
Abstract
Activation of the PI3K/Akt pathway protects the heart from ischemia-reperfusion injury (IRI). The phosphatase PTEN is the main negative regulator of this pathway. We hypothesized that reduced PTEN levels could protect against IRI. Isolated perfused mouse hearts from PTEN+/− and their littermates PTEN+/+ (WT), were subjected to 35 min global ischemia and 30 min reperfusion, with and without 2, 4 or 6 cycles ischemic preconditioning (IPC). The end point was infarct size, expressed as a percentage of the myocardium at risk (I/R%). PTEN and Akt levels were determined using Western blot analysis. Unexpectedly, there were no significant differences in infarction between PTEN+/− and WT (42.1 ± 5.0% Vs. 45.6 ± 3.3%). However, the preconditioning threshold was significantly reduced in the PTEN+/− Vs. WT, with 4 cycles of IPC being sufficient to reduce I/R%, compared to 6 cycles in the WT (4 cycles IPC: 29.8. ± 3.69% in PTEN+/− Vs. 45.5. ± 5.08% in WT, P < 0.01). In addition, the ratio between the phospho/total Akt (Ser473 and Thr308) was slightly but significantly increased in the PTEN+/− indicating an upregulation of PI3K/Akt pathway. Interestingly, the levels of the other phosphatases that may negatively regulate the PI3K/Akt pathway (PP2A, SHIP2 and PHLPP) were not significantly different between littermates and PTEN+/−. In conclusion, PTEN haploinsufficiency alone does not induce cardioprotection in this model; however, it reduces the threshold of protection induced by IPC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
It is well established that the PI3K/Akt pathway is a pivotal step in cardioprotection against ischemia-reperfusion injury [2, 3, 8, 10], and strategies to enhance its activity in order to promote tissue salvage, provide an attractive target for clinical treatment of myocardial infarction [2, 19, 31]. PI3K activity results in an increased production of the second messenger phosphatidylinositol (3,4,5 phosphate (PI(3,4,5)P3) and this in turn activates a downstream cascade of prosurvival events [12, 13, 24].
Phosphatase and tensin homologue deleted on chromosome 10 (PTEN) is a lipid phosphatase which dephosphorylates PI(3,4,5)P3 to PI(4,5)P2 [13, 14] (Fig. 1). This phosphatase is constitutively active and considered the main downregulator of the pro-oncogenic PI3K/Akt. It, therefore, functions to negatively regulate proliferation, growth and survival. However, a reversible inhibition of PTEN may have a major impact in treatment of apoptosis related diseases as inhibition of PTEN can enhance the PIP3-PI3K/Akt survival pathway [19, 23, 30]. PTEN has been associated with cardiovascular diseases, for example, in a Japanese study of patients with type 2 diabetes, 3 different mutations in the PTEN gene were identified [11]. Moreover, it has been shown in diabetic Goto Kakazaki rat hearts that the expression of cardiac PTEN is increased in conjunction with a desensitized insulin signalling pathway [18]. In addition, it has been shown that these rats have a higher threshold to IPC and therefore are more difficult to protect against ischemia-reperfusion injury [27]. We were the first to demonstrate the potential importance of PTEN in the protection against IRI by showing that the cardioprotection induced by acute atorvastatin treatment does not occur when the drug was administered chronically, for 1 or 3 weeks, the upregulation of PTEN being associated with this loss of protection [15]. More recently, Cai and Semenza [5] were the first to demonstrate that PTEN is subject to alterations during IPC; this group identified, in an isolated perfused rat heart model of IPC, a reduction in the activity of PTEN [5]. In addition other groups have investigated specific PTEN inhibition in the murine cardiomyocyte and have reported a hypertrophic and reduced contractile phenotype compared with an increased phosphorylation of Akt [6]. It appears that decreasing PTEN activity may be a desirable target for treating apoptotic and cell growth related cardiovascular diseases, such as that seen in myocardial infarction.

