
Abstract
Background
Treatment with warfarin greatly reduces the risk of stroke related to atrial fibrillation, but will not be effective unless patients adhere to treatment. Lack of fixed dosing makes it difficult to objectively estimate adherence to treatment from prescription data.
Objective
To evaluate two methods that assess adherence to warfarin from prescription data.
Design
Retrospective study of Swedish health care registers.
Patients and methods
Age- and sex-specific dose requirements were determined from approx. 1 million blood tests and dosing instructions. By applying these dosages to 163,785 warfarin-treated patients with atrial fibrillation, we calculated the quantity of warfarin that was needed to keep these patients on effective treatment during a mean follow-up of 3.9 years and compared that with the dispensed quantities. The ratio of available drug/time at risk constitutes a measure of adherence on group level. In addition, time intervals between refills were used to assess discontinuation.
Results
Both methods showed that 45 % of the patients did not have enough warfarin to last 80 % of the time at risk. Between 16 and 21 % of the patients discontinued within the first year, followed by 8–9 % annually during the following years. Patients with high bleeding risk and patients with low embolic risk showed lower endurance.
Conclusions
Adherence to treatment with warfarin can be estimated on group level from prescription data and may be useful for comparison of adherence with warfarin and new oral anticoagulants. When applied to a large warfarin-treated cohort with atrial fibrillation, we found that adherence is low and that measures aiming for improvements are needed .
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oral anticoagulants (OAC) are recommended for preventing thromboembolic events in patients with atrial fibrillation (AF) in combination with one additional risk factor [1]. Until recently, the only available drugs were vitamin K antagonists such as warfarin, which necessitate continuous laboratory monitoring and dose adjustments to achieve the desired effect. The effect is measured as prothrombin time (PT) expressed in a standardized way as INR (international normalized ratio). The maximum benefit is normally achieved at a therapeutic interval of INR 2.0–3.0 [2]. To evaluate the effectiveness of warfarin control over time, Rosendaal et al. [3] developed a method to estimate the time spent within the therapeutic range, which can be applied to individuals or on group level. Several studies have shown that the time in therapeutic range (TTR) is directly correlated with outcome [4–6]. Despite this, modern well-controlled randomized trials have failed to reach higher TTR values than 55–66 % [7–9] due to interactions with food, with other drugs, non-adherence to treatment and unknown causes [10].
In studies based on self-reporting, adherence of >75 % has been reported among patients on secondary prevention 1 year after a stroke/TIA [11, 12]. This is similar to adherence reported in clinical trials [13]. A study of actually dispensed warfarin in a large population-based cohort showed that adherence was 68 % 1 year after therapy initiation, 57 % after 2 years, and 39 % after 5 years [14]. Other retrospective observational studies have reported warfarin therapy persistence between 57 and 74 % after 1 year of therapy [15].
These diverging figures, illustrate that known participation in a study affects both patients and profession. In self-reported studies there is a risk for over-estimation of adherence, due to patients’ desire to perform, and due to recall bias. This is illuminated in a small cohort of AF patients in whom there was no association between TTR and patients’ self-perceived persistence to therapy but a significant correlation between TTR and the frequency by which patients came back to pharmacies for warfarin refill [16].
Aim
To evaluate methods to assess adherence to warfarin in general populations that can be used for comparisons with new oral anticoagulants in clinical settings using prescription data.
Materials and methods
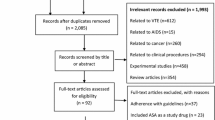
We used the Swedish Patient register to identify all 307,870 individuals with a diagnosis of AF at any Swedish hospital or hospital affiliated open clinic between July 1, 2005 and December 31, 2010.
From the National Prescribed Drugs register, we got information about warfarin purchases made by these patients. This register stores details about every prescription that is handled in all pharmacies throughout Sweden. Since this is done automatically in a national online database, the register is almost complete. The Patient register and the Drug register were cross-linked using unique personal identification numbers given to all residents of Sweden. By doing this, we found that 163,785 of all the AF patients in the Patient Register had received warfarin at least once between July 1, 2005 and December 31, 2011. These warfarin-treated AF patients constitute our study group. Minimum follow-up was 1 year. Mean follow-up was 3.9 years.
