
Abstract
Background
The Achilles tendon is one of the most common sites of tendon injury and rupture. One of the early events of wound healing is angiogenesis, in which neovascularization prompts delivery of inflammatory cells and fibroblasts to the wound site. Angiogenesis is controlled by a variety of mitogenic, chemotactic, or inhibitory peptides and lipid factors that act on invading endothelial and smooth muscle cells. One of the most important angiogenic factors is the vascular endothelial cell growth factor (VEGF), a glycosylated protein of 46–48 kDa composed of two disulfide-linked subunits.
Methods
We therefore investigated the expression of VEGF during healing of artificial lesions of the Achilles tendon in a sheep model by immunohistochemical, biochemical, molecular, and cell biology methods. Two groups were created, the Achilles tendon was tenotomized, and the animals were killed at 3 and 24 weeks. Each group consisted of 6 specimens. Six animals which did not undergo surgery served as controls.
Results
VEGF could be immunostained in tenocytes of ruptured but not in normal adult tendons. At microvessels, the receptors VEGFR-1 (flt-1) and VEGFR-2 (KDR) could also be visualized. High VEGF levels in ruptured and negligible levels in normal Achilles tendons could be confirmed and quantified by enzyme-linked immunoassay (ELISA). The highest VEGF concentrations were found in ruptured tendons, whereas the VEGF content in healthy adult tendons was negligible. Interestingly, the VEGF concentration of the original tendon stump was higher after 3 weeks than that of the newly regenerated tendon tissue. However, this difference was not significant (p>0.05). Reverse transcription-polymerase chain reaction (RT-PCR) showed that the splice variants VEGF120 and VEGF164 are expressed at 3 weeks and 24 weeks, respectively.
Conclusion
These results prove the presence of the splice variants VEGF120 and VEGF164 in ruptured tendons during the healing process. The demonstrated up-regulation of VEGF in intrinsic tenocytes suggests a role for VEGF in mechanisms of angiogenesis and Achilles tendon repair. Further research is needed to evaluate if VEGF might be a possible tool to enhance the process of tendon healing.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The biochemical mechanism of tendon healing remains controversial. Both extrinsic and intrinsic mechanisms of nutrition and tissue repair have been implicated [6, 8, 11, 23]. One of the early events of wound healing is angiogenesis [16], in which neovascularization prompts delivery of inflammatory cells and fibroblasts to the wound site.
The formation of new blood vessels (angiogenesis) is a necessary event during embryogenesis, but occurs rarely in the adult with a few exceptions such as the female reproductive system, wound healing, and pathological processes like cancer or rheumatoid arthritis [14, 15, 16, 19, 20]. Angiogenesis is controlled by a variety of mitogenic, chemotactic, or inhibitory peptide and lipid factors that act on invading endothelial and smooth muscle cells [16]. One of the most important angiogenic factors is the vascular endothelial cell growth factor (VEGF; alternative term: vascular permeability factor, VPF), a glycosylated protein of 46–48 kDa composed of two disulfide-linked subunits.
VEGF/VPF is an endothelial cell mitogen, promotes angiogenesis in vivo, and renders the microvasculature hyperpermeable to circulating macromolecules [6, 7, 12, 17, 35, 36, 37, 38]. In addition, VEGF is chemotactic for monocytes and a procoagulant. In normal tissues, VEGF is expressed during embryogenesis and in a limited number of sites in adults, e.g., in the circumventricular organs [16]. In the disease state, VEGF can be detected in various tumor cells, osteoarthritic cartilage, the synovial pannus in rheumatoid arthritis, or keratinocytes during wound healing [6, 7, 12, 17, 35, 36, 37, 38]. In humans, five different VEGF isoforms with 121, 145, 165, 189, and 206 amino acids can be generated as a result of alternative splicing from the single VEGF gene [13]. In other species, these splice forms vary by one or two amino acids (e.g., in sheep: VEGF 120, VEGF 144, VEGF 164, VEGF 188, VEGF205) [12]. These isoforms differ in their molecular mass and in their biological properties such as their ability to bind to heparin or heparan-sulfate proteoglycans and to different VEGF receptors (VEGFR) [12]. The splice forms VEGF121, VEGF145, and VEGF165 are secreted, whereas VEGF189 is tightly bound to cell surface heparan-sulfate, and VEGF206 is an integral membrane protein [13, 31]. In contrast to the other forms, VEGF121 does not bind to heparin or extracellular matrix proteoglycans. The signalling tyrosine kinase receptor VEGFR-1 (flt-1, fms-like tyrosine kinase 1) binds VEGF121 and VEGF165, and VEGFR-2 (KDR, kinase domain region/flk-1, fetal liver kinase 1) additionally binds VEGF145 (apart from certain VEGF-related peptides). The co-receptors neuropilin-1 and -2 selectively bind the 165 residue VEGF isoform [31].
