
Abstract
Introduction
Functional instability is defined as a repeated ankle inversion sprain and a giving way sensation. Previous studies have described the damage of sensori-motor control in ankle sprain as being a possible cause of functional instability. The aim of this study was to evaluate the inversion angle replication errors in patients with functional instability after ankle sprain.
Materials and methods
The difference between the index angle and replication angle was measured in 12 subjects with functional instability, with the aim of evaluating the replication error. As a control group, the replication errors of 17 healthy volunteers were investigated. The side-to-side differences of the replication errors were compared between both the groups, and the relationship between the side-to-side differences of the replication errors and the mechanical instability were statistically analyzed in the unstable group.
Results
The side-to-side difference of the replication errors was 1.0 ± 0.7° in the unstable group and 0.2 ± 0.7° in the control group. There was a statistically significant difference between both the groups. The side-to-side differences of the replication errors in the unstable group did not statistically correlate to the anterior talar translation and talar tilt.
Conclusion
The patients with functional instability had the deficit of joint position sense in comparison with healthy volunteers. The replication error did not correlate to the mechanical instability. The patients with functional instability should be treated appropriately in spite of having less mechanical instability.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankle sprain is the most common injury in sporting activities with the rupture of the lateral ankle ligaments [8]. Functional instability has been well discussed in previous reports as the result of ankle sprain [6, 7]. Functional instability is defined objectively as a repeated ankle inversion sprain and subjectively as a “giving way sensation” at the ankle, which might be present in up to 15–60% of patients after ankle sprain [15]. Previous studies have described the damage of sensori-motor control in ankle sprain as being a possible cause of functional instability. The methods, which used to demonstrate this, have included the postural balance test, peroneal muscle reaction time to sudden ankle inversion, peroneal nerve conduction velocity, and joint position sense of the ankle [1–5, 9–14, 16–21, 26, 29]. However, this variety of methods used to evaluate functional instability resulted in a disparity in their results. Moreover, it is unclear that these methods could be always used clinically. It is very important to evaluate the proprioception in patients with functional instability as well as the effect of rehabilitation and orthosis on the unstable ankle. Several studies have shown joint position sense disorder to be caused by a significant difference between the stable ankle and unstable ankle in the inversion angle replication error [9, 14, 19]. The aim of this study was to evaluate the inversion angle replication error in patients with functional instability after ankle sprain using our new methods.
Materials and methods
Participants
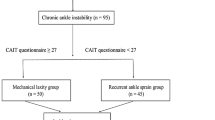
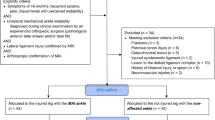
Twelve patients with a history of repeated unilateral ankle sprain participated in this study (unstable group). The patients consisted of six men and six women with an average age of 30.2 years (range 16–35 years). All patients had chronic lateral instability with symptoms of pain, a giving way sensation and some functional disability of the ankle. All patients were diagnosed clinically as having a lateral ankle ligament injury according to the preoperative assessment such as stress radiography, MRI, and subsequently underwent the anatomic repair of the ATFL using the Broström technique or reconstruction using a free gracilis tendon graft. ESSKA CONSENSUS 1990 activity score was used as the evaluation activity level during the period from injury to the surgical treatment (Table 1) [26].
Seventeen healthy individuals (12 males, 5 females) who did not have a history of ankle sprain or any ankle pain, participated in this study as the control group. Their median age was 28.1 years (range 22–34 years).
Mechanical instability
Stress radiography for anterior talar translation and talar tilt was performed with manual max force. The same physician performed all stress radiographies. The distance from the joint surface of the talus to the posterior articular tip of the tibia was measured as the distance of anterior talar translation. The talar tilt was measured as the angle between the horizontal skeletal joint surfaces of the talus and the tibia.
Measurements of ankle joint position sense
The subjects were placed in a sitting position with the knee flexed at 70°. Each subject took off shoes and socks, and placed the foot on a goniometer footplate (Nakamura brace Co., Shimane, Japan) with the ankle at 20° planter flexion (Fig. 1). The goniometer footplate can rotate internally, which indicates that the pivot of foot movement is aligned approximately with the axis of inversion movement. The center of rotation of the goniometer footplate is just below the tuberosity of the calcaneus. Subjects were blindfolded to eliminate visual input and to facilitate concentration during testing, and they were asked to relax their leg muscles. The foot was passively rotated internally at random to one of six positions (5°, 10°, 15°, 20°, 25°, and 30°), always starting from 0°. The footplate was rotated manually to the index angle in approximately 1 s, and held in position for 5 s. Then the ankle was returned to the 0° position. After that, the subjects moved their ankle to match the previous test angle actively. The difference between the index angle and replication angle was recorded as the replication error. Each angle was repeated twice and the replication errors were measured in both the ankles.

