissors can be used instead. We then cut the lig. rotundum and ovarium proprium step by step, open the peritoneum towards the bladder and distract the bladder. The parametria together with the uterine artery are coagulated and severed down to the paracervical area. Positions of the instruments are changed and the same steps are repeated on the left side. We place a phantom into the vagina to mark the end of the cervix uteri and open the anterior vaginal wall after coagulation distant from the portio uteri. The uterus is disconnected from the vagina circumferentially including ligg. sacrouterinae and extracted via the vagina in toto. The phantom is re-placed again to maintain the inside pressure and the end of the vagina is closed endoscopically with resorbable PDS sutures, usually with extracorporal knotting. After rinsing, a drain is placed and the operation is finished.
Procedure of VH
Vaginal hysterectomy (VH) is performed in a Trendelenburg position with maximum adduction of the legs. After desinfection and sterile coverage, the vaginal situs is inspected using a Martin speculum and the portio cervicis is fixated by three forceps. A circumferential incision is made, the bladder is distracted from the anterior cervix and the spatium vesico-uterinum opened. After this, the Douglas peritoneum is opened, a larger speculum is placed and the bowels are pushed back with cloth. Both the ligg. sacro-uterinae are clamped, cut and ligated, and then the parametria are disconnected the same way, close to the uterus, presenting the situs using Breisky specula. The tubes and adnexes are inspected for pathologies and ligated separately. After the removal of the uterus, the peritoneum is closed circumferentially with extraperitonealization of the adnexal stumps. Ligg. sacro-uterinae are joined together and the vagina is closed by absorbable sutures.
Procedure of AH
AH is done either through a horizontal laparotomy above the symphysis or by vertical incision, depending on the size of the uterus and the indication for surgery. After opening and inspection of the abdominal cavity and pushing the bowels out of the pelvis, the fundus uteri is fixated by two forceps at both the corners. Both ligg. rotunda are cut through and ligated, the retroperitoneal spaces are opened and both ureters are visualised. If the adnexes are intended to remain in situ, these are disconnected from the uterus. The peritoneum towards the spatium vesico-uterinum is opened, the bladder distracted down to the anterior cervix and held back by a Breisky speculum. Then, the parametria are cut close to the uterus after fixation with clamps and ligated. Finally, the uterus is removed after clamping the vagina below the portio cervicis, and the vagina is closed by several absorbable sutures. Usually a drain is placed in the Douglas space and the abdomen is closed in different layers.
Results
Patients’ characteristics and indications
Forty-three patients met the criteria for evaluation of TLH. Indications for hysterectomy were fibroids (n = 21), endometrial cancer (n = 10), bleeding anomalies (n = 7), dysplasia of the cervix uteri (n = 3), endometriosis (1×) and trophoblast disease (1×). In 23/43 cases (53%), surgery on the ovaries or tubes (cysts, tumors) was performed additionally. In six cases with endometrial cancer, laparoscopic pelvic or paraaortic lymphadenectomy (LNE) was added. Data of these cases were not taken into account for comparison of intra- and post-operative results. Median age of all patients with TLH was 48 years (32–72) and of those without LNE was 46 years (32–72). Patients’ median weight was 68 kg (53–115), and median parity 1 (0–6, mean 1.3).
Eighty-seven patients had VH for comparison. Major indications were uterine or genital prolapse (n = 53, 61%), fibroids (18×), cervical dysplasia (12×), and bleeding anomalia (4×). In the majority of cases (n = 50, 58%), fixative procedures such as colporrhaphia anterior/posterior were combined. Median age was 56 years (32–86), which was significantly higher (P < 0.001) than that of the TLH group. However, looking at patients without fixative procedures (n = 37), there was no difference in age (median 47 years, 32–76). Patients’ median weight in the VH group was 68 kg (50–120) (VH without prolapse 65 kg, 50–120), which was not statistically different from the other two groups. Median parity of VH patients with or without prolapse was 2 (0–10, mean 2.36), which was significantly higher than that of the TLH cohort (P < 0.001) and the AH group (P < 0.001).