If the doses used by the patients were known, adherence to treatment could be estimated according to the drug at disposal principle. This is expressed by the time the available drug is expected to last divided by the time at risk.
For most prescribed drugs, but not for warfarin, information about the doses used is found in the Drug register. This lack makes it difficult to assess individual adherence to warfarin from prescription data, but adherence in large groups of patients may still be assessed if there is information about doses used by large groups of well-managed patients. Such data were used for our new Auricula method for estimating adherence to warfarin treatment. To validate this method, we also assessed adherence to warfarin by means of a variation of the refill frequency method. The study was approved by the Ethical Review Board in Stockholm, Sweden.
The Auricula method
In the first step, we used information from the Swedish anticoagulation and atrial fibrillation register Auricula [17] to determine what mean doses of warfarin in relation to age and sex that were needed to achieve the desired therapeutic anticoagulant effect. The Auricula cohort consisted of 25,238 warfarin-treated patients with AF registered during the period 2006–2011.
Of these, 15,232 (60.3 %) were male and 10,006 (39.7 %) were female. The mean age was 73.0 ± 10.2 years. For this group, we had access to 1,024,020 INR values with associated dosing instructions. We excluded INR values and dosing instructions made during the first 30 days of treatment before maintenance doses had been found. Thus, our calculations are made from 926,233 INR test results with associated dosing instructions. Patients were stratified according to gender and age using 1-year classes. INR values and doses were analyzed according to the age at the time of the test. Time in therapeutic range (TTR) was calculated according to the Rosendaal method [3]. In the second step, we attributed age- and sex-specific doses derived from the Auricula cohort to patients in the national Patient register, e.g., all 307,870 patients with a hospital diagnosis of non-valvular AF in Sweden, and calculated how much warfarin would be needed to cover all days at risk for this group.
To test the robustness of the results achieved with mean doses from Auricula, we generated normally distributed simulated doses with the same standard deviations as in Auricula. Generated negative doses were disregarded. This simulation was repeated 10 times, similar to a bootstrap procedure, to see how much skewing of dose requirements in the derivation cohort distorted the results.
In the final third step, we calculated how many days the supplies of the whole population, and of subgroups, would have lasted with perfect adherence and related that to the number of days at risk. Non-adherence was defined as patients having access to less warfarin than needed to cover 80 % of the time at risk, in accordance with the practice in previous studies [18–20].
The refill interval method
In general, drugs in Sweden cannot be prescribed in larger quantities than what is expected to last 3 months. This is, however, not a strict rule, and available sizes of packages influence prescriptions. For instance, a patient with a maintenance dose of 1, 5 tablets a day needs approximately 140 tablets during a three-month period, but will most likely receive a prescription for 200 tablets, because warfarin comes in packages of 100 tablets. In consequence, this patient does not have to come for a refill as often as every third month. The duration of the interval between purchases, and the quantities dispensed, may therefore be used to estimate the individual dose.
With the Refill Interval method, we considered patients to be on treatment for the full time between two purchases of warfarin, as long as they did come back for more at least once in a 6-month period. If there was no new purchase within 6 months, the patient was considered to have terminated treatment at a date corresponding to the previous purchase plus the mean interval between purchases before discontinuation. Patients who only made one purchase were considered to have stopped after having consumed the dispensed quantity at the age- and sex-specific mean daily dose of the Auricula cohort.
We then calculated each patient’s cumulative time on treatment and related that to each patient’s time at risk in the same way as with the Auricula method.
Results
The Auricula method
Warfarin dose requirement
The median daily dose of warfarin was 4.13 mg in the Auricula cohort. The mean dose was 4.20 ± 1.89 mg (Fig 1). There was a linear inverse relationship between age and dose in both men and women (Fig 2). Patients in the youngest age group had twice as high doses as patients in the oldest age group (6.07 ± 2.74 mg vs. 3.01 ± 1.45 mg, p < 0.0001) and higher in men than among women. The mean dose, expressed as milligrams per day, could be described by the equation 9.344333–0.067688 × age (years) for men, and by 8.994259–0.068527 × age (years) for women.

