
Abstract
Hypothesis
Subtalar instability is thought to be one of the possible causes for chronic functional instability of the foot and ankle. The purpose of this study was to determine the extent of ligament injury that is followed by subtalar instability and to depict consecutive pathologic joint motion.
Methods
Twelve fresh human cadaver lower legs were investigated with respect to pathologic motion and mobility of the subtalar joint in a modified spinal column simulator after arthrodesis of the talocrural articulation and selective sectioning of the lateral ligaments of the subtalar joint. In order to simulate several injury mechanisms, ligaments were dissected starting anteriorly in group one (n = 6) and posteriorly in group two (n = 6).
Results
Dissection of the bifurcate ligament in group one resulted in a significant increase in plantar- and dorsiflexion, dissection of the inferior extensor retinaculum resulted in a significant increase in eversion and inversion. Additional dissection of the lateral talocalcaneal ligament resulted in a significant increase in internal and external rotation. Dissection of the calcaneofibular ligament in group two was followed by significant kinematic changes regarding all degrees of motion in the subtalar joint.
Conclusions
The calcaneofibular ligament plays a key role in lateral stabilisation of the subtalar joint. Therefore, ligaments of the subtalar joint should be included in surgical repair.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The subtalar joint plays a fundamental role in the transmission of loads between the leg and the foot [41]. Soft tissue trauma from inversion of the ankle most commonly involves the ligamentous structures of the lateral aspect of the ankle and sinus tarsi. These injuries can result in severe pain and/or instability of the ankle and subtalar joint [30]. In 20–40% of all cases, an acute lesion of the lateral ligaments of the ankle develops into chronic ankle instability [29, 46, 47]. Lateral ankle instability is frequently accompanied by subtalar instability. The latter can also appear as an isolated problem [20]. Ankle instability and sinus tarsi syndrome must be ruled out in cases of subtalar instability, since these syndromes can appear with similar symptoms [19, 21, 25]. Ankle and subtalar joint instability should be addressed separately in the clinical setting [33].
Subtalar instability occurs in 10–25% of patients suffering from lateral ankle instability [27]. The exact aetiology of subtalar instability is still discussed controversially [19]. Subtalar instability was first mentioned as a separate clinical entity in 1962, when Rubin and Witten [33] suggested a clinical significance of subtalar instability and proposed a radiographic method for evaluating the degree of instability. Diagnosis of subtalar instability remains difficult both clinically and radiographically [7, 17, 21, 29, 30, 51, 52].
Elements of the triple joint complex including the talocalcaneal joint, the calcaneocuboideal joint and the talonavicular joint are closely linked biomechanically and functionally [1, 11]. There are different concepts about the function of the single ligaments at the subtalar joint. Smith and Cahill [5, 39] have supposed that the interosseous talocalcaneal ligament is not important for the stabilisation of the subtalar joint. Knudson et al. [26] have shown experimentally that this ligament contributes substantially to supination stability, but not appreciably to pronation stability. Others have stated that the calcaneofibular ligament plays a key role in providing lateral stability to the subtalar joint [19]. In 1977, Brantigan et al. [3] documented a lateral instability in the subtalar joint by stress tomography in three patients, who were not treated for rupture of the calcaneofibular ligament.
It remains cryptic, which ligament injury in particular results in a relevant clinical subtalar instability. Therefore, the following questions are addressed in this study: Does a dissection of one of the mentioned ligaments cause a significant increase in rotation of the ankle compared to the intact joint? Does dissection of certain ligaments result in pathological kinematic in the subtalar joint?
Materials and methods
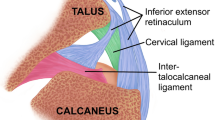
Twelve fresh human cadaver lower legs were amputated 13 cm above the ankle. Exclusion criteria were obvious joint abnormalities, injuries or arthritic changes on the lateral radiograph. Selective dissection of the lateral ligaments of the subtalar joint was then performed after dedicated anatomical preparation by an anatomist. Soft tissues were removed 10 cm distally from the amputation level. The proximal tibia and fibula were embedded into a cylinder of polymethylmetacrylate (PMMA, Technovit 3040, Heraus Kulzer GmbH, Wehrheim, Germany) to ensure a perpendicular alignment of the lower leg to the surface of the cylinder. The cylinder was connected to an adaptor for fixation in the upper part of a movement simulator. The lateral ligaments of the subtalar joint were prepared. The bifurcate ligament, the inferior extensor retinaculum, the interosseous talocalcaneal ligament, the lateral talocalcaneal ligament and the calcaneofibular ligament were identified and marked with soft straps (Fig. 1). To prevent movements in the ankle joint, an arthrodesis in a neutral position with crossing 4.5 mm malleolar screws was performed. Screw position was confirmed by standard anteroposterior and lateral radiographs.

