
Abstract
Introduction
Early diagnosis and treatment of hip dysplasia are widely accepted as major factors for beneficial outcome. However, modalities for reduction and retention as well as for imaging are currently under clinical investigation. Local and general risk factors, e.g., breech presentation and the family’s desire to avoid in-hospital treatment are major concerns in the decision-making process and consultation. For treatment of unstable hips in newborns the treatment with the Tübingen splint has proven good results in recent studies. However, mid- and long-term outcome studies are missing. We report on clinical results and X-ray parameter of initially unstable hips after treatment with the Tübingen splint at two time points: 12–24 and 24–48 months of age.
Materials and Methods
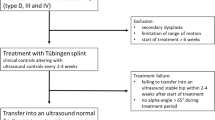
Included were newborns with 83 unstable hips (type D, III, IV according to Graf) which were successfully treated with the Tübingen splint—used as reduction splint 24 h per day/7 days per week—until type I hips were documented by ultrasound examination. Measurments are based on routine pelvic X-ray control at the age of 12–24 and 24–48 months. The acetabular angle was determined and according to the Tönnis-Classification evaluated into: normal findings (< 1 s), slightly dysplastic findings (1–2 s) and severely dysplastic findings (> 2 s). Children with secondary hip dysplasia were not included in this series.
Results
In 2nd year of life, 45 hips (54.2%; initial hip type D: 47.4%, III: 63.2%, IV: 42.9%) of the formerly unstable hips show normal X-ray findings. Although final ultrasound showed normal findings, at this time point 28 hips (33.7%; initial hip type D: 34.2%, III: 31.6%, IV: 42.9%) were slightly dysplastic and 10 (12.0%%; initial hip type D: 18.4%, III: 5.3%, IV: 14.3%) still severely dysplastic. At the age of 24–48 months, the percentage of radiologic normal hips had increased to 61 hips (73.5%; initial hip type D: 68.4%, III: 81.6%, IV: 57.1%), the number of slightly (19 hips) and severely dysplastic (3 hips) hips had decreased 22.9% (initial hip type D: 28.9%, III: 15.8%, IV: 28.6%) respectively 3.6% (initial hip type D: 2.6%, III: 2.6%, IV: 14.3%). At this time no operative intervention was neccessary.
Conclusions
Our mid-term data show on the one hand a good development of unstable hips after successful treatment with the Tübingen splint. On the other hand despite successful therapy and normal ultrasound findings at the end of treatment further imaging by X-ray are mandatory to close follow-up and to detect those which might need surgical correction of residual dysplasia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The introduction of hip ultrasound examinations in the first 6 weeks of life lead to a strong decrease of the need of invasive measures for the treatment of DDH: previously 0.16–0.3% of children with DDH required a surgical intervention. Currently only 0.01–0.13% [1,2,3]. Katthagen et al. [4] showed that the average age at start of treatment was 9 months and the need for operative intervention was 30.7% before introduction of the well-baby program in Germany. Ultrasound findings according to Graf differentiate into four hip types with ten sub groups: the normal hip types Ia, Ib, the immature hip types IIa and dysplastic but stable hip types IIb, IIc (stable), and the unstable hip types IIc (unstable), D, IIIa, IIIb and IV. For the treatment of stable hips, the Tübingen Splint has proven successful outcomes. Here the children are held in stable position of the hip in 90°–110° of flexion and an abduction limited to 40°–50° (Fig. 1) [5]. However, for treatment of unstable hips, the use of plaster casts in human position, e.g., Fettweis plaster or various splints, e.g., Pavlik harness for closed reduction and retention has been established with a success rate of 73–92% [6, 7]. Treatment with Fettweis plaster or Pavlik harness is associated with complication rates for avascular femoral head necrosis from 2.38–16% [8,9,10]. In recent studies—as an alternative to Fettweis plaster and Pavlik harness—a successful treatment of unstable hip types with the Tübingen splint was shown [11, 12].