Individual mean doses of warfarin among patients in the Auricula cohort

Daily doses of warfarin in milligrams in relation to age and sex. Error bars represent 95 % CI. Based on 926,233 dosing instructions
Treatment intensity and time in therapeutic range
The mean INR value of approximately 1 million INR values in Auricula was 2.49 ± 0.66 (median 2.40). The overall TTR for the entire cohort was 74.6 % with 10.5 % of the time above INR 3.0 and 14.8 % below INR 2.0, for values in relation to age and sex, see Table 1. Younger patients spent more time out of therapeutic range than older patients. There were no significant differences between the sexes with respect to TTR.
Application to the national AF cohort
During the study period approximately 837 kg of warfarin were distributed among 163,785 AF patients. The demographic composition of the Auricula cohort and the national AF cohort was almost the same; mean age 73.3 ± 9.9 years vs.73.2 ± 10.2 years, female sex 39.7 vs. 40.6 %.
Age- and sex-specific mean doses from Auricula were attributed to the patients in the national cohort to estimate how long the dispensed quantity was likely to last. Assuming that all patients consumed warfarin at the mean age- and sex-specific dose until they ran out of supply, we estimated that 16 % of the patients discontinued treatment within the first year, followed by 8–9 % annual dropout rate during the following years (Fig. 3). Forty-five per cent of the patients showed non-adherence, defined as having had access to less warfarin than needed to cover 80 % of the time. The lowest adherence was found lower among the youngest and the oldest (Table 2) without differences between men at women at equal ages (not shown). Patients with prior bleedings, renal or liver disease, alcohol abuse or dementia had lower adherence (Table 3). Patients at low risk of embolic stroke (CHA2DS2-VASc score 0–1) were more often non-adherent than patients with higher risk scores (46.1 vs. 56.6 %, p < 0.0001). Conversely, patients at high bleeding risk (modified HAS-BLED score ≥4) more often non-adherent than patient with lower bleeding risk (50.7 vs. 54.7 %, p < 0.0001)

Percentage of patients in the national AF cohort remaining on warfarin treatment in relation to time from treatment start
To further explore the Auricula method, we assigned patients with random doses normally distributed around the mean values in Auricula, using the same standard deviations. Repeated simulations yielded very consistent estimates, only differing by 0.2 % when performed on the entire warfarin exposed cohort of 163,785 patients. When performed in smaller subsets, the influence of chance on the results increased. In random samples of 10,000 patients results varied by 1.2 %, in samples of 1,000 patients by 3.1 % and in samples of 100 patients by 8.5 %.
The refill interval method
When dispensed quantities of warfarin were divided by the number of days between refill visits, the median dose was estimated to be 4.60 mg per day. Assuming that all patients consumed warfarin at a regular rate until they ran out of supply, this method estimated that 21 % of the patients discontinued treatment within the first year, followed by 8–9 % annual dropout rate during the following years (Fig. 3). Approximately 45 % of the patients showed non-compliance. Patients with high bleeding risk and patients with low embolic showed lower endurance (Table 3).
Discussion
Using two new methods for assessment of adherence to warfarin treatment from drug prescription data, we found that 45 % of patients using warfarin against AF-related stroke did not have access to enough warfarin to last 80 % of the time at risk. After 3 years, between one-third and half of them no longer used warfarin. Some may have stopped because of bleedings, as indicated by lower adherence among patients with a history of bleedings. Others may have stopped because they only had temporary treatment in conjunction with a planned cardioversion, as indicated by low adherence among young patients without risk factors. It is, however, highly improbable that this accounts for more than a small portion of all discontinuations.
Our findings confirm earlier observations of low adherence among young patients, and among patients with low thromboembolic risk (CHA2DS2-VASc score 0–1) [11, 14] as well as among patients with dementia, alcohol abuse and bleeding problems [21]. The finding that patients with high bleeding risk (modified HAS-BLED score ≥4) were sooner to stop treatment confirms the findings by Hylek and co-workers [22]. Unlike others [14, 23], we found no difference in adherence between men and women at equal ages.