Measurement of the replication errors. The foot without shoes and socks was placed on a goniometer footplate with the ankle at 20° planter flexion. The goniometer footplate can rotate internally, which indicates that the pivot of foot movement was aligned approximately with the axis of inversion movement
Evaluation
Comparison of the side-to-side differences of the replication errors between both groups
The side-to-side differences of the replication errors in the unstable group were compared with that in the control group.
The relationship between the mechanical instability and replication errors in the unstable group
The relationship between the side-to-side differences of the replication errors and the anterior talar translation and talar tilt were statistically analyzed, respectively.
Statistical analysis
Differences between the two groups were calculated using Student’s t test for dependent variables. A P-value of less than 0.05 was considered significant. Pearson’s correlation coefficients test was used to calculate the relationship between the side-to-side differences of the replication errors and the anterior talar translation and talar tilt.
Results
Comparison of the side- to-side differences between both the groups
The replication error of the unstable ankle was 3.4 ± 1.0° and that of the stable ankle was 2.3 ± 0.9° in the unstable group. There was a statistically significant difference between the unstable and stable ankles in the unstable group (Table 2). The replication error of the right ankle was 2.3 ± 0.8° and that of the left ankle was 2.1 ± 0.6° in the control group. There was no significant difference between both the ankles. The side-to-side difference of the replication errors in the unstable group was 1.0 ± 0.7° and was 0.2 ± 0.7° in the control group. There was also a statistically significant difference between both the groups (Fig. 2).

Comparison of the side-to-side differences of the replication errors between both the groups. The side-to-side difference of the replication errors in the unstable group was 1.0 ± 0.7° and was 0.2 ± 0.7° in the control group. There was a statistically significant difference between both the groups
The relationship between the mechanical instability and proprioceptive differences in the unstable group
The mean side-to-side differences of the anterior talar translation and talar tilt between the unstable and stable ankles were 3.2 ± 2.1 mm and 7.3 ± 4.0°, respectively (Table 2). The side-to-side differences of the replication errors in the unstable group did not statistically correlate to the anterior talar translation (r = −0.509, P = 0.09) and talar tilt (r = −0.11, P = 0.73) (Figs. 3, 4).

The relationship between the side-to-side differences of the replication errors and that of anterior talar translation in the unstable group. The side-to-side differences of the replication errors in the unstable group did not statistically correlate to the anterior talar translation (r = −0.509, P = 0.09)

The relationship between the side-to-side differences of the replication error and that of the talar tilt in the unstable group. The side-to-side differences of the replication errors in the unstable group also did not statistically correlate to the talar tilt (r = −0.11, P = 0.73)
Discussion
The residual chronic ankle instability after ankle sprain is frequently seen in clinical [15]. The cause of chronic ankle instability is not only mechanical instability, which is defined as over movement beyond the physiological ankle range of motion, but also as functional instability, which is due to a deficit of sensori-motor control. Freeman et al. [6, 7] described that the functional instability arose from the sensori-motor control deficits. Mechanoreceptors are present in the structures of the lateral aspect of the ankle including the lateral ligaments, capsule, and retinaculum, and the damage of that structure by inversion ankle sprain might result in functional instability [25, 28]. In previous studies, the joint angle replication error has been measured to evaluate the sensori-motor ability of the ankle in patients with functional instability, and a significant difference in inversion replication errors between functionally stable and unstable subjects has been reported [9, 14, 19]. Jerosch et al. [14] described that the mean replication error values for the unstable ankle was 2.52°. Konradsen et al. [19] reported that the replication error value for the unstable ankles was 2.5° and the healthy contralateral side was 2.0° in 23 unilaterally and functionally unstable subjects, and there was a significant difference between the unstable and stable ankle. In the present study, the replication error for the unstable ankle was 3.4 ± 1.0° and was 2.3 ± 0.8° for the stable ankle, which was similar to those of previous reports. The replication errors for the healthy subjects have been reported as being between 1° and 3°, and our result was 2.2°, which is in agreement with the previous reports [9, 14, 19].