An understanding of the cellular and molecular pathways that govern the events of tendon healing is critical to the future advancement of treatment. Studies on the factors that initiate and control the cells and molecules involved in tendon healing will lead to new insights and direct additional efforts in tendon regeneration research.
The aim of this study was to examine the expression of VEGF and its receptors (FLT 1 and KDR/FLK-1) to elucidate the complex process of tendon healing. For that purpose, we studied the expression of VEGF in a tendon healing model in sheep with immunohistochemical, biochemical, and molecular biology methods.
Materials and methods
The animal experiment was performed at the Trauma & Reconstructive Surgery Department, Charité, Campus Virchow-Clinicum, Humbold University of Berlin. All procedures were performed with permission of the local government animal rights protection authorities in accordance with the National Institute of Health guidelines for the use of laboratory animals.
Twelve skeletally mature, female merino sheep were used for anterior cruciate ligament (ACL) reconstruction. All animals (average weight: 51.4 kg) were screened to ensure good physical condition. This animal experiment was carried out to examine the effect of radiofrequency shrinkage on the chronically relaxed ACL. To reduce postoperative activity, all animals underwent a tenotomy of the Achilles tendon. The animals were assigned to two groups and killed at 3 and 24 weeks. Each group consisted of 6 animals. Anesthesia was induced intravenously with thiopental-sodium and maintained with isoflurane and nitrous oxide. Postoperatively, the animals were returned to their cages and were allowed to move without any restrictions. Animals were euthanasized with an overdose of potassium chloride and thiopental-sodium. The knees were harvested, and the grafts were explanted. Six normal Achilles tendons of sheep which did not undergo surgery were selected from a local abattoir and served as controls. The tendons were obtained immediately after death and were frozen in a freezer (−20°C).
Immunohistochemistry
For immunohistochemistry, tissue samples were fixed in 3% paraformaldehyde, embedded in paraffin, sectioned, irradiated at 750 W in a microwave oven with 3% hydrogen peroxide in 0.01 M sodium citrate buffer, pH 6.0 (twice for 5 min), dewaxed, immunostained with anti-VEGF (1:40 in Tris-buffered saline, 60 min; sc7269 mouse monoclonal IgG2a, Santa Cruz Biotechnology, CA, USA), anti-VEGFR-1 (1:80; sc316-G goat polyclonal antibody; Santa Cruz), or anti-VEGFR-2 (1:80; goat polyclonal antibody; Santa Cruz), followed by biotinylated secondary antibodies and a peroxidase-labeled streptavidin-biotin staining technique; nuclei were counterstained with hemalum.
Enzyme-linked immunosorbent assay
For enzyme-linked immunosorbent assay (ELISA), frozen tissue samples were crushed in an achate mortar under liquid nitrogen, homogenized in 150 mM NaCl 20 mM Tris/HCl-buffer, pH 7.4, a soluble fraction obtained by centrifugation (48,000×g, 60 min), and aliquots (100 μl) analyzed by a sandwich ELISA (R&D Systems, Minneapolis, MN, USA) that detects all VEGF splice forms. Human recombinant VEGF165 (PreproTech, Rocky Hill, NJ, USA) served as the standard.
Reverse transcription-polymerase chain reaction (RT-PCR) for VEGF splice variants [13]
For RT-PCR, frozen samples (1 g) were crushed in an achate mortar under liquid nitrogen, RNA isolated by the phenol-guanidinium thiocyanate method, purified by isopropanol and repeated ethanol precipitation, and contaminating DNA was destroyed by digestion with RNase-free DNase I (20 min 25°C; Boehringer, Mannheim, Germany). After inactivation, the DNase (15 min 65°C), cDNA was generated with 1 μl (20 pmol) oligo (dT)15 primer (Amersham Pharmacia Biotech, Uppsala, Sweden) and 0.8 μl superscript RNase H− reverse transcriptase (Gibco, Paisley, UK) for 60 min at 37°C as described [11]. For PCR, 4 μl cDNA were incubated with 30.5 μl water, 4 μl 25 mM MgCl2, 1 μl dNTP, 5 μl 10×PCR buffer, and 0.5 μl (2.5 U) platinum Taq DNA polymerase (Gibco), and the following primers (2.5 μl each containing 10 pmol) [12]:
Results
VEGF can be immunostained in tenocytes of ruptured adult but not healthy tendons
By immunocytochemistry, VEGF can be visualized in tenocytes of ruptured human Achilles tendons, but not in healthy adult ones (Fig. 1). In ruptured tendons, the immunoreactivity was restricted to distinct areas of the tendons. Apart from the cytoplasm of the tenocytes, the pericellular space was also immunopositive. To visualize the possible target for the angiogenic peptide, some sections were immunostained for VEGFR-1/flt-1 and VEGFR-2/KDR (Fig. 1c,d). Endothelial cells in microvessels of ruptured tendons stained intensely.