a The prepared ligaments at the lower ankle joint are marked with coloured soft straps: blue calcaneofibular ligament, white lateral talocalcaneal ligament, red inferior extensor retinaculum, yellow bifurcate ligament. b Shows a close up of the marked ligaments. The interosseous talocalcaneal ligament is not shown, because it can not visualise before cutting the inferior extensor retinaculum
A previously described spinal movement simulator introduced by Wilke [49] was modified to measure ankle kinematics (Fig. 2). It is a biomechanical testing device with electrical stepper motors exerting defined-pure momentums on mono- and poly-segmental preparations. This simulator consisted of a fixed platform on which a gimbal (cardanic joint) moved freely. The tibia and fibula of the test specimen were fixed to the platform. The calcaneus was fixed to the gimbal. The simulator thus allowed a completely unrestricted range of motion. Three computer-controlled electric motors within the gimbal controlled specific rotations around each of the three orthogonal axes.

Prepared foot with the highlighted ligaments in the spinal column simulator
Symmetrical movements like plantar-/dorsi-flexion, inversion/eversion and internal/external rotation could be produced. The applied forces and moments were registered with a six component load cell (Schunk, Lauffen/Neckar, Germany) as described previously [49]. During each measurement, rotation was performed around one axis only. The chosen torques were ±2.5 Nm for plantar-/dorsi-flexion (rotation in the sagittal plane) and inversion/eversion (rotation in the frontal plane), and ±10 Nm for external/internal rotation (rotation in the transverse plane). Three loading cycles for each principal direction were necessary to determine the angular kinematics. The first two cycles always produced an angle slightly lower than the maximum angle measured in the third cycle. Measurements beyond the third cycle showed little to no further changes. Thus, only the third cycle of each test was used for the analysis.
Relative motions of the calcaneus against the talus were registered with a three dimensional motion analysis system based on ultrasound sensors (Zebris, Isny, Germany) and recorded by the system software. An ultrasound transmitter and a standard microphone were linked on t-shaped measuring carriers. Space coordinates of every sound transmitter could be determined with a spatial resolution of 0.1 mm. Thus, absolute space positions of the measuring carriers could be calculated. Data was then transferred to a PC workstation at the parallel printer interface. The software calculated the coordinates, angle and translatory motion values with real time presentation on a monitor. Specimens were aligned, in such way, that the center line of the foot was exactly in the longitudinal axis of the leg (y-axis) of the coordinate system. Zero position of the foot was the anatomical neutral-zero-position of the foot. Thus, it was ensured, that the foot was in zero position of the stepper motors and in neutral zero position of the coordinate system. This ultrasound motion analysis system is accurate for angular measurements to 0.2° (0.1%). The joint coordinate system proposed by the International Society of Biomechanics was used [38].
The twelve lower leg specimens were then assigned into two groups. For simulating several injury mechanisms, ligaments were dissected from anterior to posterior, beginning with the bifurcate ligament, followed by the inferior extensor retinaculum, the interosseous talocalcaneal ligament, the lateral talocalcaneal ligament and calcaneofibular ligament in group one (n = 6). In group two (n = 6), ligaments were dissected from posterior to anterior, beginning with the calcaneofibular ligament, followed by the lateral talocalcaneal ligament, the inferior extensor retinaculum, the interosseous talocalcaneal ligament and the bifurcate ligament. The sequential ligament transection was utilised to assess relative contributions of the subtalar ligaments to the subtalar stability. Three dimensional range of motion was measured in the native condition and after dissection of each ligament. Specimens were kept moist throughout the experiment with 0.9% saline solution.
The maximum range of motion for each joint and each of the rotational axes was then measured. The range of motion obtained for each experimental condition was divided by the value obtained from the intact joint to normalise the data. Normalised values were then averaged across all specimens. Single data of the joint with dissected ligaments and data of the intact joint were compared and analysed with the Friedman test and the Wilcoxon test. The significance level was defined as P < 0.05.