In the present study, the replication error in the unstable group did not statistically correlate to the stress radiographs. Several studies have shown a distinct relationship between mechanical instability and functional instability. Lentell et al. [23] reported that the values of the passive movement sense into the inversion and talar tilt for the unstable ankle were significantly greater than that for the stable ankle. However, Konradsen et al. [20] demonstrated that there was no significant difference between the mechanically stable ankle and unstable ankle for values of position sense. Lephart et al. [24] described that the proprioceptive function to prevent a sprain in the mechanically unstable ankle might deviate with abnormal ankle movement beyond the physiological limitation. In our series, some patients with less mechanical instability had a greater degree of replication error. It should be noted that patients without remarkable mechanical instability have functional instability and should be treated appropriately. Halasi et al. [11] reported that surgical treatment could improve the joint position sense of the unstable ankle. The decision to proceed with the surgical treatment should be made according to the evaluation of not only mechanical instability but also the functional instability. The limitation of our study about the relationship between the mechanical instability and functional instability is that the number of patients is small and the measurement of the mechanical instability was not performed using the quantitative measurement device. Further investigation with more numbers of patients using the quantitative measurement device would be required.
In previous studies, functional instability after ankle sprain was evaluated using several methods including the postural sway, joint position sense, peroneal muscle reaction time, and eversion strength [1–5, 9–14, 16–21, 27, 29]. It is documented that postural sway has a strong correlation to functional instability, however, it is unspecific for the unstable ankle with the functional instability [5, 27]. Konradsen et al. [20] investigated ankle eversion strength, joint position sense and peroneal reaction time to sudden inversion after ankle inversion injury. According to their results, the change in joint position sense was the most prominent. Joint position sense was an easy and convenient way to objectively evaluate functional instability. Therefore, we chose to use joint position sense for our evaluation.
A criticism of our study is that, our method does not correctly reproduce the inversion movement. Konradsen et al. [19–21] described the mechanism of repeated ankle sprain as follows. In a normal stride, the foot is brought forward to 10° of inversion and the lateral border of the foot passes just 5 mm above the ground in the late swing phase [30]. A deficit in the ankle joint position sense might increase the inversion angle, which would cause a collision between the lateral border of the foot and the ground surface during this phase, and a small amount of the side-to-side difference of replication error might cause ankle sprain. In our method, it is reasonable to measure the replication error in internal rotation with planter flexion assuming misjudgment of the inversion angle when the foot catches the ground during the late swing phase. The greater degree of the replication error in our method might indicate an increased risk of a collision of the lateral border of the foot with the ground. Additionally, our method is easy and does not require a special device such as a computer or some electronic device. It was very practical to assess the proprioceptive function of the patients with functional instability by our method in the outpatient clinic, rehabilitation room, and so on. Harasi and Kynsburg et al. [11, 22] demonstrated that joint position sense in chronic unstable ankle improved after surgical treatment or proprioceptive training using the slope box test. Further evaluation of the inversion angle replication error after surgical treatment or conservative treatment with proprioceptive training program was needed.
In conclusion, an unstable ankle has the deficit of joint position sense in comparison with a healthy contralateral side in patients with functional instability. The joint position sense in the unstable ankle does not statistically correlate to the mechanical instability, although the number of the present study is small. The measurement of the inversion angle replication error using our method might become the useful tool to assess the functional instability and further studies should be conducted to evaluate the effect of surgical training or of proprioceptive training using our method.