Diagram representing the phosphatases, which regulate the PI3K/Akt pathway
We therefore hypothesised that downregulation of PTEN levels may induce cardioprotection following ischemia-reperfusion injury. To investigate this we used a murine model of congenital PTEN haploinsufficiency [22] and subjected the isolated perfused mouse hearts to global ischemia and reperfusion injury.
Following the negative results we have obtained (e.g. the reduced level of PTEN did not correlate with protection against myocardial infarction) we further investigated the level of other phosphatases which may inhibit the PI3K/Akt signaling pathway (Fig. 1) hypothesizing that they may be upregulated to compensate for PTEN haploinsufficiency. In addition we also examined the threshold for ischemic preconditioning (IPC) in these hearts in which the PI3K/Akt pathway has been shown to be slightly more active due to a reduced PTEN level. We hypothesized that PTEN haploinsuficiency may be associated with a reduced threshold for IPC expression.
2 Materials and methods
2.1 Materials
Primary and secondary antibodies to total and phosphorylated forms of Akt and PTEN as well as total PP2A (Protein Phosphatase 2A) were obtained from Cell Signaling Technology (Hitchin, UK), primary and secondary antibodies to β-actin were obtained from Abcam UK, SHIP2 (SRC Homology 2 containing Inositol 5 Phosphate) and PHLPP1 (PH domanin Leucine rich repeat Protein Phosphatase) antibodies were purchased from Bethyl Laboratories. The Hybond ECL nitrocellulose membranes and the ECL Western blotting reagent were from Amersham Biosciences (Little Chalfont, UK). Protein content was measured with the BCA (bicicinoic acid) assay from Sigma (Aldrich, UK).
2.2 Experimental procedures
2.2.1 Haploinsufficient mice
Male PTEN haploinsufficient mice (PTEN+/−) and their littermate controls (PTEN+/+), aged of 10–15 weeks [22] were used in these experiments. Animal experiments were conducted in accordance with the Animals (Scientific Procedures) Act 1986 published by the UK Home Office and the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 86–23, revised 1985).
DNA was extracted from mouse tail tips 0.5 cm long using a Qiagen DNeasy kit with a proteinase K and spin column extraction method (Qiagen, UK), PCR reactions contained 0.5 µM primers (MWG, Germany) of PTEN Wild type—5′ GTC TCT GGT CCT TAC TTC C 3′, PTEN common—5′ TTG CAC AGT ATC CTT TTG AAG 3′, PTEN neo/NEW—5′ACG AGA CTA GTG AGA CGT GC 3′. PCR reaction mixtures were obtained from Promega, UK and were mixed with DNA before running 35 amplification cycles on a thermocycler. The DNA was analysed on a 2% agarose gel with ethidium bromide and exposed to UV light. The PCR products generate a wild type phenotype (from littermate control PTEN+/+) expressed as a single band running to 240 bp and a haploinsufficient phenotype (from PTEN+/−) expressed as two bands running to 240 and 320 bp.
2.3 Langendorff isolated perfused mouse heart
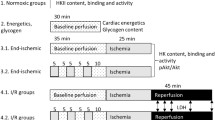
Mice were given 100 U of heparin by intraperitoneal injection before being sacrificed by cervical dislocation. Hearts were rapidly excised and retrogradely perfused via the aorta in a Langendorff apparatus (ADInstruments) at a constant pressure of 100 mmHg, with oxygenated Krebs–Henseleit buffer containing NaCl 118 mm, NaHCO3 24 mm, KCl 4 mM, NaH2PO4 1 mm, CaCl2 1.8 mm, MgCl2 1.2 mm and glucose 10 mm [ 25 ]. The heart rate and the contractile function were monitored using a fluid filled balloon inserted into the left ventricle and connected to a pressure transducer. Myocardial temperature, monitored with a temperature probe placed on the surface of the heart, was maintained at 37 ± 0.5°C. Isolated perfused hearts were subjected to a 30 min stabilisation period followed by 35 min global ischemia and 30 min reperfusion, with and without 2, 4 or 6 cycles ischemic preconditioning (IPC) (n = 5–8 per group). Each IPC cycle consisted of 5 min global ischemia followed by 5 min reperfusion. Infarct size was measured as follows. At the end of reperfusion, 1% triphenyltetrazolium chloride (TTC) solution was perfused through the aorta and the heart was maintained at 37°C for 10 min before storing at −20°C. TTC reacts with dehydrogenases from the living tissue staining it red, while the dead tissue remains off-white. Subsequently, hearts were transversally sliced (<1 mm slices), immersed 12 h in formalin for a better delineation of the risk and infarct areas, photographed and planimetered using the NIH Image 1.63 software package (National Institutes of Health, Bethesda, MD, USA), and infarct size (white) calculated as the percentage of whole heart at risk.