The cases of AH taken into account for comparison were 103. Indications were fibroids with or without bleeding anomalies (65×), endometrial cancer/sarcoma (29×), cervix dysplasia (1×), bleeding irregularities (7×), and trophoblast disease (1×). For all indications see Table 1. In 55 cases (53%) further surgical steps such as tubectomy or salpingo-ovarectomy were performed. Seven patients had pelvic or paraaortic LNE for endometrial cancer: data of these were not taken into account for intra- and post-operative results. Of all the patients with AH, 61 (59%) had laparotomies before and 18 (17%) had caesarean section. Patients’ median age in this cohort was 50 years (36–86), which was statistically different towards the TLH group (P = 0.02), but not towards the VH cohort. Median parity was 1 (0–7, mean 1.19), which was statistically lower when compared with the VH (P < 0.001) but not with the TLH group.
Intra-operative findings
The total time, which was necessary for the operation, was longest in the TLH group and shortest in the VH group. With a median of 130 min (75–270), TLHs took longer time than AHs (median 115 min, 30–230, P = 0.06), which was at the border of significance. In the VH group, median operation time was 90 min (40–175), which was significantly shorter than that of AH and TLH (P < 0.001 each). In the group of VH without pelvic repair, operation time was similar (92 min, 40–130).
However, uterus weight was lowest in the VH group with a median of 92 g (20–360). In the TLH group, uterus weight was higher (med 150 g, 44–954) and in the AH group highest (median 290 g, 18–2,652). This difference between AH and VH as well as TLH was highly significant (P < 0.001 each). Comparing VH with TLH, uterus weight also was significantly (P = 0.004) lower in the VH group.
Intra-operative blood loss as noticed in the operation protocols was lowest in the TLH group with a median of 200 ml (50–600); followed by AH with a median of 250 ml (50–1,800). It was highest in the VH group with a median of 300 ml (50–800), which was at the border of significance towards the TLH cohort (P = 0.07), but not towards the AH group. However, regarding patients only with VH and no additional surgery for prolapse, blood loss (median 250 ml, 100–800) was comparable to that of the AH group.
Post-operative results
Regarding post-operative need of analgetics, patients with TLH received analgetics for a median of 1.5 days (0–12). This was shorter than that of patients with VH (with or without pelvic repair) with a median of 2 days (0–10), which however, was not statistically different. Patients with AH had analgetics for a median of 4 days (0–39), which was significantly longer than that of patients with TLH (P = 0.002) and VH (P < 0.001).
Furthermore, post-operative hospital stay was longest for patients with AH with a median of 8 days (4–41), which was significantly longer than that of patients with VH (median 7 days, 4–13, P < 0.001) and patients with TLH (median 6 days, 2–15, P < 0.001). Comparing VH and TLH, this difference was not statistically significant. Looking at patients with VH without additional fixative measures (n = 37), the duration of the hospital stay (median 6 days, 5–9) was comparable to that of patients in the TLH group. For all comparisons see Table 2.
Correlations between results
Taking all three groups together, patients’ median age was 51 years, median parity was 2, median weight was 68 kg, median time for surgery was 110 min, blood loss in median was 250 ml, all patients received analgetics for a median of 3 days, and median duration of hospital stay was 7 days.
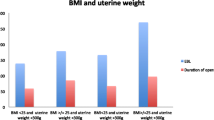
Higher age was significantly related with higher body weight (P = 0.007), lower uterus weight (P < 0.001) and longer hospital stay (P = 0.008), blood loss was borderline non-significant (P = 0.059). Patients’ weight correlated significantly with operation time (P = 0.039). As could be expected, the duration of surgery also correlated with uterus weight (P = 0.021), intra-operative blood loss (P = 0.001), duration of post-operative analgetica intake (P = 0.026) and hospital stay (P < 0.001). Not surprisingly, the duration of analgetica intake itself was correlated significantly with time to hospital discharge (P < 0.001). For all correlations see Table 3.
Complications
Complications in general were rare, but rather specific for the applied surgical methods. Five patients with VH developed hematoma post-operatively, three of these had additional measures for pelvic repair. One of these five patients had a vaginal revision, and another patient with VH, without additional measures needed subsequent laparoscopy with intra-abdominal coagulation. In the VH group, two cases of rectum lesions were observed. However, both had further surgery for genital prolapse, and the rectum lesions had occurred at colporrhaphia posterior and at sacro-spinal fixation of the vagina. Both lesions could be repaired intra-operatively. Further, one patient with VH and pelvic repair showed stenosis of the ureter with proximal dilatation, which required inlay of a double-J catheter.