Results
Measurements of the range of motion are summarised in Tables 1 and 2 for both the groups.
In group one (dissection from anterior to posterior), dissection of the bifurcate ligament lead to a significant increase of plantar- and dorsi-flexion (P = 0.028). Dissection of the inferior extensor retinaculum resulted in a significant increase of eversion and inversion (P = 0.046). Additional dissection of the lateral talocalcaneal ligament was followed by a significant increase of internal and external rotation (P = 0.028; Fig. 3).

Pathological movement in the hind foot is shown after gradual separation of the ligaments in proportion to the native condition in group one. The range of motion obtained for each experimental condition was divided by the value obtained in the native condition (NA = 1) to normalise the data. NA Native condition, BL bifurcate ligament, IER inferior extensor retinaculum, ITCL interosseous talocalcaneal ligament, LTCL lateral talocalcaneal ligament, CFL calcaneofibular ligament. Asterisk indicates statistical significant differences in comparison to the native condition
In group two (dissection from posterior to anterior), dissection of the calcaneofibular ligament lead to a significant change of overall joint kinematics, i.e. it altered all motion directions in the subtalar joint. Thus, it developed a relevant subtalar instability (P = 0.028; Fig. 4).

Pathological movement in the hind foot is shown after gradual separation of the ligaments in proportion to the native condition in group two. The range of motion obtained for each experimental condition was divided by the value obtained in the native condition (NA = 1) to normalize the data. NA Native condition, BL bifurcate ligament, IER inferior extensor retinaculum, ITCL interosseous talocalcaneal ligament, LTCL lateral talocalcaneal ligament, CFL calcaneofibular ligament. Asterisk indicates statistical significant differences in comparison to the native condition
Discussion
Subtalar joint motion is complex and occurs in three planes [22, 26, 35]. The subtalar joint plays a key role in adapting the foot to the ground [41]. The complex anatomy of the subtalar joint makes depiction and assessment of ligament injuries of this joint particularly troublesome [50]. Injuries of the subtalar joint are frequently associated with injuries of both the talotibial and talofibular articulation [19]. Subtalar instability can be defined as chronic functional instability with increased values of talar tilt and talocalcaneal displacement as measured with standardised stress radiographs [19]. In cases of chronic ankle instability, subtalar instability has to be ruled out and assessed separately [52]. Because both mechanism and symptoms of ankle and subtalar instability are similar, the latter is frequently overlooked in the presence of the former [50]. Chronic subtalar instability results in pathological kinematics of the subtalar joint complex that may lead to early-onset posttraumatic osteoarthritis [2]. Even minimal pathological movements and repetitive ankle sprains almost certainly lead to early joint wear [2].
The inferior extensor retinaculum was described by Stephens and Sammarco [42] to play a significant role in subtalar joint stability in neutral and dorsiflexion positions. It is a ligamentous structure consisting of three roots, the lateral, intermediate and medial root. The lateral root attaches to the lateral aspect of the tarsal sinus and blends with the inferior peroneal retinaculum at the superolateral margin of the calcaneus. The intermediate root attaches just medially to it. The medial root diverges from the inferior extensor retincaculum and enters the depths of the tarsal sinus and anterolateral aspect of the tarsal canal branching into the medial, lateral and talar components [18]. The function of the inferior extensor retinaculum is to serve as a pulley for the extensor tendons [18]. The present study suggests that the inferior extensor retinaculum is also important for the inversion and eversion of the foot (Fig. 3).
The calcaneofibular ligament provides lateral stability for both the ankle and subtalar joint. The calcaneofibular ligament runs from the anterior part of the end of the lateral malleolus [53]. It is rarely injured solely. It usually occurs with a lesion of the anterior talofibular ligament. Rupture of this ligament is reported to result in an increase of motion in the subtalar joint [3, 15]. A subtalar tilt was seen in stress radiographs after dissection or rupture of the calcaneofibular ligament [7, 28]. Isolated sectioning of the calcaneofibular ligament of cadaver ankles resulted in a 5 mm tilt of the calcaneus in the subtalar joint [15]. Dissection of the calcaneofibular ligament results in a significant increase in the external rotation at the talocalcaneal joint with a maximum of 2.9° [23]. Some authors have shown a stabilizing function of the calcaneofibular ligament during inversion in the subtalar joint [24]. This is in accordance with our results, since we have seen a significantly wider range of motion after dissection of the calcaneofibular ligament in all three planes (Fig. 4). The lateral talocalcaneal ligament was found to merge into the calcaneofibular ligament, whereas it originates from the lateral tubercle of the talus, runs obliquely inferiorly and posteriorly and attaches to the lateral surface of the calcaneus [41].