2.4 Western blot analysis
The levels of total and phosphorylated PTEN (Ser380/Thr382/Thr383) and Akt (at Ser473 and Thr308) were measured using Western blot analysis; samples being normalised to β-actin and expressed in arbitrary units (A.U.) as previously described [2, 17, 27]. In addition the Western blot method was used to investigate the level of other phosphatases, which may affect the PI3K/Akt pathway, namely PP2A, SHIP2 and PHLPP (Fig. 1). The heart samples, collected from PTEN+/− and from their littermates were mounted in the Langendorff system and preconditioned or kept on normal perfusion for the same duration (control, base line hearts) (n = 4–5 in each group), then snap-frozen in liquid nitrogen and stored at −80°C. Shortly after, proteins were extracted by homogenising the samples on ice in a suspension buffer consisting of 100 mm NaCl, 10 mm Tris (pH 7.6), 1 mm EDTA (pH 8.0), 2 mm sodium pyrophosphate, 2 mm sodium fluoride, 2 mm β glycerophosphate and a protease inhibitor cocktail, followed by high-speed centrifugation. The supernatants were then assayed for protein content using a bicinchoninic acid (BCA) assay and the proteins separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) and then transferred to Hybond enhanced chemiluminescence (ECL) nitrocellulose membranes. The nitrocellulose membranes were then exposed to photographic film, scanned and the intensities of the protein bands, expressed as arbitrary units (A.U.), were measured by computerised densitometry (NIH Image 1.63). Each sample was corrected for well loading by normalisation to β-actin.
2.5 Statistical analysis
The data were analysed using Student’s t test and expressed as a mean ± SEM and considered significantly different when P < 0.05.
3 Results
3.1 Breeding and genotyping haploinsufficient mice
Tail DNA extracted from littermate controls+/+ amplified one band of 240 bp and DNA extracted from PTEN haploinsufficient+/− mice amplified two bands of 240 and 320 bp (Fig. 2) Because females+/− become infertile at a very early age, the most successful breeding regime favored male PTEN+/− breeding with female+/+ which produced a 40:60% ratio of PTEN+/− to littermate+/+ phenotypes.

Representative PCR gel used for the identification of the PTEN+/− (lines 2, 3, 6–8) and their control littermates PTEN+/+ (lines 4, 5)
3.2 Myocardial Infarct size in PTEN+/− and littermate controls PTEN+/+
To investigate the effect of PTEN haploinsufficiency on cardioprotection following ischemia-reperfusion injury, male PTEN+/− mice and their littermate controls +/+ were subjected to a standard protocol of IR as previously described [25]. Unexpectedly, no protection in response to IR was seen in the haploinsufficient myocardium. There were no differences in the heart function (data not included) prior to ischemia or at reperfusion and, as shown in Fig. 3, isolated hearts from littermate controls+/+ developed an infarct size of 42.9 ± 3% which was similar to the PTEN+/− hearts which developed an infarct size of 43.7 ± 4%.