For AHs, no severe intra-operative complications were documented. Nevertheless, two patients developed ileus during the post-operative period. One patient showed intra-abdominal hemorrhage, which required re-laparotomy, and one patient had a vesico-vaginal fistula a few weeks after the operation, which led to a second intervention. In seven cases, hematoma or complications in wound healing with laparotomy have been reported.
At TLH, three cases of intra-operative lesion of the bladder occurred, which in all cases could be repaired immediately. In no case, a switch towards secondary laparotomy had to be performed. During the post-operative stay, two revisions had to be made, one for obstructed bowel hernia into a trocar incision at the left lower abdomen, and one laparoscopy for intra-abdominal infection. Furthermore, two local hematomata and one case of pyelonephritis have been registered, which neither required any revision.
Discussion
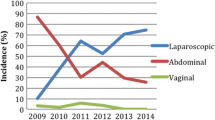
For several decades, indications for the two methods of hysterectomy, vaginal or abdominal one, seemed rather clear in most cases. For patients with smaller uterus, absence of other adnexal pathologies, at least one delivery before, no previous laparotomies, and optionally prolapse, VH was the method of choice. As this procedure is time saving and cost effective and showed best post-operative recovery [13], VH was recommended as the first choice in several guidelines [14]. In any other case, laparotomy had to be performed. Distributions of methods vary in different countries. Rates of AHs, 63% in the USA [15], 67% in the UK [16], and 80% in Denmark [17] have been reported. With developments of endoscopic techniques, LAVH and TLH were added to this spectrum from 1980s and 1990s onwards. Rates of laparoscopically assisted or performed HEs vary from 3 [16] to 9.9% [10] in different regions. As could be expected, our own patient group matched these indications for different ways of HE very well. Patients with VH were significantly older, had more previous deliveries, lower uterus weight and required additional procedures for prolapse in 58% of cases. AH was recommended in case of previous laparotomy such as caesarean section, in cases of large fibroids, or for exploration of uncertain genital tumors. Just as in the TLH group, about half of the patients had surgery on the tubes or ovaries before. TLH was mainly offered to younger patients with none or few previous deliveries, smaller uteri, and indication for exploration of adnexal pathologies. Surprisingly, there was no difference in patients’ weight between the three groups. As reported by Heinberg et al. [18], obesity caused longer operation time, a correlation, which was also demonstrated in our overall patients’ group, but no significant decrease in TLH rate.
With a median of 90 min, VH was significantly the fastest, and TLH with a median of 130 min the slowest. Additional vaginal surgery for pelvic repair did not prolong operation time for VH significantly. Abdelmonem et al. [19] reported times of 103 min for VH, 127 min for AH, and 157 min for TLH. In earlier studies, much longer times for TLH up to 244 min have been found [6], indicating developments in skills and techniques. In our patient group, time for TLH was not statistically different from that of AH. This is in concordance with the study of Ribeiro et al. [20] on 60 patients. As 53% of each TLH and AH cohort had additional surgery for adnexal pathologies, both groups are comparable very well. Undoubtedly, for TLH a certain learning curve is necessary for surgeons beginning with this technique. In a large Canadian trial, a median of 115 min during the first year and 90 min in the following years of TLH have been reported at evaluation of 1,647 cases [11].
As could also be expected, patients with AH had significantly the highest uterus weights with a median of 290 g, and patients with VH the lowest ones. Although differences in blood loss were not statistically significant, this was highest at vaginal operation with a median of 300 ml compared to 200 ml in the TLH group. However, this higher blood loss in the VH cohort was mainly due to surgical steps performed for pelvic repair. Looking at patients with VH and no additional measures, the median blood loss of 250 ml was comparable to that of AH. Some studies described highest blood loss for VH [8], others for AH [19]. Yet, there is an agreement that TLH is the method which shows the lowest risk of hemorrhage, as was demonstrated on a meta-analysis of 3,643 cases [21].