Immunostaining of vascular endothelial cell growth factor (VEGF) in ruptured (a) and in healthy adult sheep Achilles tendons (b) and its receptors VEGFR-1/flt-1 (c) and VEGFR-2/KDR (d) in tenotomized sheep Achilles tendons. Nuclei in the sections were counterstained with Meyer's hemalum. The VEGF antibody is cross-reactive with all VEGF splice forms. No immunoreactions were detectable after adsorption of the VEGF antibody to recombinant VEGF165 or after omitting the primary antibodies. Bar=10 μm (a–c) or 100 μM (d), original magnifications ×360 (a–c) or ×180 (d)
VEGF concentrations are negligible in healthy adult Achilles tendons, but high in ruptured ones
To quantify the VEGF concentrations in Achilles tendons, surgical or pathological samples were homogenized and VEGF measured by a sensitive ELISA (Fig. 2). The highest VEGF concentrations were found in ruptured tendons at week 3 postoperatively, with a decreasing VEGF concentration observed after 24 weeks. The VEGF content in healthy adult tendons was negligible. Interestingly, the VEGF concentration of the original tendon stump after 3 weeks (zone A in Fig. 3) was higher than that of the newly regenerated tendon tissue (zone B in Fig. 3). However, this difference was not significant (p>0.05).

VEGF concentrations are strongly increased in tenotomized but not in normal Achilles tendons. Samples were homogenized in buffer, and immunoreactive VEGF determined in the homogenates by an ELISA detecting all soluble VEGF splice variants. Means±standard deviations from n=6 animals each. Zones a and b refer to the localization of the original tendon stump and the newly regenerated tendon tissue in Fig. 1

Sheep Achilles tendon, anterior view, 24 weeks after tenotomy. Zone A shows the original tendon stump and zone B, the newly regenerated tendon tissue
The splice forms VEGF120 and VEGF164 can be detected in ruptured tendons
Since the VEGF antibody detects all splice forms and SDS-PAGE lacks the resolution to separate variants with 20–40 residues difference due to the high glycosylation of the VEGF protein, we analyzed the expression of these differently biologically active splice forms by RT-PCR with primers yielding different-sized products (Fig. 4). From all samples of the four ruptured tendons (3 weeks and 24 weeks) investigated, two PCR products were obtained: One with 186 bp corresponding to VEGF120 and one with 318 bp corresponding to VEGF164.

RT-PCR amplification with primers allowing the discrimination of VEGF splice variants detect only VEGF120 and VEGF164 in tenotomized Achilles tendons (AT), but not in normal Achilles tendons (C). RNA from the different samples was digested with DNase, reverse transcribed, the cDNA amplified with primers annealing with the VEGF exons 1 (sense) and 8 (antisense), and the PCR products separated on 2% agarose gels that were stained with ethidium bromide. Two products are detectable in ruptured tendons: a 186 bp band derives from VEGF120 with exons 6 and 7 spliced out, and a 318 bp band is from VEGF164 with exon 6 spliced out. It is easily possible to separate other splice variants, e.g., VEGF188, from the splice forms detected (not shown). A separate RT-PCR for glycerin aldehyde-3-phosphate dehydrogenase (GAPDH) yielding a 983 bp product served as control for the intactness of the mRNA applied
In conclusion, VEGF mRNA and protein can be detected in tenocytes of ruptured but not in normal Achilles tendons.