Infarct size developed in the hearts of PTEN+/− and their littermates PTEN+/+ subjected to ischemia-reperfusion injury. Each circle represents an individual value, the horizontal line represents the mean of the group
3.3 Western blot analysis of PTEN and Akt in PTEN+/− and littermate PTEN+/+ myocardium
PTEN and the pro survival kinase Akt levels were compared in PTEN+/− and littermate control+/+ heart samples using western blot analysis. As expected, the basal level of total PTEN was significantly reduced from 0.84 ± 0.1 arbitrary units (A.U.) in littermate PTEN+/+ controls to 0.35 ± 0.07 A.U. in haploinsufficient PTEN+/− mouse myocardium as shown in Fig. 4a (P < 0.05). In addition, there was no significant difference between phosphorylated (inactivated), PTEN between the groups (0.14 ± 0.018 A.U. in PTEN+/−, Vs.0.19 ± 0.050 A.U. in littermates, P > 0.2).

PI3K/Akt/PTEN pathway in the PTEN+/+ and PTEN+/− hearts. a PTEN levels; (I) western blot scans; (II) relative densitometry after normalisation to β-actin; b Phospho Thr308 Akt: (I) western blot scans; (II) relative densitometry after normalisation to total Akt; c
Phospho Ser473 Akt: (I) western blot scans; (II) relative densitometry after normalisation to total Akt; * P < 0.005; n = 3 for each group; +/+ = littermates; +/− = PTEN+/−, A.U. arbitrary units
Akt is a kinase that requires phosphorylation of amino acids Ser473 and Thr308 for full activation. Therefore western blot probing of these two phosphorylation sites were investigated in order to obtain a better indication of the activation of PI3K/Akt pathway in relation to the PTEN level. Phosphorylated Akt at Thr308 was significantly increased (P < 0.03) in the haploinsufficient mice (0.27 ± 0.037 A.U.) when compared to littermates+/+ (0.10 ± 0.035 A.U.), as shown in Fig. 4b. Increased phosphorylation of Akt at Ser473, in PTEN haploinsufficient mice (0.62 ± 0.156 A.U.) was also significantly higher when compared to their littermates (0.20 ± 0.088 A.U.; P < 0.05)(Fig. 4c). Taken together these data indicate that, under basal conditions, the myocardium from the PTEN haploinsufficient mice has significantly reduced PTEN level and increased Akt phosphorylation compared to their littermate controls+/+. These changes, however, are not enough to confer protection against IRI as demonstrated in the previous section (Fig. 3).
3.4 PTEN+/− status and the level of other phosphatases which may regulate PI3K/Akt
We hypothesized that the lack of protection against ischemia-reperfusion injury in the myocardium of the PTEN+/− mice could have been due to the upregulation of other phosphatases known to downregulate this pathway (Fig. 1). Therefore we measured the level of PP2A (Protein phosphatase A), SHIP2 (SRC homology 2 containing inositol-5-phosphatase) and PHLPP (PH domain leucine-rich repeat protein phosphatase). Our data, presented in Fig. 5, show that there were no significant differences between PTEN haploinsuficient and control hearts.

The level of phosphatases which may regulate PI3K/Akt pathway in PTEN+/− and PTEN+/+ mouse hearts: a PP2A; b SHIP2; c PHLPP. The data are presented as western blots and the respective bar graphs of the normalised value to β-actin content
3.5 Reduced threshold to IPC protection in PTEN+/− compared to their littermate PTEN +/+
In summary, so far, in the PTEN haploinsuficient myocardium, the PI3K/Akt prosurvival pathway is activated, however not enough to induce protection. Further on we investigated the hypothesis that the threshold for IPC may be reduced in these transgenic mice. Isolated hearts were subjected to an IPC protocol consisting of 2, 4 or 6 cycles of 5 min global ischemia, 5 min reperfusion followed by 35 min lethal ischemia and 30 min reperfusion. There were no significant differences in the cardiac functions between groups, however, we observed a significant reduction in infarction with 6 cycles IPC in both groups. In the littermate controls+/+ the infarct size was reduced from 43.8 ± 2.3% to 28.6 ± 1.6% (P < 0.05) and similarly, in the PTEN+/− group, from 44.9 ± 5.2% to 27.2 ± 1.2% (P < 0.05) (Fig. 6). Interestingly, similar protection was also observed with four cycles of IPC but only in the PTEN+/− hearts (29.8. ± 3.7% Vs. 45.5. ± 5.1% in control hearts, P < 0.05), indicating that the myocardium from these animals have a reduced threshold for protection (Fig. 6).