Our estimate that 16–21 % of the patients discontinue treatment within the first year, followed by 8–9 % annual dropout rate during the following years is lower than what was reported in a Canadian population-based study [14] where 32 % discontinued treatment already within the first year of treatment. The introduction of structured care for patients on anticoagulant treatment in Sweden during recent years may account for some of this difference, since it has been shown to improve adherence to treatment [15]. How adherence of warfarin is related to outcome was not the topic of the present study. However, it is reasonable to believe that poor compliance will result in an unfavorable outcome [24, 25].
Atrial fibrillation is a disease that is associated with aging. The mean age of AF populations is generally reported to be around 75 years. Considering that dose requirements of warfarin decline with increasing age, it is clear that the Defined Daily Dose (DDD) of 7.5 mg specified by the World Health Organization (WHO) has little resemblance with the real doses used by AF patients. In Auricula, it was 4.5 mg for men and 3.7 mg for women. It may therefore be questioned if the DDD concept is relevant for warfarin.
Advantages with the methods used
Both of the methods we used produced similar results although they are based on different principles. They thereby validate each other. The methods appear to be neutral in relation to which drug they are used to assess, and should therefore be possible to use for comparisons of adherence between different drugs, e.g., between warfarin and new oral anticoagulants. Being able to identify groups of patients where adherence is low may also be important from a health economic perspective, since it has been shown that non-adherence to warfarin in AF patients is associated to higher total health care costs [26]. This information may be used to target interventions to improve adherence. Assessment of adherence with these methods produces rapid results at very low costs, compared to the costs of prospective studies based on self-reporting from the patients, and without the biases that affect interventional studies.
Limitations
Methods based on the drug at disposal principle are prone to exaggerate adherence to treatment. True adherence is always lower, because patients may not take all medicine they purchase.
Patients who come back for refills are likely to have consumed what they already purchased, but if there is only one prescription it is impossible to know how much of it that was used as intended. Nor is it possible to know if the last refill in a series was used or still rests in a drawer. Therefore, estimates are likely to be more accurate for patients with many refills.
It is difficult to distinguish direct discontinuation from poor compliance with drug at disposal-based methods unless patients come back for refills at regular intervals. The Refill Interval method may therefore be less sensitive to this bias effect, than the Auricula method. The Auricula method, on the other hand, may be more exact for assessing per cent of time a risk with treatment. Used together they complement each other and make it possible to perform more secure estimates. The difficulties in differentiating between patients who frequently forget their medication and patients who abruptly stop taking it are certainly a limitation. However, a finding of low adherence still signifies that these patients did not have the protection against AF-related stroke that was originally intended.
Management of patients in Sweden is often managed in specialized centres and TTR values are often very high in comparison with most other countries [6]. Sweden also has a relatively genetically homogenous population whose individual contacts with the health care system can be followed over decades with very few individuals lost to follow-up. It is possible that the methods we propose will not work as well in a setting very much different from ours.
Conclusion
Adherence to treatment with warfarin can be estimated on group level from prescription data and may be useful for comparison of adherence with warfarin and new oral anticoagulants. When applied to a large warfarin-treated cohort with atrial fibrillation, we found that adherence is low and that measures aiming for improvements are needed.