The bifurcate ligament stabilizes both the anterior portion of the subtalar joint (the talocalcaneonavicular joint) and the midtarsal (Chopart’s) joint. The common origin of both the calcaneonavicular and calcaneocuboidal parts of the bifurcate ligament is located at the dorsal aspect of the anterior process of the calcaneus. According to Schmidt and Grünwald [36], the calcaneonavicular part is stronger (average diameter of 3 mm) and longer (average length of 15 mm) than the calcaneocuboidal part (2 mm in diameter and 9 mm in length).
The interosseous talocalcaneal ligament attaches to the bottom of the sinus tarsi, runs oblique superiorly, posteriorly and laterally to the posteroinferior articular facet of the talus [41]. A cadaveric study indicated that the interosseous talocalcaneal ligament contributes substantially to supination stability, but not to pronation stability [26]. Another study pointed out that interosseous talocalcaneal ligament failure causes inversion instability of the subtalar joint [44]. Another cadaveric experimental study demonstrated that a combined injury of the anterior talofibular ligament and the interosseous talocalcaneal ligament can induce anterolateral rotatory instability of the ankle joint [45]. After dissection of the interosseous talocalcaneal ligament, the dorsiflexion of the talocalcaneal joint increased to 43% [22].
In vitro and clinical studies showed that reconstruction of the calcaneofibular and anterior talofibular ligament lead to more favourable results than reconstruction of the anterior talofibular ligament alone, especially if there is a relevant instability of the subtalar joint [4, 8, 9, 16]. If the ends of the ligaments are too weak and reconstruction of the lateral ligaments is not possible, the use of local autograft tissue is necessary [43]. The periosteal flap reconstruction is therefore favoured by many authors as the gold standard, since it resembles an anatomical reconstruction [12, 32, 43]. Alternatively, the plantaris tendon may be used as a free tendon graft [35]. Others have applied free tendon transfers and extra-anatomical tenodeses [6, 10, 13, 14, 27, 31, 34, 37, 40, 48].
However, there are some limitations on this study. First, it is an in vitro study. Normal motion of the foot is a combination of different axis and normally not around a single axis. Secondly, proprioception, which has an influence on the stability of the subtalar joint, cannot be assessed in a cadaver study. Therefore, results of this study cannot directly be transferred to the in vivo situation. Additionally, the result of the ligament dissection can depend on the order of the dissection performed. We have chosen this particular dissection design, since isolated ligament ruptures are rare and only a combination of ligament dissection showed a relevant increase of motion (Table 1, external/internal rotation).
This study clarifies the mechanical relevance of each of the lateral ligaments of the subtalar joint. In conclusion, the calcaneofibular ligament is a key for lateral subtalar stability. Dissection of this ligament results in significant increase of all three motion planes (Table 2). This ligament should be reconstructed in cases of chronic instability of the subtalar joint or combined ankle and subtalar instability. Dissection of the bifurcate ligament lead to significant increase of plantar-/dorsi-flexion. Additional dissection of the inferior extensor retinaculum results in significant increase of inversion/eversion and further dissection of the lateral talocalcaneal ligament produces significant increase of internal/external rotation.