Infarct size developed in the hearts of PTEN+/− and their littermates PTEN+/+, subjected to different IPC protocols (2, 4 or 6 cycles of 5 min ischemia and 5 min reperfusion) prior to ischemia reperfusion injury. Each circle represents a heart, the horizontal line the mean value for the group. C non preconditioned hearts, 2,4 and 6 the respective numbers of preconditioning episodes (* P < 0.05; n = 6 for each group)
3.6 Akt phosphorylation and IPC in PTEN+/− and their littermates PTEN+/+
In Fig. 7 the phosphorylation of Akt at Ser473 and The308 during preconditioning protocol is presented. As previously shown, both Ser473 and Thr308 demonstrate significantly increased phosphorylation at the basic level (non preconditioned, non ischemic hearts) in the PTEN+/− Vs. PTEN+/+ hearts (Fig. 4). The phosphorylation of Akt at Ser473 is significantly increased with 4 as well as 6 cycles of ischemic preconditioning in both PTEN+/+ and PTEN+/− hearts (Fig. 7a). However, the infarct data show that PTEN+/+ hearts are not protected with 4 cycles IPC (Fig. 6). This brings to attention the importance of the Thr308 site. Fig. 7b shows that, while the haploinsuficient hearts have already high levels of Phospho Thr308 and are protected by IPC, PTEN+/+ hearts are protected only when the level of Thr308 phosphorylation achieves a significant difference Vs. 4 cycles, needing probably an augmented stimulation necessary to counterbalance the increased level of PTEN.

Phosphorylated Akt normalised to the total Akt in PTEN+/− and PTEN+/+ mouse hearts subjected to 4 or 6 cycles of IPC. a Phospho Ser473/total Akt; b Phospho Thr308/total Akt.; n = 3 in all groups; * P < 0.05 Vs. PTEN+/+ baseline (non preconditioned heart); ** P < 0.05 Vs. PTEN +/− baseline; # P < 0.05, 4 cycles PTEN+/+; the bars marked “@” are the groups in which preconditioning protection was achieved (as shown in Fig. 6)
4 Discussion
It is known that the activation of the PI3K/Akt prosurvival kinase pathway is essential for cardioprotection [2–4, 10, 16, 21]. The lipid phosphatase, PTEN, is the main negative regulator of PI3K/Akt pathway. It has the ability to dephosphorylate the product of PI3K activity, PI(3,4,5)P3, thereby blocking the cascade of events generated downstream of this secondary messenger [13, 14, 19]. As a consequence there will be a decreased level of Akt phosphorylation [19]. The activity of PTEN is reflected by its cellular level and the phosphorylated form is considered either inactive or tagged for quick ubiquitination [20, 26, 30]. Therefore, we hypothesised that PTEN haploinsufficiency would confer protection to the myocardium undergoing an ischemia-reperfusion injury.
However, in our isolated mouse heart model PTEN haploinsufficiency did not afford the expected cardioprotection. In order to elucidate the cause of this result we verified the cellular levels of PTEN and Akt within the myocardial tissue. In comparison to the littermate controls+/+ we observed a significant, decrease in total PTEN in the PTEN+/− hearts. There have been previous reports demonstrating that the mutated PTEN allele in this mouse model of PTEN haploinsufficiency results in phenotype of reduced PTEN activity, where the phosphatase activity from this allele is abnormal, even though the protein constitution is only slightly affected [28]. In addition, the reduced PTEN activity in these mice has been associated with physiological consequences [22, 29]. For example these animals exhibit insulin hypersensitivity when compared with their littermates [29]. Moreover, as described by Podsypanina et al. [22], they are predisposed to tumours of proliferative tissues such as prostate and endometrium.