Tübingen splint
Standard ultrasound examination of the hip joint according to Graf is possible from the first month after birth. As the reproducebility of ultrasound decreases with age, after the sixth month of age radiological controls of dysplastic hips are recommended [13]. Previous X-ray controls are not useful because of yet unossified structures like the femoral head [14]. By various lines (e.g., Hilgenreiner line, Perkins line, Shenton Menard line) and angles [e.g., acetabular (AC) angle and center edge angle] assessment and graduations of the hip pathology can be performed on radiographs (Fig. 2). For investigations and classification of dysplastic hips, the determination of the acetabular angle has proven to be valid and reproducible (Fig. 3) [15]. Here, an angle along the Hilgenreiner line and the acetabular roof is measured. For the Tönnis classification of abnormalities based on the acetabular angle, age, side of dysplastic hips and gender has to be recognized: (1) normal findings (< 1 s), (2) slightly dysplastic hips (1–2 s) and (3) severely dysplastic hips (> 2 s) are differentiated (s = standard deviation) [16].

Pelvic X-ray of a 5 year old girl. Horizontal line Hilgenreiner line (a); vertical lines Perkins lines (b); line below the left femoral neck Shenton Menard line (c); acetabular (AC) angle right (asterisk) and center edge angle left hip (hash)

a Pelvic X-ray of a 16 month old child (initial sonografic hip type D right and IIIa left) with AC-angle right: 28.0° (1–2 s) and left: 32.5° (2 s); b Pelvic X-ray with 39 months with: AC-angle right: 22.2° (< 1 s) and left: 19.2° (< 1 s)
To the best knowledge of the authors at this time, there are no studies that show mid- and long-term results of unstable hips after treatment with the Tübingen splint.
We report on results based on X-ray parameter of initially unstable hips after successful treatment with the Tübingen splint with a follow-up X-ray at the age of 12–24 and 24–48 months.
Materials and methods
Patients
104 of initial 109 unstable hips (type D: n = 51; type III: n = 46; type IV: n = 12) treated with the Tübingen splint could be transferred in a type I hip according to Graf (success rate 95.4%). There were 5 failures (4.6%): 1 hip type III and 4 type IV, which were successfully treated with Fettweis plaster afterwards [12]. In our department, the Tübingen splint is used as a reduction device and the newborns had to wear the splint initially 24 h per day/7 days per week.
In the period from 01/2003 to 08/2016 anonymised data for 83 successfully converted unstable hips (type D: 38, type III: 38, type IV: 7) were included in the study. Age at baseline was treatment start ≤ 6 weeks. The patients had no limitation of abduction.
Patients with secondary hip dysplasia—e.g., children with infantile cerebral palsy or other neuromuscular diseases—were excluded. The presence of a routine pelvic X-ray control at the age of 12–24 and 24–48 months was mandatory for this study.
Methods
Measurements were taken from routine X-ray controls at the age of 12–24 and 24–48 months of patients after successful treatment with the Tübingen Splint. We evaluated: (1) average age at first and second X-ray control, (2) the AC-index according to the Tönnis classification and subdivided into: normal findings (< 1 s), slightly dysplastic findings (1 s-2 s) and severely dysplastic findings (> 2 s).
Avascular necrosis of the femoral head were determined according to the Kalamchi and MacEwen classification into type I–IV.
Statistical analysis
Results are presented as mean ± SEM. Statistical significance was calculated by the unpaired Student’s t test, using IBM SPSS statistics version 22.
Results
There were 60 patients with 83 unstable hips [bilateral: n = 23 (27.7%)] who had a routine pelvic X-ray in second year of life (mean: 14.7 month, SD: 2.2, range 12–22 months) and at the age of 24–48 months (mean: 31.2 months, SD: 6.0, range 22–48 months).
The X-ray results at the age of 12–24 months showed normal findings in 45 hips (54.2%; initial hip type D: 47.4%, III: 63.2%, IV: 42.9%). However, 28 hips (33.7%; initial hip type D: 34.2%, III: 31.6%, IV: 42.9%) were slightly and 10 hips (12.0%; initial hip type D: 21.1%, III: 5.3%, IV:14.3%) were severely dysplastic (Figs. 4, 5, 6).