References
Astion DJ, Deland JT, Otis JC, Kenneally S (1997) Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 79:241–246
Becker HP, Rosenbaum D (1999) Chronisch-rezidivierende Bandinstabilitäten am lateralen Sprunggelenk. Orthopäde 28:483–492
Brantigan JW, Pedegana LR, Lippert FG (1977) Instability of the subtalar joint Diagnosis by stress tomography in three cases. J Bone Joint Surg Am 59:321–324
Brunner R, Gächter A (1991) Repair of fibular ligaments: comparison of reconstructive techniques using plantaris and peroneal tendons. Foot Ankle 11:359–367
Cahill DR (1965) The anatomy and function of the contents of the human tarsal sinus and canal. Anat Rec 153:1–17
Chrisman OD, Snook G (1969) Reconstruction of lateral ligament tears of the ankle: an experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg 51-A:904–912
Clanton TO (1989) Instability of the subtalar joint. Orthop Clin North Am 20:583–592
Colville MR, Grondel RJ (1995) Anatomic reconstruction of the lateral ankle ligaments using a split peroneus brevis tendon graft. Am J Sports Med 23:210–213
Colville MR (1995) Reconstruction of the lateral ankle ligaments. Instr Course Lect 44:341–348
Elmslie DL (1934) Recurrent subluxation of the ankle. Ann Surg 100:364–367
Fellmann J, Zollinger H (1996) Versteifungseingriffe am unteren Sprunggelenk-wechselnde Konzepte im Wandel der Zeit. Z Orthop Ihre Grenzgeb 134:341–345
Glas E, Paar O, Smasal V, Bernett P (1985) Die Periostlappenplastik (PLP) am Außenbandapparat des oberen Sprunggelenkes. Unfallchirurg 88:219–222
Gould N, Seligson D, Gassman J (1980) Early and late repair of lateral ligament of the ankle. Foot Ankle Int 1:84–89
Harper MC (1991) The lateral ligamentous support of the subtalar joint. Foot Ankle Int 11:319–325
Heilman AE, Braly WG, Bishop JO, Noble PC, Tullos HS (1990) An anatomic study of subtalar instability. Foot Ankle 10:224–228
Hollis JM, Blasier RD, Flahiff CM, Hofmann OE (1995) Biomechanical comparison of reconstruction techniques in simulated lateral ankle ligament injury. Am J Sports Med 23:678–682
Ishii T, Miyagawa S, Fukubayashi T, Hayashi K (1996) Subtalar stress radiography using forced dorsiflexion and supination. J Bone Joint Surg Br 78:56–60
Jotoku T, Kinoshita M, Okuda R, Abe M (2006) Anatomy of ligamentous structures in the tarsal sinus and canal. Foot Ankle Int 27(7):533–538
Karlsson J, Eriksson BI, Renström PA (1997) Subtalar ankle instability. A review. Sports Med 24:337–346
Karlsso J, Eriksson BI, Renström P (1998) Subtalar instability of the foot. A review and results after surgical treatment. Scand J Med Sci Sports 8:191–197
Kato T (1995) The diagnosis and treatment of instability of the subtalar joint. J Bone Joint Surg Br 77:400–406
Kjaersgaard-Andersen P, Wethelund JO, Helmig P, Soballe K (1988) The stabilizing effect of the ligamentous structures in the sinus and canalis tarsi on movements in the hindfoot An experimental study. Am J Sports Med 16:512–516
Kjaersgaard-Andersen P, Wethelund JO, Helmig P, Nielsen S (1987) Effect of the calcaneofibular ligament on hindfoot rotation in amputation specimens. Acta Orthop Scand 58:135–138
Kjaersgaard-Andersen P, Wethelund J-O, Nielsen S (1987) Lateral talocalcaneal instability following section of the calcaneofibular ligament. Foot Ankle 7:355–361
Klenerman L (1998) The management of sprained ankle. J Bone Joint Surg Br 80:11–12
Knudson GA, Kitaoka HB, Lu CL, Luo ZP, An KN (1997) Subtalar joint stability Talocalcaneal interosseous ligament function studied in cadaver specimens. Acta Orthop Scand 68:442–446
Larsen E (1988) Tendon transfer for lateral ankle and subtalar joint instability. Acta Orthop Scand 59:168–172
Laurin CA, Quellet R, St-Jacques R (1968) Talar and subtalar tilt: an experimental investigation. Can J Surg 11:270–279
Louwerens JW, Ginai AZ, van Linge B (1995) Stress radiography of the talocrural and subtalar joints. Foot Ankle Int 16:148–155