Taking into account the importance of keeping PI3K/Akt pathway tightly controlled in order to avoid hypertrophy and malignancy, we hypothesized that there may be upregulation of other phosphatases (as PP2A [32], SHIP2 [1], and PHLPP [7] to compensate for the low level of PTEN which may explain the lack of cardioprotection in the PTEN+/− hearts. However, we could not find any change in the level of these phosphatases.
Interestingly though, the myocardium of our PTEN+/− mice exhibited not only a significantly smaller level of PTEN but also an increased level of phosphorylated Akt at both sites (Ser473 and Thr308) when compared with the PTEN+/+ hearts. It is important to underline that PTEN is a constitutively active phosphatase, while Akt is activated by phosphorylation [19], therefore it appears as if the PI3K/Akt pathway is in a slightly activated state in the PTEN+/− mouse.
It is well documented that increases in Akt activity can induce cardioprotection against ischemia-reperfusion injury and such increases can be stimulated by pharmacological agents, in addition to mechanical activators such as ischemic preconditioning [4, 9, 17]. However, in our PTEN+/− hearts, the degree of decrease in PTEN and increase in active Akt, even if significantly different from the PTEN+/+ hearts, was not sufficient to induce protection. Unfortunately the complete deletion of PTEN is lethal and the PTEN−/− embryos die in early gestation [22]. There has been success in organ targeted specific deletion of the PTEN gene, when Crackower et al. [6], produced a murine cardiomyocyte specific PTEN double knock out(−/−). These hearts became hypertrophic and had impaired contractility. This discovery highlights that complete PTEN inhibition within the heart can have major physiological implications.
Wong et al. [29] investigated insulin sensitivity, and demonstrated that insulin injections increased activity of the insulin receptor substrate pathway and enhanced glucose uptake in the PTEN+/− over and above their littermate controls. This data suggested that, in order to obtain an effect of PTEN haploinsuficiency on PI3K/Akt activity, a stimulation of the PI3K/Akt pathway above basal conditions, is required. Therefore, we further hypothesised that the myocardium from these mice should manifest a lower threshold for protection in the setting of ischemic preconditioning. To investigate this, myocardium from PTEN+/− and their littermate PTEN+/+ was subjected to 2, 4 and 6 cycles of IPC. As predicted, we noted a reduced threshold for preconditioning in the PTEN+/− hearts in which protection against infarction could be achieved with less cycles than in the case of the littermate+/+ hearts, suggesting that PTEN downregulation can be cardioprotective if it is associated with another potential protective agent.
To conclude, the data from our studies show that, in our model of murine myocardial ischemia-reperfusion injury, PTEN haploinsufficiency alone is not sufficient to induce cardioprotection, however, a reduced PTEN activity can facilitate the protection induced by activators of the PI3K/Akt prosurvival kinase pathway. Therefore, it might be possible that reducing PTEN could have therapeutic implications in the survival of the myocardium following an ischemia reperfusion injury. However, due to the potentially carcinogenic nature of this signalling pathway it is important to obtain specific, reversible manipulation of the PTEN function.