a Newborn with hip type IV left (arrow); b pelvic X-ray after 12 months with AC-angle right: 19.3° (< 1 s) and left: 26.8° (1–2 s); c pelvic X-ray after 25 months with: AC-angle right: 19.7° (< 1 s) and left: 24.0° (1–2 s)

First X-ray control 12–24 months (AC-angle according to Tönnis classification), n = 83: normal findings (< 1 s): 54.2%; slightly dysplasia (1–2 s): 33.7%; severely dysplasia (2 s): 12.0%

AC angle in degree (°) after 12–24 months. Light gray diamonds: normal findings (45), dark gray diamonds: slightly dysplastic (28), red diamonds: severely dysplastic (10), n = 83
At the second time point at the age of 24–48 months normal findings were seen in 61 hips (73.5%; initial hip type D: 68.4%, III: 81.6%, IV: 85.7%), slightly dysplasia in 19 hips (22.9%; initial hip type D: 28.9%, III: 15.8%, IV: 14.3%) and severely dysplasia in 3 hips (3.6%; initial hip type D: 2.6%, III: 2.6%, IV:14.3%) (Figs. 7, 8).

Second X-ray control 24–48 months (AC-angle according to Tönnis classification), n = 83: normal findings (< 1 s): 73.5%; slighlty dysplasia (1–2 s): 22.9%; severely dysplasia (2 s): 3.6%

AC angle in degree (°) after 24–48 months. Light gray diamonds: normal findings (61), dark gray diamonds: slightly dysplastic (19), red diamonds: severely dysplastic (3), n = 83
In comparison of pelvic X-rays in second year of life versus second to fourth year of life, there was total increase of normal findings of 35.6%. Interestingly, 6.7% (2 hip type D, 1 hip type III) of patients with initially normal findings deteriorated into slightly dysplastic hips, one hip (2.2%, hip type IV) even deteriorated into a severely dysplastic finding. A total decrease of slightly dysplastic hips by 32.1% was seen between the two time points. Here 32.1% of initially slightly dysplastic hips show constant slightly dysplasia and 67.9% improved in normal findings. In comparison of severely dysplastic findings a decrease of 70.0% was noticed. Here 60.0% of severely dysplastic findings improved into slightly dysplastic findings, 20.0% were constant severely dysplastic and 20.0% improved in normal findings (Fig. 9).