Post-operatively, patients with TLH had the shortest intake of analgetics (median 1.5 days) and the fastest recovery, leading to the shortest hospital stay. However, the difference between TLH and VH was not statistically significant, and patients with only VH without pelvic repair had similar duration of post-operative recovery. In contrast, patients with AH had to take analgetics longest (median 4 days) and stayed in hospital for a median of 8 days. This prolonged stay was also found in all other comparative studies such as the UK EVALUATE trial [22]. Economically, this prolonged reconstitution could outweigh the initial higher costs of TLH, mainly caused by use of disposable instruments.
Complication rates of all HEs were low and comparable to those in literature [23, 24], where TLH is regarded to show more complications than VH or AH. Major complications of TLH are urinary tract lesions. In our patient group of 43 patients, we had 3 cases of bladder lesions, which all could be repaired laparoscopically during the same operation. Makinen et al. [8] described a 7.2-fold risk of ureter injury for patients with TLH compared to those with AH. In this large trial, bowel injury was the predominant complication of VH. In our VH collective, two cases of rectum lesion were seen, but both occurred during fixative procedures and not by hysterectomy itself. AH offers the best overview of the intra-operative situs and the possibility of direct palpation of all structures. By this, intra-operative complications are rare, but laparotomy is most invasive and more likely to cause post-operative complications such as ileus or problems with wound healing.
One aspect, which gains growing attention, is patients’ convenience and satisfaction, especially for benign diseases. Undoubtedly, HE is successful in curing or improving symptoms caused by uterine pathologies [25]. Nevertheless, gynecologists have to deal with demands for less invasive therapies. Kluivers et al. [26] described better contentedness with TLH, and Silva-Filho et al. [13] with VH compared to AH. However, neither Ellstrom et al. [27] nor El Toukhy et al. [28] found a significant influence of the way of hysterectomy on patients’ well-being and sexual function. Nevertheless, TLH as less invasive procedure with improved post-operative recovery and shorter hospital stay [29] should be offered to patients especially as an alternative to the abdominal approach. As VH still is the fastest, even when surgery for pelvic repair is included, this method is an excellent option unless there are further intra-abdominal pathologies. To offend patients’ criticism of HE performed too frequently as “de-feminising” procedures, alternatives such as supracervical HE [30], or uterus conserving therapies like enucleation of fibroids, embolisation or endometrium ablation should also be discussed individually.
References
Sutton C (1997) Hysterectomy: a historical perspective. Baillieres Clin Obstet Gynaecol 11(1):1–22
Zubke W, Solomayer E, Gardanis C, Wallwiener D (2006) Die Geschichte der Hysterektomie. Geburtshilfe Frauenheilkd 66:93–96
Keshavarz H, Hillis S, Kieke B, Marchbanks P (2002) Hysterectomy surveillance—United States, 1994–1999. MMWR CDC Surveill Summ51(SS05):1–8
Nezhat F, Nezhat C, Gordon S, Wilkins E (1992) Laparoscopic versus abdominal hysterectomy. J Reprod Med 37(3):247–250
Canis M, Mage G, Chapron C, Wattiez A, Pouly JL, Bruhat MA (1993) Laparoscopic hysterectomy. A preliminary study 12. Surg Endosc 7(1):42–45
Hasson HM, Rotman C, Rana N, Asakura H (1993) Experience with laparoscopic hysterectomy. J Am Assoc Gynecol Laparosc 1(1):1–11
Gyr T, Ghezzi F, Arslanagic S, Leidi L, Pastorelli G, Franchi M (2001) Minimal invasive laparoscopic hysterectomy with ultrasonic scalpel. Am J Surg 181(6):516–519
Makinen J, Johansson J, Tomas C, Tomas E, Heinonen PK, Laatikainen T et al (2001) Morbidity of 10 110 hysterectomies by type of approach. Hum Reprod 16(7):1473–1478
Johnson N, Barlow D, Lethaby A, Tavender E, Curr L, Garry R (2005) Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials. BMJ 330(7506):1478