Discussion
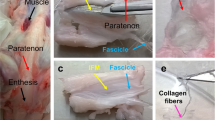
Normal adult human tendons show a relatively low vascularization due to the low metabolic requirements and rates of this predominantly extracellular tissue [1, 10, 23, 25, 26, 27, 32, 33, 34, 41]. However, they have a well-organized peri- and intratendinous network of blood vessels. Tendons receive their blood supply from vessels coming from the muscle, bone, or periosteum, and especially from vessels surrounding the tendon, in the paratenon, mesotenon, and synovial sheet [1, 10, 23, 25, 26, 27, 41]. An injury such as a spontaneous or traumatic tendon rupture destroys this well-organized peri- and intratendineous network of blood vessels [8, 21, 23]. Therefore, angiogenesis—the formation of blood vessels from pre-existing capillaries—is a necessary event during tendon healing.
Growth factors or cytokines are multifunctional proteins that play important roles in the complex cell-cell interactions leading to wound healing [7]. Using molecular biology, biochemical, and immunocytochemical techniques, we could show that VEGF is expressed in injured Achilles tendons at the site of rupture, whereas this angiogenic peptide was undetectable in normal tendons. VEGF appears to be one of the most important inducers of angiogenesis—despite the fact that a variety of other angiogenic factors have been identified, including members of the fibroblast growth factor family (FGF), transforming growth factors (TGF) α and β, hepatocyte growth factor, tumor necrosis factor (TNF) α, angiogenin, interleukin 8, and others [16, 38, 40]. So far, angiogenesis factors have not been identified in embryonic or adult tendons, except mRNA for basic FGF in tenocytes after experimental transection [11] and—during previous experimental work of this study—mRNA for VEGF at the repair site of healing canine flexor tendon in an experimental model [6].
The essential role of VEGF and its receptors, VEGFR-1 and -2, for embryonic vasculogenesis and angiogenesis have been clearly demonstrated by gene knockout studies in mice [9, 39]. However, also after birth, VEGF plays a major role in development, e.g., in longitudinal bone growth by stimulating angiogenesis into the epiphyseal growth plate [19]. In the fully grown animal, VEGF is likely to be required for active angiogenesis processes, such as corpus luteum development and wound healing [16]. In addition, several studies have shown that VEGF plays a pivotal role in the angiogenesis of certain tumors, e.g., glioblastomas, and other pathologic conditions associated with high neovascularization, e.g., diabetic retinopathy, age-related macular degeneration, rheumatoid arthritis [14, 15, 16, 20]. VEGF re-expression in tenocytes of tenotomized tendons is likely to be induced by a wound healing process. Interestingly, tenocytes produce the two most diffusible splice forms, VEGF120 and VEGF164, that bind to the two signaling receptors VEGFR-1 and VEGFR-2. These splice forms are comparable to VEGF121 and VEGF165 found in humans [12]. These isoforms differ in their molecular mass and in their biological properties such as their ability to bind to heparin or heparan-sulfate proteoglycans and to different VEGFRs [12].
Synovial diffusion and vascular perfusion both contribute to the nutrition of healing Achilles tendons [23]. In areas of injury where blood vessels have been traumatically disrupted, angiogenesis creates capillary networks and granulation tissue to transport cells essential for inflammation and collagen synthesis. The initial signaling processes are now thought to be mediated by several growth factors including VEGF. The demonstrated up-regulation of VEGF in intrinsic tenocytes suggests a role for VEGF in mechanisms of angiogenesis and Achilles tendon repair. Although an unambiguous association between VEGF expression and strength of the tendon site remains to be established, focal expression of VEGF at the repair site has the potential to provide an angiogenetic stimulus for vascular ingrowth during the postoperative healing phase of the Achilles tendon.
Since the Achilles tendon most frequently ruptures within a zone of hypovascularity [22, 24], tendon healing can be impaired by a poor local blood supply of the tendon [21]. VEGF might be a potential clinical tool to influence the process of tendon healing. Since growth factors are peptides with dose-dependent multiple functions, the optimal dose of VEGF for therapeutical use has to be established. The tissue concentrations and the time course of VEGF expression found in the present study may provide a basis for further studies. Another major problem for the clinical use of growth factors involves appropriate delivery systems. Further research must also focus on the question of which delivery systems are most suitable for the application of VEGF.
It is noteworthy that VEGF could be found in tissue biopsies of degenerative Achilles tendons [35]. VEGF might be a key molecule in the complex process of tendon degeneration because it might be the inducer of neovascularization during chronic Achilles tendinopathy [2, 3, 4, 5, 24, 28]. Since metalloproteinase-induced tissue degradation mostly precedes neoangiogenesis, VEGF might also have the potential to alter the mechanical strength of a tissue.