References
Arnold BL, Docherty CL (2006) Low-load eversion force sense, self-reported ankle instability, and frequency of giving way. J Athl Train 41:233–238
Bernier JN, Perrin DH, Rijke A (1997) Effect of unilateral functional instability of the ankle on postural sway and inversion and eversion strength. J Athl Train 32:226–232
De Simoni C, Wetz HH, Zanetti M, Hodler J, Jacob H, Zollinger H (1996) Clinical examination and magnetic resonance imaging in the assessment of the ankle sprains treated with an orthosis. Foot Ankle Int 17:177–182
Docherty CL, Valovich McLeod TC, Shultz SJ (2006) Postural control deficits in participants with functional ankle instability as measured by the balance error scoring system. Clin J Sport Med 16:203–208
Evans GA, Hardcastle P, Frenyo AD (1984) Acute rupture of the lateral ligament of the ankle. To suture or not to suture? J Bone Joint Surg 66B:209–212
Freeman MAR, Dean MRE, Hanham IWF (1965) The etiology and prevention of the functional instability of the foot. J Bone Joint Surg 47B:678–685
Freeman MAR (1965) Instability of the foot after injuries to the lateral ligament of the ankle. J Bone Joint Surg 47B:678–685
Garrick JG, Requa RK (1988) The epidemiology of the foot and ankle injuries in sports. Clin Sports Med 7:29–36
Glencross D, Thornton E (1981) Position sense following joint injury. J Sports Med Phys Fitness 21:23–27
Guskiewicz KM, Perrin DH (1996) Research and clinical applications of assessing balance. J Sport Rehabil 5:45–63
Halasi T, Kynsburg A, Talley A, Berkes I (2005) Changes in joint position sense after surgically treated chronic lateral ankle instability. Br J Sports Med 39:818–824
Isakov E, Mizrahi J (1997) Is balance impaired by recurrent sprained ankle? Br J Sports Med 31:65–7
Isakov E, Mizrahi J, Solzi P, Susak Z, Lotem M (1986) Response of the peroneal muscles to sudden inversion of the ankle during standing. Int J Sports Biomech 2:100–109
Jerosch J, Bischof M (1996) Proprioceptive capabilities of the ankle in stable and unstable joints. Sports Exerc Inj 2:167–171
Kannus P, Renström P (1991) Treatment for acute tears of the lateral ligaments of the ankle. Operation, case, or early controlled motion. J Bone Joint Surg 73A:305–312
Karlsson J, Andreasson GO (1992) The effect of external ankle support in chronic lateral ankle joint instability: an electromyographic study. Am J Sports Med 20:257–261
Karlsson J, Lansinger O (1992) Lateral instability of the ankle joint. Clin Orthop 276:253–261
Kleinrensink GJ, Stoeckart R, Meulstee J, Kaulesar S, Vleeming A, Snijders CJ, van Noort A (1994) Lowered motor conduction velocity of the peroneal nerve after inversion trauma. Med Sci Sports Exerc 26:877–883
Konradsen L, Magnusson P (2000) Increased inversion angle replication error in functional ankle instability. Knee Surg Sports Traumatol Arthrosc 8(4):246–251
Konradsen L, Olesen S, Hansen HM (1998) Ankle sensorimotor control and eversion strength after acute ankle inversion injuries. Am J Sports Med 26:72–7
Konradsen L, Ravin JB, Sørensen AI (1993) Proprioception at the ankle: The effect of anaesthetic blockade of ligament receptors. J Bone Joint Surg 75B:433–436
Kynsburg A, Halasi T, Talley A, Berkes I (2006) Changes in joint position sense after conservatively treated chronic lateral ankle instability. Knee Surg Sports Traumatol Arthrosc 14:1299–1306
Lentell G, Baas B, Lopez D, McGuire L, Sarrels M, Snyder P (1995) The contributions of proprioceptive deficits, muscle function, and anatomic laxity to functional instability of the ankle. J Orthop Sports Phys Ther 25:206–15
Lephart SM, Pincivero DM, Giroldo JL, Fu FH (1997) The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med 25:130–137
Michelson JD, Hutchins C (1995) Mechanoreceptors in human ankle ligaments. J Bone Joint Surg 77B:219–224
Scavenius M, Bak K, Hansen S, Norring K, Jensen KH, Jorgensen U (1999) Isolated total ruptures of the anterior cruciate ligament—a clinical study with long-term follow-up of 7 years. Scand J Med Sci Sports 9:114–119
Staples OS (1972) Result study of ruptures of lateral ligaments of the ankle. Clin Orthop 85:50–58
Takebayashi T, Yamashita T, Minaki Y, Ishii S (1997) mechanosensitive afferent units in the lateral ligament of the ankle. J Bone Joint Surg 79B:490–493
Tropp H, Odenrick P, Gillquist J (1985) Stabilometry recordings in functional and mechanical instability of the ankle joint. Int J Sports Med 6: 180–182
Winter DA (1991) The biomechanics and motor control in human gait: normal, elderly and pathological. University of Waterloo Press, Ontario, pp 21–22
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nakasa, T., Fukuhara, K., Adachi, N. et al. The deficit of joint position sense in the chronic unstable ankle as measured by inversion angle replication error. Arch Orthop Trauma Surg 128, 445–449 (2008). https://doi.org/10.1007/s00402-007-0432-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-007-0432-6