References
Backers K, Blero D, Paternotte N, Zhang J, Erneux C (2003) The termination of PI3K signalling by SHIP1 and SHIP2 inositol 5-phosphatases. Adv Enzyme Regul 43:15–28
Bell RM, Yellon DM (2003) Bradykinin limits infarction when administered as an adjunct to reperfusion in mouse heart: the role of PI3K, Akt and eNOS. J Mol Cell Cardiol 35(2):185–193
Bhamra GS, Hausenloy DJ, Davidson SM, Carr RD, Paiva M, Wynne AM, Mocanu MM, Yellon DM (2008) Metformin protects the ischemic heart by the Akt-mediated inhibition of mitochondrial permeability transition pore opening. Basic Res Cardiol 103:274–284
Bullard AJ, Yellon DM (2005) Chronic erythropoietin treatment limits infarct-size in the myocardium in vitro. Cardiovasc Drugs Ther 19:333–336
Cai Z, Semenza GL (2005) PTEN activity is modulated during ischemia and reperfusion: involvement in the induction and decay of preconditioning. Circ Res 97:1351–1359
Crackower MA, Oudit GY, Kozieradzki I, Sarao R, Sun H, Sasaki T, Hirsch E, Suzuki A, Shioi T, Irie-Sasaki J, Sah R, Cheng HY, Rybin VO, Lembo G, Fratta L, Oliveira-dos-Santos AJ, Benovic JL, Kahn CR, Izumo S, Steinberg SF, Wymann MP, Backx PH, Penninger JM (2002) Regulation of myocardial contractility and cell size by distinct PI3K-PTEN signaling pathways. Cell 110:737–749
Gao T, Furnari F, Newton AC (2005) PHLPP: a phosphatase that directly dephosphorylates Akt, promotes apoptosis, and suppresses tumor growth. Mol Cell 18:13–24
Hausenloy DJ, Mocanu MM, Yellon DM (2004) Cross-talk between the survival kinases during early reperfusion: its contribution to ischemic preconditioning. Cardiovasc Res 63:305–312
Hausenloy DJ, Wynne AM, Yellon DM (2007) Ischemic preconditioning targets the reperfusion phase. Basic Res Cardiol 102:445–452
Hausenloy DJ, Yellon DM (2004) New directions for protecting the heart against ischaemia-reperfusion injury: targeting the reperfusion injury salvage kinase (RISK)-pathway. Cardiovasc Res 61:448–460
Ishihara H, Sasaoka T, Kagawa S, Murakami S, Fukui K, Kawagishi Y, Yamazaki K, Sato A, Iwata M, Urakaze M, Ishiki M, Wada T, Yaguchi S, Tsuneki H, Kimura I, Kobayashi M (2003) Association of the polymorphisms in the 5′-untranslated region of PTEN gene with type 2 diabetes in a Japanese population. FEBS Lett 554:450–454
Kane LP, Weiss A (2003) The PI-3 kinase/Akt pathway and T cell activation: pleiotropic pathways downstream of PIP3. Immunol Rev 192:7–20
Lee JO, Yang H, Georgescu MM, Di Cristofano A, Maehama T, Shi Y, Dixon JE, Pandolfi P, Pavletich NP (1999) Crystal structure of the PTEN tumor suppressor: implications for its phosphoinositide phosphatase activity and membrane association. Cell 99:323–334
Maehama T, Dixon JE (1998) The tumor suppressor, PTEN/MMAC1, dephosphorylates the lipid second messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem 273:13375–13378
Mensah K, Mocanu MM, Yellon DM (2005) Failure to protect the myocardium against ischemia/reperfusion injury after chronic atorvastatin treatment is recaptured by acute atorvastatin treatment: a potential role for phosphatase and tensin homolog deleted on chromosome ten? J Am College Cardiol 45:1287–1291
Miki T, Miura T, Tanno M, Nishihara M, Naitoh K, Sato T, Takahashi A,Shimamoto K (2007) Impairment of cardioprotective PI3K-Akt signaling by post-infarct ventricular remodeling is compensated by an ERK-mediated pathway. Basic Res Cardiol 102:163–170
Mocanu MM, Bell RM, Yellon DM (2002) PI3 kinase and not p42/p44 appears to be implicated in the protection conferred by ischemic preconditioning. J Mol Cell Cardiol 34:661–668
Mocanu MM, Field DC, Yellon DM (2006) A potential role for PTEN in the diabetic heart. Cardiovasc Drugs Ther 20:319–321