Mabit C, Boncoeur-Martel MP, Chaudruc JM, Valleix D, Descottes B, Caix M (1997) Anatomic and MRI study of the subtalar ligamentous support. Surg Radiol Anat 19:111–117
Pisani G (1996) Chronic laxity of the subtalar joint. Orthopedics 19:431–437
Rosenbaum D, Engelhardt M, Becker HP, Claes L, Gerngross H (1999) Clinical and functional outcome after anatomic and nonanatomic ankle ligament reconstruction: Evans tenodesis versus periosteal flap. Foot Ankle Int 20:636–639
Rubin G, Witten M (1962) The subtalar joint and the symptom of turning over on the ankle: a new method of evaluation utilizing tomography. Am J Orthop 16–19
Sammarco GJ, Idusuyi OB (1999) Reconstruction of the lateral ankle ligaments using a split peroneus brevis tendon graft. Foot Ankle Int 20:97–103
Sarrafian SK (1993) Biomechanics of the subtalar joint complex. Clin Orthop Relat Res 290:17–26
Schmidt HM, Grünewald E (1981) Untersuchungen an den Bandsystemen der talocruralen und intertarsalen Gelenke des Menschen. Gegenbaurs Morphol Jahrb 127:792–831
Schon LC, Clanton TO, Baxter DE (1991) Reconstruction for subtalar instability: a review. Foot Ankle 11:319–325
Siegler S, Chen J, Schneck CD (1988) The three-dimensional kinematics and flexibility characteristics of the human ankle and subtalar joints—part I: kinematics. J Biomech Eng 110:364–373
Smith JW (1958) The ligamentous structures in the canalis and sinus tarsi. J Anat 92:616–620
Smith PA, Miller SJ, Berni AJ (1995) A modified Chrisman–Snook procedure for reconstruction of the lateral ligaments of the ankle: review of 18 cases. Foot Ankle 16:259–266
Stagni R, Leardini A, O’Connor JJ, Giannini S (2003) Role of passive structures in the mobility and stability of the human subtalar joint: a literature review. Foot Ankle Int 24(5):402–409
Stephens MM, Sammarco GJ (1992) The stabilizing role of the lateral ligament complex around the ankle and subtalar joints. Foot Ankle 13:130–136
Thermann H, Zwipp H, Tscherne H (1997) Treatment algorithm of chronic ankle and subtalar instability. Foot Ankle Int 18:163–169
Tochigi Y, Amendola A, Rudert MJ, Baer TE, Brown TD, Hillis SL, Saltzman CL (2004) The role of the interosseous talocalcaneal ligament in subtalar joint stability. Foot Ankle Int 25:588–596
Tochigi Y, Takahashi K, Yamagata M, Tamaki T (2000) Influence of the interosseous talocalcaneal ligament injury on stability of the ankle-subtalar joint complex—a cadaveric experimental study. Foot Ankle Int 21:486–491
van Hellemondt FJ, Louwerens JW, Sijbrandij ES, van Gils AP (1997) Stress radiography and stress examination of the talocrural and subtalar joint on helical computed tomography. Foot Ankle Int 18:482–488
Verhagen RA, de Keizer G, van Dijk CN (1995) Long-term follow-up of inversion trauma of the ankle. Arch Orthop Trauma Surg 114:92–96
Vidal J, Fassio B, Buscayret C, Escare P, Allier Y (1974) Instabilité externe de la cheville. Rev chir Ortoped 60:635–642
Wilke HJ, Claes L, Schmitt H, Wolf S (1994) A universal spine tester for in vitro experiments with muscle force simulation. Eur Spine J 3:91–97
Zwipp H, Rammelt S, Grass R (2002) Ligamentous injuries about the ankle and subtalar joints. Clin Podiatr Med Surg 19:195–229
Zwipp H, Krettek C (1986) Diagnostik und Therapie der akuten und chronischen Bandinstabilität des unteren Sprunggelenkes. Orthopäde 15:472–478
Zwipp H, Tscherne H (1982) Die radiologische Diagnostik der Rotationsinstabilität im hinteren unteren Sprunggelenk. Unfallheilkunde 85:494–498
Zwipp H (1994) Chirurgie des Fußes, 1 edn. Springer, Heidelberg
Acknowledgments
The authors wish to thank Ursula Range for the statistical support as well as Thomas Albrecht for the photographical work.
Conflict of interest statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weindel, S., Schmidt, R., Rammelt, S. et al. Subtalar instability: a biomechanical cadaver study. Arch Orthop Trauma Surg 130, 313–319 (2010). https://doi.org/10.1007/s00402-008-0743-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-008-0743-2