Comparison of first X-ray versus second X-ray, n = 83, improvement of 19 slightly dysplastic hips and 6 severely dysplastic hips into normal findings, 2 severely dysplastic hips into slightly dysplastic hips, deterioration of 4 normal findings (3 slightly dysplasia and 1 severely dysplasia)
In two cases (2.4%) an avascular necrosis of the femoral head type I was seen (both hip type IV).
In addition, the contralateral hip joints with stable hip types I–IIc (n = 37) were also examined. At the first time point (12–24 months) 29 hips showed normal findings (78.4%) and 8 were slightly dysplastic (21.6%). The X-ray results at the age of 24–48 months showed normal findings in 35 hips (94.6%) and slightly dysplasia in 2 cases (5.4%). Here one normal finding deteriorated.
In none of the patients an operative intervention was performed at the end of the X-ray examinations. In one case (severely dysplastic hip) an operative intervention and for the two other severely dysplastic hips close controls were recommended.
Discussion
After ultrasound controlled transfer into stable hips, the development of a normal cartilaginous joint is possible. Normally dysplastic but stable hip joints were controlled or were treated which various splints, e.g., Tübingen splint. Unstable hips were usually treated with plaster casts in human position, e.g., Fettweis plaster or with the Pavlik harness [17,18,19,20]. However, in certain cases, the Tübingen splint could be used as alternative therapy possibility even for unstable hips. In our department, for example, unstable hips—with age at start of treatment ≤ 6 weeks and without limitation in abduction—were treated with the Tübingen splint. Advantages of this splint are easy handling, adjustment according to growth in size and easy cleaning compared to other harness’ and splints. Therefore, the Tübingen splint has a high parents compliance. Here we show similarly good results in comparison to other studies [11]. However, with each therapy, the bony remodeling and maturation is delayed in comparison to the cartilaginous remodeling. Therefore, various studies show the need of regular X-ray controls to detect and possibly treat residual hip dysplasia in an early stage [21,22,23]. To classify hip dysplasia, the Tönnis classification has been proven successfully [24]. In this context, our study supports previous conclusions that it is necessary to regularly control the children to confirm regular development of the hip joint. Previous studies show that it is essential to regularly evaluate development of the hip joint until the maturation of the musculoskeletal system [25]. Follow-up controls are mandatory since bone maturation is delayed and secondary instability and/or delay in bone remodeling may lead to recurrence of dysplasia and necessity of surgical correction. Symptoms will occur very late and prevention of irreversible damage to acetabular cartilage can only be achieved by surgical interventions. After successful treatment of unstable hips with the Pavlik harness residual dysplasia was seen in 5–34% [21, 22, 26]. In these cases, studies with X-ray follow-up are needed to detect residual hip dysplasia.
The risk of radiation-induced cancer (2 pelvic X-ray) compared to naturally occurring cancer appears to be less than 1 per million [21]. However, other studies prefer the start of X-ray controls after the second year of life to reduce the radiation exposure [27]. The Kalamchi and MacEwen classification is a well-accepted tool for determination and classification of AVN [28]. We detected two out of 83 hips (2.4%) with avascular necrosis of the femoral head according to the Kalamchi and MacEwen classification at the end of 4th year of life. In comparison to other studies our results of unstable hips treating with the Tübingen splint show a low AVN rate of 2.4% (8–10). But these comparisons are limited because of different patient groups which were included in the studies—explicitly owing to age at diagnosis, age at treatment and different hip types. In our study, an operative intervention was not performed after completion of the second X-Ray but one surgical intervention and closed controls for the 3 severely dysplastic hips were recommended.
Conclusion
This is the first study to show that treatment with the Tübingen splint, even in unstable hips has results, that are comparable to treatment with Fettweis plaster or Pavlik harness. But our mid-term follow-up data also shows that despite successful therapy with the Tübingen splint unstable hips need regular X-ray follow-up controls to observe the development of all hip joints and to detect those which might need surgical correction of residual dysplasia. We recommend that even after treatment with the Tübingen splint regular X-ray controls should be performed.
References
Farr S, Grill F, Müller D (2008) When is the optimal time for hip ultrasound screening?. Orthopade 37(6):532 (534–6, 538–540)
Grill F, Müller D (1997) Results of hip ultrasonographic screening in Austria. Orthopade 26(1):25–32
Graf R (2017) Hip sonography: background; technique and common mistakes; results; debate and politics; challenges. Hip Int J Clin Exp Res Hip Pathol Ther 27(3):215–219