Reference
Camm AJ, Lip GY, De Caterina R et al (2012) 2012 focused update of the esc guidelines for the management of atrial fibrillation: An update of the 2010 esc guidelines for the management of atrial fibrillation developed with the special contribution of the european heart rhythm association. Europace 14:1385–1413
Aguilar MI, Hart R (2005) Oral anticoagulants for preventing stroke in patients with non-valvular atrial fibrillation and no previous history of stroke or transient ischemic attacks. Cochrane Database Syst Rev 3:CD001927
Rosendaal FR, Cannegieter SC, van der Meer FJ et al (1993) A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost 69:236–239
Connolly SJ, Pogue J, Eikelboom J et al (2008) Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 118:2029–2037
Morgan CL, McEwan P, Tukiendorf A et al (2009) Warfarin treatment in patients with atrial fibrillation: observing outcomes associated with varying levels of INR control. Thromb Res 124:37–41
Wallentin L, Yusuf S, Ezekowitz MD et al (2010) Efficacy and safety of dabigatran compared with warfarin at different levels of international normalised ratio control for stroke prevention in atrial fibrillation: an analysis of the RE-LY trial. Lancet 376:975–983
Patel MR, Mahaffey KW, Garg J et al (2011) Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. New Eng J Med 365:883–891
Connolly SJ, Ezekowitz MD, Yusuf S et al (2009) Dabigatran versus warfarin in patients with atrial fibrillation. New Eng J Med 361:1139–1151
Granger CB, Alexander JH, McMurray JJ et al (2011) Apixaban versus warfarin in patients with atrial fibrillation. New Eng J Med 365:981–992
Jorgensen AL, Hughes DA, Hanson A et al (2013) Adherence and variability in warfarin dose requirements: assessment in a prospective cohort. Pharmacogenomics 14:151–163
Sappok T, Faulstich A, Stuckert E et al (2001) Compliance with secondary prevention of ischemic stroke: a prospective evaluation. Stroke 32:1884–1889
Hamann GF, Weimar C, Glahn J et al (2003) Adherence to secondary stroke prevention strategies–results from the german stroke data bank. Cerebrovasc Dis 15:282–288
De Schryver EL, van Gijn J, Kappelle LJ et al (2005) Non-adherence to aspirin or oral anticoagulants in secondary prevention after ischaemic stroke. J Neurol 252:1316–1321
Gomes T, Mamdani MM, Holbrook AM et al (2012) Persistence with therapy among patients treated with warfarin for atrial fibrillation. Arch Intern Med 172:1687–1689
Maxwell W, Bennett CL (2012) Will newer anticoagulants improve therapy persistence? Arch Intern Med 172:1689–1690
Wang Y, Kong MC, Ko Y (2013) Comparison of three medication adherence measures in patients taking warfarin. J Thromb Thrombol 36:416–421
Auricula. In: Auricula annual report 2011 [auricula årsrapport 2011]. UCR, Uppsala Clinical Research Center 2013, http://www.ucr.uu.se/auricula/index.php/arsrapporter. Accessed 23 Jan 2014
Mattson ME, Friedman LM (1984) Issues in medication adherence assessment in clinical trials of the national heart, lung, and blood institute. Controll Clin Trial 5:488–496
Kimmel SE, Chen Z, Price M et al (2007) The influence of patient adherence on anticoagulation control with warfarin: results from the international normalized ratio adherence and genetics (in-range) study. Arch Intern Med 167:229–235
Yeaw J, Benner JS, Walt JG et al (2009) Comparing adherence and persistence across 6 chronic medication classes. J Manag Care Pharm 15:728–740
Ewen S, Rettig-Ewen V, Mahfoud F et al (2014) Drug adherence in patients taking oral anticoagulation therapy. Clin Res Cardiol 103:173–182
Hylek EM, Evans-Molina C, Shea C et al (2007) Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 115:2689–2696
Glader EL, Sjölander M, Eriksson M et al (2010) Persistent use of secondary preventive drugs declines rapidly during the first 2 years after stroke. Stroke 41:397–401
White HD, Gruber M, Feyzi J et al (2007) Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: results from SPORTIF III and V. Arch Intern Med 167:239–245
Nieuwlaat R, Connolly BJ, Hubers LM, ACTIVE Investigators et al (2012) Quality of individual INR control and the risk of stroke and bleeding events in atrial fibrillation patients: a nested case control analysis of the ACTIVE W study. Thromb Res 129:715–719
Casciano JP, Dotiwala ZJ, Martin BC et al (2013) The costs of warfarin underuse and nonadherence in patients with atrial fibrillation: a commercial insurer perspective. J Manag Care Pharm 19:302–316
Conflict of interest
None of the authors have support from any company for the submitted work. MS has nothing to declare. LF has given lectures, received funding or participated as consultant to Sanofi-Aventis, Boehringer-Ingelheim, Bayer, BMS, and St Jude Medical.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Skeppholm, M., Friberg, L. Adherence to warfarin treatment among patients with atrial fibrillation. Clin Res Cardiol 103, 998–1005 (2014). https://doi.org/10.1007/s00392-014-0742-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-014-0742-y