Mocanu MM, Yellon DM (2007) PTEN, the Achilles’ heel of myocardial ischemia/reperfusion injury? Br J Pharmacol 150:833–838
Ning K, Miller LC, Laidlaw HA, Burgess LA, Perera NM, Downes CP, Leslie NR, Ashford ML (2006) A novel leptin signalling pathway via PTEN inhibition in hypothalamic cell lines and pancreatic beta-cells. EMBO J 25:2377–2387
Philipp S, Critz SD, Cui L, Solodushko V, Cohen MV, Downey JM (2006) Localizing extracellular signal-regulated kinase (ERK) in pharmacologica preconditioning’s trigger pathway. Basic Res Cardiol 101:159–167
Podsypanina K, Ellenson LH, Nemes A, Gu J, Tamura M, Yamada KM, Cordon-Cardo C, Catoretti G, Fisher PE, Parsons R (1999) Mutation of Pten/Mmac1 in mice causes neoplasia in multiple organ systems. Proc Natl Acad Sci USA 96:1563–1568
Schmid AC, Byrne RD, Vilar R, Woscholski R (2004) Bisperoxovanadium compounds are potent PTEN inhibitors. FEBS Lett 566:35–38
Simpkin JC, Yellon DM, Davidson SM, Lim SY, Wynne AM, Smith CC (2007) Apelin-13 and apelin-36 exhibit direct cardioprotective activity against ischemiareperfusion injury. Basic Res Cardiol 102:518–528
Smith CCT, Mocanu MM, Davidson SM, Wynne AM, Simpkin JC, Yellon DM (2006) Leptin, the obesity-associated hormone, exhibits direct cardioprotective effects. Br J Pharmacol 149:5–13
Torres J, Pulido R (2001) The tumor suppressor PTEN is phosphorylated by the protein kinase CK2 at its C terminus. Implications for PTEN stability to proteasome-mediated degradation. J Biol Chem 276:993–998
Tsang A, Hausenloy DJ, Mocanu MM, Carr RD, Yellon DM (2005) Preconditioning the diabetic heart: the importance of Akt phosphorylation. Diabetes 54:2360–2364
Wang H, Douglas W, Lia M, Edelmann W, Kucherlapati R, Podsypanina K, Parsons R, Ellenson LH (2002) DNA mismatch repair deficiency accelerates endometrial tumorigenesis in Pten heterozygous mice. Am J Pathol 160:1481–1486
Wong JT, Kim PT, Peacock JW, Yau TY, Mui AL, Chung SW, Sossi V, Doudet D, Green D, Ruth TJ, Parsons R, Verchere CB, Ong CJ (2007) Pten (phosphatase and tensin homologue gene) haploinsufficiency promotes insulin hypersensitivity. Diabetologia 50:395–403
Wu DN, Pei DS, Wang Q, Zhang GY (2006) Down-regulation of PTEN by sodium orthovanadate inhibits ASK1 activation via PI3-K/Akt during cerebral ischemia in rat hippocampus. Neurosci Lett 404:98–102
Yellon DM, Hausenloy DJ (2005) Realizing the clinical potential of ischemic preconditioning and postconditioning. Nat Clin Pract Cardiovasc Med 2:568–575
Zuluaga S, Alvarez-Barrientos A, Gutierrez-Uzquiza A, Benito M, Nebreda AR, Porras A (2007) Negative regulation of Akt activity by p38[alpha] MAP kinase in cardiomyocytes involves membrane localization of PP2A through interaction with caveolin-1. Cell Signal 19:62–74
Acknowledgments
We thank Professor Ramon Parsons and Professor Dario Alessi for their generous gift of the PTEN+/− mouse model. For breeding advice we would like to thank Gail Fraser from Dundee University and Richard Pugh from UCL. We thank British Heart Foundation for providing the funding for this research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Returned for 1. Revision: 29 November 2007 1. Revision received: 5 May 2008
Returned for 2. Revision: 2 June 2008 2. Revision received: 5 June 2008
Rights and permissions
About this article
Cite this article
Siddall, H.K., Warrell, C.E., Yellon, D.M. et al. Ischemia-reperfusion injury and cardioprotection: investigating PTEN, the phosphatase that negatively regulates PI3K, using a congenital model of PTEN haploinsufficiency. Basic Res Cardiol 103, 560–568 (2008). https://doi.org/10.1007/s00395-008-0735-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00395-008-0735-y