Further research is needed to evaluate the effect of VEGF application on the process of tendon healing.
References
Ahmed IM, Lagopoulos M, McConnel P, Soames RW, Sefton GK (1998) Blood supply of the Achilles tendon. J Orthop Res 16:591–596
Astrom M, Rausing A (1995) Chronic Achilles tendonopathy. A survey of surgical and histopathological findings. Clin Orthop 316:151–164
Astrom M, Westlin N (1994) Blood flow in chronic Achilles tendinopathy. Clin Orthop 308:166–172
Backman C, Boquist L, Friden J, Lorentzon R, Toolanen G (1990) Chronic Achilles paratendinosis with tendinosis: an experimental model in the rabbit. J Orthop Res 8:541–547
Backman C, Friden J, Widmark A (1991) Blood flow in chronic Achilles tendinosis: radioactive microsphere study in rabbits. Acta Orthop Scand 62:386–387
Bidder M, Towler DA, Gelberman RH, Boyer MI (2000) Expression of mRNA for vascular endothelial growth factor at the repair site of healing canine flexor tendon. J Orthop Res 18:247–252
Callard R, Gearing A (1994) The cytokine facts book. Academic Press, London
Carlstedt CA, Madsen K, Wredmark T (1986) Biomechanical and biochemical studies of tendon healing after conservative and surgical treatment. Arch Orthop Trauma Surg 105:211–215
Carmeliet P, Ferreira V, Breier G, Pollefeyt S, Kiekens L, Gerstenstein M, Fahrig M, Vandenhoeck A, Harpal K, Eberhardt C, Declerq C, Pawling J, Moons L, Collen D, Risau W, Nagy A (1996) Abnormal blood vessel development and lethality in embryos lacking a single VEGF allele. Nature 380:435–439
Carr AJ, Norris SH (1989) The blood supply of the calcaneal tendon. J Bone Joint Surg Br 71:100–101
Chang J, Most D, Thunder R, Mehrara B, Longaker MT, Lineaweaver WC (1998) Molecular studies in flexor tendon wound healing: the role of basic fibroblast growth factor gene expression. J Hand Surg 23:1052–1058
Cheung CY, Brace RA (1998) Ovine vascular endothelial growth factor: nucleotide sequence and expression in fetal tissues. Growth Factors 16:11–22
Eckhart L, Ban J, Ballaun C, Weniger W, Tschachler E (1999) Reverse transcription-polymerase chain reaction products of alternatively spliced mRNAs form heteroduplexes and heteroduplex complexes. J Biol Chem 274:2613–2615
Fava RA, Olsen NJ, Spencer-Green G, Yeo K-T, Yeo T-K, Berse B, Jackman RW, Senger DR, Dvorak HF, Brown LF (1994) Vascular permeability factor/endothelial growth factor (VPF/VEGF): accumulation and expression in human synovial fluids and rheumatoid synovial tissue. J Exp Med 180:341–346
Feindt J, Becker I, Blömer U, Hugo H-H, Mehdorn HM, Krisch B, Mentlein R (1995) Expression of somatostatin receptor subtypes in cultured astrocytes and gliomas. J Neurochem 65:1997–2005
Ferrara N (1999) Molecular and biological properties of vascular endothelial growth factor. J Mol Med 77:527–543
Finkenzeller G, Sparacio A, Technau A, Marme D, Siemeister G (1997) Sp1 recognition sites in the proximal promoter of the human vascular endothelial growth factor gene are essential for platelet-derived growth factor-induced gene expression. Oncogene 15:669–676
Fong DH, Rossant J, Gersenstein M, Breitman ML (1995) Role of the Flt-1 receptor tyrosine kinase in regulating the assembly of vascular endothelium. Nature 376:66–70
Gerber HP, Vu TH, Ryan AM, Kolwalski J, Werb Z, Ferrara N (1999) VEGF couples hypertrophic cartilage remodeling, ossification and angiogenesis during endochondral bone formation. Nat Med 5:623–628
Held-Feindt J, Krisch B, Mentlein R (1999) Molecular and functional analysis of the somatostatin receptor subtype 2 (sst2) in human glioma cells. Mol Brain Res 64:101–107
Hepp WR, Blauth W (1978) Repair of defects in the Achilles tendon with the peroneus brevis muscle. Arch Orthop Trauma Surg 91:195–200
Jarvinen M, Józsa, LG, Kannus, P, Jarvinen TL, Kvist M, Leadbetter W (1997) Histopathological findings in chronic tendon disorders. Scan J Med Sci Sports 7:86–95