Katthagen BD, Mittelmeier H, Becker D (1988) Incidence and start of inpatient treatment of pediatric hip dislocations in West Germany. Z Orthop Ihre Grenzgeb 126(5):475–483
Bernau A (1990) The Tübingen hip flexion splint in the treatment of hip dysplasia. Z Orthop Ihre Grenzgeb 128(4):432–435
Fettweis E (1968) Sit-crouch-position-plaster in hip joint dysplasies. Arch Orthop Unfallchir 63(1):38–51
Pavlik A (1957) Method of functional therapy with strap braces as a principle of conservative therapy of congenital dislocation of the hip in infants. Z Orthop Ihre Grenzgeb 89(3):341–352
Bensahel H, Csukonyi Z, Huguenin P (1988) Vascular disorders of the proximal femur following treatment of congenital hip dislocation. Arch Orthop Trauma Surg Arch Orthopadische Unf-Chir 107(6):372–376
van der Sluijs JA, De Gier L, Verbeke JI, Witbreuk MMEH., Pruys JEH, van Royen BJ (2009) Prolonged treatment with the Pavlik harness in infants with developmental dysplasia of the hip. J Bone Joint Surg Br 91(8):1090–1093
Walton MJ, Isaacson Z, McMillan D, Hawkes R, Atherton WG (2010) The success of management with the Pavlik harness for developmental dysplasia of the hip using a United Kingdom screening programme and ultrasound-guided supervision. J Bone Joint Surg Br 92(7):1013–1016
Seidl T, Lohmaier J, Hölker T, Funk J, Placzek R, Trouillier HH (2012) Reduction of unstable and dislocated hips applying the Tübingen hip flexion splint? Orthopade 41(3):195–199
Kubo H, Pilge H, Weimann-Stahlschmidt K, Stefanovska K, Westhoff B, Krauspe R (2017) Use of the Tübingen splint for the initial management of severely dysplastic and unstable hips in newborns with DDH: an alternative to Fettweis plaster and Pavlik harness. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-017-2827-3
Lehmann HP, Hinton R, Morello P, Santoli J (2000) Developmental dysplasia of the hip practice guideline: technical report. Committee on quality improvement, and subcommittee on developmental dysplasia of the hip. Pediatrics 105(4):E57
Starr V, Ha BY (2014) Imaging update on developmental dysplasia of the hip with the role of MRI. AJR Am J Roentgenol 203(6):1324–1335
Schrading S, Schulze A (2016) Preoperative diagnostic imaging and planning. Orthopade 45(8):644–652
Tönnis D (1997) Röntgenuntersuchung und arthrographie des Hüftgelenks im Kleinkindesalter. Orthopade 26(1):49–58
Sochart DH, Paton RW (1996) Role of ultrasound assessment and harness treatment in the management of developmental dysplasia of the hip. Ann R Coll Surg Engl 78(6):505–508
Allington NJ (2015) Successful Pavlik Harness Treatment for Developmental Dysplasia of the Hip and Normal X-Ray at the Age of 2 Years: Is a Longer Follow-up Necessary? J Pediatr Orthop 37(5):328–331
Bian Z, Guo Y, Tian W (2009) Treatment of developmental dysplasia of the hip in children: results of closed reduction and immobilization in hip spica cast. Zhonghua Wai Ke Za Zhi 47(13):1017–1019
Kotlarsky P, Haber R, Bialik V, Eidelman M (2015) Developmental dysplasia of the hip: What has changed in the last 20 years? World J Orthop 6(11):886–901
Sarkissian EJ, Sankar WN, Zhu X, Wu CH, Flynn JM (2015) Radiographic follow-up of DDH in infants: are X-rays necessary after a normalized ultrasound? J Pediatr Orthop 35(6):551–555
Alexiev VA, Harcke HT, Kumar SJ (2006) Residual dysplasia after successful Pavlik harness treatment: early ultrasound predictors. J Pediatr Orthop 26(1):16–23
Tucci JJ, Kumar SJ, Guille JT, Rubbo ER (1991) Late acetabular dysplasia following early successful Pavlik harness treatment of congenital dislocation of the hip. J Pediatr Orthop 11(4):502–505
Miao M, Cai H, Hu L, Wang Z (2017) Retrospective observational study comparing the international hip dysplasia institute classification with the Tonnis classification of developmental dysplasia of the hip. Medicine (Baltimore) 96(3):e5902
Modaressi K, Erschbamer M, Exner GU (2011) Dysplasia of the hip in adolescent patients successfully treated for developmental dysplasia of the hip. J Child Orthop 5(4):261–266
Cashman JP, Round J, Taylor G, Clarke NMP (2002) The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. J Bone Jt Surg Br 84(3):418–425
Dornacher D, Cakir B, Reichel H, Nelitz M (2010) Early radiological outcome of ultrasound monitoring in infants with developmental dysplasia of the hips. J Pediatr Orthop Part B 19(1):27–31
Demirhan M, Dikici F, Eralp L, Onen M, Göksan B (2002) A treatment algorithm for developmental dysplasia of the hip for infants 0 to 18 months of age and its prospective results. Acta Orthop Traumatol Turc 36(1):42–51
Funding
No funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All Authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards (Ethics committee vote of the University of Dusseldorf, study no. 4949).
Rights and permissions
About this article

Cite this article
Kubo, H., Pilge, H., Nepp, K. et al. Development of unstable hips after treatment with the Tübingen splint: mid-term follow-up of 83 hip joints. Arch Orthop Trauma Surg 138, 629–634 (2018). https://doi.org/10.1007/s00402-018-2882-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-018-2882-4