Hoffman CP, Kennedy J, Borschel L, Burchette R, Kidd A (2005) Laparoscopic hysterectomy: the Kaiser Permanente San Diego experience. J Minim Invasive Gynecol 12(1):16–24
Wattiez A, Soriano D, Cohen SB, Nervo P, Canis M, Botchorishvili R et al (2002) The learning curve of total laparoscopic hysterectomy: comparative analysis of 1647 cases. J Am Assoc Gynecol Laparosc 9(3):339–345
Chapron C, Fernandez B, Dubuisson JB (2000) Total hysterectomy for benign pathologies: direct costs comparison between laparoscopic and abdominal hysterectomy. Eur J Obstet Gynecol Reprod Biol 89(2):141–147
Silva-Filho AL, Werneck RA, de Magalhaes RS, Belo AV, Triginelli SA (2006) Abdominal vs vaginal hysterectomy: a comparative study of the postoperative quality of life and satisfaction. Arch Gynecol Obstet 74(1):21–24
ACOG Committee Opinion (2005) Number 311, April 2005. Appropriate use of laparoscopically assisted vaginal hysterectomy. Obstet Gynecol 105(4):929–930
Farquhar CM, Steiner CA (2002) Hysterectomy rates in the United States 1990–1997. Obstet Gynecol 99(2):229–234
Maresh MJ, Metcalfe MA, McPherson K, Overton C, Hall V, Hargreaves J et al (2002) The VALUE national hysterectomy study: description of the patients and their surgery. BJOG 109(3):302–312
Gimbel H, Settnes A, Tabor A (2001) Hysterectomy on benign indication in Denmark 1988–1998. A register based trend analysis. Acta Obstet Gynecol Scand 80(3):267–272
Heinberg EM, Crawford BL III, Weitzen SH, Bonilla DJ (2004) Total laparoscopic hysterectomy in obese versus nonobese patients. Obstet Gynecol 103(4):674–680
Abdelmonem A, Wilson H, Pasic R (2006) Observational comparison of abdominal, vaginal and laparoscopic hysterectomy as performed at a university teaching hospital. J Reprod Med 51(12):945–954
Ribeiro SC, Ribeiro RM, Santos NC, Pinotti JA (2003) A randomized study of total abdominal, vaginal and laparoscopic hysterectomy. Int J Gynaecol Obstet 83(1):37–43
Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R (2006) Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 19:CD003677
Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M et al (2004) EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy. Health Technol Assess 8(26):1–154
McPherson K, Metcalfe MA, Herbert A, Maresh M, Casbard A, Hargreaves J et al (2004) Severe complications of hysterectomy: the VALUE study. BJOG 111(7):688–694
Meltomaa SS, Makinen JI, Taalikka MO, Helenius HY (1999) One-year cohort of abdominal, vaginal, and laparoscopic hysterectomies: complications and subjective outcomes. J Am Coll Surg 189(4):389–396
Flory N, Bissonnette F, Amsel RT, Binik YM (2006) The psychosocial outcomes of total and subtotal hysterectomy: a randomized controlled trial. J Sex Med 3(3):483–491
Kluivers KB, Hendriks JC, Mol BW, Bongers MY, Bremer GL, de Vet HC et al (2007) Quality of life and surgical outcome after total laparoscopic hysterectomy versus total abdominal hysterectomy for benign disease: a randomized, controlled trial. J Minim Invasive Gynecol 14(2):145–152
Ellstrom MA, Astrom M, Moller A, Olsson JH, Hahlin M (2003) A randomized trial comparing changes in psychological well-being and sexuality after laparoscopic and abdominal hysterectomy. Acta Obstet Gynecol Scand 82(9):871–875
El Toukhy TA, Hefni M, Davies A, Mahadevan S (2004) The effect of different types of hysterectomy on urinary and sexual functions: a prospective study. J Obstet Gynaecol 24(4):420–425
Chou DC, Rosen DM, Cario GM, Carlton MA, Lam AM, Chapman M et al (1999) Home within 24 hours of laparoscopic hysterectomy. Aust NZJ Obstet Gynaecol 39(2):234–238
Sarmini OR, Lefholz K, Froeschke HP (2005) A comparison of laparoscopic supracervical hysterectomy and total abdominal hysterectomy outcomes. J Minim Invasive Gynecol 12(2):121–124
Acknowledgments
This study contains material analyzed by Ms. K. Klauser in preparation of her thesis to achieve the degree of MD at Ludwig-Maximilians University, Medical Faculty, in Munich, Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schindlbeck, C., Klauser, K., Dian, D. et al. Comparison of total laparoscopic, vaginal and abdominal hysterectomy. Arch Gynecol Obstet 277, 331–337 (2008). https://doi.org/10.1007/s00404-007-0481-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-007-0481-7