Józsa LG, Kannus P (1997) Human tendons—anatomy, physiology, and pathology. Human Kinetics, London
Kannus P, Jozsa L (1991) Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 981 patients. J Bone Joint Surg Am 73:1507–1525
Koch S, Tillmann B (1995) The distal tendon of the biceps brachii: structure and clinical correlations. Ann Anat 177:467–474
Lang J (1960) Über das Gleitgewebe der Sehnen, Muskeln, Fascien und Gefäße. Z Anat Entwicklungsgesch 122:197–231
Lang J (1963) Über die Blutgefäße der Sehnenscheiden. Acta Anat 54:273–309
Messner K, Wei Y, Andersson B, Gillquist J, Rasanen T (1999) Rat model of Achilles tendon disorder. A pilot study. Cells Tissues Organs 165:30–39
Milanini J, Vinals F, Poussegur J, Pages G (1998) p42/p44 MAP kinase module plays a key role in the transcriptional regulation of the vascular endothelial growth factor gene in fibroblasts. J Biol Chem 273:18165–18172
Movin T, Gad A, Reinholt FP, Rolf C (1997) Tendon pathology in long standing achillodynia. Biopsy findings in 40 patients. Acta Orthop Scand 68:170–175
Neufeld G, Cohen T, Gengrinovitch S, Poltrak Z (1999) Vascular endothelial growth factor and its receptors. FASEB J 13:9–22
Petersen W, Stein V, Tillmann B (1999) Blood supply of the quadriceps tendon. Unfallchirurg 102:543–547
Petersen W, Stein V, Tillmann B (1999) Blood supply of the tibialis anterior tendon. Arch Orthop Trauma Surg 119:371–375
Petersen W, Bobka T, Stein V, Tillmann B (2000) Blood supply of the peroneal tendons: injection and immunohistochemical studies of cadaver tendons. Acta Orthop Scand 71:168–174
Pufe T, Petersen W, Tillmann B, Mentlein R (2001) The angiogenetic peptide vascular endothelial growth factor is expressed in foetal and ruptured tendons. Virchows Arch 439:579–585
Pufe T, Petersen W, Tillmann B, Mentlein R (2001) Expression of the vascular endothelial growth factor in osteoarthritic cartilage. Arthritis Rheum 44:1082–1088
Pufe T, Petersen W, Tillmann B, Mentlein R (2001) The splice variants VEGF 121 and VEGF 165 are expressed in synovium of rheumatoid arthritis. J Rheumatol 28:1482–1486
Ryuto M, Ono M, Izumi H, Yoshida S, Weich HA, Kohno K, Kuwano M (1996) Induction of vascular endothelial growth factor by tumor necrosis factor alpha in human glioma cells. Possible roles of SP-1. J Biol Chem 271:28220–28228
Shalaby F, Rossant J, Yamaguchi TP, Gerstenstein M, Wu XF, Breitman ML, Schuh AC (1995) Failure of blood-island formation and vasculogenesis in Flk-1-deficient mice. Nature 376:62–66
Stavri GT, Zachary IC, Baskervillle PA, Martin JF, Erusalimsky JD (1995) Basic fibroblast growth factor upregulates the expression of vascular endothelial growth factor in vascular smooth muscle cells. Synergistic action with hypoxia. Circulation 92:11–14
Stein V. Laprell H, Tinnemeyer S, Petersen W (2000) Quantitative assessment of the intravascular volume of the human Achilles tendon. Acta Orthop Scand 181:313–314
Acknowledgements
We wish to thank Frank Lichte, Karin Stengel, and Regine Worm for their expert technical assistance. This work was supported by a grant from the 'Forschungsschwerpunkt Muskel- und Skelettsystem' of the Medical Faculty of the University of Kiel. All animal experiments were performed with permission of the local government animal rights protection authorities in accordance with the National Institute of Health guidelines for the use of laboratory animals. All other parts of the experiments comply with the current laws of Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Petersen, W., Pufe, T., Unterhauser, F. et al. The splice variants 120 and 164 of the angiogenic peptide vascular endothelial cell growth factor (VEGF) are expressed during Achilles tendon healing. Arch Orthop Trauma Surg 123, 475–480 (2003). https://doi.org/10.1007/s00402-003-0490-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-003-0490-3